
Preoperative Predictors of Neoplasia in Patients Undergoing Small Bowel Resection for Complicated Crohn’s Disease: A Multicentre Case-Control Study

 , ,
, , 
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Patients
2.2. Data Collection
2.3. Radiological Assessments
2.4. Outcomes
2.5. Statistical Analysis
2.6. Ethical Concerns
3. Results
3.1. Patient Characteristics
3.2. Surgical Procedure
3.3. Cross-Sectional Imaging
3.4. SBN Characteristics
3.5. Risk Factors of SBN
3.6. SBA Characteristics and Risk Factors for SBA
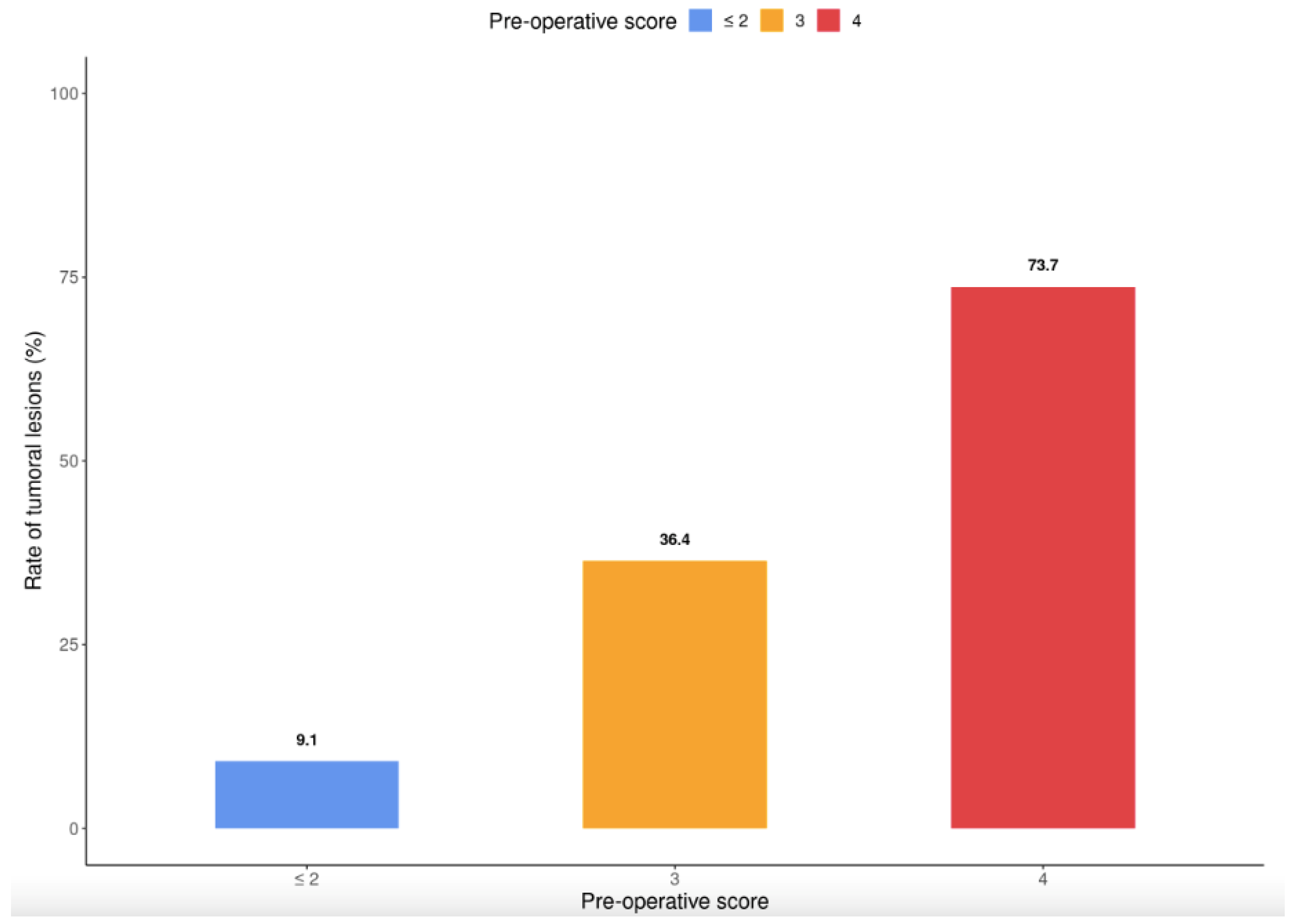
3.7. Development of a Score for Predicting the Presence of SBA
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ng, S.C.; Bernstein, C.N.; Vatn, M.H.; Lakatos, P.L.; Loftus, E.V.; Tysk, C.; O’Morain, C.; Moum, B.; Colombel, J.F. Geographical variability and environmental risk factors in inflammatory bowel disease. Gut 2013, 62, 630–649. [Google Scholar] [CrossRef] [PubMed]
- Beaugerie, L.; Svrcek, M.; Seksik, P.; Bouvier, A.M.; Simon, T.; Allez, M.; Brixi, H.; Gornet, J.M.; Altwegg, R.; Beau, P.; et al. Risk of Colorectal High-Grade Dysplasia and Cancer in a Prospective Observational Cohort of Patients with Inflammatory Bowel Disease. Gastroenterology 2013, 145, 166–175.e8. Available online: https://linkinghub.elsevier.com/retrieve/pii/S0016508513004587 (accessed on 8 December 2021). [CrossRef] [PubMed]
- Jess, T.; Loftus, E.V., Jr.; Velayos, F.S.; Harmsen, W.S.; Zinsmeister, A.R.; Smyrk, T.C.; Schleck, C.D.; Tremaine, W.J.; Melton, L.J., III; Munkholm, P.; et al. Risk of Intestinal Cancer in Inflammatory Bowel Disease: A Population-Based Study from Olmsted County, Minnesota. Gastroenterology 2006, 130, 1039–1046. Available online: https://linkinghub.elsevier.com/retrieve/pii/S0016508505025862 (accessed on 8 December 2021). [CrossRef] [PubMed]
- Aparicio, T.; Henriques, J.; Manfredi, S.; Tougeron, D.; Bouché, O.; Pezet, D.; Piessen, G.; Coriat, R.; Zaanan, A.; Legoux, J.L.; et al. Small bowel adenocarcinoma: Results from a nationwide prospective ARCAD-NADEGE cohort study of 347 patients. Int. J. Cancer 2020, 14, 967–977. [Google Scholar] [CrossRef]
- Aparicio, T.; Zaanan, A.; Svrcek, M.; Laurent-Puig, P.; Carrere, N.; Manfredi, S.; Locher, C.; Afchain, P. Small bowel adenocarcinoma: Epidemiology, risk factors, diagnosis and treatment. Dig. Liver Dis. 2014, 46, 97–104. Available online: https://linkinghub.elsevier.com/retrieve/pii/S1590865813001849 (accessed on 8 December 2021). [CrossRef] [Green Version]
- Axelrad, J.E.; Olen, O.; Sachs, M.C.; Erichsen, R.; Pedersen, L.; Halfvarson, J.; Askling, J.; Ekbom, A.; Sørensen, H.T.; Ludvigsson, J.F. Inflammatory bowel disease and risk of small bowel cancer: A binational population-based cohort study from Denmark and Sweden. Gut 2020, 70, 297–308. [Google Scholar] [CrossRef] [PubMed]
- Elriz, K.; Carrat, F.; Carbonnel, F.; Marthey, L.; Bouvier, A.M.; Beaugerie, L. Incidence, Presentation, and Prognosis of Small Bowel Adenocarcinoma in Patients with Small Bowel Crohn’s Disease: A Prospective Observational Study. Inflamm. Bowel. Dis. 2013, 19, 1823–1826. Available online: https://academic.oup.com/ibdjournal/article/19/9/1823-1826/4608893 (accessed on 8 December 2021).
- Beaugerie, L.; Brousse, N.; Bouvier, A.M.; Colombel, J.F.; Lémann, M.; Cosnes, J.; Hébuterne, X.; Cortot, A.; Bouhnik, Y.; Gendre, J.P.; et al. Lymphoproliferative disorders in patients receiving thiopurines for inflammatory bowel disease: A prospective observational cohort study. Lancet 2009, 374, 1617–1625. Available online: https://linkinghub.elsevier.com/retrieve/pii/S0140673609613027 (accessed on 8 December 2021). [CrossRef]
- Kotlyar, D.S.; Lewis, J.D.; Beaugerie, L.; Tierney, A.; Brensinger, C.M.; Gisbert, J.P.; Loftus, E.V., Jr.; Peyrin-Biroulet, L.; Blonski, W.C.; Van Domselaar, M.; et al. Risk of Lymphoma in Patients with Inflammatory Bowel Disease Treated with Azathioprine and 6-Mercaptopurine: A Meta-analysis. Clin. Gastroenterol. Hepatol. 2015, 13, 847–858.e4. Available online: https://linkinghub.elsevier.com/retrieve/pii/S1542356514007678 (accessed on 8 December 2021). [CrossRef]
- Lemaitre, M.; Kirchgesner, J.; Rudnichi, A.; Carrat, F.; Zureik, M.; Carbonnel, F.; Dray-Spira, R. Association Between Use of Thiopurines or Tumor Necrosis Factor Antagonists Alone or in Combination and Risk of Lymphoma in Patients with Inflammatory Bowel Disease. JAMA 2017, 318, 1679. [Google Scholar] [CrossRef]
- Kumar, S.; Fend, F.; Quintanilla-Martinez, L.; Kingma, D.W.; Sorbara, L.; Raffeld, M.; Banks, P.M.; Jaffe, E.S. Epstein-Barr Virus–Positive Primary Gastrointestinal Hodgkin’s Disease: Association with Inflammatory Bowel Disease and Immunosuppression. Am. J. Surg. Pathol. 2000, 24, 66. Available online: http://journals.lww.com/00000478-200001000-00008 (accessed on 8 December 2021). [CrossRef] [PubMed]
- Muller, M.; Broséus, J.; Feugier, P.; Thieblemont, C.; Beaugerie, L.; Danese, S.; Arnone, D.; Ndiaye, N.C.; Kokten, T.; Houlgatte, R.; et al. Characteristics of Lymphoma in Patients with Inflammatory Bowel Disease: A Systematic Review. J. Crohns Colitis 2021, 15, 827–839. Available online: https://academic.oup.com/ecco-jcc/article/15/5/827/5908884 (accessed on 8 December 2021). [CrossRef] [PubMed]
- Sokol, H.; Beaugerie, L.; Maynadié, M.; Laharie, D.; Dupas, J.L.; Flourié, B.; Lerebours, E.; Peyrin-Biroulet, L.; Allez, M.; Simon, T.; et al. Excess primary intestinal lymphoproliferative disorders in patients with inflammatory bowel disease. Inflamm. Bowel. Dis. 2012, 18, 2063–2071. Available online: https://academic.oup.com/ibdjournal/article/18/11/2063-2071/4608933 (accessed on 8 December 2021). [CrossRef] [PubMed]
- Simon, M.; Cosnes, J.; Gornet, J.M.; Seksik, P.; Stefanescu, C.; Blain, A.; Pariente, B.; Nancey, S.; Vuitton, L.; Nachury, M.; et al. Endoscopic Detection of Small Bowel Dysplasia and Adenocarcinoma in Crohn’s Disease: A Prospective Cohort-Study in High-Risk Patients. J. Crohns Colitis 2017, 11, 47–52. [Google Scholar] [CrossRef] [Green Version]
- Palascak-Juif, V.; Bouvier, A.M.; Cosnes, J.; Flourié, B.; Bouché, O.; Cadiot, G.; Lémann, M.; Bonaz, B.; Denet, C.; Marteau, P.; et al. Small Bowel Adenocarcinoma in Patients with Crohnʼs Disease Compared with Small Bowel Adenocarcinoma de Novo. Inflamm. Bowel. Dis. 2005, 11, 828–832. Available online: https://academic.oup.com/ibdjournal/article/11/9/828-832/4685908 (accessed on 8 December 2021). [CrossRef]
- Holubar, S.D.; Dozois, E.J.; Loftus, E.V., Jr.; Teh, S.H.; Benavente, L.A.; Harmsen, S.W.; Wolff, B.G.; Cima, R.R.; Larson, D.W. Primary intestinal lymphoma in patients with inflammatory bowel disease: A descriptive series from the prebiologic therapy era. Inflamm. Bowel. Dis. 2011, 17, 1557–1563. Available online: https://academic.oup.com/ibdjournal/article/17/7/1557-1563/4633566 (accessed on 8 December 2021). [CrossRef] [PubMed]
- Soyer, P.; Hristova, L.; Boudghène, F.; Hoeffel, C.; Dray, X.; Laurent, V.; Fishman, E.K.; Boudiaf, M. Small bowel adenocarcinoma in Crohn disease: CT-enterography features with pathological correlation. Abdom. Imaging 2012, 37, 338–349. [Google Scholar] [CrossRef]
- Van Assche, G.; Dignass, A.; Panes, J.; Beaugerie, L.; Karagiannis, J.; Allez, M.; Ochsenkühn, T.; Orchard, T.; Rogler, G.; Louis, E.; et al. The second European evidence-based Consensus on the diagnosis and management of Crohn’s disease: Definitions and diagnosis. J. Crohns Colitis 2010, 4, 7–27. Available online: https://academic.oup.com/ecco-jcc/article/4/1/7/402141 (accessed on 8 December 2021). [CrossRef] [Green Version]
- Silverberg, M.S.; Satsangi, J.; Ahmad, T.; Arnott, I.D.; Bernstein, C.N.; Brant, S.R.; Caprilli, R.; Colombel, J.F.; Gasche, C.; Geboes, K.; et al. Toward an Integrated Clinical, Molecular and Serological Classification of Inflammatory Bowel Disease. Rep. A Work. Party 2005, 19 (Suppl. SA), 5A–36A. Available online: https://www.hindawi.com/journals/cjgh/2005/269076/abs/ (accessed on 8 December 2021).
- Sobin, L.H.; Gospodarowicz, M.K. TNM Classification of Malignant Tumours, 7th ed.; Wiley Blackwell: Hoboken, NJ, USA, 2010. [Google Scholar]
- Panes, J.; Bouhnik, Y.; Reinisch, W.; Stoker, J.; Taylor, S.A.; Baumgart, D.C.; Danese, S.; Halligan, S.; Marincek, B.; Matos, C.; et al. Imaging techniques for assessment of inflammatory bowel disease: Joint ECCO and ESGAR evidence-based consensus guidelines. J. Crohns Colitis 2013, 7, 556–585. Available online: https://academic.oup.com/ecco-jcc/article/7/7/556/406563 (accessed on 8 December 2021). [CrossRef] [Green Version]
- Teefey, S.A.; Roarke, M.C.; Brink, J.A.; Middleton, W.D.; Balfe, D.M.; Thyssen, E.P.; Hildebolt, C.F. Bowel wall thickening: Differentiation of inflammation from ischemia with color Doppler duplex. U.S. Radiol. 1996, 198, 547–551. [Google Scholar] [CrossRef] [PubMed]
- Cahill, C. Small bowel adenocarcinoma and Crohn’s disease: Any further ahead than 50 years ago? World J. Gastroenterol. 2014, 20, 11486. Available online: http://www.wjgnet.com/1007-9327/full/v20/i33/11486.htm (accessed on 8 December 2021). [CrossRef] [PubMed]
- Jaskowiak, N.T.; Michelassi, F. Adenocarcinoma at a strictureplasty site in Crohn’s disease: Report of a case. Dis. Colon. Rectum. 2001, 44, 284–287. Available online: https://journals.lww.com/00003453-200144020-00020 (accessed on 8 December 2021). [CrossRef] [PubMed]
- Piton, G.; Cosnes, J.; Monnet, E.; Beaugerie, L.; Seksik, P.; Savoye, G.; Cadiot, G.; Flourie, B.; Capelle, P.; Marteau, P.; et al. Risk Factors Associated with Small Bowel Adenocarcinoma in Crohn’s Disease: A CaseControl Study. Am. J. Gastroenterol. 2008, 103, 1730–1736. Available online: http://www.nature.com/doifinder/10.1111/j.1572-0241.2008.01847.x (accessed on 8 December 2021). [CrossRef]
- Solem, C.A.; Harmsen, W.S.; Zinsmeister, A.R.; Loftus, E.V. Small Intestinal Adenocarcinoma in Crohn’s Disease. Inflamm. Bowel. Dis. 2004, 10, 4. [Google Scholar] [CrossRef]
- Wieghard, N.; Mongoue-Tchokote, S.; Young, J.I.; Sheppard, B.C.; Tsikitis, V.L. Prognosis of small bowel adenocarcinoma in Crohn’s disease compares favourably with de novo small bowel adenocarcinoma. Color. Dis. 2017, 19, 446–455. [Google Scholar] [CrossRef]
- Grolleau, C.; Pote, N.M.; Guedj, N.S.; Zappa, M.; Theou-Anton, N.; Bouhnik, Y.; Panis, Y.; Cazals-Hatem, D.L. Small bowel adenocarcinoma complicating Crohn’s disease: A single-centre experience emphasizing the importance of screening for dysplasia. Virchows Arch. 2017, 471, 611–617. Available online: http://link.springer.com/10.1007/s00428-017-2125-z (accessed on 8 December 2021). [CrossRef]
- Bojesen, R.D.; Riis, L.B.; Høgdall, E.; Nielsen, O.H.; Jess, T. Inflammatory Bowel Disease and Small Bowel Cancer Risk, Clinical Characteristics, and Histopathology: A Population-Based Study. Clin. Gastroenterol. Hepatol. 2017, 15, 1900–1907.e2. Available online: https://linkinghub.elsevier.com/retrieve/pii/S1542356517307991 (accessed on 8 December 2021). [CrossRef]
- Schottenfeld, D.; Beebe-Dimmer, J.L.; Vigneau, F.D. The Epidemiology and Pathogenesis of Neoplasia in the Small Intestine. Ann. Epidemiol. 2009, 19, 58–69. Available online: https://linkinghub.elsevier.com/retrieve/pii/S1047279708003207 (accessed on 8 December 2021). [CrossRef] [Green Version]
- Svrcek, M.; Piton, G.; Cosnes, J.; Beaugerie, L.; Vermeire, S.; Geboes, K.; Lemoine, A.; Cervera, P.; El-Murr, N.; Dumont, S.; et al. Small Bowel Adenocarcinomas Complicating Crohnʼs Disease Are Associated with Dysplasia: A Pathological and Molecular Study. Inflamm. Bowel. Dis. 2014, 20, 1584–1592. Available online: https://academic.oup.com/ibdjournal/article/20/9/1584-1592/4579170 (accessed on 8 December 2021). [CrossRef]
- Hussain, T.; Jeganathan, N.A.; Karagkounis, G.; Stocchi, L.; Shawki, S.; Holubar, S.D.; Gordon, I.; Hull, T.; Liska, D. Small bowel adenocarcinoma in Crohn’s disease: A rare but devastating complication. Tech. Coloproctol. 2020, 24, 1055–1062. Available online: https://link.springer.com/10.1007/s10151-020-02269-8 (accessed on 8 December 2021). [CrossRef] [PubMed]
- Chin, Y.H.; Jain, S.R.; Lee, M.H.; Ng, C.H.; Lin, S.Y.; Mai, A.S.; Muthiah, M.D.; Foo, F.J.; Sundar, R.; Ong, D.E.H.; et al. Small bowel adenocarcinoma in Crohn’s disease: A systematic review and meta-analysis of the prevalence, manifestation, histopathology, and outcomes. Int. J. Colorectal. Dis. 2021, 37, 239–250. [Google Scholar] [CrossRef] [PubMed]
- Weber, N.K.; Fletcher, J.G.; Fidler, J.L.; Barlow, J.M.; Pruthi, S.; Loftus, E.V.; Pardi, D.S.; Smyrk, T.C.; Becker, B.D.; Pasha, S.F.; et al. Clinical characteristics and imaging features of small bowel adenocarcinomas in Crohn’s disease. Abdom. Imaging 2015, 40, 1060–1067. [Google Scholar] [CrossRef] [PubMed]
- Liu, Z.; Liu, K.; Gao, J.; Jing, C.; Ma, Y.; Zheng, S.; Shan, J. Prognostic Value of Lymph Node Evaluation in Stage II Small Bowel Adenocarcinoma: An Updated Analysis of Surveillance, Epidemiology, and End Results Database. Front. Oncol. 2022, 12, 865745. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8989959/ (accessed on 29 December 2022). [CrossRef] [PubMed]
- Overman, M.J.; Hu, C.Y.; Wolff, R.A.; Chang, G.J. Prognostic value of lymph node evaluation in small bowel adenocarcinoma: Analysis of the surveillance, epidemiology, and end results database. Cancer 2010, 116, 5374–5382. Available online: https://onlinelibrary.wiley.com/doi/10.1002/cncr.25324 (accessed on 8 December 2021). [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Overall, n = 200 | Case, n = 50 | Control, n = 150 | p | |
|---|---|---|---|---|
| Female sex, n (%) | 95 (48%) | 20 (40%) | 75 (50%) | 0.2 |
| Median age, years (IQR) | 38.0 (28.0–50.0) | 50.5 (41.0–59.8) | 34.0 (26.2–42.8) | <0.001 |
| Body mass index, kg/m2 (IQR) | 20.7 (18.5–23.3) | 19.9 (18.5–22.8) | 20.9 (18.5–23.6) | 0.4 |
| Smoker, n (%) | 76 (39%) | 13 (28%) | 63 (43%) | 0.068 |
| Family history of IBD, n (%) | 18 (9.1%) | 8 (17%) | 10 (6.7%) | 0.042 |
| Median CD duration, years (IQR) | 8.5 (3.1–17.5) | 19.7 (6.2–27.8) | 7.5 (2.5–13.0) | <0.001 |
| Age at diagnosis (years) °, n (%) | 0.3 | |||
| - A1 (<17) | 18 (9.0%) | 4 (8.2%) | 14 (9.3%) | |
| - A2 (17–40) | 160 (80%) | 37 (76%) | 123 (82%) | |
| - A3 (>40) | 21 (11%) | 8 (16%) | 13 (8.7%) | |
| Disease location °, n (%) | 0.4 | |||
| - L1 (ileal disease) | 133 (66%) | 32 (64%) | 101 (67%) | |
| - L2 (colonic disease) | 1 (0.5%) | 1 (2.0%) | 0 (0%) | |
| - L3 (ileocolonic disease) | 59 (30%) | 15 (30%) | 44 (29%) | |
| - L4 (isolated upper disease) | 7 (3.5%) | 2 (4.0%) | 5 (3.3%) | |
| Behaviour °, n (%) | <0.001 | |||
| - B1 (non-stricturing and non-penetrating) | 5 (2.5%) | 5 (10%) | 0 (0%) | |
| - B2 (structuring) | 86 (43%) | 31 (62%) | 55 (37%) | |
| - B3 (penetrating) | 109 (55%) | 14 (28%) | 95 (63%) | |
| Perineal disease, n (%) | 54 (27%) | 12 (24%) | 42 (28%) | 0.6 |
| Extra-intestinal manifestation, n (%) | 34 (17%) | 13 (27%) | 21 (14%) | 0.036 |
| History of corticosteroid use, n (%) | 0.090 | |||
| Naive to corticoids, n (%) | 44 (23%) | 5 (10%) | 39 (27%) | |
| Corticosensibility, n (%) | 71 (36%) | 23 (48%) | 48 (33%) | |
| Corticosteroid dependence, n (%) | 37 (19%) | 8 (17%) | 29 (20%) | |
| Corticosteroid resistance, n (%) | 42 (22%) | 12 (25%) | 30 (20%) | |
| 5ASA use, n (%) | 16 (8.2%) | 3 (6.5%) | 13 (8.8%) | 0.8 |
| Immunosuppressant use, n (%) | 119 (60%) | 30 (61%) | 89 (60%) | 0.9 |
| Thiopurines use, n (%) | 37 (31%) | 10 (33%) | 27 (30%) | 0.7 |
| Methotrexate use, n (%) | 12 (10%) | 2 (7.1%) | 10 (11%) | 0.7 |
| Adalimumab use, n (%) | 22 (11%) | 3 (6.2%) | 19 (13%) | 0.2 |
| Infliximab use, n (%) | 37 (19%) | 8 (17%) | 29 (19%) | 0.7 |
| Vedolizumab use, n (%) | 2 (1.0%) | 0 (0%) | 2 (1.3%) | >0.9 |
| Ustekinumab use, n (%) | 6 (3.0%) | 4 (8.3%) | 2 (1.3%) | 0.032 |
| Previous surgery for IBD, n (%) | 62 (31%) | 14 (28%) | 48 (32%) | 0.6 |
| Previous stricturoplasty, n (%) | 5 (36%) | 2 (22%) | 3 (60%) | 0.3 |
| Surgical Characteristics | Overall, n = 200 | Case, n = 50 | Control, n = 150 | p |
|---|---|---|---|---|
| Indication for surgery, n (%) | 0.002 | |||
| - fistula | 38 (19%) | 9 (18%) | 29 (19%) | |
| - abscess | 46 (23%) | 4 (8.0%) | 42 (28%) | |
| - stricture | 103 (52%) | 31 (62%) | 72 (48%) | |
| - peritonitis | 8 (4.0%) | 2 (4.0%) | 6 (4.0%) | |
| - others | 5 (2.5%) | 4 (8.0%) | 1 (0.7%) | |
| Laboratory parameters at the time of surgery | ||||
| - haemoglobin, g/dL (IQR) | 12.6 (11.4–13.6) | 11.9 (11.0–13.4) | 12.8 (11.6–13.7) | 0.069 |
| - ferritin, μg/L (IQR) | 82.0 (33.0–160.0) | 76.0 (25.5–166.2) | 82.0 (36.5–160.0) | 0.6 |
| - albumin, g/L (IQR) | 34.0 (31.0–38.0) | 32.2 (27.4–35.0) | 34.0 (31.0–38.0) | 0.003 |
| - CRP, mg/L (IQR) | 17.0 (5.0–40.0) | 25.0 (6.5–63.0) | 14.0 (5.0–36.5) | 0.2 |
| Time between imaging and surgery, days (IQR) | 32.0 (10.2–84.8) | 44.0 (16.8–127.5) | 29.5 (10.0–78.0) | 0.090 |
| Oncological surgery, n (%) | 15 (7.5%) | 13 (26%) | 2 (1.3%) | <0.001 |
| Length of resection, cm (IQR) | 29.0 (20.0–40.0) | 31.0 (20.0–45.0) | 28.0 (19.0–38.0) | 0.2 |
| Stoma, n (%) | 66 (33%) | 22 (44%) | 44 (29%) | 0.056 |
| Number of nodes analysed, n (%) | 10.0 (2.00.0) | 17.5 (6.0–21.2) | 2.0 (1.0–6.0) | <0.001 |
| Laparoscopy, n (%) | 131 (66%) | 39 (80%) | 92 (62%) | 0.022 |
| Overall, n = 200 | Case, n = 50 | Control, n = 150 | p | |
|---|---|---|---|---|
| Presence of a stricture, n (%) | 189 (94%) | 46 (92%) | 143 (95%) | 0.5 |
| Maximum parietal wall thickness, mm (IQR) | 10.0 (8.0–12.0) | 11.0 (9.0–13.0) | 10.0 (7.0–12.0) | 0.013 |
| Presence of parietal reinforcement, n (%) | 184 (93%) | 40 (83%) | 144 (97%) | 0.004 |
| Presence of sub-mucosal parietal oedema, n (%) | 125 (63%) | 23 (46%) | 102 (68%) | 0.004 |
| Presence of adenopathy > 1 cm, n (%) | 55 (28%) | 14 (28%) | 41 (27%) | >0.9 |
| Presence of mesenteric fat infiltration, n (%) | 147 (74%) | 29 (58%) | 118 (79%) | 0.004 |
| Presence of tissue infiltration, n (%) | 45 (22%) | 17 (34%) | 28 (19%) | 0.025 |
| Stricture irregularity, n (%) | 47 (24%) | 19 (39%) | 28 (19%) | 0.006 |
| Multiple lesions, n (%) | 8 (4%) | 3 (6%) | 5 (3,3%) | 0.4 |
| Abscess, n (%) | 60 (30%) | 13 (26%) | 47 (32%) | 0.5 |
| Perforation, n (%) | 9 (4.5%) | 4 (8.0%) | 5 (3.3%) | 0.2 |
| Fistula, n (%) | 79 (40%) | 20 (40%) | 59 (39%) | >0.9 |
| Length of inflammatory involvement, cm (IQR) | 20.0 (11.0–30.0) | 20.0 (11.5–35.0) | 20.0 (11.0–30.0) | 0.3 |
| Upstream dilatation > 28 cm, n (%) | 112 (56%) | 33 (67%) | 79 (53%) | 0.072 |
| If MRI had been performed | ||||
| Parietal enhancement on final MRI, n (%) | 0.014 | |||
| - low | 2 (3.0%) | 2 (20%) | 0 (0%) | |
| - moderate | 38 (57%) | 6 (60%) | 32 (56%) | |
| - intense | 27 (40%) | 2 (20%) | 25 (44%) | |
| - stratified | 38 (57%) | 3 (30%) | 35 (61%) | 0.065 |
| If two successive examinations were performed | ||||
| Significant increase in size of adenopathy, n (%) | 2 (9.5%) | 2 (22%) | 0 (0%) | 0.2 |
| Increase in parietal thickening, n (%) | 6 (30%) | 3 (38%) | 3 (25%) | 0.6 |
| Change in mesenteric fat infiltration, n (%) | 9 (43%) | 4 (44%) | 5 (42%) | >0.9 |
| Modification of contrast uptake, n (%) | 3 (15%) | 2 (25%) | 1 (8.3%) | 0.5 |
| Upstream dilatation, n (%) | 7 (33%) | 3 (33%) | 4 (33%) | >0.9 |
| Score of 1–10 for radiological suspicion of cancer, n (IQR) | 2.0 (1.0–3.2) | 6.0 (3.0–8.0) | 2.0 (0.0–3.0) | <0.001 |
| Score > 5 for radiological suspicion of cancer, n (%) | 31(16%) | 26 (52%) | 5 (3.3%) | <0.001 |
| n = 50 | |
|---|---|
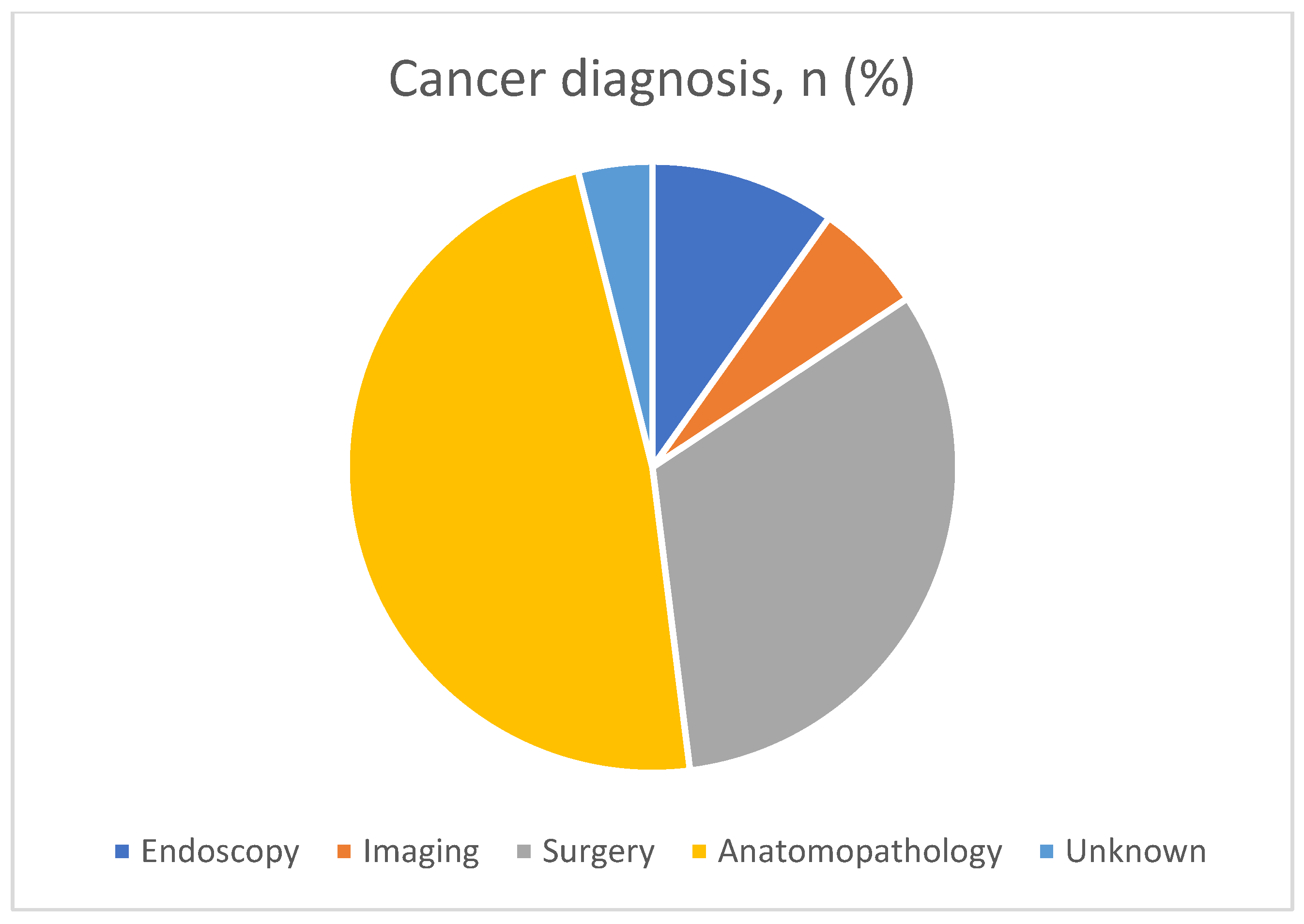
| Cancer diagnosis, n (%) | |
| - Endoscopy | 5 (10%) |
| - Imaging | 3 (6.1%) |
| - Surgery | 16 (33%) |
| - Anatomopathology | 24 (49%) |
| - unknown | 2 (4%) |
| Neoplasia location, n (%) | |
| - ileum | 44 (90%) |
| - jejunum | 3 (6.1%) |
| - duodenum | 1 (2.0%) |
| - unknown | 2 (4%) |
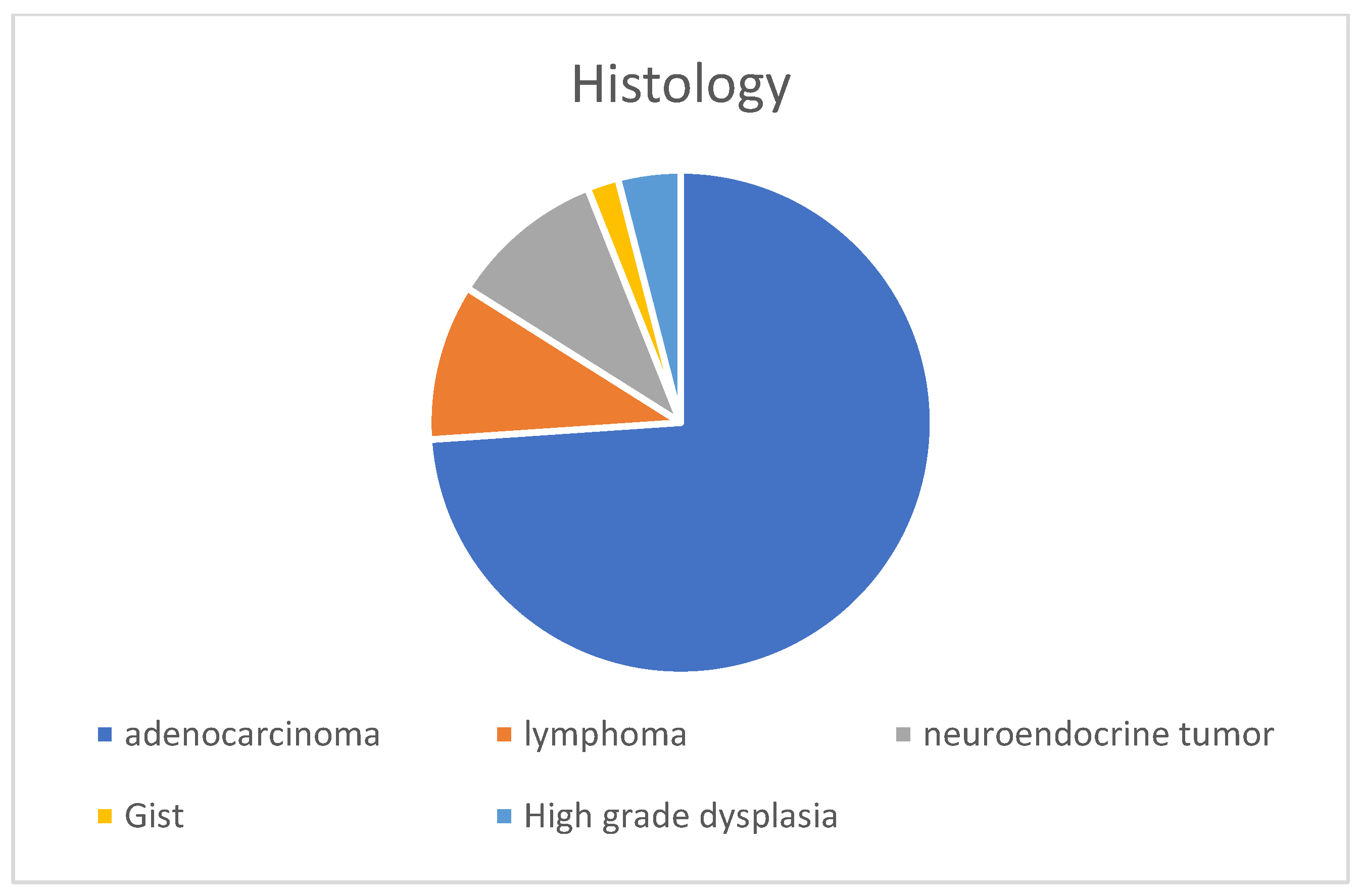
| Histology, n (%) | |
| - Adenocarcinoma | 35 (71%) |
| - Adenocarcinoma + neuroendocrine tumour | 1 (2.0%) |
| - Lymphoma | 5 (10%) |
| - Neuroendocrine tumour | 5 (10%) |
| - GIST | 1 (2.0%) |
| - High-grade dysplasia | 2 (4.1%) |
| Signet ring cells, n (%) | 13 (27%) |
| Family history of cancer, n (%) | 2 (4.5%) |
| Personal history of cancer, n (%) | 2 (4.1%) |
| EBV, n (%) | 0 (0%) |
| Differentiation of tumour, n (%) | |
| - well | 21 (55%) |
| - moderate | 14 (37%) |
| - low | 3 (7.9%) |
| TNM: T, n (%) | |
| - T1–2 | 7 (16.7%) |
| - T3–4 | 35 (83.3%) |
| TNM: N, n (%) | |
| - N0 | 27 (61%) |
| - N1–2 | 15 (34%) |
| - N3 | 2 (4.5%) |
| Metastasis (>M1), n (%) | 12 (27%) |
| Positive surgical margins [≥R1], n (%) | 10 (22%) |
| Microsatellite instability status, n (%) | 3 (8.6%) |
| Adjuvant chemotherapy, n (%) | 30 (65%) |
| Palliative chemotherapy, n (%) | 6 (13%) |
| Immunotherapy, n (%) | 2 (4.3%) |
| 0ncological surveillance, n(%) | 14 (31%) |
| Death, n (%) | 16 (32%) |
| Age at death, years (IQR) | 50.0 (41.0–61.2) |
| Characteristic | OR | 95% CI | p |
|---|---|---|---|
| Age ≥ 50 years | 28.0 | 5.05–206 | <0.001 |
| Indication for surgery: stricture | 5.84 | 1.27–35.4 | 0.034 |
| Median Crohn’s disease duration ≥ 17.5 years | 4.25 | 1.33–14.3 | 0.015 |
| Presence of mesenteric fat infiltration | 0.27 | 0.07–0.93 | 0.043 |
| Colonne1 | n = 36 |
|---|---|
| Diagnosis of neoplasia, n (%) | |
| - Endoscopy | 3 (8.3%) |
| - Imaging | 1 (2.8%) |
| - Surgery | 14 (39%) |
| - Anatomopathology | 17 (47%) |
| - unknown | 1 (2.8%) |
| Neoplasia location, n (%) | |
| - ileum | 33 (92%) |
| - jejunum | 2 (5.6%) |
| - duodenum | 1 (2.8%) |
| Signet ring cells, n (%) | 12 (33%) |
| Family history of cancer, n (%) | 2 (6.5%) |
| Personal history of cancer, n (%) | 0 (0%) |
| Tumour differentiation, n (%) | |
| - well | 15 (47%) |
| - moderate | 14 (44%) |
| - low | 3 (9.4%) |
| TNM: T, n (%) | |
| - T1–2 | 4 (11.1%) |
| - T3–4 | 32 (89%) |
| TNM: N, n (%) | |
| - N0 | 22 (61%) |
| - N1–2 | 12 (33%) |
| - N3 | 2 (5.6%) |
| Metastasis (>M1), n (%) | 11 (31%) |
| Positive surgical margins [≥R1], n (%) | 9 (26%) |
| Microsatellite instability status, n (%) | 3 (10%) |
| Treatment, n (%) | |
| - Revision surgery | 5 (14%) |
| - Adjuvant chemotherapy | 22 (69%) |
| - Palliative chemotherapy | 5 (16%) |
| - Immunotherapy, n (%) | 1 (3.1%) |
| - Oncological surveillance, n (%) | 8 (26%) |
| Death, n (%) | 16 (44%) |
| Age at death, years (IQR) | 50.0 (41.0–61.2) |
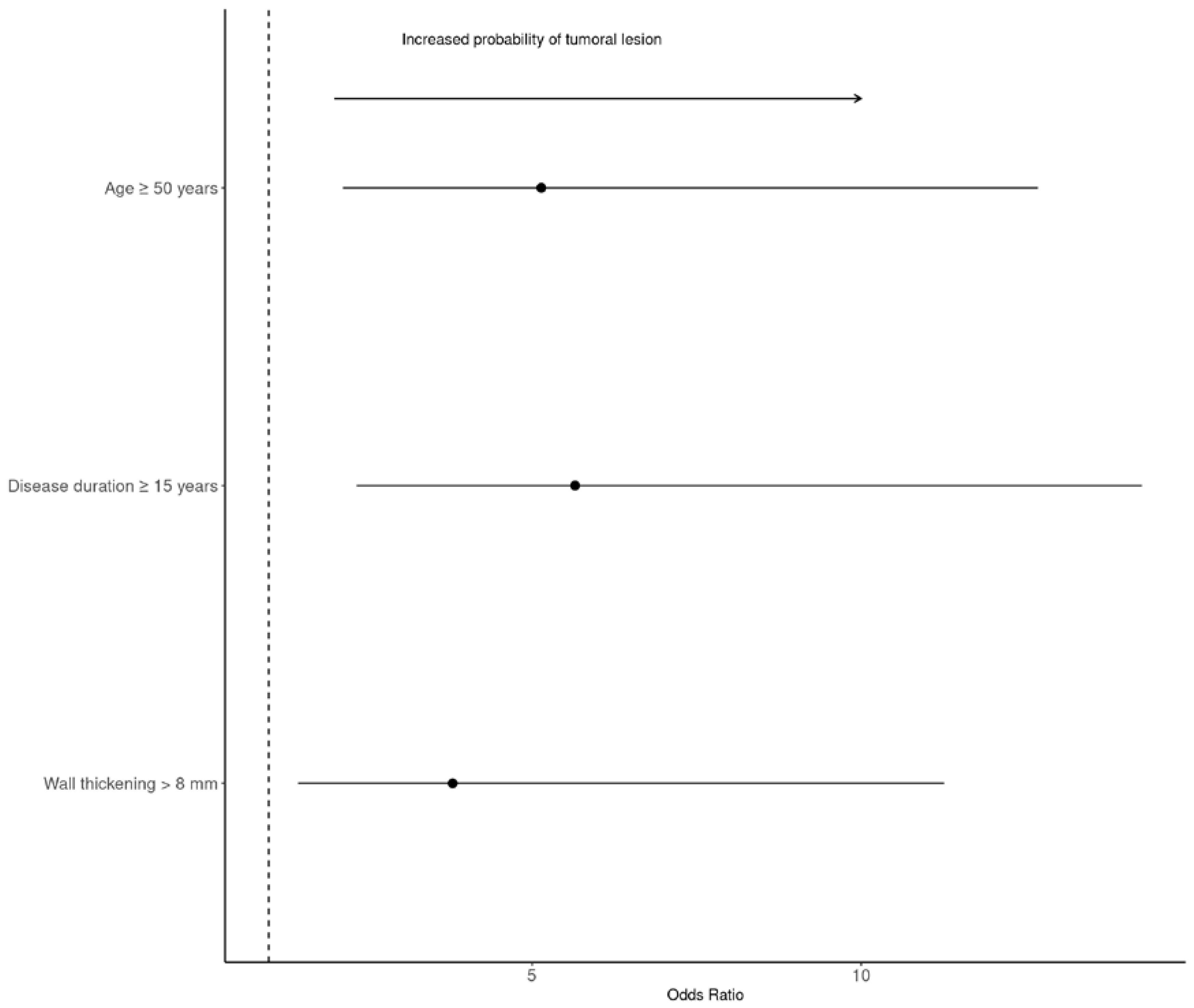
| Characteristic | OR | 95% CI | p |
|---|---|---|---|
| Age at the time of surgery ≥ 50 years | 5.14 | 2.12, 12.7 | <0.001 |
| Median Crohn’s disease duration ≥ 15 years | 5.65 | 2.33, 14.3 | <0.001 |
| Maximum parietal wall thickness > 8 mm | 3.79 | 1.45, 11.3 | 0.006 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chappe, C.; Salut, C.; Amiot, A.; Gaye, D.; Frulio, N.; Lapuyade, B.; Vuitton, L.; Altwegg, R.; Gilletta, C.; Fumery, M.; et al. Preoperative Predictors of Neoplasia in Patients Undergoing Small Bowel Resection for Complicated Crohn’s Disease: A Multicentre Case-Control Study. Cancers 2023, 15, 2004. https://doi.org/10.3390/cancers15072004
Chappe C, Salut C, Amiot A, Gaye D, Frulio N, Lapuyade B, Vuitton L, Altwegg R, Gilletta C, Fumery M, et al. Preoperative Predictors of Neoplasia in Patients Undergoing Small Bowel Resection for Complicated Crohn’s Disease: A Multicentre Case-Control Study. Cancers. 2023; 15(7):2004. https://doi.org/10.3390/cancers15072004
Chicago/Turabian StyleChappe, Capucine, Cecile Salut, Aurelien Amiot, Delphine Gaye, Nora Frulio, Bruno Lapuyade, Lucine Vuitton, Romain Altwegg, Cyrielle Gilletta, Mathurin Fumery, and et al. 2023. "Preoperative Predictors of Neoplasia in Patients Undergoing Small Bowel Resection for Complicated Crohn’s Disease: A Multicentre Case-Control Study" Cancers 15, no. 7: 2004. https://doi.org/10.3390/cancers15072004
APA StyleChappe, C., Salut, C., Amiot, A., Gaye, D., Frulio, N., Lapuyade, B., Vuitton, L., Altwegg, R., Gilletta, C., Fumery, M., Bouguen, G., Serrero, M., Nachury, M., de Suray, N., Caillo, L., Simon, M., Laharie, D., Rivière, P., & Poullenot, F. (2023). Preoperative Predictors of Neoplasia in Patients Undergoing Small Bowel Resection for Complicated Crohn’s Disease: A Multicentre Case-Control Study. Cancers, 15(7), 2004. https://doi.org/10.3390/cancers15072004