
Surgical Anatomy and Approaches of the Anterior Cranial Fossa from a Transcranial and Endonasal Perspective

 ,
,  ,
, {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:Simple Summary
Abstract
1. Introduction
2. Method
3. Results
3.1. Anterior Cranial Fossa Anatomy
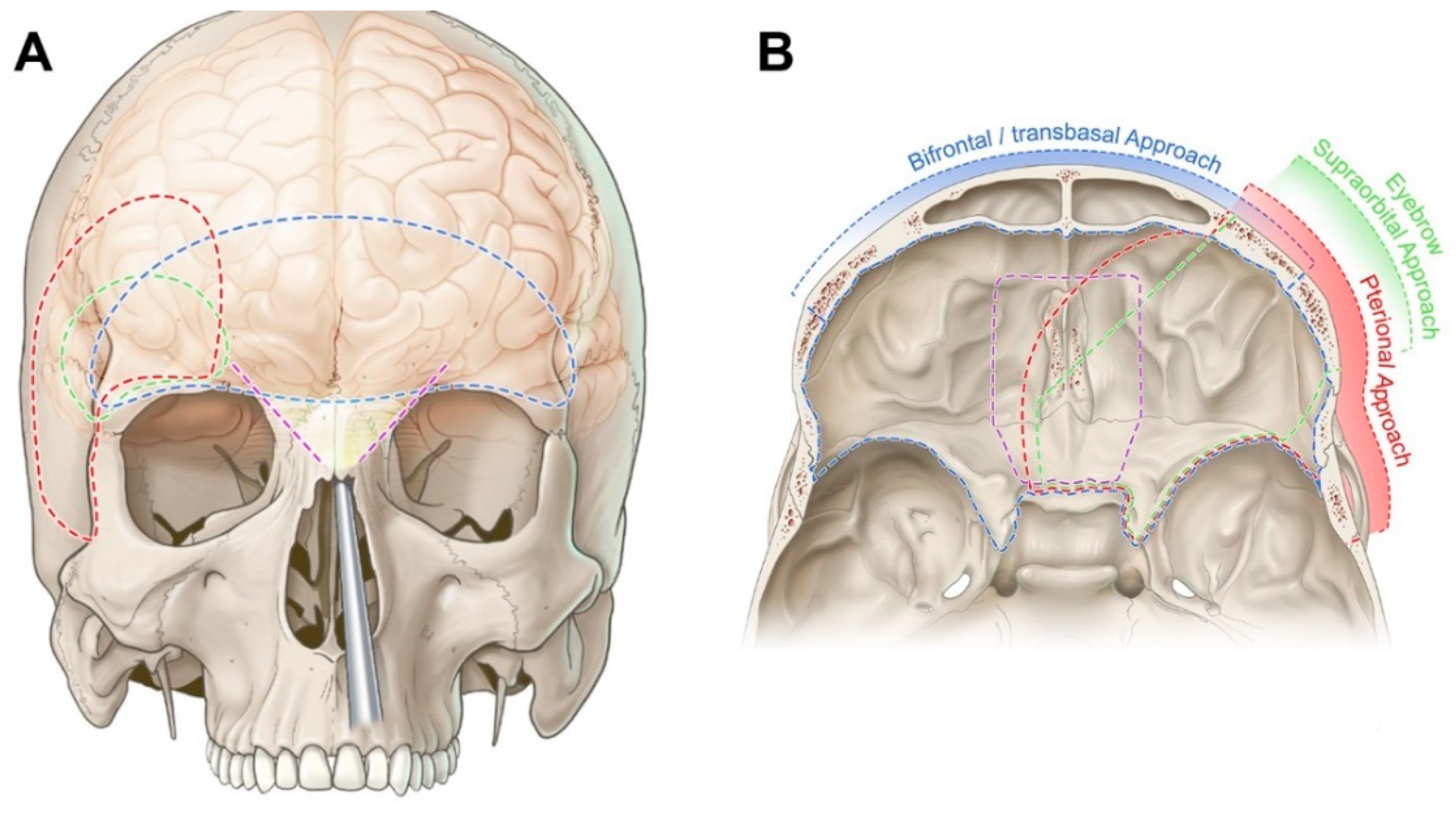
3.2. Transcranial Approaches to the Anterior Cranial Fossa
3.2.1. Bifrontal/Transbasal Approach
3.2.2. Pterional Approach
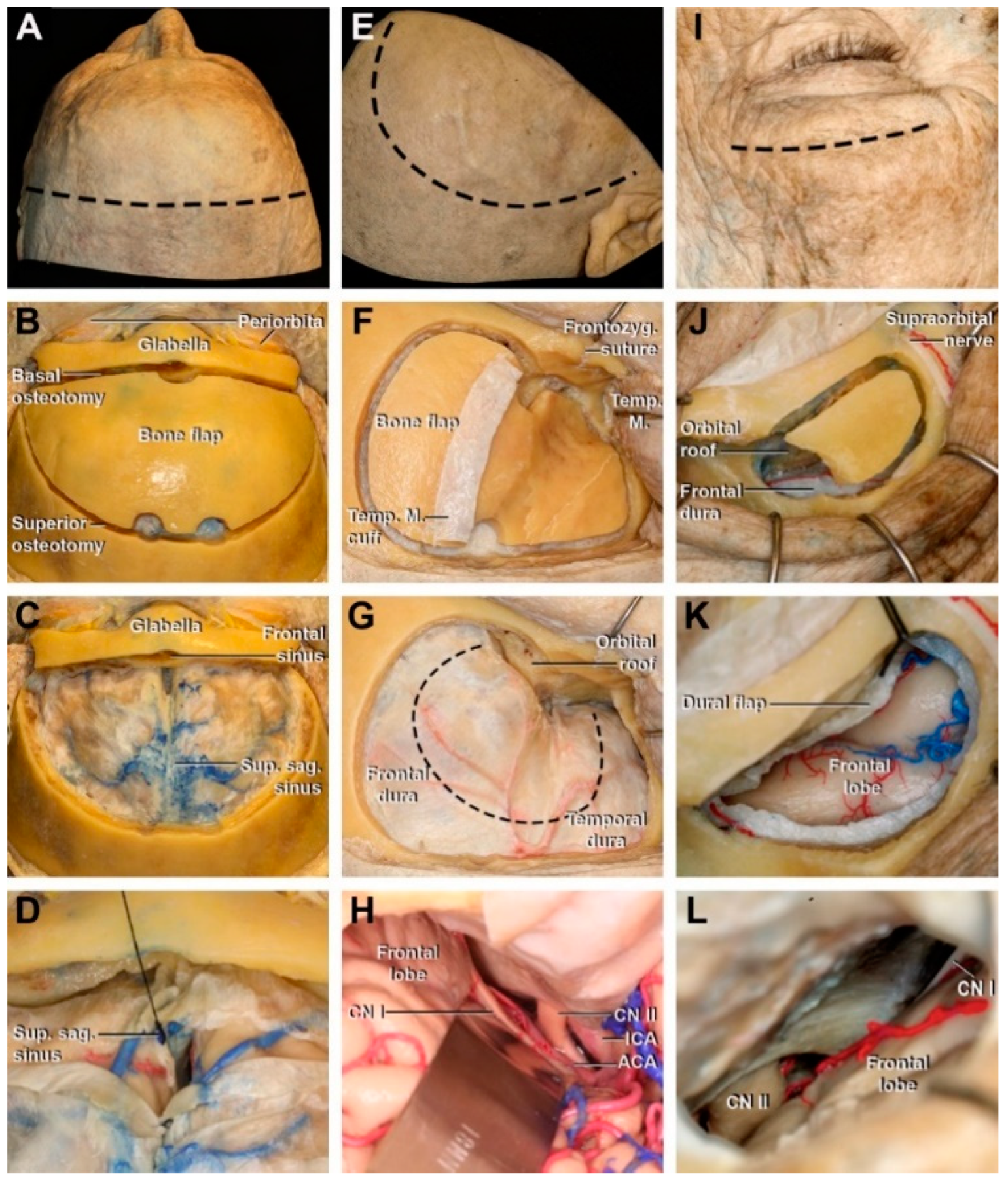
3.2.3. Eyebrow Supraorbital Approach
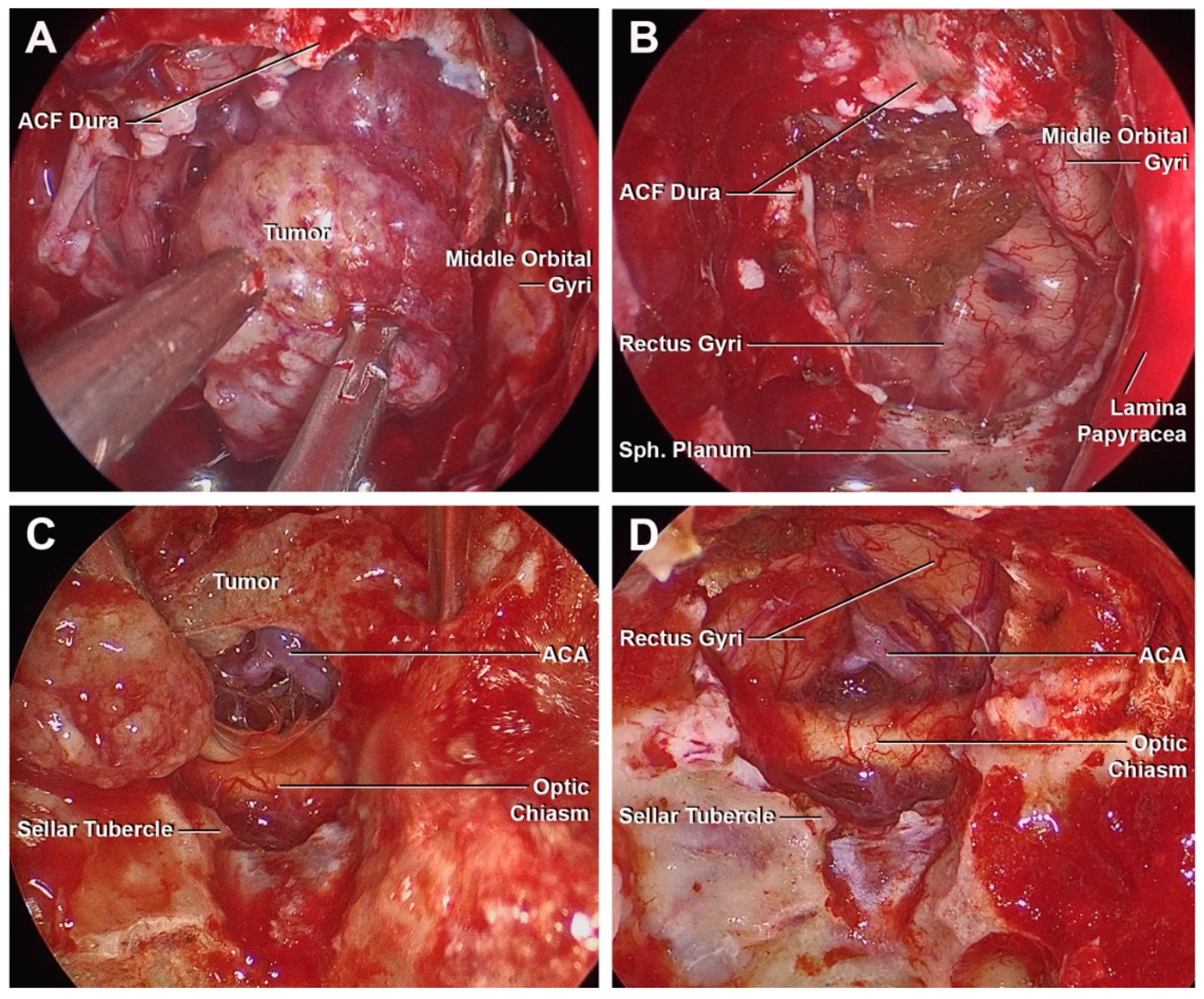
3.3. Endonasal Endoscopic Approach
3.4. Illustrative Cases
3.4.1. Case 1
3.4.2. Case 2
3.4.3. Case 3
3.4.4. Case 4
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Rhoton, A.L., Jr. The anterior and middle cranial base. Neurosurgery 2002, 51, S273–S302. [Google Scholar] [CrossRef] [PubMed]
- Bloch, O.; Demonte, F. Malignant tumors of the skull base. Preface. Neurosurg. Clin. N. Am. 2013, 24, xi–xii. [Google Scholar] [CrossRef] [PubMed]
- Ivan, M.E.; Han, S.J.; Aghi, M.K. Tumors of the anterior skull base. Expert. Rev. Neurother. 2014, 14, 425–438. [Google Scholar] [CrossRef]
- Mirimanoff, R.O.; Dosoretz, D.E.; Linggood, R.M.; Ojemann, R.G.; Martuza, R.L. Meningioma: Analysis of recurrence and progression following neurosurgical resection. J. Neurosurg. 1985, 62, 18–24. [Google Scholar] [CrossRef] [PubMed]
- Simmonds, J.C.; Rebeiz, E.E. Surgical resection of sinonasal hemangiopericytoma involving anterior skull base: Case reports and literature review. Am. J. Otolaryngol. 2017, 38, 87–91. [Google Scholar] [CrossRef] [PubMed]
- Vrionis, F.D.; Kienstra, M.A.; Rivera, M.; Padhya, T.A. Malignant tumors of the anterior skull base. Cancer Control 2004, 11, 144–151. [Google Scholar] [CrossRef]
- Rachinger, W.; Grau, S.; Tonn, J.C. Different microsurgical approaches to meningiomas of the anterior cranial base. Acta Neurochir. 2010, 152, 931–939. [Google Scholar] [CrossRef]
- Van Lindert, E.; Perneczky, A.; Fries, G.; Pierangeli, E. The supraorbital keyhole approach to supratentorial aneurysms: Concept and technique. Surg. Neurol. 1998, 49, 481–490. [Google Scholar] [CrossRef]
- Sánchez-Vázquez, M.A.; Barrera-Calatayud, P.; Mejia-Villela, M.; Palma-Silva, J.F.; Juan-Carachure, I.; Gomez-Aguilar, J.M.; Sanchez-Herrera, F. Transciliary subfrontal craniotomy for anterior skull base lesions. Technical note. J. Neurosurg. 1999, 91, 892–896. [Google Scholar] [CrossRef] [PubMed]
- Hirsch, O. Endonasal method of removal of hyoiphyseal tumors with report of two successful cases. JAMA 1910, 55, 772. [Google Scholar] [CrossRef]
- Pia, H.W. The microscope in neurosurgery—Technical improvements. Acta Neurochir. 1972, 26, 251–255. [Google Scholar] [CrossRef]
- Runnels, J.B. Microneurosurgery. The use of the operating binocular microscope. J. Kans. Med. Soc. 1974, 75, 40–41. [Google Scholar]
- Carrau, R.L.; Jho, H.D.; Ko, Y. Transnasal-transsphenoidal endoscopic surgery of the pituitary gland. Laryngoscope 1996, 106, 914–918. [Google Scholar] [CrossRef] [PubMed]
- Kassam, A.; Snyderman, C.H.; Mintz, A.; Gardner, P.; Carrau, R.L. Expanded endonasal approach: The rostrocaudal axis. Part, I. Crista galli to the sella turcica. Neurosurg. Focus 2005, 19, E3. [Google Scholar] [CrossRef]
- Patel, C.R.; Fernandez-Miranda, J.C.; Wang, W.H.; Wang, E.W. Skull Base Anatomy. Otolaryngol. Clin. N. Am. 2016, 49, 9–20. [Google Scholar] [CrossRef]
- Dehdashti, A.R.; Ganna, A.; Witterick, I.; Gentili, F. Expanded endoscopic endonasal approach for anterior cranial base and suprasellar lesions: Indications and limitations. Neurosurgery 2009, 64, 677–689. [Google Scholar] [CrossRef] [PubMed]
- Lee, W.C.; Ming Ku, P.K.; van Hasselt, C.A. New guidelines for endoscopic localization of the anterior ethmoidal artery: A cadaveric study. Laryngoscope 2000, 110, 1173–1178. [Google Scholar] [CrossRef] [PubMed]
- Frazier, C.H.I. An Approach to the Hypophysis through the Anterior Cranial Fossa. Ann. Surg. 1913, 57, 145–150. [Google Scholar] [CrossRef]
- Ng, A.F.; Quintero, R.B.; Muftah Lahirish, I.A.; Holanda, V.; Neto, M.R.; De Oliveira, E. Microsurgical Anatomy Review of Bifrontal Limited Transbasal Approach—Quantitative and Anatomy Study. World Neurosurg. 2020, 141, e1–e8. [Google Scholar] [CrossRef]
- Yaşargil, M.G.; Fox, J.L.; Ray, M.W. The Operative Approach to Aneurysms of the Anterior Communicating Artery. In Advances and Technical Standards in Neurosurgery—Volume 2. Advances and Technical Standards in Neurosurgery; Springer: Vienna, Austria, 1975; Volume 2. [Google Scholar]
- Hassler, W.; Zentner, J. Pterional approach for surgical treatment of olfactory groove meningiomas. Neurosurgery 1989, 25, 942–947. [Google Scholar] [CrossRef]
- Borghei-Razavi, H.; Eguiluz-Melendez, A.; Wenping, X.; Truong, H.Q.; Fernandes-Cabral, D.; Najera, E.; Stefko, T.; Fernandez-Miranda, J.C.; Gardner, P.A. Surgical Limitations of the Microscopic Transciliary Supraorbital Keyhole Approach to the Anterior and Middle Skull Base. World Neurosurg. 2022, 167, e1440–e1447. [Google Scholar] [CrossRef]
- Pinheiro-Neto, C.D.; Prevedello, D.M.; Carrau, R.L.; Snyderman, C.H.; Mintz, A.; Gardner, P.; Kassam, A. Improving the design of the pedicled nasoseptal flap for skull base reconstruction: A radioanatomic study. Laryngoscope 2007, 117, 1560–1569. [Google Scholar] [CrossRef] [PubMed]
- De Divitiis, E.; Esposito, F.; Cappabianca, P.; Cavallo, L.M.; de Divitiis, O.; Esposito, I. Endoscopic transnasal resection of anterior cranial fossa meningiomas. Neurosurg. Focus 2008, 25, E8. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.K.; Hattar, E.; Eloy, J.A. Endoscopic Endonasal Approach for Olfactory Groove Meningiomas: Operative Technique and Nuances. Neurosurg. Clin. N. Am. 2015, 26, 377–388. [Google Scholar] [CrossRef] [PubMed]
- Koutourousiou, M.; Fernandez-Miranda, J.C.; Wang, E.W.; Snyderman, C.H.; Gardner, P.A. Endoscopic endonasal surgery for olfactory groove meningiomas: Outcomes and limitations in 50 patients. Neurosurg. Focus 2014, 37, E8. [Google Scholar] [CrossRef]
- Pinheiro-Neto, C.D.; Scopel, T.F.; Kenning, T.J.; Peris-Celda, M. Transcribriform Approach: Surgical Anatomy (Step-by-Step). In Transnasal Endoscopic Skull Base and Brain Surgery, 2nd ed.; Aldo, C., Mangussi-Gomes, S.J., Eds.; Thieme Publishers: Rio de Janeiro, Brazil, 2019. [Google Scholar]
- Peris Celda, M.; Kenning, T.; Pinheiro-Neto, C.D. Endoscopic Superior Ethmoidal Approach for Anterior Cranial Base Resection: Tailoring the Approach for Maximum Exposure with Preservation of Nasal Structures. World Neurosurg. 2017, 104, 311–317. [Google Scholar] [CrossRef]
- Vanaclocha, V.; Saiz-Sapena, N. Surgical treatment of anterior skull base tumours. Acta Neurochir. 1997, 139, 857–868. [Google Scholar] [CrossRef]
- Spektor, S.; Valarezo, J.; Fliss, D.M.; Gil, Z.; Cohen, J.; Goldman, J.; Umansky, F. Olfactory groove meningiomas from neurosurgical and ear, nose, and throat perspectives: Approaches, techniques, and outcomes. Neurosurgery 2005, 57 (Suppl. S4), 268–280. [Google Scholar] [CrossRef]
- DeMonte, F. Surgical treatment of anterior basal meningiomas. J. Neurooncol. 1996, 29, 239–248. [Google Scholar] [CrossRef]
- Bassiouni, H.; Asgari, S.; Stolke, D. Olfactory groove meningiomas: Functional outcome in a series treated microsurgically. Acta Neurochir. 2007, 149, 109–121. [Google Scholar] [CrossRef]
- Rubin, G.; Ben David, U.; Gornish, M.; Rappaport, Z.H. Meningiomas of the anterior cranial fossa floor. Review of 67 cases. Acta Neurochir. 1994, 129, 26–30. [Google Scholar] [CrossRef] [PubMed]
- Nakamura, M.; Struck, M.; Roser, F.; Vorkapic, P.; Samii, M. Olfactory groove meningiomas: Clinical outcome and recurrence rates after tumor removal through the frontolateral and bifrontal approach. Neurosurgery 2008, 62 (Suppl. S3), 1224–1232. [Google Scholar] [CrossRef]
- Chi, J.H.; Parsa, A.T.; Berger, M.S.; Kunwar, S.; McDermott, M.W. Extended bifrontal craniotomy for midline anterior fossa meningiomas: Minimization of retraction-related edema and surgical outcomes. Neurosurgery 2006, 59 (Suppl. 2), ONS426–ONS434. [Google Scholar] [CrossRef]
- Hentschel, S.J.; DeMonte, F. Olfactory groove meningiomas. Neurosurg. Focus 2003, 14, e4. [Google Scholar] [CrossRef]
- Morales-Valero, S.F.; Van Gompel, J.J.; Loumiotis, I.; Lanzino, G. Craniotomy for anterior cranial fossa meningiomas: Historical overview. Neurosurg. Focus 2014, 36, E14. [Google Scholar] [CrossRef]
- Turazzi, S.; Cristofori, L.; Gambin, R.; Bricolo, A. The pterional approach for the microsurgical removal of olfactory groove meningiomas. Neurosurgery 1999, 45, 821–826. [Google Scholar] [CrossRef]
- Da Costa, M.D.S.; Hardesty, D.A.; Priddy, B.; Noiphithak, R.; Revuelta Barbero, J.M.; Prevedello, D.M. Extended Supraorbital Approach with Modified Eyebrow Incision: Technical Note. World Neurosurg. 2019, 128, 354–359. [Google Scholar] [CrossRef] [PubMed]
- Hadad, G.; Bassagasteguy, L.; Carrau, R.L.; Mataza, J.C.; Kassam, A.; Snyderman, C.H.; Mintz, A. A novel reconstructive technique after endoscopic expanded endonasal approaches: Vascular pedicle nasoseptal flap. Laryngoscope 2006, 116, 1882–1886. [Google Scholar] [CrossRef] [PubMed]
- Gardner, P.A.; Kassam, A.B.; Thomas, A.; Snyderman, C.H.; Carrau, R.L.; Mintz, A.H.; Prevedello, D.M. Endoscopic endonasal resection of anterior cranial base meningiomas. Neurosurgery 2008, 63, 36–54. [Google Scholar] [CrossRef]
- Pinheiro-Neto, C.D.; Peris-Celda, M.; Kenning, T. Extrapolating the Limits of the Nasoseptal Flap with Pedicle Dissection to the Internal Maxillary Artery. Oper. Neurosurg. 2019, 16, 37–44. [Google Scholar] [CrossRef]
- Choby, G.; Rabinowitz, M.R.; Patel, Z.M.; McKinney, K.A.; Del Signore, A.G.; Ebert, C.S., Jr.; Thorp, B.D.; Wang, E.W. Emerging concepts in endoscopic skull base surgery training. Int. Forum. Allergy Rhinol. 2021, 11, 1611–1616. [Google Scholar] [CrossRef]
- Fernandez-Miranda, J.C.; Gardner, P.A.; Prevedello, D.M.; Kassam, A.B. Expanded endonasal approach for olfactory groove meningioma. Acta Neurochir. 2009, 151, 287–290. [Google Scholar] [CrossRef]
- Pinheiro-Neto, C.; Rowan, N.R.; Celda, M.P.; Mukherjee, D.; Gompel, J.J.V.; Choby, G. Optimizing Quality of Life and Minimizing Morbidity through Nasal Preservation in Endoscopic Skull Base Surgery: A Contemporary Review. J. Neurol. Surg. B Skull Base 2022, 83, 602–610. [Google Scholar] [CrossRef] [PubMed]
- Kassam, A.B.; Carrau, R.L.; Snyderman, C.H.; Thomas, A.; Vescan, A.; Prevedello, D.; Mintz, A.; Gardner, P. Endoscopic reconstruction of the cranial base using a pedicled nasoseptal flap. Neurosurgery 2008, 63 (Suppl. S1), ONS44–ONS53. [Google Scholar] [CrossRef]
- Kassam, A.B.; Prevedello, D.M.; Carrau, R.L.; Snyderman, C.H.; Thomas, A.; Gardner, P.; Zanation, A.; Duz, B.; Stefko, S.T.; Byers, K.; et al. Endoscopic endonasal skull base surgery: Analysis of complications in the authors’ initial 800 patients. J. Neurosurg. 2011, 114, 1544–1568. [Google Scholar] [CrossRef]
- Conger, A.; Zhao, F.; Wang, X.; Eisenberg, A.; Griffiths, C.; Esposito, F.; Carrau, R.L.; Barkhoudarian, G.; Kelly, D.F. Evolution of the graded repair of CSF leaks and skull base defects in endonasal endoscopic tumor surgery: Trends in repair failure and meningitis rates in 509 patients. J. Neurosurg. 2018, 130, 861–875. [Google Scholar] [CrossRef] [PubMed]
- Lee, I.H.; Kim, D.H.; Park, J.S.; Jeun, S.S.; Hong, Y.K.; Kim, S.W. Cerebrospinal fluid leakage repair of various grades developing during endoscopic transnasal transsphenoidal surgery. PLoS ONE 2021, 16, e0248229. [Google Scholar] [CrossRef] [PubMed]
- Dolci, R.L.L.; Miyake, M.M.; Tateno, D.A.; Cançado, N.A.; Campos, C.A.C.; dos Santos, A.R.L.; Lazarini, P.R. Postoperative otorhinolaryngologic complications in transnasal endoscopic surgery to access the skull base. Braz. J. Otorhinolaryngol. 2017, 83, 349–355. [Google Scholar] [CrossRef] [PubMed]
- Houser, S.M. Empty nose syndrome associated with middle turbinate resection. Otolaryngol. Head. Neck Surg. 2006, 135, 972–973. [Google Scholar] [CrossRef]
- Casler, J.D.; Doolittle, A.M.; Mair, E.A. Endoscopic surgery of the anterior skull base. Laryngoscope 2005, 115, 16–24. [Google Scholar] [CrossRef]
- Plou, P.; Boccalatte, L.; Padilla-Lichtenberger, F.; Figari, M.; Ajler, P.; Larrañaga, J. Microsurgical free flaps for skull base reconstruction following tumor resection: Available techniques and complications. Neurocirugia 2023, 34, 22–31. [Google Scholar] [CrossRef]
- Louis, D.N.; Perry, A.; Wesseling, P.; Brat, D.J.; Cree, I.A.; Figarella-Branger, D.; Hawkins, C.; Ng, H.K.; Pfister, S.M.; Reifenberger, G.; et al. The 2021 WHO Classification of Tumors of the Central Nervous System: A summary. Neuro Oncol. 2021, 23, 1231–1251. [Google Scholar] [CrossRef] [PubMed]
- Martins, C.; Yasuda, A.; Campero, A.; Ulm, A.J.; Tanriover, N.; Rhoton, A., Jr. Microsurgical anatomy of the dural arteries. Neurosurgery 2005, 56 (Suppl. S2), 211–251; discussion 211–251. [Google Scholar] [CrossRef] [PubMed]






Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Plou, P.; Serioli, S.; Leonel, L.C.P.C.; Alexander, A.Y.; Agosti, E.; Vilany, L.; Graepel, S.; Choby, G.; Pinheiro-Neto, C.D.; Peris-Celda, M. Surgical Anatomy and Approaches of the Anterior Cranial Fossa from a Transcranial and Endonasal Perspective. Cancers 2023, 15, 2587. https://doi.org/10.3390/cancers15092587
Plou P, Serioli S, Leonel LCPC, Alexander AY, Agosti E, Vilany L, Graepel S, Choby G, Pinheiro-Neto CD, Peris-Celda M. Surgical Anatomy and Approaches of the Anterior Cranial Fossa from a Transcranial and Endonasal Perspective. Cancers. 2023; 15(9):2587. https://doi.org/10.3390/cancers15092587
Chicago/Turabian StylePlou, Pedro, Simona Serioli, Luciano C. P. C. Leonel, A. Yohan Alexander, Edoardo Agosti, Larissa Vilany, Stephen Graepel, Garret Choby, Carlos D. Pinheiro-Neto, and Maria Peris-Celda. 2023. "Surgical Anatomy and Approaches of the Anterior Cranial Fossa from a Transcranial and Endonasal Perspective" Cancers 15, no. 9: 2587. https://doi.org/10.3390/cancers15092587
APA StylePlou, P., Serioli, S., Leonel, L. C. P. C., Alexander, A. Y., Agosti, E., Vilany, L., Graepel, S., Choby, G., Pinheiro-Neto, C. D., & Peris-Celda, M. (2023). Surgical Anatomy and Approaches of the Anterior Cranial Fossa from a Transcranial and Endonasal Perspective. Cancers, 15(9), 2587. https://doi.org/10.3390/cancers15092587