
Innovative Invasive Loco-Regional Techniques for the Treatment of Lung Cancer

 , , , , , and
, , , , , and
Abstract
:Simple Summary
Abstract
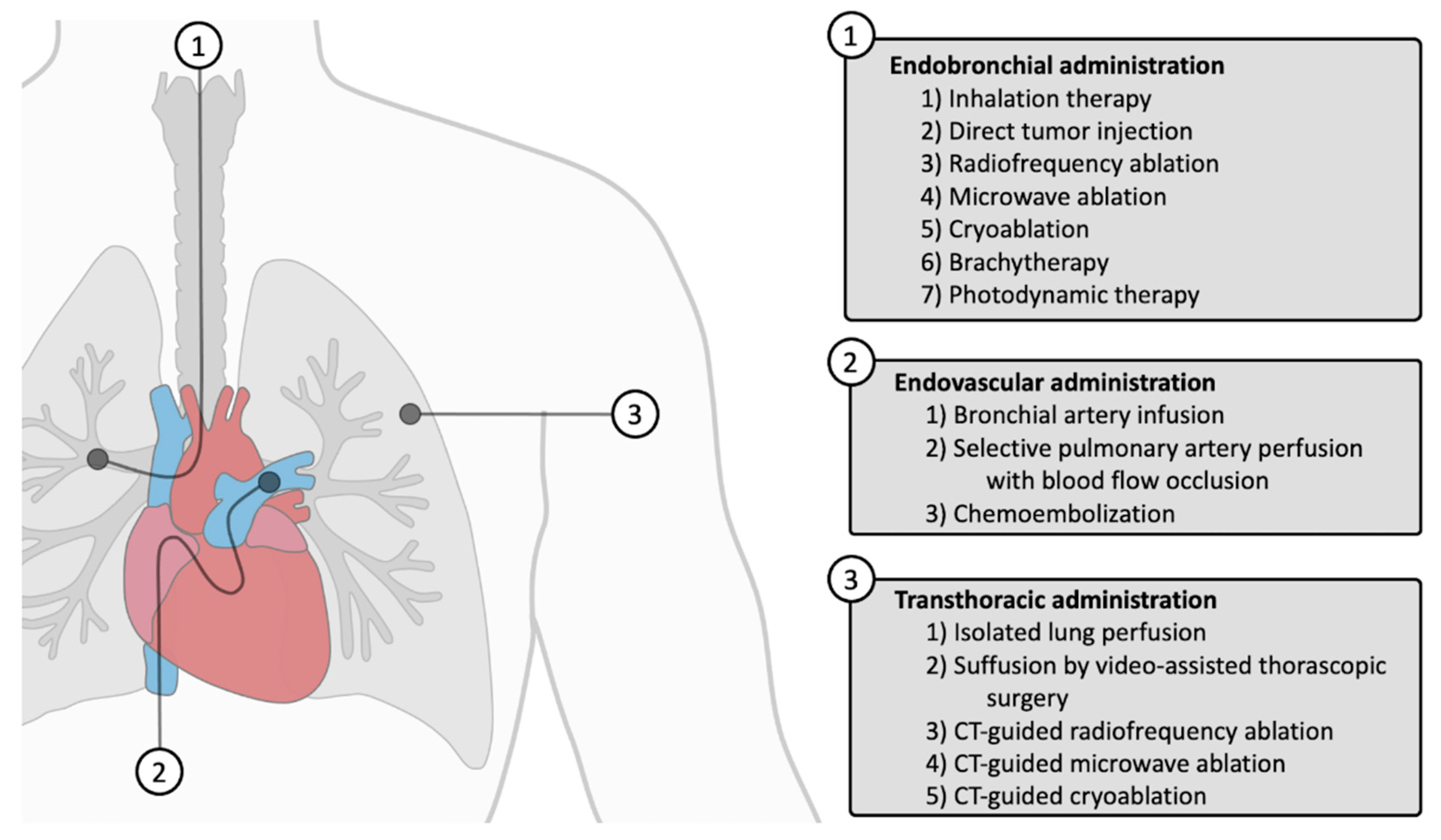
1. Introduction
2. Endobronchial Administration
2.1. Endobronchial Localization and Diagnosis
2.2. Inhalation Therapies
2.3. Navigation Therapies
2.3.1. Direct Tumor Injection
2.3.2. Brachytherapy
2.3.3. Radiofrequency Ablation (RFA)
2.3.4. Microwave Ablation (MWA)
2.3.5. Cryoablation (CRA)
2.3.6. Photodynamic Therapy (PDT)
3. Endovascular Administration
3.1. Bronchial Circulation
Bronchial Artery Infusion (BAI)
3.2. Pulmonary Circulation
3.2.1. Selective Pulmonary Artery Perfusion with Blood Flow Occlusion (SPAP-BFO)
3.2.2. Chemoembolization
4. Transthoracic Administration
4.1. Isolated Lung Perfusion (IluP)
4.2. Suffusion by Video-Assisted Thoracoscopic Surgery (VATS)
4.3. CT-Guided RFA
4.4. CT-Guided MWA
4.5. CT-Guided CRA
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Appendix A

{kind=link}
| Direct Tumor Injection | |||||||
| Author | Study | Type | Stages | Groups | N | Adj. Th. | |
| Mehta, H.J. [22] | Clinical trial | NSCLC, SCLC | Advanced | DTI (ChT) | 21 | ChT, RT, ChT/RT | |
| Mehta, H.J. [23] | Clinical trial | NSCLC, SCLC | Advanced | DTI (ChT) | 35 | None, ChT, RT | |
| Yarmus, L. [24] | Pilot study | NSCLC | IB, IIB, III, IV | DTI (ChT) | 27 | n/a, ChT | |
| Endobronchial route | Brachytherapy | ||||||
| Author | Study | Type | Stages | Groups | N | Adj. Th. | |
| Li, W. [27] | RCT | NSCLC | III, IV | BT RT | 35 36 | n/a n/a | |
| Yu, X. [32] | RCT | NSCLC | III | BT ChT | 26 26 | ChT n/a | |
| Mao, Y. [30] | RCT | NSCLC | Advanced | BT ChT | 57 45 | ChT n/a | |
| Wang, X. [31] | RCT | NSCLC | IIIB, IV | BT EGFR-TKI | 54 54 | EGFR-TKI n/a | |
| Chen, E. [26] | Meta-analysis | NSCLC | Early-stage | BT | 308 | n/a | |
| Chen, S. [28] | RCT | NSCLC | I, IIA, III | BT RFA | 15 15 | RFA n/a | |
| Chen, Z.K. [29] | Meta-analysis | NSCLC | III, IV | BT ChT | 259 257 | ChT n/a | |
| Endobronchial radiofrequency ablation | |||||||
| Author | Study | Type | Stages | Groups | N | Adj. Th. | |
| Xie, F. [35] | Case report | NSCLC | IA | fRFA | 3 | n/a | |
| Ishiwata, T. [36] | Pilot study | NSCLC | I, II | EBUS-RFA | 5 | n/a | |
| Endobronchial microwave ablation | |||||||
| Author | Study | Type | Stages | Groups | N | Adj. Th. | |
| Kashiwabara, K. [37] | Clinical trial | NSCLC, mets | Advanced | MWA | 38 | ATh | |
| Chan, J.W.Y. [38] | Clinical trial | LNs | n/a | MWA | 25 | n/a | |
| Xie, F. [39] | Pilot study | NSCLC, SCLC | Early | MWA | 13 | n/a | |
| Endobronchial cryoablation | |||||||
| Author | Study | Type | Stages | Groups | N | Adj. Th. | |
| Lee, H.S. [41] | Syst. Rev. | Lung/bronchial tumors | Advanced | CRA | 2353 | n/a | |
| Photodynamic therapy | |||||||
| Author | Study | Type | Stages | Groups | N | Adj. Th. | |
| Furuse, K. [43] | Clinical trial ph. II | NSCLC | TisN0M0, T1N0M0 | PDT | 54 | n/a | |
| McCaughan, J.S., Jr. [48] | Clinical trial | NSCLC | I, II, III, IV | PDT | 157 | n/a | |
| Kato, H. [45] | Clinical trial ph. II | NSCLC | Early | PDT | 40 | n/a | |
| Ji, W. [46] | Pilot study | NSCLC | III, IV | PDT | 10 | n/a, RT, ChT | |
| Dhillon, S.S. [44] | Clinical Trial ph. I | NSCLC | Early | PDT | 17 | n/a | |
| Lin, C. [47] | Clinical trial | NSCLC | IV | PDT | 20 | n/a | |
| Bronchial artery infusion | |||||||
| Author | Study | Type | Stages | Groups | N | Adj. Th. | |
| Nakanishi, M. [50] | Clinical trial | NSCLC | III, IV, M1b | BAI | 25 | n/a | |
| Xiong, F. [51] | RCT | NSCLC | Advanced | BAI BAI | 24 22 | n/a EGFR-TKI | |
| Zhu, J. [52] | Clinical trial | NSCLC | III | BAI | 36 | n/a | |
| Selective pulmonary artery perfusion with blood flow occlusion | |||||||
| Endovascular route | Author | Study | Groups | N | Adj. Th. | ||
| Van Putte, B.P. [53] | Preclinical | Intravenous GEM (1 g/m²) 30 min SPAP 10 min GEM (1 g/m²) SPAP 2 min GEM (1 g/m²) SPAP 2 min GEM (1 g/m²), BFO 50% 30 min SPAP 2 min GEM (1 g/m²), BFO 90% 30 min | 4 4 4 4 4 | n/a n/a n/a n/a n/a | |||
| Grootenboers, M.J. [54] | Preclinical | SPAP 2 min GEM (1 g/m2), BFO 100% 0 min SPAP 2 min GEM (1 g/m2), BFO 100% 10 min SPAP 2 min GEM (1 g/m2), BFO 100% 20 min SPAP 2 min GEM (1 g/m2), BFO 100% 30 min SPAP 2 min GEM (1.25 g/m2), BFO 100% 30 min SPAP 2 min GEM (1.5 g/m2), BFO 100% 30 min | 4 4 4 4 3 3 | n/a n/a n/a n/a n/a n/a | |||
| Van Putte, B.P. [55] | Preclinical | Intravenous GEM (1.25 g/m2) 30 min SPAP 2 min GEM (1.25 g/m2), BFO 100% 30 min SPAP 2 min GEM (1.25 g/m²)/CB, BFO 100% 30 min Intravenous CB 30 min SPAP 2 min CB, BFO 100% 30 min | 4 4 4 4 4 | n/a n/a CB n/a n/a | |||
| Sparks, P.J. [56] | Preclinical | Intravenous GEM (1.25 g/m2) 30 min SPAP 30 min GEM (1.25 g/m2), BFO 100% 30 min | 5 5 | n/a n/a | |||
| Chemoembolization | |||||||
| Author | Study | Type | Stages | Groups | N | Adj. Th. | |
| Vogl, T.J. [60] | Clinical trial | mets | n/a | CE | 52 | n/a | |
| Chang, L. [61] | Meta-analysis | N/S | N/S | CE CE | 350 150 | DEX n/a | |
| Jin, S.Q. [58] | Clinical trial | NSCLC | IIA, IIIB, IV | CE BAI | 264 513 | n/a n/a | |
| Boas, F.E. [59] | Clinical trial ph. I | mets | n/a | CE | 10 | n/a | |
| Transthoracic route | Isolated lung perfusion | ||||||
| Author | Study | Type | Stages | Groups | N | Adj. Th. | |
| Burt, M.E. [65] | Clinical trial ph. I | Un. mets | n/a | ILuP | 8 | n/a | |
| Hendriks, J.M.H. [67] | Clinical trial ph. I | Res. mets | n/a | ILuP | 16 | MS | |
| Grootenboers, M.J. [66] | Clinical trial ph. I | Res. mets | n/a | ILuP | 21 | MS | |
| den Hengst, W.A. [62] | Clinical trial ph. I | Res. mets | n/a | ILuP | 23 | n/a | |
| den Hengst, W.A. [63] | Clinical trial ph. II | Res. mets | n/a | ILuP | 50 | MS | |
| Beckers, P.A.J. [64] | Clinical trial ph. II | mets | n/a | ILuP | 107 | MS | |
| Suffusion by VATS | |||||||
| Author | Study | Type | Stages | Groups | N | Adj. Th. | |
| Demmy, T.L. [68] | Pilot study | n/a | n/a | suffusion | 4 | n/a | |
| Demmy, T.L. [69] | Clinical trial ph. I | oligomets | IV | CP suffusion | 4 | n/a | |
| CT-guided percutaneous RFA | |||||||
| Author | Study | Type | Stages | Groups | N | Adj. Th. | |
| Li, G. [73] | Meta-analysis | N/S | N/S | RFA | 1989 | n/a | |
| Jiang, B. [74] | Meta-analysis | N/S | N/S | RFA MWA CRA | 946 438 468 | n/a n/a n/a | |
| Palussière, J. [75] | Clinical trial ph. II | NSCLC | IIA | RFA | 32 | n/a | |
| Yuan, Z. [76] | Meta-analysis | N/S | N/S | RFA MWA | 2632 800 | n/a n/a | |
| Alexander, S.E. [71] | Clinical trial | NSCLC | IA | RFA | 45 | n/a | |
| Chen, S. [28] | RCT | NSCLC | I, IIA, III | RFA RFA | 15 15 | n/a BT | |
| Zhang. R. [72] | Meta-analysis | NSCLC | I | RFA SBRT | 1525 12,811 | n/a n/a | |
| CT-guided percutaneous MWA | |||||||
| Author | Study | Type | Stages | Groups | N | Adj. Th. | |
| Jiang. B. [74] | Meta-analysis | N/S | N/S | MWA RFA CRA | 438 946 468 | n/a n/a n/a | |
| Yuan, Z. [76] | Meta-analysis | N/S | N/S | MWA RFA | 2632 148 | n/a ChT | |
| Wei, Z. [81] | RCT ph. III | NSCLC | IIIB, IV | MWA ChT | 148 145 | ChT n/a | |
| Xu, S. [77] | RCT | NSCLC | I, II, III, IV | MWA | 304 | n/a | |
| Xu S [80] | RCT | NSCLC | I, II, III, IV | MWA | 234 | none, ChT, RT, TKI, IT | |
| Xu, S. [79] | RCT | NSCLC | I, II, III, IV | MWA | 496 | n/a | |
| Xu, S. [78] | RCT | NSCLC | I, II, III, IV | MWA | 552 | n/a | |
| CT-guided percutaneous CRA | |||||||
| Author | Study | Type | Stages | Groups | N | Adj. Th. | |
| de Baere, T. [82] | Clinical trial | mets | N/S | CRA | 40 | n/a | |
| Jiang, B. [74] | Meta-analysis | N/S | N/S | CRA RFA MWA | 468 946 438 | n/a n/a n/a | |
| Yang, W. [83] | RCT | NSCLC | III, IV | CRA CA | 41 40 | n/a n/a | |
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef]
- Ganti, A.K.; Klein, A.B.; Cotarla, I.; Seal, B.; Chou, E. Update of Incidence, Prevalence, Survival, and Initial Treatment in Patients With Non–Small Cell Lung Cancer in the US. JAMA Oncol. 2021, 7, 1824–1832. [Google Scholar] [CrossRef] [PubMed]
- Dingemans, A.C.; Früh, M.; Ardizzoni, A.; Besse, B.; Faivre-Finn, C.; Hendriks, L.E.; Lantuejoul, S.; Peters, S.; Reguart, N.; Rudin, C.M.; et al. Small-cell lung cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up(☆). Ann. Oncol. 2021, 32, 839–853. [Google Scholar] [CrossRef]
- Planchard, D.; Popat, S.; Kerr, K.; Novello, S.; Smit, E.F.; Faivre-Finn, C.; Mok, T.S.; Reck, M.; Van Schil, P.E.; Hellmann, M.D.; et al. Metastatic non-small cell lung cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2018, 29, iv192–iv237. [Google Scholar] [CrossRef]
- Remon, J.; Soria, J.C.; Peters, S. Early and locally advanced non-small-cell lung cancer: An update of the ESMO Clinical Practice Guidelines focusing on diagnosis, staging, systemic and local therapy. Ann. Oncol. 2021, 32, 1637–1642. [Google Scholar] [CrossRef]
- Baaklini, W.A.; Reinoso, M.A.; Gorin, A.B.; Sharafkaneh, A.; Manian, P. Diagnostic yield of fiberoptic bronchoscopy in evaluating solitary pulmonary nodules. Chest 2000, 117, 1049–1054. [Google Scholar] [CrossRef] [Green Version]
- van ‘t Westeinde, S.C.; Horeweg, N.; Vernhout, R.M.; Groen, H.J.M.; Lammers, J.J.; Weenink, C.; Nackaerts, K.; Oudkerk, M.; Mali, W.; Thunnissen, F.B.; et al. The role of conventional bronchoscopy in the workup of suspicious CT scan screen-detected pulmonary nodules. Chest 2012, 142, 377–384. [Google Scholar] [CrossRef]
- Ishiwata, T.; Gregor, A.; Inage, T.; Yasufuku, K. Bronchoscopic navigation and tissue diagnosis. Gen. Thorac. Cardiovasc. Surg. 2020, 68, 672–678. [Google Scholar] [CrossRef]
- Asano, F.; Eberhardt, R.; Herth, F.J. Virtual bronchoscopic navigation for peripheral pulmonary lesions. Respiration 2014, 88, 430–440. [Google Scholar] [CrossRef] [PubMed]
- Asano, F.; Shinagawa, N.; Ishida, T.; Shindoh, J.; Anzai, M.; Tsuzuku, A.; Oizumi, S.; Morita, S. Virtual bronchoscopic navigation combined with ultrathin bronchoscopy. A randomized clinical trial. Am. J. Respir. Crit. Care Med. 2013, 188, 327–333. [Google Scholar] [CrossRef] [PubMed]
- Ishida, T.; Asano, F.; Yamazaki, K.; Shinagawa, N.; Oizumi, S.; Moriya, H.; Munakata, M.; Nishimura, M. Virtual bronchoscopic navigation combined with endobronchial ultrasound to diagnose small peripheral pulmonary lesions: A randomised trial. Thorax 2011, 66, 1072–1077. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kemp, S.V. Navigation Bronchoscopy. Respiration 2020, 99, 277–286. [Google Scholar] [CrossRef] [PubMed]
- Folch, E.E.; Pritchett, M.A.; Nead, M.A.; Bowling, M.R.; Murgu, S.D.; Krimsky, W.S.; Murillo, B.A.; LeMense, G.P.; Minnich, D.J.; Bansal, S.; et al. Electromagnetic Navigation Bronchoscopy for Peripheral Pulmonary Lesions: One-Year Results of the Prospective, Multicenter NAVIGATE Study. J. Thorac. Oncol. 2019, 14, 445–458. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Herth, F.J.; Eberhardt, R.; Sterman, D.; Silvestri, G.A.; Hoffmann, H.; Shah, P.L. Bronchoscopic transparenchymal nodule access (BTPNA): First in human trial of a novel procedure for sampling solitary pulmonary nodules. Thorax 2015, 70, 326–332. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hiddinga, B.I.; Slebos, D.J.; David Koster, T.; Hijmering-Kappelle, L.B.M.; Hiltermann, T.J.N.; Kievit, H.; van der Wekken, A.J.; de Jonge, G.; Vliegenthart, R.; Van De Wauwer, C.; et al. The additional diagnostic value of virtual bronchoscopy navigation in patients with pulmonary nodules—The NAVIGATOR study. Lung Cancer 2023, 177, 37–43. [Google Scholar] [CrossRef] [PubMed]
- Agrawal, A.; Hogarth, D.K.; Murgu, S. Robotic bronchoscopy for pulmonary lesions: A review of existing technologies and clinical data. J. Thorac. Dis. 2020, 12, 3279–3286. [Google Scholar] [CrossRef] [PubMed]
- Nanjwade, B.K.; Adichwal, S.A.; Gaikwad, K.R.; Parikh, K.A.; Manvi, F.V. Pulmonary drug delivery: Novel pharmaceutical technologies breathe new life into the lungs. PDA J. Pharm. Sci. Technol. 2011, 65, 513–534. [Google Scholar] [CrossRef]
- Itoga, N.K.; Kinoshita, C.K.; Masutani, S.M.; Yamamoto, L.G. Factors Affecting Nebulized Albuterol Aerosol Particle Sizes. Ann. Emerg. Med. 2013, 62, S147–S148. [Google Scholar] [CrossRef]
- Labiris, N.R.; Dolovich, M.B. Pulmonary drug delivery. Part II: The role of inhalant delivery devices and drug formulations in therapeutic effectiveness of aerosolized medications. Br. J. Clin. Pharmacol. 2003, 56, 600–612. [Google Scholar] [CrossRef] [Green Version]
- Rosière, R.; Berghmans, T.; De Vuyst, P.; Amighi, K.; Wauthoz, N. The Position of Inhaled Chemotherapy in the Care of Patients with Lung Tumors: Clinical Feasibility and Indications According to Recent Pharmaceutical Progresses. Cancers 2019, 11, 329. [Google Scholar] [CrossRef] [Green Version]
- Hohenforst-Schmidt, W.; Zarogoulidis, P.; Darwiche, K.; Vogl, T.; Goldberg, E.P.; Huang, H.; Simoff, M.; Li, Q.; Browning, R.; Turner, F.J.; et al. Intratumoral chemotherapy for lung cancer: Re-challenge current targeted therapies. Drug Des. Devel. Ther. 2013, 7, 571–583. [Google Scholar] [CrossRef] [Green Version]
- Mehta, H.J.; Begnaud, A.; Penley, A.M.; Wynne, J.; Malhotra, P.; Fernandez-Bussy, S.; Cope, J.; Shuster, J.J.; Jantz, M.A. Restoration of Patency to Central Airways Occluded by Malignant Endobronchial Tumors Using Intratumoral Injection of Cisplatin. Ann. Am. Thorac. Soc. 2015, 12, 1345–1350. [Google Scholar] [CrossRef] [Green Version]
- Mehta, H.J.; Begnaud, A.; Penley, A.M.; Wynne, J.; Malhotra, P.; Fernandez-Bussy, S.; Cope, J.M.; Shuster, J.J.; Jantz, M.A. Treatment of isolated mediastinal and hilar recurrence of lung cancer with bronchoscopic endobronchial ultrasound guided intratumoral injection of chemotherapy with cisplatin. Lung Cancer 2015, 90, 542–547. [Google Scholar] [CrossRef]
- Yarmus, L.; Mallow, C.; Akulian, J.; Lin, C.T.; Ettinger, D.; Hales, R.; Voong, K.R.; Lee, H.; Feller-Kopman, D.; Semaan, R.; et al. Prospective Multicentered Safety and Feasibility Pilot for Endobronchial Intratumoral Chemotherapy. Chest 2019, 156, 562–570. [Google Scholar] [CrossRef]
- Melhus, C.S.; Simiele, S.J.; Aima, M.; Richardson, S. Learning from the past: A century of accuracy, aspirations, and aspersions in brachytherapy. Br. J. Radiol. 2022, 95, 20220500. [Google Scholar] [CrossRef]
- Chen, E.; Wang, J.; Zhang, H.; Zhang, Y.; Jia, C.; Min, X.; Liang, Y. Analysis of the efficacy and safety of iodine-125 seeds implantation in the treatment of patients with inoperable early-stage non-small cell lung cancer. J. Contemp. Brachytherapy 2021, 13, 347–357. [Google Scholar] [CrossRef] [PubMed]
- Li, W.; Guan, J.; Yang, L.; Zheng, X.; Yu, Y.; Jiang, J. Iodine-125 brachytherapy improved overall survival of patients with inoperable stage III/IV non-small cell lung cancer versus the conventional radiotherapy. Med. Oncol. 2015, 32, 395. [Google Scholar] [CrossRef] [PubMed]
- Chen, S.; Sheng, Z.; Huang, N. Radiofrequency Ablation Combined with Radioactive Seed Implantation for Nonsmall Cell Lung Cancer. J. Healthc. Eng. 2022, 2022, 4016081. [Google Scholar] [CrossRef] [PubMed]
- Chen, Z.K.; Fan, J.; Li, F.Q.; Zhou, S.Y.; Xu, Y.S. I-125 seeds with chemotherapy for progressive non-small-cell lung cancer after first-line treatment: A meta-analysis. J. Cardiothorac. Surg. 2022, 17, 75. [Google Scholar] [CrossRef]
- Mao, Y.; Yang, X.; Li, M.; Guo, W.; Zhang, W. Treating cancerous large airway stenosis with staging radioactive particle implantation guided by computed tomography and fiber bronchoscopy: A clinical study. World J. Surg. Oncol. 2017, 15, 149. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, X.; Wang, D. Clinical analysis of 125I seed implantation combined with epidermal growth factor receptor-tyrosine kinase inhibitors in advanced non-small cell lung cancer. J. BUON 2021, 26, 1879–1886. [Google Scholar]
- Yu, X.; Li, J.; Zhong, X.; He, J. Combination of Iodine-125 brachytherapy and chemotherapy for locally recurrent stage III non-small cell lung cancer after concurrent chemoradiotherapy. BMC Cancer 2015, 15, 656. [Google Scholar] [CrossRef] [Green Version]
- Chargari, C.; Deutsch, E.; Blanchard, P.; Gouy, S.; Martelli, H.; Guerin, F.; Dumas, I.; Bossi, A.; Morice, P.; Viswanathan, A.N.; et al. Brachytherapy: An overview for clinicians. CA Cancer J. Clin. 2019, 69, 386–401. [Google Scholar] [CrossRef] [Green Version]
- Vu, C.C.; Jawad, M.S.; Krauss, D.J. The Cost-Effectiveness and Value Proposition of Brachytherapy. Semin. Radiat. Oncol. 2020, 30, 87–93. [Google Scholar] [CrossRef]
- Xie, F.; Zheng, X.; Xiao, B.; Han, B.; Herth, F.J.F.; Sun, J. Navigation Bronchoscopy-Guided Radiofrequency Ablation for Nonsurgical Peripheral Pulmonary Tumors. Respiration 2017, 94, 293–298. [Google Scholar] [CrossRef] [PubMed]
- Ishiwata, T.; Motooka, Y.; Ujiie, H.; Inage, T.; Gregor, A.; Aragaki, M.; Chen, Z.; Kinoshita, T.; Donahoe, L.; Yeung, J.; et al. Endobronchial ultrasound-guided bipolar radiofrequency ablation for lung cancer: A first-in-human clinical trial. J. Thorac. Cardiovasc. Surg. 2022, 164, 1188–1197.e1182. [Google Scholar] [CrossRef]
- Kashiwabara, K.; Fujii, S.; Tsumura, S.; Sakamoto, K.; Semba, H. Efficacy and safety of transbronchial microwave ablation therapy under moderate sedation in malignant central airway obstruction patients with respiratory failure: A single-institution retrospective study. J. Cancer Res. Clin. Oncol. 2021, 147, 2751–2757. [Google Scholar] [CrossRef]
- Chan, J.W.Y.; Lau, R.W.H.; Ngai, J.C.L.; Tsoi, C.; Chu, C.M.; Mok, T.S.K.; Ng, C.S.H. Transbronchial microwave ablation of lung nodules with electromagnetic navigation bronchoscopy guidance-a novel technique and initial experience with 30 cases. Transl. Lung Cancer Res. 2021, 10, 1608–1622. [Google Scholar] [CrossRef] [PubMed]
- Xie, F.; Chen, J.; Jiang, Y.; Sun, J.; Hogarth, D.K.; Herth, F.J.F. Microwave ablation via a flexible catheter for the treatment of nonsurgical peripheral lung cancer: A pilot study. Thorac. Cancer 2022, 13, 1014–1020. [Google Scholar] [CrossRef]
- Erinjeri, J.P.; Clark, T.W. Cryoablation: Mechanism of action and devices. J. Vasc. Interv. Radiol. 2010, 21, S187–S191. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.H.; Choi, W.J.; Sung, S.W.; Kim, Y.K.; Kim, C.H.; Zo, J.I.; Park, K.J. Endoscopic cryotherapy of lung and bronchial tumors: A systematic review. Korean J. Intern. Med. 2011, 26, 137–144. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Lovell, J.F.; Yoon, J.; Chen, X. Clinical development and potential of photothermal and photodynamic therapies for cancer. Nat. Rev. Clin. Oncol. 2020, 17, 657–674. [Google Scholar] [CrossRef] [PubMed]
- Furuse, K.; Fukuoka, M.; Kato, H.; Horai, T.; Kubota, K.; Kodama, N.; Kusunoki, Y.; Takifuji, N.; Okunaka, T.; Konaka, C.; et al. A prospective phase II study on photodynamic therapy with photofrin II for centrally located early-stage lung cancer. The Japan Lung Cancer Photodynamic Therapy Study Group. J. Clin. Oncol. 1993, 11, 1852–1857. [Google Scholar] [CrossRef] [PubMed]
- Dhillon, S.S.; Demmy, T.L.; Yendamuri, S.; Loewen, G.; Nwogu, C.; Cooper, M.; Henderson, B.W. A Phase I Study of Light Dose for Photodynamic Therapy Using 2-[1-Hexyloxyethyl]-2 Devinyl Pyropheophorbide-a for the Treatment of Non-Small Cell Carcinoma In Situ or Non-Small Cell Microinvasive Bronchogenic Carcinoma: A Dose Ranging Study. J. Thorac. Oncol. 2016, 11, 234–241. [Google Scholar] [CrossRef] [Green Version]
- Kato, H.; Furukawa, K.; Sato, M.; Okunaka, T.; Kusunoki, Y.; Kawahara, M.; Fukuoka, M.; Miyazawa, T.; Yana, T.; Matsui, K.; et al. Phase II clinical study of photodynamic therapy using mono-L-aspartyl chlorin e6 and diode laser for early superficial squamous cell carcinoma of the lung. Lung Cancer 2003, 42, 103–111. [Google Scholar] [CrossRef]
- Ji, W.; Yoo, J.W.; Bae, E.K.; Lee, J.H.; Choi, C.M. The effect of Radachlorin® PDT in advanced NSCLC: A pilot study. Photodiagnosis Photodyn. Ther. 2013, 10, 120–126. [Google Scholar] [CrossRef]
- Lin, C.; Zhang, Y.; Zhao, Q.; Sun, P.; Gao, Z.; Cui, S. Analysis of the short-term effect of photodynamic therapy on primary bronchial lung cancer. Lasers Med. Sci. 2021, 36, 753–761. [Google Scholar] [CrossRef] [PubMed]
- McCaughan, J.S., Jr.; Williams, T.E. Photodynamic therapy for endobronchial malignant disease: A prospective fourteen-year study. J. Thorac. Cardiovasc. Surg. 1997, 114, 940–946; discussion 946–947. [Google Scholar] [CrossRef] [Green Version]
- Wang, K.; Yu, B.; Pathak, J.L. An update in clinical utilization of photodynamic therapy for lung cancer. J. Cancer 2021, 12, 1154–1160. [Google Scholar] [CrossRef]
- Nakanishi, M.; Yoshida, Y.; Natazuka, T. Prospective study of transarterial infusion of docetaxel and cisplatin to treat non-small-cell lung cancer in patients contraindicated for standard chemotherapy. Lung Cancer 2012, 77, 353–358. [Google Scholar] [CrossRef] [PubMed]
- Xiong, F.; Xie, Y.J.; Yang, N.; He, Q.; Feng, Z.Z.; Liu, B.Q.; Guan, Y.-S. Bronchial arterial infusion chemotherapy combined with icotinib hydrochloride to treat advanced non-small-cell-lung cancer: A randomised controlled trial. Respir. Med. 2017, 132, 276. [Google Scholar] [CrossRef]
- Zhu, J.; Zhang, H.P.; Jiang, S.; Ni, J. Neoadjuvant chemotherapy by bronchial arterial infusion in patients with unresectable stage III squamous cell lung cancer. Ther. Adv. Respir. Dis. 2017, 11, 301–309. [Google Scholar] [CrossRef]
- van Putte, B.P.; Grootenboers, M.; van Boven, W.J.; Hendriks, J.M.; van Schil, P.E.; Guetens, G.; De Boeck, G.; Pasterkamp, G.; Schramel, F.; Folkerts, G. Pharmacokinetics of gemcitabine when delivered by selective pulmonary artery perfusion for the treatment of lung cancer. Drug Metab. Dispos. 2008, 36, 676–681. [Google Scholar] [CrossRef] [Green Version]
- Grootenboers, M.J.; Schramel, F.M.; van Boven, W.J.; Hendriks, J.M.; van Schil, P.E.; De Wit, P.E.; Pasterkamp, G.; Folkerts, G.; van Putte, B.P. Selective pulmonary artery perfusion followed by blood flow occlusion: New challenge for the treatment of pulmonary malignancies. Lung Cancer 2009, 63, 400–404. [Google Scholar] [CrossRef]
- van Putte, B.P.; Grootenboers, M.; van Boven, W.J.; van Oosterhout, M.; Pasterkamp, G.; Folkerts, G.; Schramel, F. Selective pulmonary artery perfusion for the treatment of primary lung cancer: Improved drug exposure of the lung. Lung Cancer 2009, 65, 208–213. [Google Scholar] [CrossRef] [PubMed]
- Sparks, P.J.; Hines, J.; Lowry, J.; Strode, M.; Roach, M. Selective Pulmonary Artery Perfusion With Blood Flow Occlusion Delivers Concentrated Levels of Chemotherapy to Ipsilateral Hilar and Mediastinal Lymph Nodes. World J. Oncol. 2014, 5, 1–6. [Google Scholar] [CrossRef]
- Schicho, A.; Hellerbrand, C.; Krüger, K.; Beyer, L.P.; Wohlgemuth, W.; Niessen, C.; Hohenstein, E.; Stroszczynski, C.; Pereira, P.L.; Wiggermann, P. Impact of Different Embolic Agents for Transarterial Chemoembolization (TACE) Procedures on Systemic Vascular Endothelial Growth Factor (VEGF) Levels. J. Clin. Transl. Hepatol. 2016, 4, 288–292. [Google Scholar] [CrossRef] [Green Version]
- Jin, S.Q.; Zhao, H.Y.; Bai, B.; Ma, C.H.; Cao, H.L. Transcatheter arterial chemoembolization improves clinical efficacy and life quality of patients with lung cancer and reduces adverse reactions. Am. J. Transl. Res. 2021, 13, 10396–10403. [Google Scholar] [PubMed]
- Boas, F.E.; Kemeny, N.E.; Sofocleous, C.T.; Yeh, R.; Thompson, V.R.; Hsu, M.; Moskowitz, C.S.; Ziv, E.; Yarmohammadi, H.; Bendet, A.; et al. Bronchial or Pulmonary Artery Chemoembolization for Unresectable and Unablatable Lung Metastases: A Phase I Clinical Trial. Radiology 2021, 301, 474–484. [Google Scholar] [CrossRef] [PubMed]
- Vogl, T.J.; Lehnert, T.; Zangos, S.; Eichler, K.; Hammerstingl, R.; Korkusuz, H.; Lindemayr, S. Transpulmonary chemoembolization (TPCE) as a treatment for unresectable lung metastases. Eur. Radiol. 2008, 18, 2449–2455. [Google Scholar] [CrossRef] [PubMed]
- Chang, L.; Wang, W.; Jiang, N.; Rao, F.; Gong, C.; Wu, P.; Yang, J.; Liu, Z.; Guo, T. Dexamethasone prevents TACE-induced adverse events: A meta-analysis. Medicine 2020, 99, e23191. [Google Scholar] [CrossRef]
- Den Hengst, W.A.; Van Putte, B.P.; Hendriks, J.M.; Stockman, B.; van Boven, W.J.; Weyler, J.; Schramel, F.M.; Van Schil, P.E. Long-term survival of a phase I clinical trial of isolated lung perfusion with melphalan for resectable lung metastases. Eur. J. Cardiothorac. Surg. 2010, 38, 621–627. [Google Scholar] [CrossRef] [Green Version]
- den Hengst, W.A.; Hendriks, J.M.; Balduyck, B.; Rodrigus, I.; Vermorken, J.B.; Lardon, F.; Versteegh, M.I.; Braun, J.; Gelderblom, H.; Schramel, F.M.; et al. Phase II multicenter clinical trial of pulmonary metastasectomy and isolated lung perfusion with melphalan in patients with resectable lung metastases. J. Thorac. Oncol. 2014, 9, 1547–1553. [Google Scholar] [CrossRef] [Green Version]
- Beckers, P.A.J.; Versteegh, M.I.M.; Van Brakel, T.J.; Braun, J.; Van Putte, B.; Maat, A.; Vergauwen, W.; Rodrigus, I.; Den Hengst, W.; Lardon, F.; et al. Multicenter Phase II Clinical Trial of Isolated Lung Perfusion in Patients With Lung Metastases. Ann. Thorac. Surg. 2019, 108, 167–174. [Google Scholar] [CrossRef]
- Burt, M.E.; Liu, D.; Abolhoda, A.; Ross, H.M.; Kaneda, Y.; Jara, E.; Casper, E.S.; Ginsberg, R.J.; Brennan, M.F. Isolated lung perfusion for patients with unresectable metastases from sarcoma: A phase I trial. Ann. Thorac. Surg. 2000, 69, 1542–1549. [Google Scholar] [CrossRef] [PubMed]
- Grootenboers, M.J.; Hendriks, J.M.; van Boven, W.J.; Knibbe, C.A.; van Putte, B.; Stockman, B.; De Bruijn, E.; Vermorken, J.B.; Van Schil, P.E.; Schramel, F.M. Pharmacokinetics of isolated lung perfusion with melphalan for resectable pulmonary metastases, a phase I and extension trial. J. Surg. Oncol. 2007, 96, 583–589. [Google Scholar] [CrossRef]
- Hendriks, J.M.; Grootenboers, M.J.; Schramel, F.M.; van Boven, W.J.; Stockman, B.; Seldenrijk, C.A.; ten Broecke, P.; Knibbe, C.A.; Slee, P.; De Bruijn, E.; et al. Isolated lung perfusion with melphalan for resectable lung metastases: A phase I clinical trial. Ann. Thorac. Surg. 2004, 78, 1919–1926; discussion 1926–1927. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Demmy, T.L.; Wagner-Mann, C.; Allen, A. Isolated lung chemotherapeutic infusions for treatment of pulmonary metastases: A pilot study. J. Biomed. Sci. 2002, 9, 334–338. [Google Scholar] [CrossRef] [PubMed]
- Demmy, T.L.; Tomaszewski, G.; Dy, G.K.; Yendamuri, S.; Nwogu, C.; Pendyala, L.; Ramnath, N.; Adjei, A.A. Thoracoscopic organ suffusion for regional lung chemotherapy (preliminary results). Ann. Thorac. Surg. 2009, 88, 385–390; discussion 390–391. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Z.R.; Lau, R.W.H.; Ng, C.S.H. Catheter-based alternative treatment for early-stage lung cancer with a high-risk for morbidity. J. Thorac. Dis. 2018, 10, S1864–S1870. [Google Scholar] [CrossRef] [PubMed]
- Alexander, E.S.; Xiong, L.; Baird, G.L.; Fernando, H.; Dupuy, D.E. CT Densitometry and Morphology of Radiofrequency-Ablated Stage IA Non-Small Cell Lung Cancer: Results from the American College of Surgeons Oncology Group Z4033 (Alliance) Trial. J. Vasc. Interv. Radiol. 2020, 31, 286–293. [Google Scholar] [CrossRef]
- Zhang, R.; Kang, J.; Ren, S.; Xing, L.; Xu, Y. Comparison of stereotactic body radiotherapy and radiofrequency ablation for early-stage non-small cell lung cancer: A systematic review and meta-analysis. Ann. Transl. Med. 2022, 10, 104. [Google Scholar] [CrossRef] [PubMed]
- Li, G.; Xue, M.; Chen, W.; Yi, S. Efficacy and safety of radiofrequency ablation for lung cancers: A systematic review and meta-analysis. Eur. J. Radiol. 2018, 100, 92–98. [Google Scholar] [CrossRef] [PubMed]
- Jiang, B.; McClure, M.A.; Chen, T.; Chen, S. Efficacy and safety of thermal ablation of lung malignancies: A Network meta-analysis. Ann. Thorac. Med. 2018, 13, 243–250. [Google Scholar] [CrossRef] [PubMed]
- Palussière, J.; Chomy, F.; Savina, M.; Deschamps, F.; Gaubert, J.Y.; Renault, A.; Bonnefoy, O.; Laurent, F.; Meunier, C.; Bellera, C.; et al. Radiofrequency ablation of stage IA non-small cell lung cancer in patients ineligible for surgery: Results of a prospective multicenter phase II trial. J. Cardiothorac. Surg. 2018, 13, 91. [Google Scholar] [CrossRef] [Green Version]
- Yuan, Z.; Wang, Y.; Zhang, J.; Zheng, J.; Li, W. A Meta-Analysis of Clinical Outcomes After Radiofrequency Ablation and Microwave Ablation for Lung Cancer and Pulmonary Metastases. J. Am. Coll. Radiol. 2019, 16, 302–314. [Google Scholar] [CrossRef] [PubMed]
- Xu, S.; Qi, J.; Bie, Z.X.; Li, Y.M.; Li, B.; Guo, R.Q.; Li, X.G. Local progression after computed tomography-guided microwave ablation in non-small cell lung cancer patients: Prediction using a nomogram model. Int. J. Hyperthermia 2021, 38, 1366–1374. [Google Scholar] [CrossRef] [PubMed]
- Xu, S.; Qi, J.; Li, B.; Bie, Z.X.; Li, Y.M.; Li, X.G. Risk prediction of pneumothorax in lung malignancy patients treated with percutaneous microwave ablation: Development of nomogram model. Int. J. Hyperthermia 2021, 38, 488–497. [Google Scholar] [CrossRef]
- Xu, S.; Qi, J.; Li, B.; Bie, Z.X.; Li, Y.M.; Li, X.G. Risk prediction of pleural effusion in lung malignancy patients treated with CT-guided percutaneous microwave ablation: A nomogram and artificial neural network model. Int. J. Hyperthermia 2021, 38, 220–228. [Google Scholar] [CrossRef] [PubMed]
- Xu, S.; Qi, J.; Li, B.; Li, X.G. Survival prediction for non-small cell lung cancer patients treated with CT-guided microwave ablation: Development of a prognostic nomogram. Int. J. Hyperthermia 2021, 38, 640–649. [Google Scholar] [CrossRef]
- Wei, Z.; Yang, X.; Ye, X.; Feng, Q.; Xu, Y.; Zhang, L.; Sun, W.; Dong, Y.; Meng, Q.; Li, T.; et al. Microwave ablation plus chemotherapy versus chemotherapy in advanced non-small cell lung cancer: A multicenter, randomized, controlled, phase III clinical trial. Eur. Radiol. 2020, 30, 2692–2702. [Google Scholar] [CrossRef] [PubMed]
- de Baere, T.; Tselikas, L.; Woodrum, D.; Abtin, F.; Littrup, P.; Deschamps, F.; Suh, R.; Aoun, H.D.; Callstrom, M. Evaluating Cryoablation of Metastatic Lung Tumors in Patients--Safety and Efficacy: The ECLIPSE Trial--Interim Analysis at 1 Year. J. Thorac. Oncol. 2015, 10, 1468–1474. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, W.; An, Y.; Li, Q.; Liu, C.; Zhu, B.; Huang, Q.; Zhao, M.; Yang, F.; Feng, H.; Hu, K. Co-ablation versus cryoablation for the treatment of stage III-IV non-small cell lung cancer: A prospective, noninferiority, randomized, controlled trial (RCT). Thorac. Cancer 2021, 12, 475–483. [Google Scholar] [CrossRef] [PubMed]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Claes, E.; Wener, R.; Neyrinck, A.P.; Coppens, A.; Van Schil, P.E.; Janssens, A.; Lapperre, T.S.; Snoeckx, A.; Wen, W.; Voet, H.; et al. Innovative Invasive Loco-Regional Techniques for the Treatment of Lung Cancer. Cancers 2023, 15, 2244. https://doi.org/10.3390/cancers15082244
Claes E, Wener R, Neyrinck AP, Coppens A, Van Schil PE, Janssens A, Lapperre TS, Snoeckx A, Wen W, Voet H, et al. Innovative Invasive Loco-Regional Techniques for the Treatment of Lung Cancer. Cancers. 2023; 15(8):2244. https://doi.org/10.3390/cancers15082244
Chicago/Turabian StyleClaes, Erik, Reinier Wener, Arne P. Neyrinck, Axelle Coppens, Paul E. Van Schil, Annelies Janssens, Thérèse S. Lapperre, Annemiek Snoeckx, Wen Wen, Hanne Voet, and et al. 2023. "Innovative Invasive Loco-Regional Techniques for the Treatment of Lung Cancer" Cancers 15, no. 8: 2244. https://doi.org/10.3390/cancers15082244
APA StyleClaes, E., Wener, R., Neyrinck, A. P., Coppens, A., Van Schil, P. E., Janssens, A., Lapperre, T. S., Snoeckx, A., Wen, W., Voet, H., Verleden, S. E., & Hendriks, J. M. H. (2023). Innovative Invasive Loco-Regional Techniques for the Treatment of Lung Cancer. Cancers, 15(8), 2244. https://doi.org/10.3390/cancers15082244