

Applications of Machine Learning in Palliative Care: A Systematic Review
 , , , , , , and
, , , , , , and
Abstract
:Simple Summary
Abstract
1. Introduction
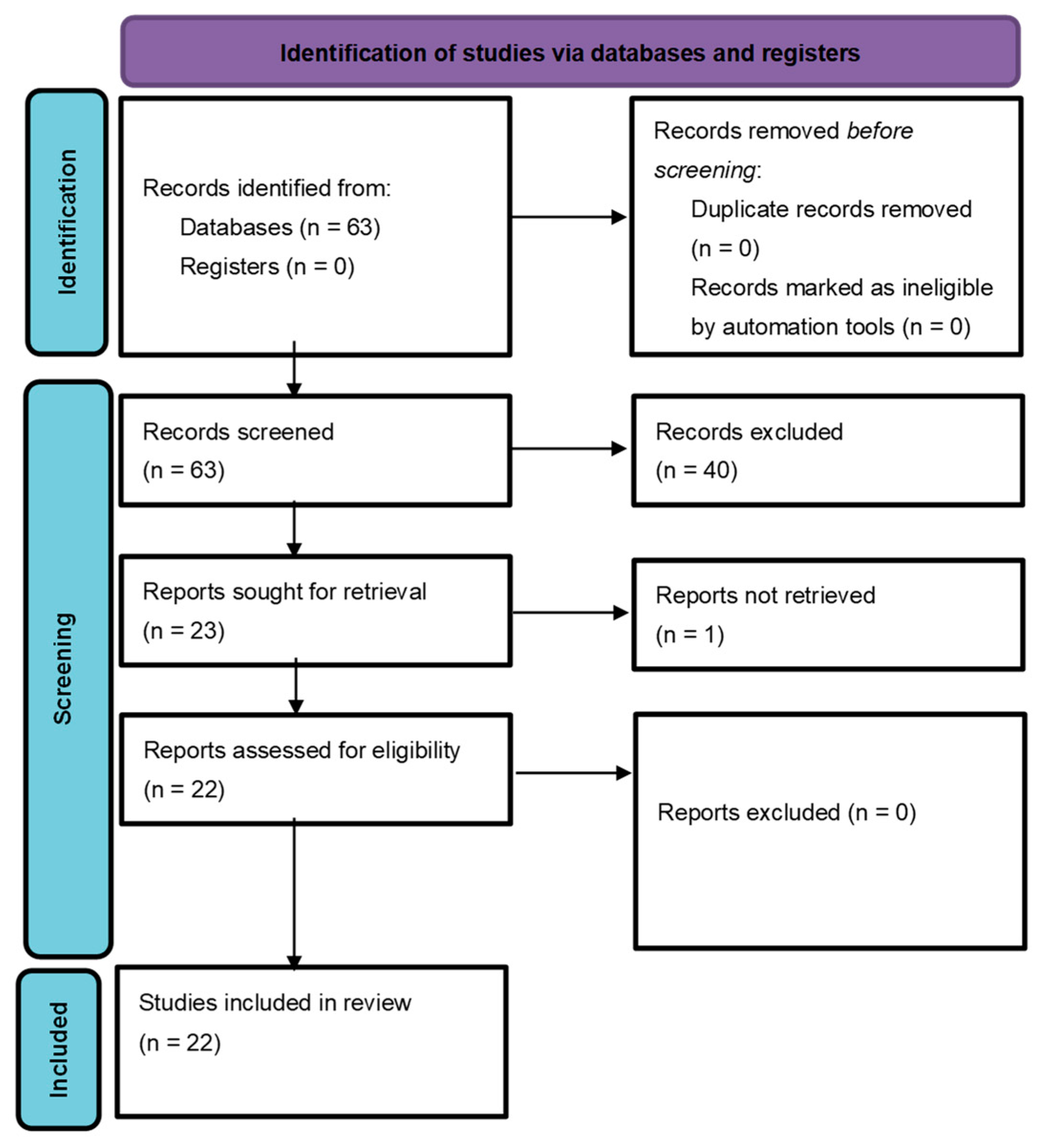
2. Methods
2.1. Literature Search
2.2. Data Extraction
- Study parameters: Title, authors, year of publication, recruitment period, number of patients in the respective sets, split, and design;
- Clinical parameters: Task, ground truth, and features that were used for prediction;
- ML parameters: Target metric, model, software, and hardware;
- Disclosures: Code availability, data availability, conflict of interest, and sources of funding.
3. Results
3.1. Disclosures and Declarations
3.2. Data and Code Availability
3.3. Machine Learning
3.4. Use Case: Machine Learning for Mortality Prediction
3.5. Use Case: Machine Learning to Support Data Annotation in Palliative Care Research
3.6. Use Case: Machine Learning for Predicting Morbidity under Palliative Therapy
3.7. Use Case: Machine Learning for Response Prediction for Palliative Therapy
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Esteva, A.; Robicquet, A.; Ramsundar, B.; Kuleshov, V.; DePristo, M.; Chou, K.; Cui, C.; Corrado, G.; Thrun, S.; Dean, J. A Guide to Deep Learning in Healthcare. Nat. Med. 2019, 25, 24–29. [Google Scholar] [CrossRef]
- Hosny, A.; Aerts, H.J.W.L. Artificial Intelligence for Global Health. Science 2019, 366, 955–956. [Google Scholar] [CrossRef] [PubMed]
- Windisch, P.; Hertler, C.; Blum, D.; Zwahlen, D.; Förster, R. Leveraging Advances in Artificial Intelligence to Improve the Quality and Timing of Palliative Care. Cancers 2020, 12, 1149. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Barash, Y.; Soffer, S.; Grossman, E.; Tau, N.; Sorin, V.; BenDavid, E.; Irony, A.; Konen, E.; Zimlichman, E.; Klang, E. Alerting on Mortality among Patients Discharged from the Emergency Department: A Machine Learning Model. Postgrad. Med. J. 2022, 98, 166–171. [Google Scholar] [CrossRef] [PubMed]
- Manz, C.R.; Chen, J.; Liu, M.; Chivers, C.; Regli, S.H.; Braun, J.; Draugelis, M.; Hanson, C.W.; Shulman, L.N.; Schuchter, L.M.; et al. Validation of a Machine Learning Algorithm to Predict 180-Day Mortality for Outpatients with Cancer. JAMA Oncol. 2020, 6, 1723–1730. [Google Scholar] [CrossRef] [PubMed]
- Avati, A.; Jung, K.; Harman, S.; Downing, L.; Ng, A.; Shah, N.H. Improving Palliative Care with Deep Learning. BMC Med. Inform. Decis. Mak. 2018, 18, 122. [Google Scholar] [CrossRef] [Green Version]
- Berg, G.D.; Gurley, V.F. Development and Validation of 15-Month Mortality Prediction Models: A Retrospective Observational Comparison of Machine-Learning Techniques in a National Sample of Medicare Recipients. BMJ Open 2019, 9, e022935. [Google Scholar] [CrossRef] [Green Version]
- Blanes-Selva, V.; Ruiz-García, V.; Tortajada, S.; Benedí, J.-M.; Valdivieso, B.; García-Gómez, J.M. Design of 1-Year Mortality Forecast at Hospital Admission: A Machine Learning Approach. Health Inform. J. 2021, 27, 1460458220987580. [Google Scholar] [CrossRef]
- Cary, M.P., Jr.; Zhuang, F.; Draelos, R.L.; Pan, W.; Amarasekara, S.; Douthit, B.J.; Kang, Y.; Colón-Emeric, C.S. Machine Learning Algorithms to Predict Mortality and Allocate Palliative Care for Older Patients with Hip Fracture. J. Am. Med. Dir. Assoc. 2021, 22, 291–296. [Google Scholar] [CrossRef]
- Durieux, B.N.; Gramling, C.J.; Manukyan, V.; Eppstein, M.J.; Rizzo, D.M.; Ross, L.M.; Ryan, A.G.; Niland, M.A.; Clarfeld, L.A.; Alexander, S.C.; et al. Identifying Connectional Silence in Palliative Care Consultations: A Tandem Machine-Learning and Human Coding Method. J. Palliat. Med. 2018, 21, 1755–1760. [Google Scholar] [CrossRef] [PubMed]
- Elfiky, A.A.; Pany, M.J.; Parikh, R.B.; Obermeyer, Z. Development and Application of a Machine Learning Approach to Assess Short-Term Mortality Risk Among Patients with Cancer Starting Chemotherapy. JAMA Netw. Open 2018, 1, e180926. [Google Scholar] [CrossRef] [Green Version]
- Elledge, C.R.; LaVigne, A.W.; Fiksel, J.; Wright, J.L.; McNutt, T.; Kleinberg, L.R.; Hu, C.; Smith, T.J.; Zeger, S.; DeWeese, T.L.; et al. External Validation of the Bone Metastases Ensemble Trees for Survival (BMETS) Machine Learning Model to Predict Survival in Patients with Symptomatic Bone Metastases. JCO Clin. Cancer Inform. 2021, 5, 304–314. [Google Scholar] [CrossRef]
- Forsyth, A.W.; Barzilay, R.; Hughes, K.S.; Lui, D.; Lorenz, K.A.; Enzinger, A.; Tulsky, J.A.; Lindvall, C. Machine Learning Methods to Extract Documentation of Breast Cancer Symptoms from Electronic Health Records. J. Pain Symptom Manag. 2018, 55, 1492–1499. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gensheimer, M.F.; Henry, A.S.; Wood, D.J.; Hastie, T.J.; Aggarwal, S.; Dudley, S.A.; Pradhan, P.; Banerjee, I.; Cho, E.; Ramchandran, K.; et al. Automated Survival Prediction in Metastatic Cancer Patients Using High-Dimensional Electronic Medical Record Data. J. Natl. Cancer Inst. 2019, 111, 568–574. [Google Scholar] [CrossRef]
- Goldstein, E.; Yeghiazaryan, K.; Ahmad, A.; Giordano, F.A.; Fröhlich, H.; Golubnitschaja, O. Optimal Multiparametric Set-up Modelled for Best Survival Outcomes in Palliative Treatment of Liver Malignancies: Unsupervised Machine Learning and 3 PM Recommendations. EPMA J. 2020, 11, 505–515. [Google Scholar] [CrossRef]
- Guo, W.; Gao, G.; Dai, J.; Sun, Q. Prediction of Lung Infection during Palliative Chemotherapy of Lung Cancer Based on Artificial Neural Network. Comput. Math. Methods Med. 2022, 2022, 4312117. [Google Scholar] [CrossRef]
- Heyman, E.T.; Ashfaq, A.; Khoshnood, A.; Ohlsson, M.; Ekelund, U.; Holmqvist, L.D.; Lingman, M. Improving Machine Learning 30-Day Mortality Prediction by Discounting Surprising Deaths. J. Emerg. Med. 2021, 61, 763–773. [Google Scholar] [CrossRef]
- Lee, R.Y.; Brumback, L.C.; Lober, W.B.; Sibley, J.; Nielsen, E.L.; Treece, P.D.; Kross, E.K.; Loggers, E.T.; Fausto, J.A.; Lindvall, C.; et al. Identifying Goals of Care Conversations in the Electronic Health Record Using Natural Language Processing and Machine Learning. J. Pain Symptom Manag. 2021, 61, 136–142.e2. [Google Scholar] [CrossRef] [PubMed]
- Lin, Y.-J.; Chen, R.-J.; Tang, J.-H.; Yu, C.-S.; Wu, J.L.; Chen, L.-C.; Chang, S.-S. Machine-Learning Monitoring System for Predicting Mortality Among Patients with Noncancer End-Stage Liver Disease: Retrospective Study. JMIR Med. Inform. 2020, 8, e24305. [Google Scholar] [CrossRef]
- Macieira, T.G.R.; Yao, Y.; Keenan, G.M. Use of Machine Learning to Transform Complex Standardized Nursing Care Plan Data into Meaningful Research Variables: A Palliative Care Exemplar. J. Am. Med. Inform. Assoc. 2021, 28, 2695–2701. [Google Scholar] [CrossRef]
- Manukyan, V.; Durieux, B.N.; Gramling, C.J.; Clarfeld, L.A.; Rizzo, D.M.; Eppstein, M.J.; Gramling, R. Automated Detection of Conversational Pauses from Audio Recordings of Serious Illness Conversations in Natural Hospital Settings. J. Palliat. Med. 2018, 21, 1724–1728. [Google Scholar] [CrossRef] [PubMed]
- Nieder, C.; Mannsåker, B.; Yobuta, R. Independent Validation of a Comprehensive Machine Learning Approach Predicting Survival After Radiotherapy for Bone Metastases. Anticancer Res. 2021, 41, 1471–1474. [Google Scholar] [CrossRef]
- van Helden, E.J.; Vacher, Y.J.L.; van Wieringen, W.N.; van Velden, F.H.P.; Verheul, H.M.W.; Hoekstra, O.S.; Boellaard, R.; Menke-van der Houven van Oordt, C.W. Radiomics Analysis of Pre-Treatment [18F]FDG PET/CT for Patients with Metastatic Colorectal Cancer Undergoing Palliative Systemic Treatment. Eur. J. Nucl. Med. Mol. Imaging 2018, 45, 2307–2317. [Google Scholar] [CrossRef] [Green Version]
- Wang, L.; Sha, L.; Lakin, J.R.; Bynum, J.; Bates, D.W.; Hong, P.; Zhou, L. Development and Validation of a Deep Learning Algorithm for Mortality Prediction in Selecting Patients with Dementia for Earlier Palliative Care Interventions. JAMA Netw. Open 2019, 2, e196972. [Google Scholar] [CrossRef]
- Yang, T.Y.; Kuo, P.-Y.; Huang, Y.; Lin, H.-W.; Malwade, S.; Lu, L.-S.; Tsai, L.-W.; Syed-Abdul, S.; Sun, C.-W.; Chiou, J.-F. Deep-Learning Approach to Predict Survival Outcomes Using Wearable Actigraphy Device Among End-Stage Cancer Patients. Front. Public Health 2021, 9, 730150. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.; Li, Y.; McConnell, W. Predicting Potential Palliative Care Beneficiaries for Health Plans: A Generalized Machine Learning Pipeline. J. Biomed. Inform. 2021, 123, 103922. [Google Scholar] [CrossRef] [PubMed]
- Parikh, R.B.; Manz, C.; Chivers, C.; Regli, S.H.; Braun, J.; Draugelis, M.E.; Schuchter, L.M.; Shulman, L.N.; Navathe, A.S.; Patel, M.S.; et al. Machine Learning Approaches to Predict 6-Month Mortality Among Patients with Cancer. JAMA Netw. Open 2019, 2, e1915997. [Google Scholar] [CrossRef] [Green Version]
- Alcorn, S.R.; Fiksel, J.; Wright, J.L.; Elledge, C.R.; Smith, T.J.; Perng, P.; Saleemi, S.; McNutt, T.R.; DeWeese, T.L.; Zeger, S. Developing an Improved Statistical Approach for Survival Estimation in Bone Metastases Management: The Bone Metastases Ensemble Trees for Survival (BMETS) Model. Int. J. Radiat. Oncol. Biol. Phys. 2020, 108, 554–563. [Google Scholar] [CrossRef]
- Lau, F.; Downing, G.M.; Lesperance, M.; Shaw, J.; Kuziemsky, C. Use of Palliative Performance Scale in End-of-Life Prognostication. J. Palliat. Med. 2006, 9, 1066–1075. [Google Scholar] [CrossRef] [PubMed]
- Pirovano, M.; Maltoni, M.; Nanni, O.; Marinari, M.; Indelli, M.; Zaninetta, G.; Petrella, V.; Barni, S.; Zecca, E.; Scarpi, E.; et al. A New Palliative Prognostic Score: A First Step for the Staging of Terminally Ill Cancer Patients. Italian Multicenter and Study Group on Palliative Care. J. Pain Symptom Manag. 1999, 17, 231–239. [Google Scholar] [CrossRef] [PubMed]
- Anota, A.; Hamidou, Z.; Paget-Bailly, S.; Chibaudel, B.; Bascoul-Mollevi, C.; Auquier, P.; Westeel, V.; Fiteni, F.; Borg, C.; Bonnetain, F. Time to Health-Related Quality of Life Score Deterioration as a Modality of Longitudinal Analysis for Health-Related Quality of Life Studies in Oncology: Do We Need RECIST for Quality of Life to Achieve Standardization? Qual. Life Res. 2015, 24, 5–18. [Google Scholar] [CrossRef] [Green Version]
- Temel, J.S.; Greer, J.A.; Muzikansky, A.; Gallagher, E.R.; Admane, S.; Jackson, V.A.; Dahlin, C.M.; Blinderman, C.D.; Jacobsen, J.; Pirl, W.F.; et al. Early Palliative Care for Patients with Metastatic Non-Small-Cell Lung Cancer. N. Engl. J. Med. 2010, 363, 733–742. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hui, D.; Mori, M.; Watanabe, S.M.; Caraceni, A.; Strasser, F.; Saarto, T.; Cherny, N.; Glare, P.; Kaasa, S.; Bruera, E. Referral Criteria for Outpatient Specialty Palliative Cancer Care: An International Consensus. Lancet Oncol. 2016, 17, e552–e559. [Google Scholar] [CrossRef] [Green Version]
- Lindvall, C.; Lilley, E.J.; Zupanc, S.N.; Chien, I.; Udelsman, B.V.; Walling, A.; Cooper, Z.; Tulsky, J.A. Natural Language Processing to Assess End-of-Life Quality Indicators in Cancer Patients Receiving Palliative Surgery. J. Palliat. Med. 2019, 22, 183–187. [Google Scholar] [CrossRef] [PubMed]
- Brizzi, K.; Zupanc, S.N.; Udelsman, B.V.; Tulsky, J.A.; Wright, A.A.; Poort, H.; Lindvall, C. Natural Language Processing to Assess Palliative Care and End-of-Life Process Measures in Patients with Breast Cancer with Leptomeningeal Disease. Am. J. Hosp. Palliat. Care 2020, 37, 371–376. [Google Scholar] [CrossRef]
- Windisch, P.; Koechli, C.; Rogers, S.; Schröder, C.; Förster, R.; Zwahlen, D.R.; Bodis, S. Machine Learning for the Detection and Segmentation of Benign Tumors of the Central Nervous System: A Systematic Review. Cancers 2022, 14, 2676. [Google Scholar] [CrossRef] [PubMed]
- Nelson, S.J.; Zeng, K.; Kilbourne, J.; Powell, T.; Moore, R. Normalized Names for Clinical Drugs: RxNorm at 6 Years. J. Am. Med. Inform. Assoc. 2011, 18, 441–448. [Google Scholar] [CrossRef] [Green Version]
- McDonald, C.J.; Huff, S.M.; Suico, J.G.; Hill, G.; Leavelle, D.; Aller, R.; Forrey, A.; Mercer, K.; DeMoor, G.; Hook, J.; et al. LOINC, a Universal Standard for Identifying Laboratory Observations: A 5-Year Update. Clin. Chem. 2003, 49, 624–633. [Google Scholar] [CrossRef] [Green Version]
- Bernstam, E.V.; Warner, J.L.; Krauss, J.C.; Ambinder, E.; Rubinstein, W.S.; Komatsoulis, G.; Miller, R.S.; Chen, J.L. Quantitating and Assessing Interoperability between Electronic Health Records. J. Am. Med. Inform. Assoc. 2022, 29, 753–760. [Google Scholar] [CrossRef]
- Scheibner, J.; Sleigh, J.; Ienca, M.; Vayena, E. Benefits, Challenges, and Contributors to Success for National eHealth Systems Implementation: A Scoping Review. J. Am. Med. Inform. Assoc. 2021, 28, 2039–2049. [Google Scholar] [CrossRef] [PubMed]
- Lehne, M.; Sass, J.; Essenwanger, A.; Schepers, J.; Thun, S. Why Digital Medicine Depends on Interoperability. NPJ Digit. Med. 2019, 2, 79. [Google Scholar] [CrossRef] [Green Version]
- Ellis, D.; Dvorak, J.; Hirschowitz, L.; Judge, M.; Kwiatkowski, A.; Srigley, J.; Washington, M.K.; Wells, M. The International Collaboration on Cancer Reporting (ICCR): Development of Evidence-Based Core Data Sets for Pathology Cancer Reporting. Pathology 2013, 45, S9. [Google Scholar] [CrossRef]
- Rubin, D.L.; Kahn, C.E., Jr. Common Data Elements in Radiology. Radiology 2017, 283, 837–844. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Title | Author | Year | Disease | Task |
|---|---|---|---|---|
| Improving palliative care with deep learning | Avati et al. [7] | 2018 | Disease agnostic | Predicting mortality within 3–12 months using EHR data from the previous 12 months |
| Development and validation of 15-month mortality prediction models: a retrospective observational comparison of machine-learning techniques in a national sample of Medicare recipients | Berg et al. [8] | 2019 | Disease agnostic | Predicting 15-month mortality among community-dwelling Medicare beneficiaries |
| Design of 1-year mortality forecast at hospital admission: A machine learning approach | Blanes-Selva et al. [9] | 2021 | Disease agnostic | Predicting 1-year mortality for patients admitted to a hospital |
| Machine Learning Algorithms to Predict Mortality and Allocate Palliative Care for Older Patients with Hip Fracture | Cary et al. [10] | 2021 | Hip fracture | Predicting 30-day and 1-year mortality for patients >65 years treated for hip fractures in inpatient rehabilitation facilities |
| Identifying Connectional Silence in Palliative Care Consultations: A Tandem Machine-Learning and Human Coding Method | Durieux et al. [11] | 2018 | Disease agnostic | Predicting conversational pauses in palliative care conversations so that human coders could classify the pauses as connectional or not |
| Development and Application of a Machine Learning Approach to Assess Short-term Mortality Risk Among Patients with Cancer Starting Chemotherapy | Elfiky et al. [12] | 2018 | Cancer | Predicting 30-day mortality of cancer patients undergoing chemotherapy |
| External Validation of the Bone Metastases Ensemble Trees for Survival (BMETS) Machine Learning Model to Predict Survival in Patients with Symptomatic Bone Metastases | Elledge et al. [13] | 2021 | Cancer | Predicting survival in patients receiving palliative radiation for symptomatic bone metastases |
| Machine Learning Methods to Extract Documentation of Breast Cancer Symptoms from Electronic Health Records | Forsyth et al. [14] | 2018 | Breast cancer | Extracting patient-reported symptoms from free-text health records of breast cancer patients receiving chemotherapy |
| Automated Survival Prediction in Metastatic Cancer Patients Using High-Dimensional Electronic Medical Record Data | Gensheimer et al. [15] | 2019 | Metastatic cancer | Predicting survival from date of first visit after metastatic cancer diagnosis |
| Optimal multiparametric set-up modelled for best survival outcomes in palliative treatment of liver malignancies: unsupervised machine learning and 3 PM recommendations | Goldstein et al. [16] | 2020 | Primary and secondary liver malignancies | Clustering patients with liver malignancies according to their survival probability |
| Prediction of Lung Infection during Palliative Chemotherapy of Lung Cancer Based on Artificial Neural Network | Guo, Gao et al. [17] | 2022 | Advanced lung cancer | Predicting lung infections in lung cancer patients undergoing palliative chemotherapy |
| Improving Machine Learning 30-Day Mortality Prediction by Discounting Surprising Deaths | Heyman et al. [18] | 2021 | Disease agnostic | Predicting 30-day mortality upon emergency department discharge |
| Identifying Goals of Care Conversations in the Electronic Health Record Using Natural Language Processing and Machine Learning | Lee et al. [19] | 2020 | Disease agnostic | Identifying goals of care conversation in notes in the electronic health records of patients with a critical illness and/or receiving palliative care |
| Machine-Learning Monitoring System for Predicting Mortality Among Patients with Noncancer End-Stage Liver Disease: Retrospective Study | Lin et al. [20] | 2020 | Non-cancer end-stage liver disease | Predicting survival in patients with non-cancer end-stage liver disease |
| Use of machine learning to transform complex standardized nursing care plan data into meaningful research variables: a palliative care exemplar | Macieira et al. [21] | 2021 | Disease agnostic | Classifying DIOs (groups of diagnosis, intervention and outcome) into a palliative care framework for hospitalized patients receiving palliative care |
| Automated Detection of Conversational Pauses from Audio Recordings of Serious Illness Conversations in Natural Hospital Settings | Manukyan et al. [22] | 2018 | Disease agnostic | Predicting conversational pauses in palliative care conversations so that human coders could classify the pauses as connectional or not |
| Validation of a Machine Learning Algorithm to Predict 180-Day Mortality for Outpatients with Cancer | Manz et al. [6] | 2020 | Cancer | Predicting 180-day mortality in an outpatient oncology cohort |
| Independent Validation of a Comprehensive Machine Learning Approach Predicting Survival After Radiotherapy for Bone Metastases | Nieder et al. [23] | 2021 | Cancer | Predicting survival in patients receiving palliative radiation for symptomatic bone metastases |
| Radiomics analysis of pre-treatment [18F]FDG PET/CT for patients with metastatic colorectal cancer undergoing palliative systemic treatment | Van Helden et al. [24] | 2018 | Metastatic colorectal cancer | Predicting response in patients with metastatic colorectal cancer receiving 1st- or 3rd-line palliative chemotherapy |
| Development and Validation of a Deep Learning Algorithm for Mortality Prediction in Selecting Patients with Dementia for Earlier Palliative Care Interventions | Wang et al. [25] | 2019 | Alzheimer’s disease and related dementias | Predicting 6-month, 1-year, and 2-year mortality in patients with Alzheimer’s disease and related dementias |
| Deep-Learning Approach to Predict Survival Outcomes Using Wearable Actigraphy Device Among End-Stage Cancer Patients | Yang et al. [26] | 2021 | End-stage cancer | Predicting in-hospital death of end-stage cancer patients on a hospice care unit using wristband actigraphy |
| Predicting potential palliative care beneficiaries for health plans: A generalized machine learning pipeline | Zhang et al. [27] | 2021 | 12 chronic health conditions | Predicting 1-year mortality in people with certain chronic health conditions from the general population |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vu, E.; Steinmann, N.; Schröder, C.; Förster, R.; Aebersold, D.M.; Eychmüller, S.; Cihoric, N.; Hertler, C.; Windisch, P.; Zwahlen, D.R. Applications of Machine Learning in Palliative Care: A Systematic Review. Cancers 2023, 15, 1596. https://doi.org/10.3390/cancers15051596
Vu E, Steinmann N, Schröder C, Förster R, Aebersold DM, Eychmüller S, Cihoric N, Hertler C, Windisch P, Zwahlen DR. Applications of Machine Learning in Palliative Care: A Systematic Review. Cancers. 2023; 15(5):1596. https://doi.org/10.3390/cancers15051596
Chicago/Turabian StyleVu, Erwin, Nina Steinmann, Christina Schröder, Robert Förster, Daniel M. Aebersold, Steffen Eychmüller, Nikola Cihoric, Caroline Hertler, Paul Windisch, and Daniel R. Zwahlen. 2023. "Applications of Machine Learning in Palliative Care: A Systematic Review" Cancers 15, no. 5: 1596. https://doi.org/10.3390/cancers15051596
APA StyleVu, E., Steinmann, N., Schröder, C., Förster, R., Aebersold, D. M., Eychmüller, S., Cihoric, N., Hertler, C., Windisch, P., & Zwahlen, D. R. (2023). Applications of Machine Learning in Palliative Care: A Systematic Review. Cancers, 15(5), 1596. https://doi.org/10.3390/cancers15051596