
Performance and Safety of EUS Ablation Techniques for Pancreatic Cystic Lesions: A Systematic Review and Meta-Analysis
 , , ,
, , ,  , ,
, ,
Abstract
:Simple Summary
Abstract
1. Introduction
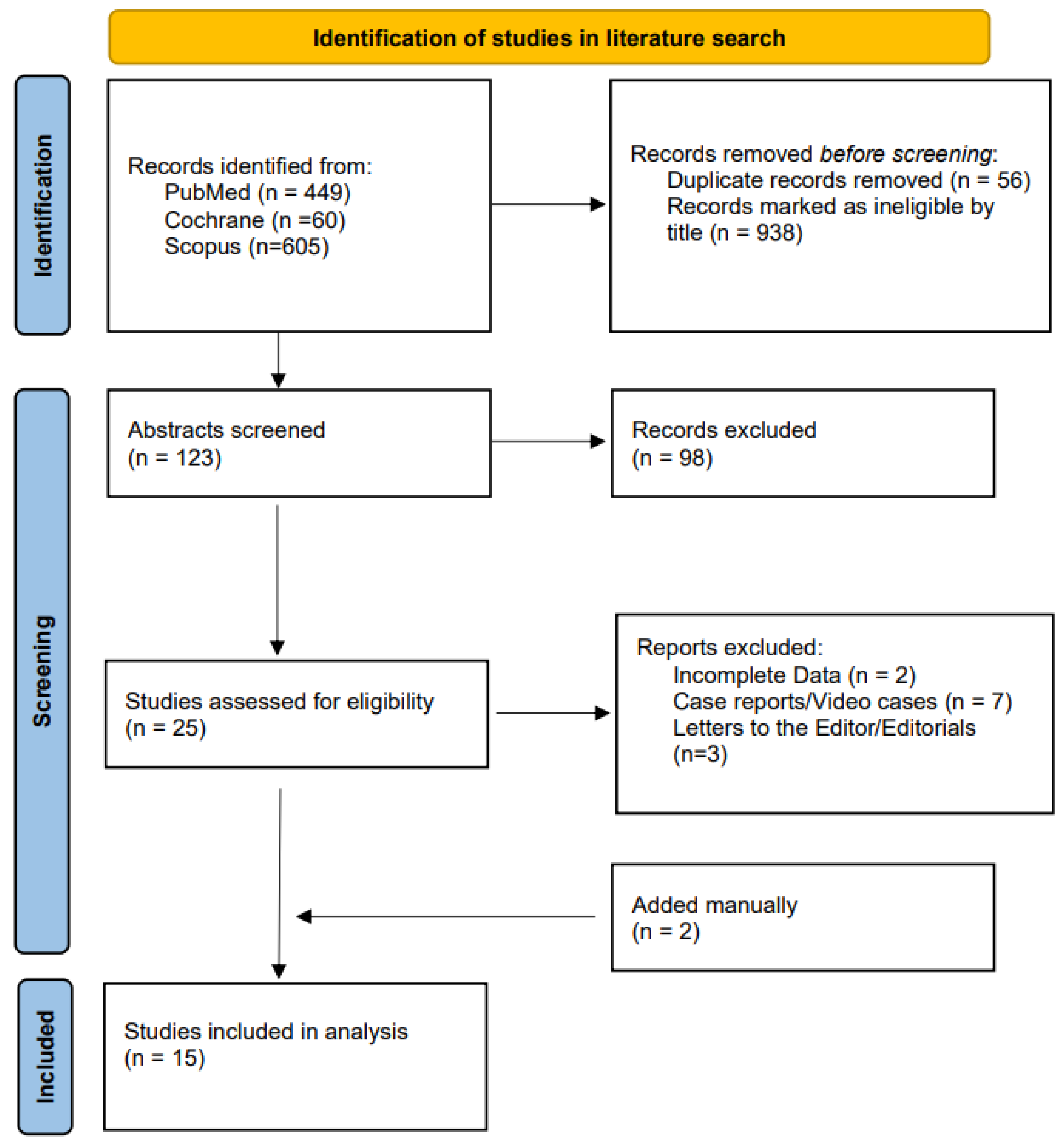
2. Materials and Methods
2.1. Inclusion and Exclusion Criteria
2.2. Search Strategy
2.3. Data Abstraction and Quality Assessment
2.4. Outcomes
2.5. Statistical Analysis
2.6. Quality of Evidence
3. Results
3.1. Characteristics of Included Studies
3.2. Quality Assessment
3.3. Primary Outcome—Complete Cyst Resolution
3.4. Secondary Outcomes
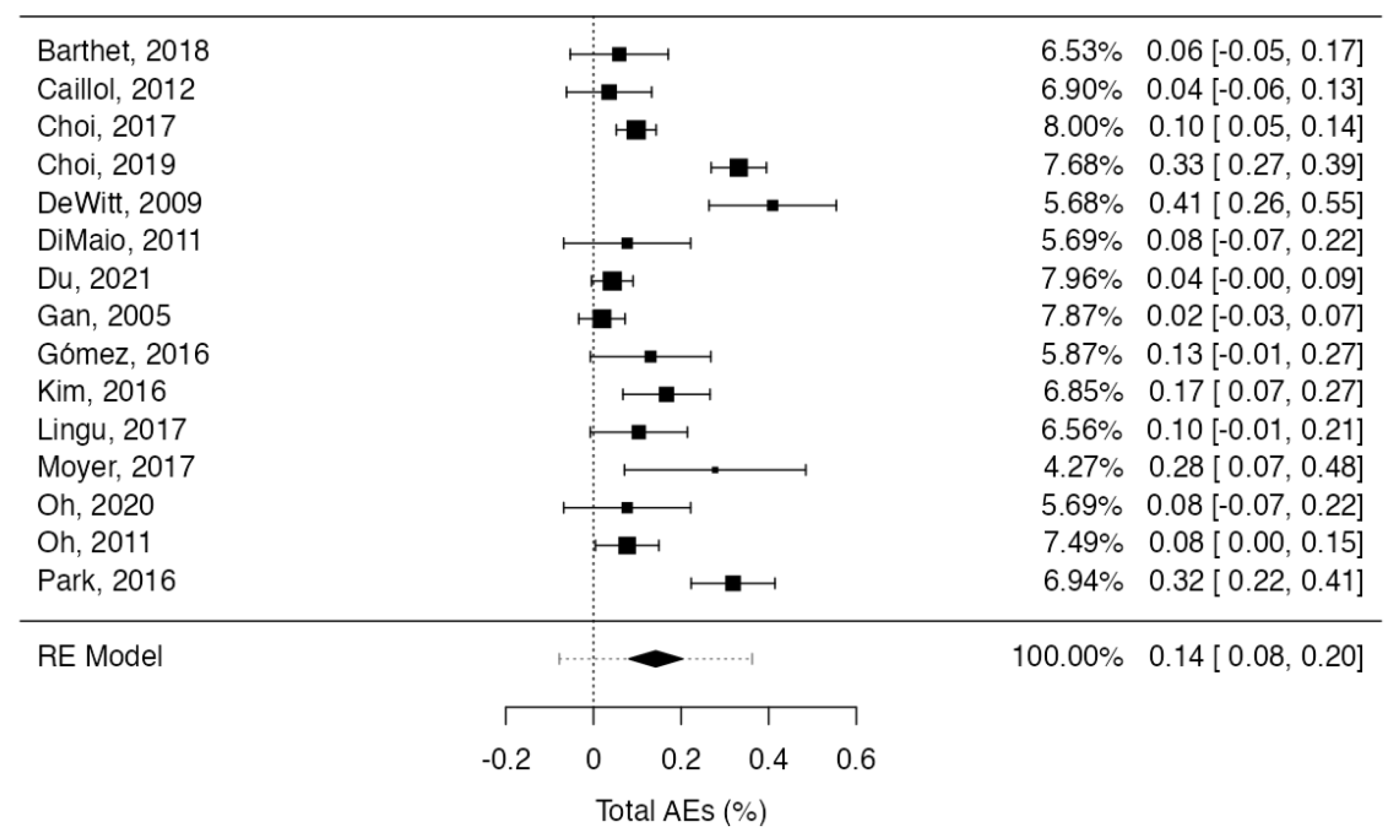
3.5. Adverse Events
3.6. Subgroup Analysis
3.7. Quality of Evidence
3.8. Publication Bias
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Singh, R.R.; Gopakumar, H.; Sharma, N.R. Diagnosis and Management of Pancreatic Cysts: A Comprehensive Review of the Literature. Diagnostics 2023, 13, 550. [Google Scholar] [CrossRef] [PubMed]
- Yoon, J.G.; Smith, D.; Ojili, V.; Paspulati, R.M.; Ramaiya, N.H.; Tirumani, S.H. Pancreatic Cystic Neoplasms: A Review of Current Recommendations for Surveillance and Management. Abdom. Radiol. 2021, 46, 3946–3962. [Google Scholar] [CrossRef] [PubMed]
- Vege, S.S.; Ziring, B.; Jain, R.; Moayyedi, P.; Adams, M.A.; Dorn, S.D.; Dudley-Brown, S.L.; Flamm, S.L.; Gellad, Z.F.; Gruss, C.B.; et al. American Gastroenterological Association Institute Guideline on the Diagnosis and Management of Asymptomatic Neoplastic Pancreatic Cysts. Gastroenterology 2015, 148, 819–822. [Google Scholar] [CrossRef] [PubMed]
- Conlon, K. European Evidence-Based Guidelines on Pancreatic Cystic Neoplasms. Gut 2018, 67, 789–804. [Google Scholar] [CrossRef]
- Marchegiani, G.; Salvia, R.; Stefano, A.; Alberto, B.; Tommaso, P.; Andrea, C.; Laura, M.; Costanza, Z.C.; Claudio, B.; Mohammed, A.H.; et al. Guidelines on Pancreatic Cystic Neoplasms: Major Inconsistencies with Available Evidence and Clinical Practice—Results From an International Survey. Gastroenterology 2021, 160, 2234–2238. [Google Scholar] [CrossRef]
- Tanaka, M.; Fernández-del Castillo, C.; Kamisawa, T.; Jang, J.Y.; Levy, P.; Ohtsuka, T.; Salvia, R.; Shimizu, Y.; Tada, M.; Wolfgang, C.L. Revisions of International Consensus Fukuoka Guidelines for the Management of IPMN of the Pancreas. Pancreatology 2017, 17, 738–753. [Google Scholar] [CrossRef]
- Keane, M.G.; Dadds, H.R.; El Sayed, G.; Luong, T.V.; Davidson, B.R.; Fusai, G.K.; Thorburn, D.; Pereira, S.P. Clinical and Radiological Features That Predict Malignant Transformation in Cystic Lesions of the Pancreas: A Retrospective Case Note Review. AMRC Open Res. 2020, 1, 4. [Google Scholar] [CrossRef]
- Van Huijgevoort, N.C.M.; del Chiaro, M.; Wolfgang, C.L.; van Hooft, J.E.; Besselink, M.G. Diagnosis and Management of Pancreatic Cystic Neoplasms: Current Evidence and Guidelines. Nat. Rev. Gastroenterol. Hepatol. 2019, 16, 676–689. [Google Scholar] [CrossRef]
- Farrell, J.J.; Fernández-del Castillo, C. Pancreatic Cystic Neoplasms: Management and Unanswered Questions. Gastroenterology 2013, 144, 1303–1315. [Google Scholar] [CrossRef]
- Van der Gaag, N.A.; Berkhemer, O.A.; Sprangers, M.A.; Busch, O.R.C.; Bruno, M.J.; de Castro, S.M.; van Gulik, T.M.; Gouma, D.J. Quality of Life and Functional Outcome After Resection of Pancreatic Cystic Neoplasm. Pancreas 2014, 43, 755–761. [Google Scholar] [CrossRef]
- Shah, K.P.; Baugh, K.A.; Brubaker, L.S.; Van Buren, G.; Villafane-Ferriol, N.; McElhany, A.L.; Mohamed, S.; Silberfein, E.J.; Hsu, C.; Massarweh, N.N.; et al. Long-Term Assessment of Pancreatic Function After Pancreatectomy for Cystic Neoplasms. J. Surg. Res. 2020, 247, 547–555. [Google Scholar] [CrossRef] [PubMed]
- Marinelli, V.; Secchettin, E.; Andrianello, S.; Moretti, C.; Donvito, S.; Marchegiani, G.; Esposito, A.; Casetti, L.; Salvia, R. Psychological Distress in Patients under Surveillance for Intraductal Papillary Mucinous Neoplasms of the Pancreas: The “Sword of Damocles” Effect Calls for an Integrated Medical and Psychological Approach a Prospective Analysis. Pancreatology 2020, 20, 505–510. [Google Scholar] [CrossRef] [PubMed]
- Sharib, J.; Esserman, L.; Koay, E.J.; Maitra, A.; Shen, Y.; Kirkwood, K.S.; Ozanne, E.M. Cost-Effectiveness of Consensus Guideline Based Management of Pancreatic Cysts: The Sensitivity and Specificity Required for Guidelines to Be Cost-Effective. Surgery 2020, 168, 601–609. [Google Scholar] [CrossRef] [PubMed]
- Lobo, J.M.; Scheiman, J.M.; Zaydfudim, V.M.; Shami, V.M.; Sauer, B.G. Clinical and Economic Outcomes of Patients Undergoing Guideline-Directed Management of Pancreatic Cysts. Am. J. Gastroenterol. 2020, 115, 1689–1697. [Google Scholar] [CrossRef]
- Zhang, L.; Tan, S.; Huang, S.; Zhong, C.; Lü, M.; Peng, Y.; Tang, X. The Safety and Efficacy of Endoscopic Ultrasound-Guided Ablation Therapy for Solid Pancreatic Tumors: A Systematic Review. Scand J. Gastroenterol. 2020, 55, 1121–1131. [Google Scholar] [CrossRef]
- Liu, M.; Li, X.-J.; Zhang, X.-E.; Kuang, M.; Xie, X.-Y.; Huang, G.-L. Long-Term Outcomes of Combined Radiofrequency Ablation and Multipronged Ethanol Ablation for the Treatment of Unfavorable Hepatocellular Carcinoma. Diagn. Interv. Radiol. 2023, 29, 342–349. [Google Scholar] [CrossRef]
- Garg, R.; Mohammed, A.; Singh, A.; Harnegie, M.; Rustagi, T.; Stevens, T.; Chahal, P. EUS-Guided Radiofrequency and Ethanol Ablation for Pancreatic Neuroendocrine Tumors: A Systematic Review and Meta-Analysis. Endosc. Ultrasound 2022, 11, 170. [Google Scholar] [CrossRef]
- So, H.; Ko, S.W.; Shin, S.H.; Kim, E.H.; Son, J.; Ha, S.; Song, K.B.; Kim, H.J.; Kim, M.-H.; Park, D.H. Comparison of EUS-Guided Ablation and Surgical Resection for Nonfunctioning Small Pancreatic Neuroendocrine Tumors: A Propensity Score–Matching Study. Gastrointest Endosc. 2023, 97, 741–751.e1. [Google Scholar] [CrossRef]
- Inderson, A.; Slingerland, M.; Farina Sarasqueta, A.; de Steur, W.O.; Boonstra, J.J. EUS-Guided Radiofrequency Ablation for a Left Adrenal Oligometastasis of an Esophageal Adenocarcinoma. VideoGIE 2018, 3, 159–161. [Google Scholar] [CrossRef]
- Teoh, A.Y.-B.; Seo, D.W.; Brugge, W.; Dewitt, J.; Kongkam, P.; Linghu, E.; Moyer, M.T.; Ryu, J.K.; Ho, K.Y. Position Statement on EUS-Guided Ablation of Pancreatic Cystic Neoplasms from an International Expert Panel. Endosc. Int. Open 2019, 07, E1064–E1077. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Huang, X.; Lin, J.; Demner-Fushman, D. Evaluation of PICO as a Knowledge Representation for Clinical Questions. AMIA Annu. Symp. Proc. AMIA Symposium. AMIA Symp. 2006, 2006, 359–363. [Google Scholar]
- DerSimonian, R.; Laird, N. Meta-Analysis in Clinical Trials. Control Clin. Trials 1986, 7, 177–188. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.T. Measuring Inconsistency in Meta-Analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef]
- Higgins, J.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.; Welch, V. (Eds.) Cochrane Handbook for Systematic Reviews of Interventions, 2nd ed.; John Wiley & Sons: Chichester, UK, 2019. [Google Scholar]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2021. [Google Scholar]
- Guyatt, G.H.; Oxman, A.D.; Kunz, R.; Woodcock, J.; Brozek, J.; Helfand, M.; Alonso-Coello, P.; Falck-Ytter, Y.; Jaeschke, R.; Vist, G.; et al. GRADE Guidelines: 8. Rating the Quality of Evidence—Indirectness. J. Clin. Epidemiol. 2011, 64, 1303–1310. [Google Scholar] [CrossRef]
- Park, D.H.; Choi, J.-H.; Oh, D.; Lee, S.S.; Seo, D.-W.; Lee, S.K.; Kim, M.-H. Endoscopic Ultrasonography-Guided Ethanol Ablation for Small Pancreatic Neuroendocrine Tumors: Results of a Pilot Study. Clin. Endosc. 2015, 48, 158. [Google Scholar] [CrossRef]
- Oh, D.; Ko, S.W.; Seo, D.-W.; Hong, S.-M.; Kim, J.H.; Song, T.J.; Park, D.H.; Lee, S.K.; Kim, M.-H. Endoscopic Ultrasound-Guided Radiofrequency Ablation of Pancreatic Microcystic Serous Cystic Neoplasms: A Retrospective Study. Endoscopy 2021, 53, 739–743. [Google Scholar] [CrossRef]
- Oh, H.; Seo, D.W.; Song, T.J.; Moon, S.; Park, D.H.; Soo Lee, S.; Lee, S.K.; Kim, M.; Kim, J. Endoscopic Ultrasonography-Guided Ethanol Lavage with Paclitaxel Injection Treats Patients with Pancreatic Cysts. Gastroenterology 2011, 140, 172–179. [Google Scholar] [CrossRef]
- Moyer, M.T.; Sharzehi, S.; Mathew, A.; Levenick, J.M.; Headlee, B.D.; Blandford, J.T.; Heisey, H.D.; Birkholz, J.H.; Ancrile, B.B.; Maranki, J.L.; et al. The Safety and Efficacy of an Alcohol-Free Pancreatic Cyst Ablation Protocol. Gastroenterology 2017, 153, 1295–1303. [Google Scholar] [CrossRef]
- Linghu, E.; Du, C.; Chai, N.; Li, H.; Wang, Z.; Sun, Y.; Xu, W.; Guo, X.; Ning, B.; Sun, L.; et al. A Prospective Study on the Safety and Effectiveness of Using Lauromacrogol for Ablation of Pancreatic Cystic Neoplasms with the Aid of EUS. Gastrointest. Endosc. 2017, 86, 872–880. [Google Scholar] [CrossRef]
- Kim, K.H.; McGreevy, K.; La Fortune, K.; Cramer, H.; DeWitt, J. Sonographic and Cyst Fluid Cytologic Changes after EUS-Guided Pancreatic Cyst Ablation. Gastrointest. Endosc. 2017, 85, 1233–1242. [Google Scholar] [CrossRef] [PubMed]
- Gómez, V.; Takahashi, N.; Levy, M.J.; McGee, K.P.; Jones, A.; Huang, Y.; Chari, S.T.; Clain, J.E.; Gleeson, F.C.; Pearson, R.K.; et al. EUS-Guided Ethanol Lavage Does Not Reliably Ablate Pancreatic Cystic Neoplasms (with Video). Gastrointest. Endosc. 2016, 83, 914–920. [Google Scholar] [CrossRef]
- Gan, S.I.; Thompson, C.C.; Lauwers, G.Y.; Bounds, B.C.; Brugge, W.R. Ethanol Lavage of Pancreatic Cystic Lesions: Initial Pilot Study. Gastrointest. Endosc. 2005, 61, 746–752. [Google Scholar] [CrossRef] [PubMed]
- Du, C.; Chai, N.; Linghu, E.; Li, H.; Feng, X.; Ning, B.; Wang, X.; Tang, P. Long-Term Outcomes of EUS-Guided Lauromacrogol Ablation for the Treatment of Pancreatic Cystic Neoplasms: 5 Years of Experience. Endosc. Ultrasound 2022, 11, 44. [Google Scholar] [CrossRef] [PubMed]
- DiMaio, C.J.; DeWitt, J.M.; Brugge, W.R. Ablation of Pancreatic Cystic Lesions. Pancreas 2011, 40, 664–668. [Google Scholar] [CrossRef]
- DeWitt, J.; McGreevy, K.; Schmidt, C.M.; Brugge, W.R. EUS-Guided Ethanol versus Saline Solution Lavage for Pancreatic Cysts: A Randomized, Double-Blind Study. Gastrointest. Endosc. 2009, 70, 710–723. [Google Scholar] [CrossRef]
- Choi, J.-H.; Seo, D.; Song, T.; Park, D.; Lee, S.; Lee, S.; Kim, M.-H. Long-Term Outcomes after Endoscopic Ultrasound-Guided Ablation of Pancreatic Cysts. Endoscopy 2017, 49, 866–873. [Google Scholar] [CrossRef]
- Caillo, F. Ethanol Lavage of 14 Mucinous Cysts of the Pancreas: A Retrospective Study in Two Tertiary Centers. Endosc. Ultrasound 2012, 1, 48. [Google Scholar] [CrossRef]
- Barthet, M.; Giovannini, M.; Lesavre, N.; Boustiere, C.; Napoleon, B.; Koch, S.; Gasmi, M.; Vanbiervliet, G.; Gonzalez, J.-M. Endoscopic Ultrasound-Guided Radiofrequency Ablation for Pancreatic Neuroendocrine Tumors and Pancreatic Cystic Neoplasms: A Prospective Multicenter Study. Endoscopy 2019, 51, 836–842. [Google Scholar] [CrossRef]
- Choi, J.H.; Lee, S.H.; Choi, Y.H.; You, M.S.; Shin, B.-S.; Paik, W.H.; Ryu, J.K.; Kim, Y.-T. Safety of Endoscopic Ultrasound-Guided Ethanol Ablation for Pancreatic Cystic Lesions: A Single-Center Experience of 214 Patients. Hepatobiliary Pancreat. Dis. Int. 2019, 18, 562–568. [Google Scholar] [CrossRef]
- An, S.; Sung, Y.-N.; Kim, S.J.; Seo, D.-W.; Jun, S.-Y.; Hong, S.-M. Pancreatic Cysts after Endoscopic Ultrasonography-Guided Ethanol and/or Paclitaxel Ablation Therapy: Another Mimic of Pancreatic Pseudocysts. Pathobiology 2022, 89, 49–55. [Google Scholar] [CrossRef]
- Polkowski, M.; Jenssen, C.; Kaye, P.; Carrara, S.; Deprez, P.; Gines, A.; Fernández-Esparrach, G.; Eisendrath, P.; Aithal, G.; Arcidiacono, P.; et al. Technical Aspects of Endoscopic Ultrasound (EUS)-Guided Sampling in Gastroenterology: European Society of Gastrointestinal Endoscopy (ESGE) Technical Guideline–March 2017. Endoscopy 2017, 49, 989–1006. [Google Scholar] [CrossRef] [PubMed]
- Bispo, M.; Caldeira, A.; Leite, S.; Marques, S.; Moreira, T.; Moutinho-Ribeiro, P.; Nunes, N. Endoscopic Ultrasound-Guided Ablation of Focal Pancreatic Lesions: The GRUPUGE Perspective. GE Port J. Gastroenterol. 2020, 27, 410–416. [Google Scholar] [CrossRef] [PubMed]
- Younis, F.; Ben-Ami Shor, D.; Lubezky, N.; Geva, R.; Osher, E.; Shibolet, O.; Phillips, A.; Scapa, E. Endoscopic Ultrasound-Guided Radiofrequency Ablation of Premalignant Pancreatic-Cystic Neoplasms and Neuroendocrine Tumors: Prospective Study. Eur. J. Gastroenterol. Hepatol. 2022, 34, 1111–1115. [Google Scholar] [CrossRef]
- Armellini, E.; Facciorusso, A.; Crinò, S.F. Efficacy and Safety of Endoscopic Ultrasound-Guided Radiofrequency Ablation for Pancreatic Neuroendocrine Tumors: A Systematic Review and Metanalysis. Medicines 2023, 59, 359. [Google Scholar] [CrossRef]
- Crinò, S.F.; Napoleon, B.; Facciorusso, A.; Lakhtakia, S.; Borbath, I.; Caillol, F.; Do-Cong Pham, K.; Rizzatti, G.; Forti, E.; Palazzo, L.; et al. Endoscopic Ultrasound-Guided Radiofrequency Ablation Versus Surgical Resection for Treatment of Pancreatic Insulinoma. Clin. Gastroenterol. Hepatol. 2023, in press. [Google Scholar] [CrossRef]
- Feng, X.; Linghu, E.; Chai, N.; Li, H. New Treatment of the Pancreatic Cystic Neoplasm: Endoscopic Ultrasonography-Guided Radiofrequency Ablation Combined with Lauromacrogol Ablation. Turk. J. Gastroenterol. 2018, 29, 99–102. [Google Scholar] [CrossRef]
- Choi, J.H.; Lee, S.H.; Choi, Y.H.; Kang, J.; Paik, W.H.; Ahn, D.-W.; Ryu, J.K.; Kim, Y.-T. Clinical Outcomes of Endoscopic Ultrasound-Guided Ethanol Ablation for Pancreatic Cystic Lesions Compared with the Natural Course: A Propensity Score Matching Analysis. Ther. Adv. Gastroenterol. 2018, 11. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Study | Year | Design | Country | Recruitment Period | Number of Patients | Mean Age | Gender (% Female) | Mean Diameter (Range) mm | SB-IPMN (%) | MCN (%) | SCN (%) | Pseudocyst (%) | Indeterminate (%) | Head (%) | Body (%) | Tail (%) | Maximum Follow Up (Months) | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Barthet et al. | 2018 | Prospective cohort | Multicenter | France | 2 years | 17 | 65.7 (range 65–83) | 10 (59%) | 28.0 (9.0–60.0) | 16 (94%) | 1 (6%) | 0 | 0 | 0 | 10 (59%) | 4 (24%) | 3 (18%) | 12 |
| Caillol et al. | 2012 | Retrospective cohort | Two-center | France | 2001–2010 | 13 | 68.5 (range 49–81) | 6 (46%) | 23.9 (11.0–50.0) | 0 | 13 (100%) | 0 | 0 | 0 | 9 (64%) | 3 (21%) | 2 (14%) | 118 |
| Choi et al. | 2017 | Prospective cohort | Single center | Korea | 2005–2015 | 158 | 51 (IQR 20–85) | 115 (70%) | Median 32.0 (IQR 26.0–41.0) | 11 (7%) | 71 (43%) | 16 (10%) | 3 (2%) | 63 (38%) | 42 (26%) | 86 (52%) | 36 (22%) | NR |
| Choi et al. | 2019 | Retrospective cohort | Single center | Korea | 2006–2018 | 214 | 55.61 (SD ± 14.7) | 140 (65%) | 32.2 (SD ± 9.6) | 63 (29%) | 57 (27%) | 69 (32%) | 25 (12%) | 0 | 89 (42%) | 69 (32%) | 56 (26%) | NR |
| DeWitt et al. | 2009 | Randomized trial, double-blind | Multicenter | USA | 2004–2007 | 39 | 69.1 (SD ± 13.2) | 27 (64%) | 20.5 (10.0–40.0) | 17 (41%) | 17 (41%) | 5 (12%) | 3 (7%) | 0 | 18 (43%) | 16 (38%) | 8 (19%) | 39 |
| DiMaio et al. | 2011 | Retrospective cohort | Single center | USA | 2001–2008 | 21 | 70 (NR) | 9 (69%) | 20.1 (SD ± 7.1) | 13 (100%) | 0 | 0 | 0 | 0 | 8 (62%) | 4 (30%) | 1 (8%) | 18 |
| Du et al. | 2021 | Prospective cohort | Multicenter | China | 2015–2020 | 70 | 50.3 (SD ± 14.2) | 50 (71%) | 32.0 (9.0–110.0) | 0 | 27 (39%) | 34 (49%) | 0 | 9 (13%) | 37 (53%) | 23 (47%) | 55 | |
| Gan et al. | 2005 | Pilot study | Single center | USA | 2001–2003 | 25 | 64.5 (NR) | 20 (80%) | 19.4 (6.0–37.0) | 3 (12%) | 14 (56%) | 3 (12%) | 1 (4%) | 1 (4%) | 8 (32%) | 8 (32%) | 9 (36%) | 12 |
| Gómez et al. | 2016 | Prospective cohort | Single center | USA | 2004–2014 | 23 | 70 (range 53–86) | 10 (44%) | 27.5 (14.9–49.3) | 15 (65%) | 4 (17%) | 4 (17%) | 0 | 0 | 15 (65%) | 6 (26%) | 2 (9%) | 82 |
| Kim et al. | 2016 | Prospective cohort | Single center | USA | 2004–2015 | 36 | 69.1 (SD ± 12.2) | 24 (67%) | 25.8 (SD ± 8.7) | 14 (39%) | 16 (44%) | 5 (14%) | 1 (3%) | 0 | 14 (39%) | 22 (61%) | 119 | |
| Linghu et al. | 2017 | Prospective cohort | Single center | China | 2015–2016 | 29 | 56 (SD ± 15) | 20 (68%) | 30.6 (SD ± 15.0) | 0 | 15 (52%) | 12 (41%) | 0 | 2 (7%) | NR | NR | NR | 15 |
| Moyer et al. | 2017 | Randomized trial, double-blind | Single center | USA | 2011–2016 | 39 | NR | 23 (59%) | 25 (15.5–42.0) | 27 (69%) | 9 (23%) | 0 | 0 | 3 (8%) | 19 (49%) | 19 (49%) | 1 (3%) | 12 |
| Oh et al. | 2020 | Retrospective cohort | Single center | Korea | 2018–2019 | 13 | 60 (IQR 50.5–70) | 5 (39%) | Median 50 (IQR 34.0–52.5) | 0 | 0 | 13 (100%) | 0 | 0 | 5 (39%) | 8 (62%) | 15 | |
| Oh et al. | 2011 | Prospective cohort | Single center | Korea | 2005–2009 | 52 | 49.5 (range 22–81) | 34 (65%) | 31.8 (17.0–68.0) | 0 | 9 (17%) | 15 (29%) | 2 (4%) | 26 (50%) | 16 (31%) | 17 (33%) | 19 (37%) | 44 |
| Park et al. | 2016 | Prospective cohort | Single center | Korea | NR | 91 | 58 (range 28–83) | 67 (74%) | 30.0 (20.0–50.0) | 9 (10%) | 12 (13%) | 33 (36%) | 9 (10%) | 28 (31%) | 35 (38%) | 32 (35%) | 24 (26%) | 117 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Papaefthymiou, A.; Johnson, G.J.; Maida, M.; Gkolfakis, P.; Ramai, D.; Facciorusso, A.; Arvanitakis, M.; Ney, A.; Fusai, G.K.; Saftoiu, A.; et al. Performance and Safety of EUS Ablation Techniques for Pancreatic Cystic Lesions: A Systematic Review and Meta-Analysis. Cancers 2023, 15, 2627. https://doi.org/10.3390/cancers15092627
Papaefthymiou A, Johnson GJ, Maida M, Gkolfakis P, Ramai D, Facciorusso A, Arvanitakis M, Ney A, Fusai GK, Saftoiu A, et al. Performance and Safety of EUS Ablation Techniques for Pancreatic Cystic Lesions: A Systematic Review and Meta-Analysis. Cancers. 2023; 15(9):2627. https://doi.org/10.3390/cancers15092627
Chicago/Turabian StylePapaefthymiou, Apostolis, Gavin J. Johnson, Marcello Maida, Paraskevas Gkolfakis, Daryl Ramai, Antonio Facciorusso, Marianna Arvanitakis, Alexander Ney, Giuseppe K. Fusai, Adrian Saftoiu, and et al. 2023. "Performance and Safety of EUS Ablation Techniques for Pancreatic Cystic Lesions: A Systematic Review and Meta-Analysis" Cancers 15, no. 9: 2627. https://doi.org/10.3390/cancers15092627
APA StylePapaefthymiou, A., Johnson, G. J., Maida, M., Gkolfakis, P., Ramai, D., Facciorusso, A., Arvanitakis, M., Ney, A., Fusai, G. K., Saftoiu, A., Tabacelia, D., Phillpotts, S., Chapman, M. H., Webster, G. J., & Pereira, S. P. (2023). Performance and Safety of EUS Ablation Techniques for Pancreatic Cystic Lesions: A Systematic Review and Meta-Analysis. Cancers, 15(9), 2627. https://doi.org/10.3390/cancers15092627