

Ultrasound for Breast Cancer Screening in Resource-Limited Settings: Current Practice and Future Directions

Abstract
:Simple Summary
Abstract
1. Introduction
2. Main BC Screening Tools
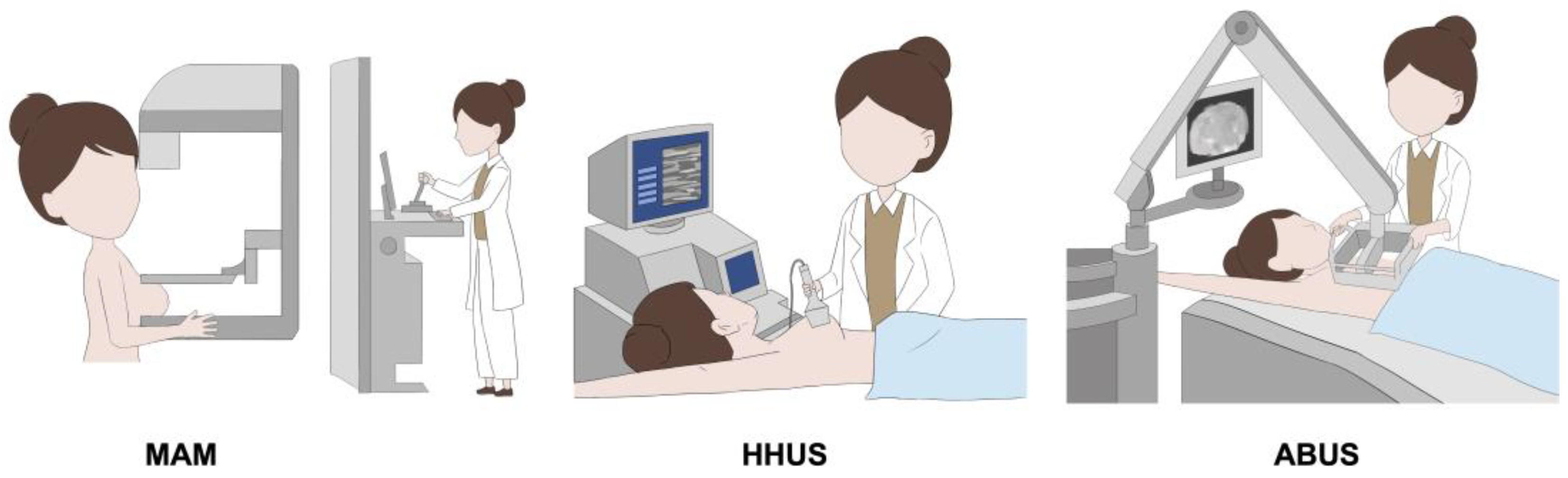
2.1. MAM, HHUS, and ABUS
2.2. Diagnostic Performance Comparison between MAM and US
2.3. US as a Primary Tool in BC Screening
2.4. ABUS in BC Screening
3. Novel Techniques in US for BC Screening
3.1. Computer-Aided Detection (CAD) in ABUS
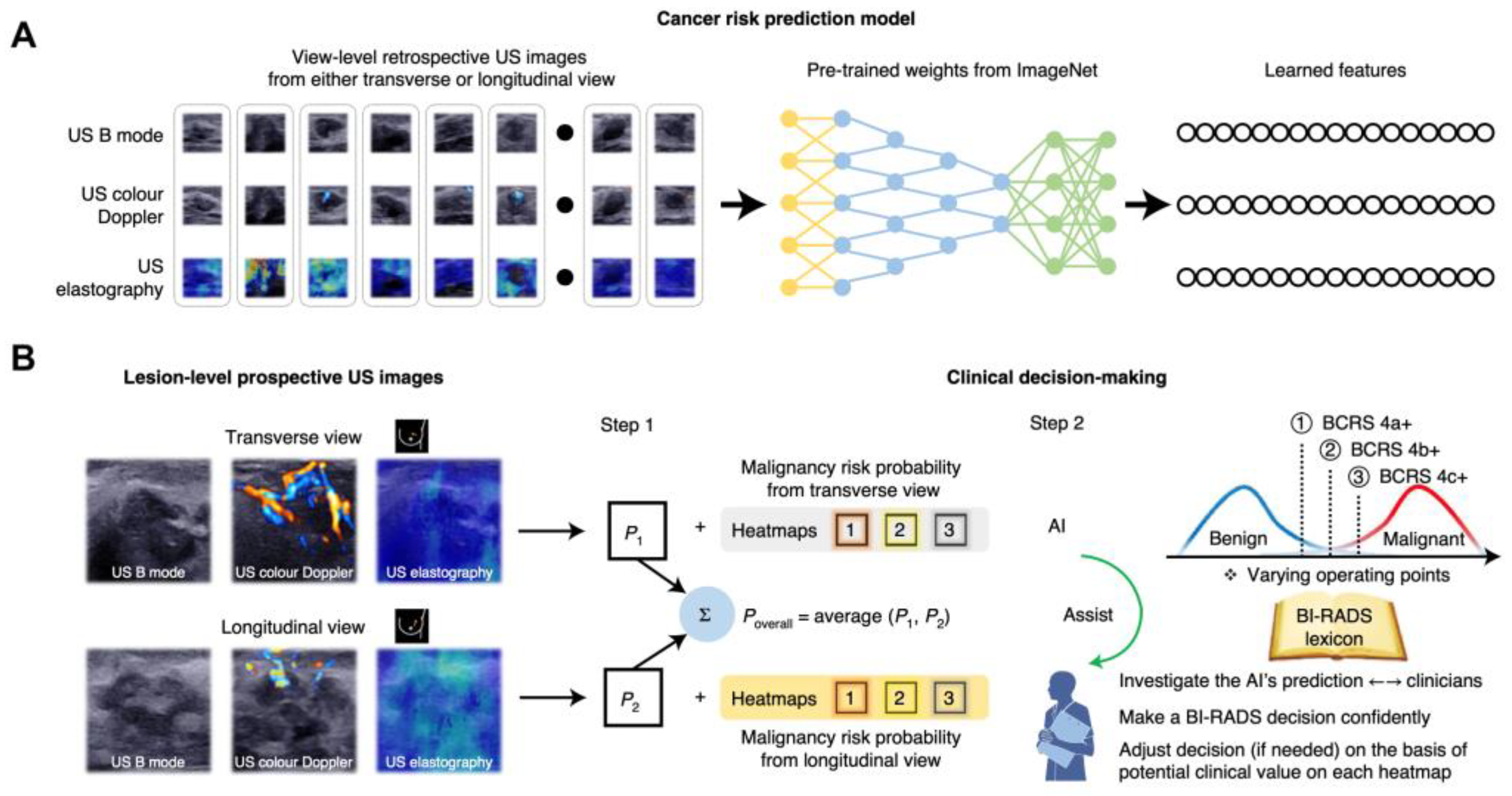
3.2. Deep Learning (DL) in ABUS

3.3. Portable US Devices in LMICs
4. Implementation of US for BC Screening in LMICs
4.1. Data Management
4.2. Public Awareness
4.3. Target Group
4.4. Effective Treatment
4.5. Novel Techniques
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA A Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Torre, L.A.; Siegel, R.L.; Ward, E.M.; Jemal, A. Global Cancer Incidence and Mortality Rates and Trends—An Update. Cancer Epidemiol. Biomark. Prev. 2016, 25, 16–27. [Google Scholar] [CrossRef] [Green Version]
- Lima, S.M.; Kehm, R.D.; Terry, M.B. Global Breast Cancer Incidence and Mortality Trends by Region, Age-Groups, and Fertility Patterns. E Clin. Med. 2021, 38, 100985. [Google Scholar] [CrossRef] [PubMed]
- Mollura, D.J.; Culp, M.P.; Lungren, M.P. (Eds.) Radiology in Global Health: Strategies, Implementation, and Applications; Springer: Berlin/Heidelberg, Germany, 2019; ISBN 978-3-319-98484-1. [Google Scholar]
- Béatrice, L.-S.; Chiara, S.; Dana, L.; Lamia, B.-T.; Véronique, B.; Franca, B.; Kurt, S. Breast-Cancer Screening—Viewpoint of the IARC Working Group. N. Engl. J. Med. 2015, 6, 2353–2358. [Google Scholar]
- Wilkerson, A.D.; Obi, M.; Ortega, C.; Sebikali-Potts, A.; Wei, W.; Pederson, H.J.; Al-Hilli, Z. Young Black Women May Be More Likely to Have First Mammogram Cancers: A New Perspective in Breast Cancer Disparities. Ann. Surg. Oncol. 2023, 30, 1–5. [Google Scholar] [CrossRef]
- Salameh, J.-P.; Kashif Al-Ghita, M.; McInnes, M.D.F.; Seely, J.M. Screening with Breast Cancer Mammography: Re-Evaluation of Current Evidence. Can. Assoc. Radiol. J. 2023, 084653712211481. [Google Scholar] [CrossRef]
- Corbex, M.; Burton, R.; Sancho-Garnier, H. Breast Cancer Early Detection Methods for Low and Middle Income Countries, a Review of the Evidence. Breast 2012, 21, 428–434. [Google Scholar] [CrossRef]
- Al-Foheidi, M.; Al-Mansour, M.M.; Ibrahim, E.M. Breast Cancer Screening: Review of Benefits and Harms, and Recommendations for Developing and Low-Income Countries. Med. Oncol. 2013, 30, 471. [Google Scholar] [CrossRef]
- Welch, H.G.; Prorok, P.C.; O’Malley, A.J.; Kramer, B.S. Breast-Cancer Tumor Size, Overdiagnosis, and Mammography Screening Effectiveness. N. Engl. J. Med. 2016, 375, 1438–1447. [Google Scholar] [CrossRef]
- Wong, I.O.L.; Kuntz, K.M.; Cowling, B.J.; Lam, C.L.K.; Leung, G.M. Cost Effectiveness of Mammography Screening for Chinese Women. Cancer 2007, 110, 885–895. [Google Scholar] [CrossRef]
- Dixon, A.M. Breast Ultrasound: How, Why and When; Churchill Livingstone: London, UK, 2008; ISBN 978-0-443-10076-5. [Google Scholar]
- Wang, J.; Zheng, S.; Ding, L.; Liang, X.; Wang, Y.; Greuter, M.J.W.; de Bock, G.H.; Lu, W. Is Ultrasound an Accurate Alternative for Mammography in Breast Cancer Screening in an Asian Population? A Meta-Analysis. Diagnostics 2020, 10, 985. [Google Scholar] [CrossRef] [PubMed]
- Yuan, W.-H.; Hsu, H.-C.; Chen, Y.-Y.; Wu, C.-H. Supplemental Breast Cancer-Screening Ultrasonography in Women with Dense Breasts: A Systematic Review and Meta-Analysis. Br. J. Cancer 2020, 123, 673–688. [Google Scholar] [CrossRef]
- Bowles, D.; Quinton, A. The Use of Ultrasound in Breast Cancer Screening of Asymptomatic Women with Dense Breast Tissue: A Narrative Review. J. Med. Imaging Radiat. Sci. 2016, 47, S21–S28. [Google Scholar] [CrossRef] [Green Version]
- Sood, R.; Rositch, A.F.; Shakoor, D.; Ambinder, E.; Pool, K.-L.; Pollack, E.; Mollura, D.J.; Mullen, L.A.; Harvey, S.C. Ultrasound for Breast Cancer Detection Globally: A Systematic Review and Meta-Analysis. J. Glob. Oncol. 2019, 5, 1–17. [Google Scholar] [CrossRef]
- Paci, E. Euroscreen Working Group Summary of the Evidence of Breast Cancer Service Screening Outcomes in Europe and First Estimate of the Benefit and Harm Balance Sheet. J. Med. Screen. 2012, 19, 5–13. [Google Scholar] [CrossRef]
- Schopper, D.; de Wolf, C. How Effective Are Breast Cancer Screening Programmes by Mammography? Review of the Current Evidence. Eur. J. Cancer 2009, 45, 1916–1923. [Google Scholar] [CrossRef]
- Leong, S.P.L.; Shen, Z.-Z.; Liu, T.-J.; Agarwal, G.; Tajima, T.; Paik, N.-S.; Sandelin, K.; Derossis, A.; Cody, H.; Foulkes, W.D. Is Breast Cancer the Same Disease in Asian and Western Countries? World J. Surg. 2010, 34, 2308–2324. [Google Scholar] [CrossRef] [Green Version]
- Suzuki, A.; Kuriyama, S.; Kawai, M.; Amari, M.; Takeda, M.; Ishida, T.; Ohnuki, K.; Nishino, Y.; Tsuji, I.; Shibuya, D.; et al. Age-Specific Interval Breast Cancers in Japan: Estimation of the Proper Sensitivity of Screening Using a Population-Based Cancer Registry. Cancer Sci. 2008, 99, 2264–2267. [Google Scholar] [CrossRef]
- Kang, L.-N.; Qiao, R.-L. Cancer Screening and Prevention in China. Cancer Control 2014, 3, 131. Available online: http://www.cancercontrol.info/cc2014/cancer-screening-and-prevention-in-china/ (accessed on 15 January 2023).
- Maskarinec, G.; Pagano, I.; Chen, Z.; Nagata, C.; Gram, I.T. Ethnic and Geographic Differences in Mammographic Density and Their Association with Breast Cancer Incidence. Breast Cancer Res. Treat. 2007, 104, 47–56. [Google Scholar] [CrossRef]
- Dai, H.; Yan, Y.; Wang, P.; Liu, P.; Cao, Y.; Xiong, L.; Luo, Y.; Pan, T.; Ma, X.; Wang, J.; et al. Distribution of Mammographic Density and Its Influential Factors among Chinese Women. Int. J. Epidemiol. 2014, 43, 1240–1251. [Google Scholar] [CrossRef]
- Ciatto, S.; Visioli, C.; Paci, E.; Zappa, M. Breast Density as a Determinant of Interval Cancer at Mammographic Screening. Br. J. Cancer 2004, 90, 393–396. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McCormack, V.A.; dos Santos Silva, I. Breast Density and Parenchymal Patterns as Markers of Breast Cancer Risk: A Meta-Analysis. Cancer Epidemiol. Biomark. Prev. 2006, 15, 1159–1169. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chiu, S.Y.-H.; Duffy, S.; Yen, A.M.-F.; Tabár, L.; Smith, R.A.; Chen, H.-H. Effect of Baseline Breast Density on Breast Cancer Incidence, Stage, Mortality, and Screening Parameters: 25-Year Follow-up of a Swedish Mammographic Screening. Cancer Epidemiol. Biomark. Prev. 2010, 19, 1219–1228. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yaghjyan, L.; Colditz, G.A.; Collins, L.C.; Schnitt, S.J.; Rosner, B.; Vachon, C.; Tamimi, R.M. Mammographic Breast Density and Subsequent Risk of Breast Cancer in Postmenopausal Women According to Tumor Characteristics. J. Natl. Cancer Inst. 2011, 103, 1179–1189. [Google Scholar] [CrossRef] [Green Version]
- Boyd, N.F.; Sun, L.; Stone, J.; Fishell, E.; Jong, R.A.; Chiarelli, A. Mammographic Density and the Risk and Detection of Breast Cancer. N. Engl. J. Med. 2007, 356, 10. [Google Scholar] [CrossRef] [Green Version]
- Nothacker, M.; Duda, V.; Hahn, M.; Warm, M.; Degenhardt, F.; Madjar, H.; Weinbrenner, S.; Albert, U.-S. Early Detection of Breast Cancer: Benefits and Risks of Supplemental Breast Ultrasound in Asymptomatic Women with Mammographically Dense Breast Tissue. A Systematic Review. BMC Cancer 2009, 9, 335. [Google Scholar] [CrossRef] [Green Version]
- Youk, J.H.; Kim, E.-K.; Kim, M.J.; Kwak, J.Y.; Son, E.J. Performance of Hand-Held Whole-Breast Ultrasound Based on BI-RADS in Women with Mammographically Negative Dense Breast. Eur. Radiol. 2011, 21, 667–675. [Google Scholar] [CrossRef]
- Uchida, K.; Yamashita, A.; Kawase, K.; Kamiya, K. Screening Ultrasonography Revealed 15% of Mammographically Occult Breast Cancers. Breast Cancer 2008, 15, 165–168. [Google Scholar] [CrossRef]
- Kim, S.; Tran, T.X.M.; Song, H.; Park, B. Microcalcifications, Mammographic Breast Density, and Risk of Breast Cancer: A Cohort Study. Breast Cancer Res. 2022, 24, 96. [Google Scholar] [CrossRef]
- Athanasiou, A.; Tardivon, A.; Ollivier, L.; Thibault, F.; El Khoury, C.; Neuenschwander, S. How to Optimize Breast Ultrasound. Eur. J. Radiol. 2009, 69, 6–13. [Google Scholar] [CrossRef]
- Rella, R.; Belli, P.; Giuliani, M.; Bufi, E.; Carlino, G.; Rinaldi, P.; Manfredi, R. Automated Breast Ultrasonography (ABUS) in the Screening and Diagnostic Setting. Acad. Radiol. 2018, 25, 1457–1470. [Google Scholar] [CrossRef]
- Zanotel, M.; Bednarova, I.; Londero, V.; Linda, A.; Lorenzon, M.; Girometti, R.; Zuiani, C. Automated Breast Ultrasound: Basic Principles and Emerging Clinical Applications. Radiol. Med. 2018, 123, 1–12. [Google Scholar] [CrossRef]
- Boca, I.; Ciurea, A.I.; Ciortea, C.A.; Dudea, S.M. Pros and Cons for Automated Breast Ultrasound (ABUS): A Narrative Review. J. Pers. Med. 2021, 11, 703. [Google Scholar] [CrossRef]
- Kelly, K.M.; Richwald, G.A. Automated Whole-Breast Ultrasound: Advancing the Performance of Breast Cancer Screening. Semin. Ultrasound CT MRI 2011, 32, 273–280. [Google Scholar] [CrossRef]
- Kaplan, S.S. Automated Whole Breast Ultrasound. Radiol. Clin. N. Am. 2014, 52, 539–546. [Google Scholar] [CrossRef]
- Brem, R.F.; Tabár, L.; Duffy, S.W.; Inciardi, M.F.; Guingrich, J.A.; Hashimoto, B.E.; Lander, M.R.; Lapidus, R.L.; Peterson, M.K.; Rapelyea, J.A.; et al. Assessing Improvement in Detection of Breast Cancer with Three-Dimensional Automated Breast US in Women with Dense Breast Tissue: The SomoInsight Study. Radiology 2015, 274, 663–673. [Google Scholar] [CrossRef] [Green Version]
- Chang, J.M.; Koo, H.R.; Moon, W.K. Radiologist-Performed Hand-Held Ultrasound Screening at Average Risk of Breast Cancer: Results from a Single Health Screening Center. Acta Radiol. 2015, 56, 652–658. [Google Scholar] [CrossRef]
- Berg, W.A.; Vourtsis, A. Screening Breast Ultrasound Using Handheld or Automated Technique in Women with Dense Breasts. J. Breast Imaging 2019, 1, 283–296. [Google Scholar] [CrossRef] [Green Version]
- Huppe, A.I.; Inciardi, M.F.; Redick, M.; Carroll, M.; Buckley, J.; Hill, J.D.; Gatewood, J.B. Automated Breast Ultrasound Interpretation Times. Acad. Radiol. 2018, 25, 1577–1581. [Google Scholar] [CrossRef]
- Yang, L.; Wang, S.; Zhang, L.; Sheng, C.; Song, F.; Wang, P.; Huang, Y. Performance of Ultrasonography Screening for Breast Cancer: A Systematic Review and Meta-Analysis. BMC Cancer 2020, 20, 499. [Google Scholar] [CrossRef] [PubMed]
- Melnikow, J.; Fenton, J.J.; Whitlock, E.P.; Miglioretti, D.L.; Weyrich, M.S.; Thompson, J.H.; Shah, K. Supplemental Screening for Breast Cancer in Women With Dense Breasts: A Systematic Review for the U.S. Preventive Services Task Force. Ann. Intern. Med. 2016, 164, 268. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Luo, C.; Wang, L.; Zhang, Y.; Lu, M.; Lu, B.; Cai, J.; Chen, H.; Dai, M. Advances in Breast Cancer Screening Modalities and Status of Global Screening Programs. Chronic Dis. Transl. Med. 2022, 8, 112–123. [Google Scholar] [CrossRef] [PubMed]
- Girardi, V.; Tonegutti, M.; Ciatto, S.; Bonetti, F. Breast Ultrasound in 22,131 Asymptomatic Women with Negative Mammography. Breast 2013, 22, 806–809. [Google Scholar] [CrossRef] [PubMed]
- Ohuchi, N.; Suzuki, A.; Sobue, T.; Kawai, M.; Yamamoto, S.; Zheng, Y.-F.; Shiono, Y.N.; Saito, H.; Kuriyama, S.; Tohno, E.; et al. Sensitivity and Specificity of Mammography and Adjunctive Ultrasonography to Screen for Breast Cancer in the Japan Strategic Anti-Cancer Randomized Trial (J-START): A Randomised Controlled Trial. Lancet 2016, 387, 341–348. [Google Scholar] [CrossRef]
- Thigpen, D.; Kappler, A.; Brem, R. The Role of Ultrasound in Screening Dense Breasts—A Review of the Literature and Practical Solutions for Implementation. Diagnostics 2018, 8, 20. [Google Scholar] [CrossRef] [Green Version]
- Sprague, B.L.; Arao, R.F.; Miglioretti, D.L.; Henderson, L.M.; Buist, D.S.M.; Onega, T.; Rauscher, G.H.; Lee, J.M.; Tosteson, A.N.A.; Kerlikowske, K.; et al. National Performance Benchmarks for Modern Diagnostic Digital Mammography: Update from the Breast Cancer Surveillance Consortium. Radiology 2017, 283, 59–69. [Google Scholar] [CrossRef] [Green Version]
- Da Costa Vieira, R.A.; Biller, G.; Uemura, G.; Ruiz, C.A.; Curado, M.P. Breast Cancer Screening in Developing Countries. Clinics 2017, 72, 244–253. [Google Scholar] [CrossRef]
- Berg, W.A.; Bandos, A.I.; Mendelson, E.B.; Lehrer, D.; Jong, R.A.; Pisano, E.D. Ultrasound as the Primary Screening Test for Breast Cancer: Analysis From ACRIN 6666. J. Natl. Cancer Inst. 2016, 108, djv367. [Google Scholar] [CrossRef]
- Cho, N.; Moon, W.K.; Chang, J.M.; Yi, A.; Koo, H.R.; Han, B.-K. Sonographic Characteristics of Breast Cancers Detected by Supplemental Screening US: Comparison with Breast Cancers Seen on Screening Mammography. Acta Radiol. 2010, 51, 969–976. [Google Scholar] [CrossRef]
- Wong, J.Z.Y.; Chai, J.H.; Yeoh, Y.S.; Riza, N.K.M.; Liu, J.; Teo, Y.-Y.; Wee, H.L.; Hartman, M. Cost Effectiveness Analysis of a Polygenic Risk Tailored Breast Cancer Screening Programme in Singapore. BMC Health Serv. Res. 2021, 21, 379. [Google Scholar] [CrossRef]
- Kerlikowske, K.; Bissell, M.C.S.; Sprague, B.L.; Buist, D.S.M.; Henderson, L.M.; Lee, J.M.; Miglioretti, D.L. Advanced Breast Cancer Definitions by Staging System Examined in the Breast Cancer Surveillance Consortium. J. Natl. Cancer Inst. 2021, 113, 909–916. [Google Scholar] [CrossRef]
- Taylor, R.; Supramaniam, R.; Rickard, M.; Estoesta, J.; Moreira, C. Interval Breast Cancers in New South Wales, Australia, and Comparisons with Trials and Other Mammographic Screening Programmes. J. Med. Screen. 2002, 9, 20–25. [Google Scholar] [CrossRef]
- Bulliard, J.-L.; Sasieni, P.; Klabunde, C.; De Landtsheer, J.-P.; Yankaskas, B.C.; Fracheboud, J. Methodological Issues in International Comparison of Interval Breast Cancers. Int. J. Cancer 2006, 119, 1158–1163. [Google Scholar] [CrossRef]
- Corsetti, V.; Houssami, N.; Ghirardi, M.; Ferrari, A.; Speziani, M.; Bellarosa, S.; Remida, G.; Gasparotti, C.; Galligioni, E.; Ciatto, S. Evidence of the Effect of Adjunct Ultrasound Screening in Women with Mammography-Negative Dense Breasts: Interval Breast Cancers at 1year Follow-Up. Eur. J. Cancer 2011, 47, 1021–1026. [Google Scholar] [CrossRef]
- Shen, S.; Zhou, Y.; Xu, Y.; Zhang, B.; Duan, X.; Huang, R.; Li, B.; Shi, Y.; Shao, Z.; Liao, H.; et al. A Multi-Centre Randomised Trial Comparing Ultrasound vs Mammography for Screening Breast Cancer in High-Risk Chinese Women. Br. J. Cancer 2015, 112, 998–1004. [Google Scholar] [CrossRef] [Green Version]
- Omidiji, O.A.T.; Campbell, P.C.; Irurhe, N.K.; Atalabi, O.M.; Toyobo, O.O. Breast Cancer Screening in a Resource Poor Country: Ultrasound versus Mammography. Ghana Med. J. 2017, 51, 6. [Google Scholar] [CrossRef] [Green Version]
- Shao, H.; Li, B.; Zhang, X.; Xiong, Z.; Liu, Y.; Tang, G. Comparison of the Diagnostic Efficiency for Breast Cancer in Chinese Women Using Mammography, Ultrasound, MRI, and Different Combinations of These Imaging Modalities. J. X-Ray Sci. Technol. 2013, 21, 283–292. [Google Scholar] [CrossRef]
- Matovu, A.; Scheel, J.R.; Shadrack, P.A.; Ssembatya, R.; Njeri, A.; Galukande, M. Pilot Study of a Resource-Appropriate Strategy for Downstaging Breast Cancer in Rural Uganda. J. Glob. Radiol. 2016, 2, 1. [Google Scholar] [CrossRef] [Green Version]
- Tan, K.P.; Mohamad, A.Z.; Rumaisa, M.P.; Murni, M.R.S.A.; Radhika, S.; Nurismah, M.I.; Norlia, A.; Zulfiqar, M.A. The Comparative Accuracy of Ultrasound and Mammography in The Detection of Breast Cancer. Med. J. Malays. 2014, 69, 7. [Google Scholar]
- Anderson, B.O.; Yip, C.-H.; Smith, R.A.; Shyyan, R.; Sener, S.F.; Eniu, A.; Carlson, R.W.; Azavedo, E.; Harford, J. Guideline Implementation for Breast Healthcare in Low-Income and Middle-Income Countries: Overview of the Breast Health Global Initiative Global Summit 2007. Cancer 2008, 113, 2221–2243. [Google Scholar] [CrossRef] [PubMed]
- Song, Q.-K.; Wang, X.-L.; Zhou, X.-N.; Yang, H.-B.; Li, Y.-C.; Wu, J.-P.; Ren, J.; Lyerly, H.K. Breast Cancer Challenges and Screening in China: Lessons From Current Registry Data and Population Screening Studies. Oncologist 2015, 20, 773–779. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sun, L.; Legood, R.; Sadique, Z.; dos-Santos-Silva, I.; Yang, L. Breast Cancer Screening Programme in China: Does One Size Fit All? A Cost-Effectiveness Analysis Based on a Markov Model. Lancet 2018, 392, S2. [Google Scholar] [CrossRef]
- Huang, Y.; Tong, Z.; Chen, K.; Wang, Y.; Liu, P.; Gu, L.; Liu, J.; Yu, J.; Song, F.; Zhao, W.; et al. Interpretation of Breast Cancer Screening Guideline for Chinese Women. Cancer Biol. Med. 2019, 16, 825–835. [Google Scholar] [CrossRef]
- Kelly, K.M.; Dean, J.; Comulada, W.S.; Lee, S.-J. Breast Cancer Detection Using Automated Whole Breast Ultrasound and Mammography in Radiographically Dense Breasts. Eur. Radiol. 2010, 20, 734–742. [Google Scholar] [CrossRef] [Green Version]
- Choi, W.J.; Cha, J.H.; Kim, H.H.; Shin, H.J.; Kim, H.; Chae, E.Y.; Hong, M.J. Comparison of Automated Breast Volume Scanning and Hand-Held Ultrasound in the Detection of Breast Cancer: An Analysis of 5,566 Patient Evaluations. Asian Pac. J. Cancer Prev. 2014, 15, 9101–9105. [Google Scholar] [CrossRef] [Green Version]
- Wang, H.-Y.; Jiang, Y.-X.; Zhu, Q.-L.; Zhang, J.; Dai, Q.; Liu, H.; Lai, X.-J.; Sun, Q. Differentiation of Benign and Malignant Breast Lesions: A Comparison between Automatically Generated Breast Volume Scans and Handheld Ultrasound Examinations. Eur. J. Radiol. 2012, 81, 3190–3200. [Google Scholar] [CrossRef]
- Wang, Z.L.; Xw, J.H.; Li, J.L.; Huang, Y.; Tang, J. Comparison of Automated Breast Volume Scanning to Hand-Held Ultrasound and Mammography. Radiol. Med. 2012, 117, 1287–1293. [Google Scholar] [CrossRef]
- Chen, L.; Chen, Y.; Diao, X.-H.; Fang, L.; Pang, Y.; Cheng, A.-Q.; Li, W.-P.; Wang, Y. Comparative Study of Automated Breast 3-D Ultrasound and Handheld B-Mode Ultrasound for Differentiation of Benign and Malignant Breast Masses. Ultrasound Med. Biol. 2013, 39, 1735–1742. [Google Scholar] [CrossRef]
- Giuliano, V.; Giuliano, C. Improved Breast Cancer Detection in Asymptomatic Women Using 3D-Automated Breast Ultrasound in Mammographically Dense Breasts. Clin. Imaging 2013, 37, 480–486. [Google Scholar] [CrossRef]
- Giger, M.L.; Inciardi, M.F.; Edwards, A.; Papaioannou, J.; Drukker, K.; Jiang, Y.; Brem, R.; Brown, J.B. Automated Breast Ultrasound in Breast Cancer Screening of Women with Dense Breasts: Reader Study of Mammography-Negative and Mammography-Positive Cancers. Am. J. Roentgenol. 2016, 206, 1341–1350. [Google Scholar] [CrossRef] [Green Version]
- Wilczek, B.; Wilczek, H.E.; Rasouliyan, L.; Leifland, K. Adding 3D Automated Breast Ultrasound to Mammography Screening in Women with Heterogeneously and Extremely Dense Breasts: Report from a Hospital-Based, High-Volume, Single-Center Breast Cancer Screening Program. Eur. J. Radiol. 2016, 85, 1554–1563. [Google Scholar] [CrossRef] [Green Version]
- Choi, W.J.; Kim, S.H.; Shin, H.J.; Bang, M.; Kang, B.J.; Lee, S.H.; Chang, J.M.; Moon, W.K.; Bae, K.; Kim, H.H. Automated Breast US as the Primary Screening Test for Breast Cancer among East Asian Women Aged 40-49 Years: A Multicenter Prospective Study. Eur. Radiol. 2021, 31, 7771–7782. [Google Scholar] [CrossRef]
- Niu, L.; Bao, L.; Zhu, L.; Tan, Y.; Xu, X.; Shan, Y.; Liu, J.; Zhu, Q.; Jiang, C.; Shen, Y. Diagnostic Performance of Automated Breast Ultrasound in Differentiating Benign and Malignant Breast Masses in Asymptomatic Women: A Comparison Study With Handheld Ultrasound. J. Ultrasound Med. 2019, 38, 2871–2880. [Google Scholar] [CrossRef]
- Jeh, S.K.; Kim, S.H.; Choi, J.J.; Jung, S.S.; Choe, B.J.; Park, S.; Park, M.S. Comparison of Automated Breast Ultrasonography to Handheld Ultrasonography in Detecting and Diagnosing Breast Lesions. Acta Radiol. 2016, 57, 162–169. [Google Scholar] [CrossRef]
- Lee, J.; Kang, B.J.; Kim, S.H.; Park, G.E. Evaluation of Computer-Aided Detection (CAD) in Screening Automated Breast Ultrasound Based on Characteristics of CAD Marks and False-Positive Marks. Diagnostics 2022, 12, 583. [Google Scholar] [CrossRef]
- Tan, T.; Mordang, J.-J.; van Zelst, J.; Grivegnée, A.; Gubern-Mérida, A.; Melendez, J.; Mann, R.M.; Zhang, W.; Platel, B.; Karssemeijer, N. Computer-Aided Detection of Breast Cancers Using Haar-like Features in Automated 3D Breast Ultrasound: Computer-Aided Detection of Breast Cancers. Med. Phys. 2015, 42, 1498–1504. [Google Scholar] [CrossRef]
- Van Zelst, J.C.M.; Tan, T.; Clauser, P.; Domingo, A.; Dorrius, M.D.; Drieling, D.; Golatta, M.; Gras, F.; de Jong, M.; Pijnappel, R.; et al. Dedicated Computer-Aided Detection Software for Automated 3D Breast Ultrasound; an Efficient Tool for the Radiologist in Supplemental Screening of Women with Dense Breasts. Eur. Radiol. 2018, 28, 2996–3006. [Google Scholar] [CrossRef] [Green Version]
- Kim, Y.; Rim, J.; Kim, S.M.; Yun, B.L.; Park, S.Y.; Ahn, H.S.; Kim, B.; Jang, M. False-Negative Results on Computer-Aided Detection Software in Preoperative Automated Breast Ultrasonography of Breast Cancer Patients. Ultrasonography 2021, 40, 83–92. [Google Scholar] [CrossRef] [Green Version]
- Yang, S.; Gao, X.; Liu, L.; Shu, R.; Yan, J.; Zhang, G.; Xiao, Y.; Ju, Y.; Zhao, N.; Song, H. Performance and Reading Time of Automated Breast US with or without Computer-Aided Detection. Radiology 2019, 292, 540–549. [Google Scholar] [CrossRef]
- Xu, X.; Bao, L.; Tan, Y.; Zhu, L.; Kong, F.; Wang, W. 1000-Case Reader Study of Radiologists’ Performance in Interpretation of Automated Breast Volume Scanner Images with a Computer-Aided Detection System. Ultrasound Med. Biol. 2018, 44, 1694–1702. [Google Scholar] [CrossRef] [PubMed]
- Van Zelst, J.C.; Tan, T.; Mann, R.M.; Karssemeijer, N. Validation of Radiologists’ Findings by Computer-Aided Detection (CAD) Software in Breast Cancer Detection with Automated 3D Breast Ultrasound: A Concept Study in Implementation of Artificial Intelligence Software. Acta Radiol. 2020, 61, 312–320. [Google Scholar] [CrossRef] [PubMed]
- Mahoro, E.; Akhloufi, M.A. Applying Deep Learning for Breast Cancer Detection in Radiology. Curr. Oncol. 2022, 29, 8767–8793. [Google Scholar] [CrossRef] [PubMed]
- Freeman, K.; Geppert, J.; Stinton, C.; Todkill, D.; Johnson, S.; Clarke, A.; Taylor-Phillips, S. Use of Artificial Intelligence for Image Analysis in Breast Cancer Screening Programmes: Systematic Review of Test Accuracy. BMJ 2021, 374, n1872. [Google Scholar] [CrossRef]
- Kim, M.Y.; Kim, S.-Y.; Kim, Y.S.; Kim, E.S.; Chang, J.M. Added Value of Deep Learning-Based Computer-Aided Diagnosis and Shear Wave Elastography to b-Mode Ultrasound for Evaluation of Breast Masses Detected by Screening Ultrasound. Medicine 2021, 100, e26823. [Google Scholar] [CrossRef]
- Raya-Povedano, J.L.; Romero-Martín, S.; Elías-Cabot, E.; Gubern-Mérida, A.; Rodríguez-Ruiz, A.; Álvarez-Benito, M. AI-Based Strategies to Reduce Workload in Breast Cancer Screening with Mammography and Tomosynthesis: A Retrospective Evaluation. Radiology 2021, 300, 57–65. [Google Scholar] [CrossRef]
- Shen, Y.; Shamout, F.E.; Oliver, J.R.; Witowski, J.; Kannan, K.; Park, J.; Wu, N.; Huddleston, C.; Wolfson, S.; Millet, A.; et al. Artificial Intelligence System Reduces False-Positive Findings in the Interpretation of Breast Ultrasound Exams. Nat. Commun. 2021, 12, 5645. [Google Scholar] [CrossRef]
- Zhao, C.; Xiao, M.; Ma, L.; Ye, X.; Deng, J.; Cui, L.; Guo, F.; Wu, M.; Luo, B.; Chen, Q.; et al. Enhancing Performance of Breast Ultrasound in Opportunistic Screening Women by a Deep Learning-Based System: A Multicenter Prospective Study. Front. Oncol. 2022, 12, 804632. [Google Scholar] [CrossRef]
- Fujioka, T.; Mori, M.; Kubota, K.; Oyama, J.; Yamaga, E.; Yashima, Y.; Katsuta, L.; Nomura, K.; Nara, M.; Oda, G.; et al. The Utility of Deep Learning in Breast Ultrasonic Imaging: A Review. Diagnostics 2020, 10, 1055. [Google Scholar] [CrossRef]
- Wang, Y.; Choi, E.J.; Choi, Y.; Zhang, H.; Jin, G.Y.; Ko, S.-B. Breast Cancer Classification in Automated Breast Ultrasound Using Multiview Convolutional Neural Network with Transfer Learning. Ultrasound Med. Biol. 2020, 46, 1119–1132. [Google Scholar] [CrossRef]
- Qian, X.; Pei, J.; Zheng, H.; Xie, X.; Yan, L.; Zhang, H.; Han, C.; Gao, X.; Zhang, H.; Zheng, W.; et al. Prospective Assessment of Breast Cancer Risk from Multimodal Multiview Ultrasound Images via Clinically Applicable Deep Learning. Nat. Biomed. Eng. 2021, 5, 522–532. [Google Scholar] [CrossRef]
- Spencer, J.K.; Adler, R.S. Utility of Portable Ultrasound in a Community in Ghana. J. Ultrasound Med. 2008, 27, 1735–1743. [Google Scholar] [CrossRef] [Green Version]
- Wang, Z.; He, B.; Zhang, Y.; Li, Z.; Yao, R.; Huang, K. Design and Implementation for Portable Ultrasound-Aided Breast Cancer Screening System. J. Biomed. Eng. 2022, 39, 390–397. [Google Scholar] [CrossRef]
- Love, S.M.; Berg, W.A.; Podilchuk, C.; Aldrete, A.L.L.; Mascareño, A.P.G.; Pathicherikollamparambil, K.; Sankarasubramanian, A.; Eshraghi, L.; Mammone, R. Palpable Breast Lump Triage by Minimally Trained Operators in Mexico Using Computer-Assisted Diagnosis and Low-Cost Ultrasound. J. Glob. Oncol. 2018, 4, 1–9. [Google Scholar] [CrossRef]
- Fallowfield, L.J.; Hall, A. Psychosocial and Sexual Impact of Diagnosis and Treatment of Breast Cancer. Br. Med. Bull. 1991, 47, 388–399. [Google Scholar] [CrossRef]
- Islam, R.M.; Billah, B.; Hossain, M.N.; Oldroyd, J. Barriers to Cervical Cancer and Breast Cancer Screening Uptake in Low-Income and Middle-Income Countries: A Systematic Review. Asian Pac. J. Cancer Prev. 2017, 18, 1751–1763. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| MAM | HHUS | ABUS | |
|---|---|---|---|
| Sensitivity to dense breast | Low | High | High |
| Sensitivity to microcalcification | High | Low | Low |
| Specificity | High | Decreased | Decreased |
| Reproducibility | High | Low | High |
| Guiding further biopsy | Non | Yes | Non |
| Radiation | Yes | Non | Non |
| Breast compression pain | Yes | Non | Non |
| Equipment availability | Less | Wide | Less |
| Examination expense | Relatively expensive | Less expensive | Less expensive |
| Examination provider | Technologist | Experienced sonographer | Technologist |
| References | Patients | Sensitivity (%) | Specificity (%) | Detection Rate (per 1000 Women) | Recall Rate (per 1000 Women) | ||||
|---|---|---|---|---|---|---|---|---|---|
| MAM | MAM + ABUS | MAM | MAM + ABUS | MAM | MAM + ABUS | MAM | MAM + ABUS | ||
| Giuliano [72] | 3418 | 76 | 96.7 | 98.2 | 99.7 | 4.6 | 12.3 | NR | NR |
| Brem [39] | 15,318 | 73.2 | 100 | 85.4 | 72 | 5.4 | 7.3 | 150.2 | 284.9 |
| Giger [73] | 185 | 57.5 | 74.1 | 78.1 | 76.2 | NR | NR | NR | NR |
| Kelly [67] | 4419 | 40 | 81 | 95.15 | 98.7 | 3.6 | 7.2 | 42 | 96 |
| Wilczek [74] | 1668 | 63.6 | 100 | 99 | 98.4 | 4.2 | 6.6 | 13.8 | 22.8 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dan, Q.; Zheng, T.; Liu, L.; Sun, D.; Chen, Y. Ultrasound for Breast Cancer Screening in Resource-Limited Settings: Current Practice and Future Directions. Cancers 2023, 15, 2112. https://doi.org/10.3390/cancers15072112
Dan Q, Zheng T, Liu L, Sun D, Chen Y. Ultrasound for Breast Cancer Screening in Resource-Limited Settings: Current Practice and Future Directions. Cancers. 2023; 15(7):2112. https://doi.org/10.3390/cancers15072112
Chicago/Turabian StyleDan, Qing, Tingting Zheng, Li Liu, Desheng Sun, and Yun Chen. 2023. "Ultrasound for Breast Cancer Screening in Resource-Limited Settings: Current Practice and Future Directions" Cancers 15, no. 7: 2112. https://doi.org/10.3390/cancers15072112
APA StyleDan, Q., Zheng, T., Liu, L., Sun, D., & Chen, Y. (2023). Ultrasound for Breast Cancer Screening in Resource-Limited Settings: Current Practice and Future Directions. Cancers, 15(7), 2112. https://doi.org/10.3390/cancers15072112