

Recurrent Esthesioneuroblastoma: Long-Term Outcomes of Salvage Therapy

 , ,
, ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
3. Results
3.1. Patient Characteristics
3.2. Salvage Therapy
3.3. Secondary Recurrence
3.4. Survival Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Gore, M.R.; Zanation, A.M. Salvage Treatment of Local Recurrence in Esthesioneuroblastoma: A Meta-analysis. Skull Base 2011, 21, 1–6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maina, I.W.; Lehrich, B.M.; Goshtasbi, K.; Su, B.M.; Stubbs, V.C.; Tong, C.; Kohanski, M.A.; Lee, J.Y.; Luu, Q.C.; Newman, J.G.; et al. Extraprimary Local Recurrence of Esthesioneuroblastoma: Case Series and Literature Review. World Neurosurg. 2020, 144, e546–e552. [Google Scholar] [CrossRef] [PubMed]
- Arosio, A.D.; Bernasconi, D.P.; Valsecchi, M.G.; Pacifico, C.; Battaglia, P.; Bignami, M.; Ferrari, M.; Mattavelli, D.; Rampinelli, V.; Tomasoni, M.; et al. Patterns of recurrences in sinonasal cancers undergoing an endoscopic surgery-based treatment: Results of the MUSES* on 940 patients: *MUlti-institutional collaborative Study on Endoscopically treated Sinonasal cancers. Oral Oncol. 2022, 134, 106123. [Google Scholar] [CrossRef] [PubMed]
- Mozaffari, K.; Pradhan, A.; Yang, I.; Patel, K.; Vivas, A.C. Metastatic esthesioneuroblastoma recurrence after 19 years of remission: A systematic review with case illustration. J. Neurol. Sci. 2022, 442, 120406. [Google Scholar] [CrossRef]
- Lund, V.J.; Howard, D.; Wei, W.; Spittle, M. Olfactory Neuroblastoma: Past, Present, and Future? Laryngoscope 2003, 113, 502–507. [Google Scholar] [CrossRef]
- Loy, A.H.; Reibel, J.F.; Read, P.W.; Thomas, C.Y.; Newman, S.A.; Jane, J.A.; Levine, P.A. Esthesioneuroblastoma: Continued follow-up of a single institution’s experience. Arch. Otolaryngol. Neck Surg. 2006, 132, 134–138. [Google Scholar] [CrossRef] [Green Version]
- Miller, K.C.; Marinelli, J.P.; Janus, J.R.; Chintakuntlawar, A.V.; Foote, R.L.; Link, M.J.; Choby, G.; Van Gompel, J.J. Induction Therapy Prior to Surgical Resection for Patients Presenting with Locally Advanced Esthesioneuroblastoma. J. Neurol. Surg. Part B Skull Base 2021, 82 (Suppl. 3), e131–e137. [Google Scholar] [CrossRef]
- Lopez, D.C.; Wadley, A.E.; London, N.R., Jr. Emerging concepts in sinonasal tumor research. Curr. Opin. Otolaryngol. Head Neck Surg. 2022, 30, 33–39. [Google Scholar] [CrossRef]
- Karp, E.E.; Van Gompel, J.J.; Choby, G. Esthesioneuroblastoma (Olfactory Neuroblastoma): Overview and Extent of Surgical Approach and Skull Base Resection. J. Neurol. Surg. Rep. 2022, 83, e80–e82. [Google Scholar] [CrossRef]
- Su, S.Y.; Bell, D.; Ferrarotto, R.; Phan, J.; Roberts, D.; Kupferman, M.E.; Frank, S.J.; Fuller, C.D.; Gunn, G.B.; Kies, M.S.; et al. Outcomes for olfactory neuroblastoma treated with induction chemotherapy. Head Neck 2017, 39, 1671–1679. [Google Scholar] [CrossRef]
- Morita, A.; Ebersold, M.J.; Olsen, K.D.; Foote, R.L.; Lewis, J.E.; Quast, L.M. Esthesioneuroblastoma: Prognosis and management. Neurosurgery 1993, 32, 706–714. [Google Scholar] [CrossRef] [PubMed]
- Bs, K.G.; Abiri, A.; Abouzari, M.; Sahyouni, R.; Wang, B.Y.; Tajudeen, B.A.; Hsu, F.P.K.; Cadena, G.; Kuan, E.C. Hyams grading as a predictor of metastasis and overall survival in esthesioneuroblastoma: A meta-analysis. Int. Forum Allergy Rhinol. 2019, 9, 1054–1062. [Google Scholar] [CrossRef]
- Joshi, R.R.; Spector, M.E.; Husain, Q.; Roman, B.R.; Cracchiolo, J.; Yu, Y.; Tsai, J.; Kang, J.; McBride, S.; Lee, N.Y.; et al. Comparing Kadish, TNM, and the modified Dulguerov staging systems for esthesioneuroblastoma. J. Surg. Oncol. 2018, 119, 130–142. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gallagher, K.; Pepper, J.P.; Light, E.; McKean, E.; Marentette, L.; McHugh, J. Esthesioneuroblastoma: Updating Histologic Grading as It Relates to Prognosis. Ann. Otol. Rhinol. Laryngol. 2014, 123, 353–358. [Google Scholar] [CrossRef]
- Palejwala, S.K.; Sharma, S.; Le, C.H.; Chang, E.; Lemole, M. Complications of Advanced Kadish Stage Esthesioneuroblastoma: Single Institution Experience and Literature Review. Cureus 2017, 9, e1245. [Google Scholar] [CrossRef] [Green Version]
- Banuchi, V.E.; Dooley, L.; Lee, N.Y.; Pfister, D.G.; McBride, S.; Riaz, N.; Bilsky, M.H.; Ganly, I.; Shah, J.P.; Kraus, D.H.; et al. Patterns of regional and distant metastasis in esthesioneuroblastoma. Laryngoscope 2016, 126, 1556–1561. [Google Scholar] [CrossRef] [Green Version]
- Zeng, Q.; Tian, Y.; He, Y.; Xie, Q.; Ou, L.; Wang, M.; Chen, W.; Wei, R. Long-Term Survival Outcomes and Treatment Experience of 64 Patients With Esthesioneuroblastoma. Front. Oncol. 2021, 11, 624960. [Google Scholar] [CrossRef]
- Ferlito, A.; Rinaldo, A.; Rhys-Evans, P.H. Contemporary clinical commentary: Esthesioneuroblastoma: An update on management of the neck. Laryngoscope 2003, 113, 1935–1938. [Google Scholar] [CrossRef]
- Monroe, A.T.; Hinerman, R.W.; Amdur, R.J.; Ms, C.G.M.; Mendenhall, W.M. Radiation therapy for esthesioneuroblastoma: Rationale for elective neck irradiation. Head Neck 2003, 25, 529–534. [Google Scholar] [CrossRef]
- Zanation, A.M.; Ferlito, A.; Rinaldo, A.; Gore, M.R.; Lund, V.J.; McKinney, K.A.; Suárez, C.; Takes, R.P.; Devaiah, A. When, how and why to treat the neck in patients with esthesioneuroblastoma: A review. Eur. Arch. Oto-Rhino-Laryngol. 2010, 267, 1667–1671. [Google Scholar] [CrossRef] [Green Version]
- Davis, R.E.; Weissler, M.C. Esthesioneuroblastoma and neck metastasis. Head Neck 1992, 14, 477–482. [Google Scholar] [CrossRef] [PubMed]
- Jiang, W.; Mohamed, A.S.; Fuller, C.; Kim, B.Y.; Tang, C.; Gunn, G.B.; Hanna, E.Y.; Frank, S.J.; Su, S.Y.; Diaz, E.; et al. The role of elective nodal irradiation for esthesioneuroblastoma patients with clinically negative neck. Pract. Radiat. Oncol. 2015, 6, 241–247. [Google Scholar] [CrossRef] [Green Version]
- Demiroz, C.; Gutfeld, O.; Aboziada, M.; Brown, D.; Marentette, L.J.; Eisbruch, A. Esthesioneuroblastoma: Is There a Need for Elective Neck Treatment? Int. J. Radiat. Oncol. Biol. Phys. 2011, 81, e255–e261. [Google Scholar] [CrossRef] [PubMed]
- Yin, Z.-Z.; Luo, J.-W.; Gao, L.; Yi, J.-L.; Huang, X.-D.; Qu, Y.; Wang, K.; Zhang, S.-P.; Xiao, J.-P.; Xu, G.-Z.; et al. Spread patterns of lymph nodes and the value of elective neck irradiation for esthesioneuroblastoma. Radiother. Oncol. 2015, 117, 328–332. [Google Scholar] [CrossRef] [PubMed]
- Lechner, M.; Takahashi, Y.; Turri-Zanoni, M.; Liu, J.; Counsell, N.; Hermsen, M.; Kaur, R.P.; Zhao, T.; Ramanathan, M., Jr.; Schartinger, V.H.; et al. Clinical outcomes, Kadish-INSICA staging and therapeutic targeting of somatostatin receptor 2 in olfactory neuroblastoma. Eur. J. Cancer 2022, 162, 221–236. [Google Scholar] [CrossRef] [PubMed]
- Fujiwara, M.; Kamikonya, N.; Odawara, S.; Suzuki, H.; Niwa, Y.; Takada, Y.; Doi, H.; Terada, T.; Uwa, N.; Sagawa, K.; et al. The threshold of hypothyroidism after radiation therapy for head and neck cancer: A retrospective analysis of 116 cases. J. Radiat. Res. 2015, 56, 577–582. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gujral, D.M.; Chahal, N.; Senior, R.; Harrington, K.J.; Nutting, C.M. Radiation-induced carotid artery atherosclerosis. Radiother. Oncol. 2014, 110, 31–38. [Google Scholar] [CrossRef] [PubMed]
- Peacock, J.G.; Harmsen, W.S.; Link, M.J.; Van Gompel, J.J.; Giannini, C.; Olsen, K.D.; Garces, Y.I.; Wittich, M.A.N.; Ma, D.J.; Park, S.S.; et al. Risk of Delayed Lymph Node Metastasis in Clinically N0 Esthesioneuroblastoma. J. Neurol. Surg. Part B Skull Base 2016, 78, 68–74. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McMillan, R.A.; Van Gompel, J.J.; Link, M.J.; Moore, E.J.; Price, D.L.; Stokken, J.K.; Van Abel, K.M.; O’Byrne, J.; Giannini, C.; Chintakuntlawar, A.; et al. Long-term oncologic outcomes in esthesioneuroblastoma: An institutional experience of 143 patients. Int. Forum Allergy Rhinol. 2022, 12, 1457–1467. [Google Scholar] [CrossRef] [PubMed]
- Malouf, G.G.; Casiraghi, O.; Deutsch, E.; Guigay, J.; Temam, S.; Bourhis, J. Low- and high-grade esthesioneuroblastomas display a distinct natural history and outcome. Eur. J. Cancer 2013, 49, 1324–1334. [Google Scholar] [CrossRef]
- Kaur, G.; Kane, A.J.; Sughrue, M.E.; Madden, M.; Oh, M.C.; Sun, M.Z.; Safaee, M.; El-Sayed, I.; Aghi, M.; McDermott, M.W.; et al. The prognostic implications of Hyam’s subtype for patients with Kadish stage C esthesioneuroblastoma. J. Clin. Neurosci. 2013, 20, 281–286. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Gompel, J.J.; Giannini, C.; Olsen, K.D.; Moore, E.; Piccirilli, M.; Foote, R.L.; Buckner, J.C.; Link, M.J. Long-Term Outcome of Esthesioneuroblastoma: Hyams Grade Predicts Patient Survival. J. Neurol. Surg. Part B Skull Base 2012, 73, 331–336. [Google Scholar] [CrossRef] [Green Version]
- Dulguerov, P.; Allal, A.S.; Calcaterra, T.C. Esthesioneuroblastoma: A meta-analysis and review. Lancet Oncol. 2001, 2, 683–690. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bell, D.; Saade, R.; Roberts, D.; Ow, T.J.; Kupferman, M.; Demonte, F.; Hanna, E.Y. Prognostic Utility of Hyams Histological Grading and Kadish-Morita Staging Systems for Esthesioneuroblastoma Outcomes. Head Neck Pathol. 2015, 9, 51–59. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miyamoto, R.C.; Gleich, L.L.; Biddinger, P.W.; Gluckman, J.L. Esthesioneuroblastoma and Sinonasal Undifferentiated Carcinoma: Impact of Histological Grading and Clinical Staging on Survival and Prognosis. Laryngoscope 2000, 110, 1262–1265. [Google Scholar] [CrossRef]
- Xiong, L.; Zeng, X.-L.; Guo, C.-K.; Liu, A.-W.; Huang, L. Optimal treatment and prognostic factors for esthesioneuroblastoma: Retrospective analysis of 187 Chinese patients. BMC Cancer 2017, 17, 254. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Mean age at recurrence (years) | 56.83 (range: 30.8 to 85.1) |
| Mean time to recurrence (years) | 4.74 (range: 0.08 to 15.91) |
| Sex (%) | |
| Male | 17 (38) |
| Female | 28 (62) |
| Surgical approach for primary tumor (%) | |
| Endoscopic | 6 (13) |
| Transcranial | 28(62) |
| Combined | 8 (18) |
| Unresectable | 1 (2) |
| Lateral rhinectomy | 2 (4) |
| Other treatments (%) | |
| Radiation therapy | 41 (91) |
| Gama knife surgery | 9 (22) |
| Chemotherapy | 27 (60) |
| Hyams grade (%) | |
| Grade 1 | 4 (9) |
| Grade 2 | 17 (38) |
| Grade 3 | 18 (40) |
| Grade 4 | 6 (13) |
| Kadish stage (%) | |
| Stage A | 1 (2) |
| Stage B | 6 (13) |
| Stage C | 36 (80) |
| Stage D | 2 (4) |
| Location of Recurrence | Number of Patients (%) | Time to Recurrence (Month) |
|---|---|---|
| Sinonasal | 10 (22.2%) | 57.4 |
| Intracranial a | 14 (31.1%) | 39.6 |
| Cervical lymph node(s) | 15 (33.3%) | 52.0 |
| Distal organs b | 6 (13.3%) | 57.2 |
| Hyams Grade 1 and 2 (n = 21) | Hyams Grade 3 and 4 (n = 24) | p-Value | |
|---|---|---|---|
| Time to recurrence (years) | 5.70 | 3.75 | <0.05 |
| Sinonasal Recurrence (n = 10) | Regional or Distal Recurrence (n = 35) | p-Value | |
|---|---|---|---|
| Mean Kadish stage of primary tumors | 2.60 | 3.03 | <0.05 |
| Modalities of therapy (%) | |
| Single | 17 (44) |
| Dual | 12 (30) |
| Triple | 10 (26) |
| Surgical treatment (%) | 27 (69%) |
| Surgical approach for recurrence (%) | |
| Endoscopic | 4 (10) |
| Transcranial | 3 (8) |
| Other open surgery | 7 (18) |
| Neck dissection | 20 (51) |
| Other treatments (%) | |
| Radiation therapy | 22 (56) |
| Gama knife surgery | 8 (20) |
| Chemotherapy | 10 (26) |
| Patient # | Surgery | Kadish | Hyams | Margin Status | Radiotherapy for Primary ENB | Primary Recurrence | Secondary Recurrence | Time to Secondary Recurrence (Months) | Vital Status |
|---|---|---|---|---|---|---|---|---|---|
| 1 | Transcranial | C | 3 | Unknown | Yes | L frontal lobe, dura, bone, and skin | R oral cavity, R submandibular gland, and L parotid | 1 | Deceased |
| 2 | Transcranial | C | 2 | Negative | Yes | R frontal dura and lobe | R maxillary sinus | 82 | Deceased |
| 3 | Transcranial | C | 3 | Negative | Yes | L frontal parasagittal dura | Bilateral neck and L parotid | 32 | Alive |
| 4 | Unresectable | C | 2 | Unknown | Yes | Sinonasal cavity | Sinonasal cavity | 70 | Deceased |
| 5 | Transcranial | C | 2 | Negative | No | R nasal cavity and R maxillary sinus | R neck | 77 | Alive |
| 6 | Transcranial | C | 3 | Positive | Yes | R neck | R parietal dura | 4 | Alive |
| 7 | Combined | C | 3 | Negative | Yes | L neck | L ethmoid sinus | 5 | Alive |
| 8 | Endoscopic | B | 3 | Positive | Yes | R neck | Retropharyngeal node | 6 | Alive |
| 9 | Transcranial | B | 2 | Unknown | Yes | Maxilla/oral cavity | L maxillary sinus and L neck | 17 | Deceased |
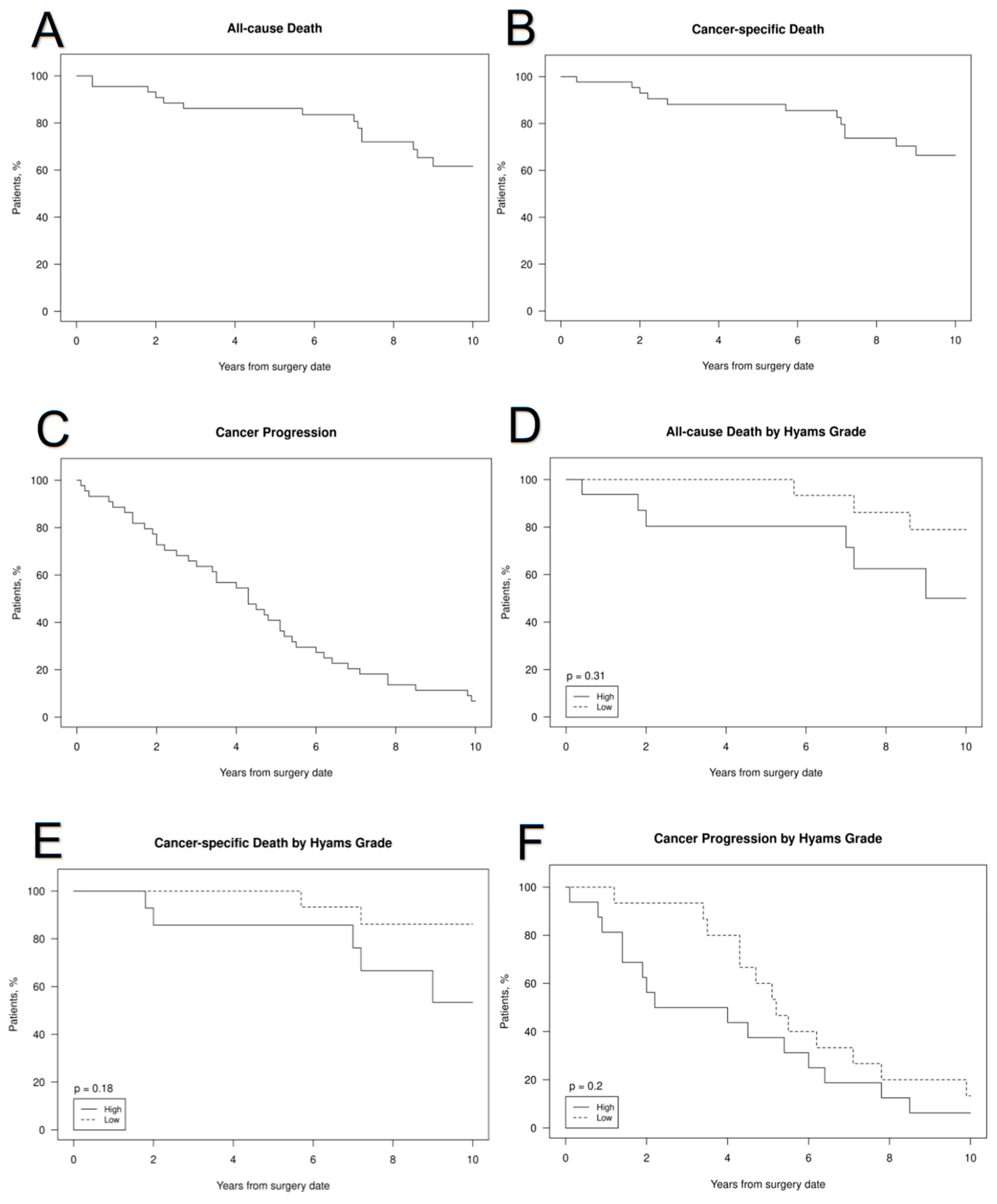
| All-Cause Death | |||
| Year | Overall | Hyams Grade | |
| High | Low | ||
| 1 | 5% (0–11%) | 6% (0–17%) | 0% (0–0%) |
| 2 | 9% (0–17%) | 20% (0–37%) | 0% (0–0%) |
| 5 | 14% (3–24%) | 20% (0–37%) | 0% (0–0%) |
| 10 | 38% (20–53%) | 50% (8–73%) | 21% (0–40%) |
| Cancer–Specific Death | |||
| High | Low | ||
| 1 | 2% (0–7%) | 0% (0–0%) | 0% (0–0%) |
| 2 | 7% (0–14%) | 14% (0–31%) | 0% (0–0%) |
| 5 | 12% (2–21%) | 14% (0–31%) | 0% (0–0%) |
| 10 | 34% (16–48%) | 47% (3–71%) | 14% (0–30%) |
| Cancer Progression | |||
| High | Low | ||
| 1 | 11% (2–20%) | 19% (0–36%) | 0% (0–0%) |
| 2 | 27% (13–39%) | 44% (13–64%) | 7% (0–19%) |
| 5 | 59% (42–71%) | 63% (29–80%) | 40% (9–60%) |
| 10 | 93% (80–98%) | 94% (58–99%) | 87% (52–96%) |
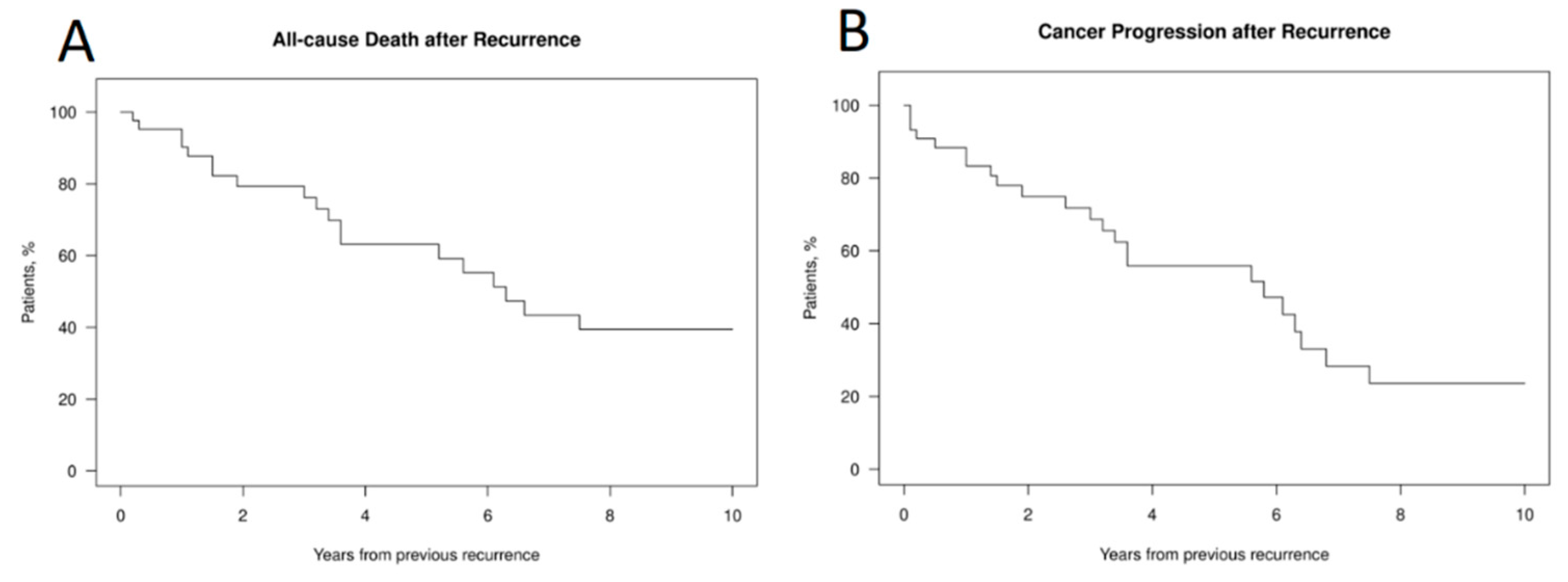
| Year | All-Cause Death | Cancer Progression |
|---|---|---|
| 1 | 10% (0–18%) | 17% (5–27%) |
| 2 | 21% (7–33%) | 25% (10–38%) |
| 5 | 37% (18–51%) | 44% (25–59%) |
| 10 | 61% (38–75%) | 76% (51–89%) |
| Parameter | All-Cause Death | Cancer-Specific Death | Cancer Progression | |||
|---|---|---|---|---|---|---|
| HR (95% CI) | p-Value | HR (95% CI) | p-Value | HR (95% CI) | p-Value | |
| Age | 0.97 (0.93, 1.01) | 0.17 | 0.96 (0.92, 1.01) | 0.10 | 0.98 (0.95, 1.00) | 0.07 |
| Sex | ||||||
| F | Ref | Ref | Ref | |||
| M | 0.64 (0.23, 1.73) | 0.38 | 0.55 (0.18, 1.67) | 0.29 | 0.81 (0.35, 1.86) | 0.62 |
| Surgery | 0.82 | 0.91 | 0.59 | |||
| Endoscopic | 5.49 (0.30, 100.93) | 0.25 | - | 2.07 (0.34, 12.54) | 0.43 | |
| Transcranial | 2.51 (0.31, 20.21) | 0.39 | - | 1.54 (0.35, 6.77) | 0.57 | |
| Combined | 1.95 (0.18, 21.61) | 0.59 | - | 2.90 (0.55, 15.22) | 0.21 | |
| Unresectable | 1.48 (0.09, 24.39) | 0.78 | - | 4.30 (0.36, 51.42) | 0.25 | |
| Lateral rhinotomy | Ref | Ref | Ref | |||
| Resection | 1.00 | 0.89 | 0.69 | |||
| 1 | Ref | Ref | Ref | |||
| 2 | - | - | 0.51 (0.07, 3.86) | 0.52 | ||
| 3 | 1.02 (0.23, 4.63) | 0.98 | 0.60 (0.08, 4.78) | 0.63 | 1.38 (0.41, 4.63) | 0.61 |
| GKS gamma knife | ||||||
| 0 | Ref | Ref | Ref | |||
| 1 | 0.48 (0.11, 2.11) | 0.33 | 0.68 (0.15, 3.04) | 0.61 | 0.63 (0.24, 1.68) | 0.36 |
| Final margins | 0.47 | 0.85 | 0.82 | |||
| Negative | Ref | Ref | Ref | |||
| Positive | 0.74 (0.09, 6.09) | 0.78 | 0.77 (0.09, 6.38) | 0.81 | 0.89 (0.29, 2.72) | 0.84 |
| Unknown | 1.70 (0.65, 4.45) | 0.28 | 1.28 (0.43, 3.85) | 0.66 | 1.25 (0.55, 2.83) | 0.60 |
| Hyams grade | ||||||
| Low | Ref | Ref | Ref | |||
| High | 1.63 (0.63, 4.24) | 0.31 | 2.07 (0.71, 6.05) | 0.19 | 1.60 (0.78, 3.29) | 0.20 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ni, G.; Pinheiro-Neto, C.D.; Iyoha, E.; Van Gompel, J.J.; Link, M.J.; Peris-Celda, M.; Moore, E.J.; Stokken, J.K.; Gamez, M.; Choby, G. Recurrent Esthesioneuroblastoma: Long-Term Outcomes of Salvage Therapy. Cancers 2023, 15, 1506. https://doi.org/10.3390/cancers15051506
Ni G, Pinheiro-Neto CD, Iyoha E, Van Gompel JJ, Link MJ, Peris-Celda M, Moore EJ, Stokken JK, Gamez M, Choby G. Recurrent Esthesioneuroblastoma: Long-Term Outcomes of Salvage Therapy. Cancers. 2023; 15(5):1506. https://doi.org/10.3390/cancers15051506
Chicago/Turabian StyleNi, Garrett, Carlos D. Pinheiro-Neto, Ehiremen Iyoha, Jamie J. Van Gompel, Michael J. Link, Maria Peris-Celda, Eric J. Moore, Janalee K. Stokken, Mauricio Gamez, and Garret Choby. 2023. "Recurrent Esthesioneuroblastoma: Long-Term Outcomes of Salvage Therapy" Cancers 15, no. 5: 1506. https://doi.org/10.3390/cancers15051506
APA StyleNi, G., Pinheiro-Neto, C. D., Iyoha, E., Van Gompel, J. J., Link, M. J., Peris-Celda, M., Moore, E. J., Stokken, J. K., Gamez, M., & Choby, G. (2023). Recurrent Esthesioneuroblastoma: Long-Term Outcomes of Salvage Therapy. Cancers, 15(5), 1506. https://doi.org/10.3390/cancers15051506