Recurrence and Survival Following Cytoreductive Surgery and Hyperthermic Intraperitoneal Chemotherapy for Synchronous and Metachronous Peritoneal Metastases of Colorectal Origin

 , and
, and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Design and Setting
2.2. Patients
2.3. Cytoreductive Surgery and Hyperthermic Intraperitoneal Chemotherapy
2.4. Follow-Up
2.5. Data Collection and Variables
2.6. Study Endpoints
2.7. Statistical Analysis
3. Results
3.1. Baseline Characteristics
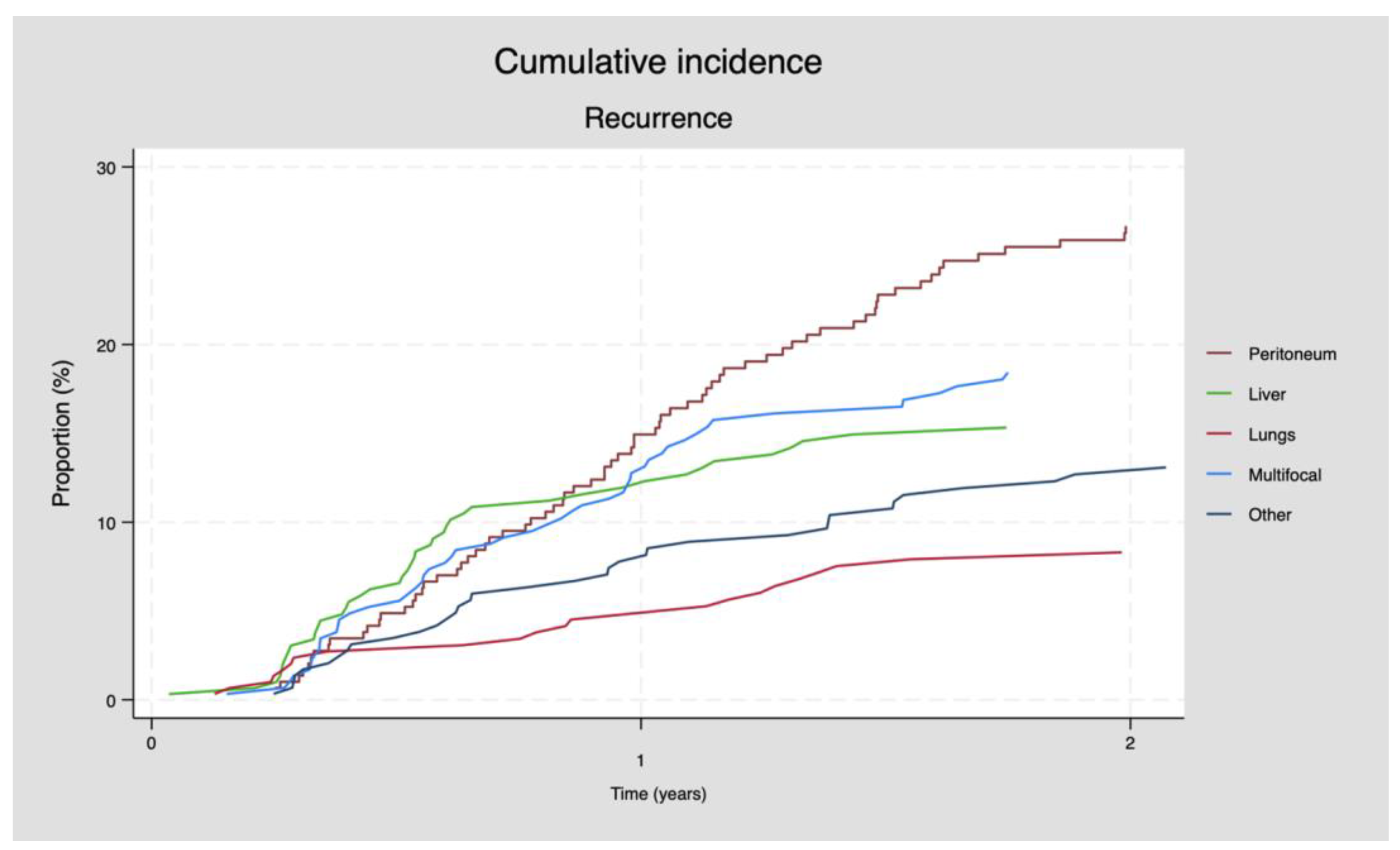
3.2. Pattern of Recurrence
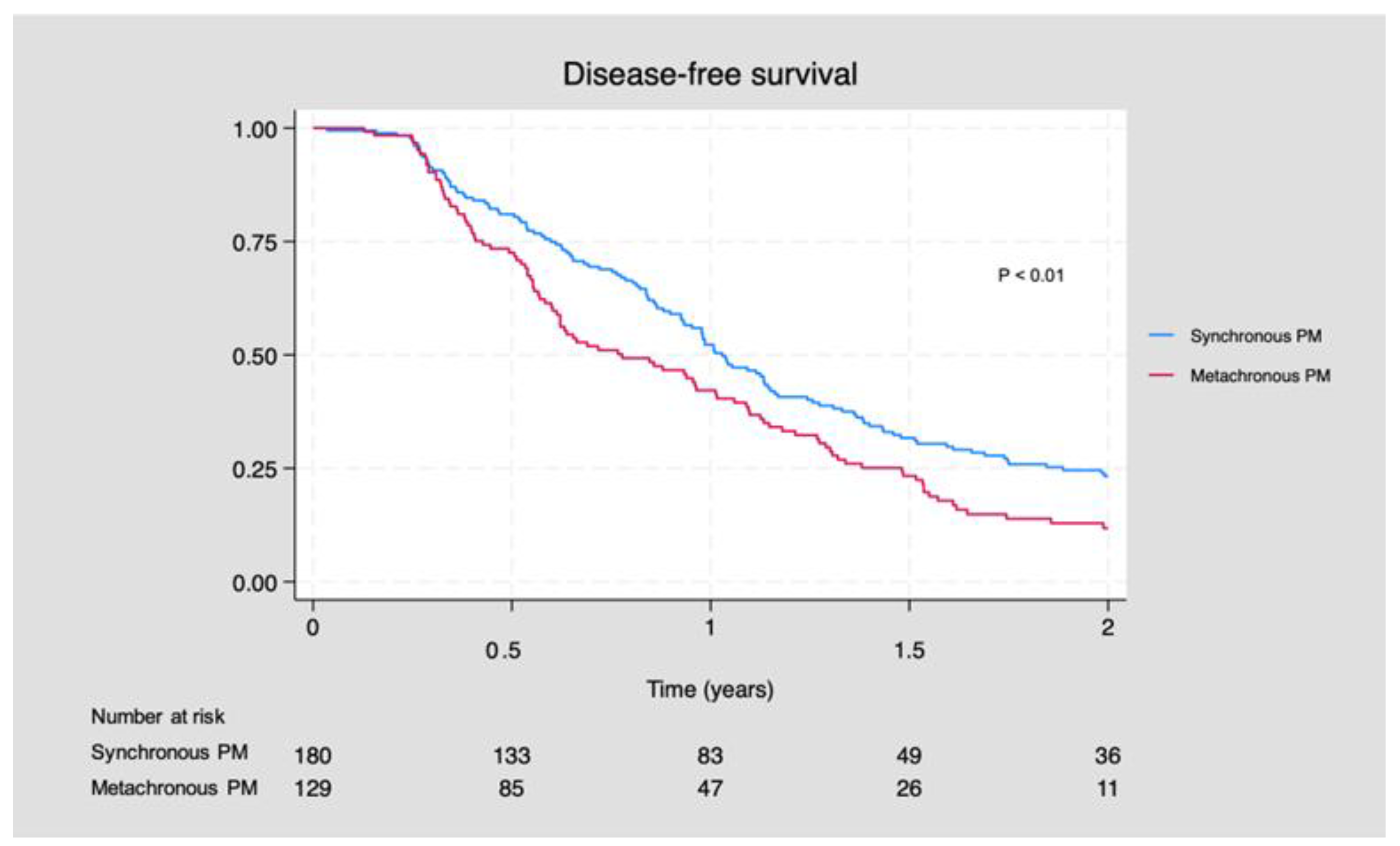
3.3. Disease-Free Survival
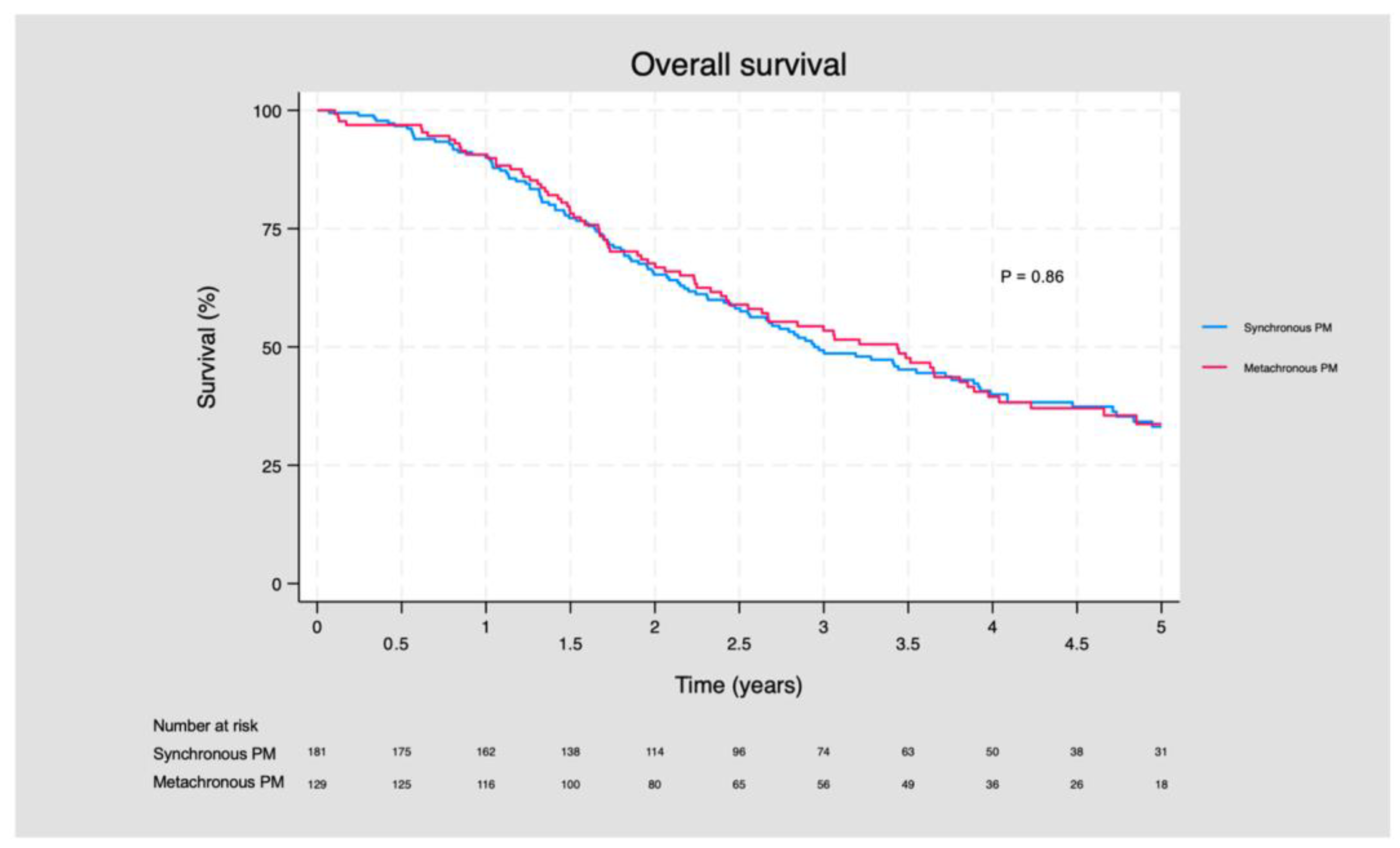
3.4. Overall Survival
3.5. Subanalyses
4. Discussion
Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Danish Colorectal Cancer Database (DCCG). Landsdaekkende Database for Kraeft i Tyk-Og Endetarm. Available online: https://dccg.dk/ (accessed on 29 January 2023). (In Danish).
- Majano, S.B.; Girolamo, C.D.; Rachet, B.; Maringe, C.; Guren, M.G.; Glimelius, B.; Iversen, L.H.; Schnell, E.A.; Lundqvist, K.; Christensen, J.; et al. Surgical Treatment and Survival from Colorectal Cancer in Denmark, England, Norway, and Sweden: A Population-Based Study. Lancet Oncol. 2019, 20, 74–87. [Google Scholar] [CrossRef] [PubMed]
- Lurvink, R.J.; Bakkers, C.; Rijken, A.; van Erning, F.N.; Nienhuijs, S.W.; Burger, J.W.; Creemers, G.J.; Verhoef, C.; Lemmens, V.E.; Hingh, I.H.D. Increase in the Incidence of Synchronous and Metachronous Peritoneal Metastases in Patients with Colorectal Cancer: A Nationwide Study: Colorectal PM: Incidence & Associated Factors. Eur. J. Surg. Oncol. 2021, 47, 1026–1033. [Google Scholar] [CrossRef] [PubMed]
- Quere, P.; Facy, O.; Manfredi, S.; Jooste, V.; Faivre, J.; Lepage, C.; Bouvier, A.M. Epidemiology, Management, and Survival of Peritoneal Carcinomatosis from Colorectal Cancer: A Population-Based Study. Dis. Colon Rectum 2015, 58, 743–752. [Google Scholar] [CrossRef]
- Ravn, S.; Christiansen, C.; Hagemann-Madsen, R.; Verwaal, V.; Iversen, L. The Validity of Registered Synchronous Peritoneal Metastases from Colorectal Cancer in the Danish Medical Registries. Clin. Epidemiol. 2020, 12, 333–343. [Google Scholar] [CrossRef]
- Ravn, S.; Heide-Jørgensen, U.; Christiansen, C.F.; Verwaal, V.J.; Hagemann-Madsen, R.H.; Iversen, L.H. Overall Risk and Risk Factors for Metachronous Peritoneal Metastasis after Colorectal Cancer Surgery: A Nationwide Cohort Study. BJS Open 2020, 4, 284–292. [Google Scholar] [CrossRef]
- Bakkers, C.; Lurvink, R.J.; Rijken, A.; Nienhuijs, S.W.; Kok, N.F.; Creemers, G.J.; Verhoef, C.; Lemmens, V.E.; van Erning, F.N.; Hingh, I.H.D. Treatment Strategies and Prognosis of Patients With Synchronous or Metachronous Colorectal Peritoneal Metastases: A Population-Based Study. Ann. Surg. Oncol. 2021, 28, 9073–9083. [Google Scholar] [CrossRef]
- Iversen, L.H.; Rasmussen, P.C.; Hagemann-Madsen, R.; Laurberg, S. Cytoreductive Surgery and Hyperthermic Intraperitoneal Chemotherapy for Peritoneal Carcinomatosis: The Danish Experience. Color. Dis. 2013, 15, e365–e372. [Google Scholar] [CrossRef] [PubMed]
- Verwaal, V.J.; Bruin, S.; Boot, H.; Slooten, G.V.; Tinteren, H.V. 8-Year Follow-up of Randomized Trial: Cytoreduction and Hyperthermic Intraperitoneal Chemotherapy versus Systemic Chemotherapy in Patients with Peritoneal Carcinomatosis of Colorectal Cancer. Ann. Surg. Oncol. 2008, 15, 2426–2432. [Google Scholar] [CrossRef]
- Quénet, F.; Elias, D.; Roca, L.; Goéré, D.; Ghouti, L.; Pocard, M.; Facy, O.; Arvieux, C.; Lorimier, G.; Pezet, D.; et al. Cytoreductive Surgery plus Hyperthermic Intraperitoneal Chemotherapy versus Cytoreductive Surgery Alone for Colorectal Peritoneal Metastases (PRODIGE 7): A Multicentre, Randomised, Open-Label, Phase 3 Trial. Lancet Oncol. 2021, 22, 256–266. [Google Scholar] [CrossRef]
- Elias, D.; Lefevre, J.H.; Chevalier, J.; Brouquet, A.; Marchal, F.; Classe, J.M.; Ferron, G.; Guilloit, J.M.; Meeus, P.; Goéré, D.; et al. Complete Cytoreductive Surgery plus Intraperitoneal Chemohyperthermia with Oxaliplatin for Peritoneal Carcinomatosis of Colorectal Origin. J. Clin. Oncol. 2009, 27, 681–685. [Google Scholar] [CrossRef]
- Kyang, L.S.; Alzahrani, N.A.; Valle, S.J.; Rahman, M.K.; Arrowaili, A.; Liauw, W.; Morris, D.L. Long-term Survival Outcomes of Cytoreductive Surgery and Perioperative Intraperitoneal Chemotherapy: Single-institutional Experience with 1225 Cases. J. Surg. Oncol. 2019, 120, 794–802. [Google Scholar] [CrossRef]
- Breuer, E.; Hebeisen, M.; Schneider, M.A.; Roth, L.; Pauli, C.; Frischer-Ordu, K.; Eden, J.; Pache, B.; Steffen, T.; Hübner, M.; et al. Site of Recurrence and Survival after Surgery for Colorectal Peritoneal Metastasis. J. Natl. Cancer Inst. 2021, 113, 1027–1035. [Google Scholar] [CrossRef]
- Dietz, M.V.; van Kooten, J.P.; Said, I.; Brandt-Kerkhof, A.R.M.; Verhoef, C.; Bremers, A.J.A.; de Wilt, J.H.W.; de Reuver, P.R.; Madsen, E.V.E. Survival Outcomes After Cytoreductive Surgery with Hyperthermic Intraperitoneal Chemotherapy in Patients with Synchronous Versus Metachronous Onset of Peritoneal Metastases of Colorectal Carcinoma. Ann. Surg. Oncol. 2022, 29, 6566–6576. [Google Scholar] [CrossRef] [PubMed]
- Hentzen, J.E.K.R.; Rovers, K.P.; Kuipers, H.; van der Plas, W.Y.; Been, L.B.; Hoogwater, F.J.H.; van Ginkel, R.J.; Hemmer, P.H.J.; van Dam, G.M.; de Hingh, I.H.J.T.; et al. Impact of Synchronous Versus Metachronous Onset of Colorectal Peritoneal Metastases on Survival Outcomes After Cytoreductive Surgery (CRS) with Hyperthermic Intraperitoneal Chemotherapy (HIPEC): A Multicenter, Retrospective, Observational Study. Ann. Surg. Oncol. 2019, 26, 2210–2221. [Google Scholar] [CrossRef] [PubMed]
- Braam, H.J.; Oudheusden, T.R.V.; Hingh, I.H.J.T.D.; Nienhuijs, S.W.; Boerma, D.; Wiezer, M.J.; Ramshorst, B.V. Patterns of Recurrence Following Complete Cytoreductive Surgery and Hyperthermic Intraperitoneal Chemotherapy in Patients with Peritoneal Carcinomatosis of Colorectal Cancer. J. Surg. Oncol. 2014, 109, 841–847. [Google Scholar] [CrossRef] [PubMed]
- Hassan, S.; Malcomson, L.; Soh, Y.J.; Wilson, M.S.; Clouston, H.; O’Dwyer, S.T.; Kochhar, R.; Aziz, O. Patterns and Timing of Recurrence Following CRS and HIPEC in Colorectal Cancer Peritoneal Metastasis. Eur. J. Surg. Oncol. 2023, 49, 202–208. [Google Scholar] [CrossRef]
- Wong, J.S.M.; Tan, G.H.C.; Chia, C.S.; Ong, J.; Ng, W.Y.; Teo, M.C.C. The Importance of Synchronicity in the Management of Colorectal Peritoneal Metastases with Cytoreductive Surgery and Hyperthermic Intraperitoneal Chemotherapy. World J. Surg. Oncol. 2020, 18, 10. [Google Scholar] [CrossRef] [PubMed]
- Sugarbaker, P.H. Colorectal Cancer: Prevention and Management of Metastatic Disease. BioMed Res. Int. 2014, 2014, 782890. [Google Scholar] [CrossRef]
- Swellengrebel, H.A.M.; Zoetmulder, F.A.N.; Smeenk, R.M.; Antonini, N.; Verwaal, V.J. Quantitative Intra-Operative Assessment of Peritoneal Carcinomatosis—A Comparison of Three Prognostic Tools. Eur. J. Surg. Oncol. 2009, 35, 1078–1084. [Google Scholar] [CrossRef] [PubMed]
- Balachandran, R.; Sørensen, M.M.; Funder, J.A.; Knudsen, A.R.; Iversen, L.H. Outcomes after Curatively Intended Treatment of Limited Peritoneal Metastases and Thermal Ablation for Liver Metastases from Colorectal Cancer. Pleura Peritoneum 2023, 8, 167–174. [Google Scholar] [CrossRef]
- Sugarbaker, P.H. Peritonectomy Procedures. In Peritoneal Carcinomatosis; Springer: Berlin/Heidelberg, Germany, 2007; pp. 247–264. [Google Scholar]
- Mehta, A.M.; Huitema, A.D.R.; Burger, J.W.A.; Brandt-Kerkhof, A.R.M.; van den Heuvel, S.F.; Verwaal, V.J. Standard Clinical Protocol for Bidirectional Hyperthermic Intraperitoneal Chemotherapy (HIPEC): Systemic Leucovorin, 5-Fluorouracil, and Heated Intraperitoneal Oxaliplatin in a Chloride-Containing Carrier Solution. Ann. Surg. Oncol. 2017, 24, 990–997. [Google Scholar] [CrossRef] [PubMed]
- Verwaal, V.J.; Funder, J.A.; Sørensen, M.M.; Iversen, L.H. The Impact of Postoperative Complications Following Cytoreductive Surgery Combined with Oxaliplatin Based Heated Intraperitoneal Chemotherapy. Eur. J. Surg. Oncol. 2022, 48, 183–187. [Google Scholar] [CrossRef] [PubMed]
- National Guidelines, Danish Colorectal Cancer Group. Kliniske Retningslinjer for Behandling Af Kolorektal Kræft. Available online: https://dccg.dk/retningslinjer/ (accessed on 29 January 2023). (In Danish).
- Laghi, A.; Bellini, D.; Rengo, M.; Accarpio, F.; Caruso, D.; Biacchi, D.; Giorgio, A.D.; Sammartino, P. Diagnostic Performance of Computed Tomography and Magnetic Resonance Imaging for Detecting Peritoneal Metastases: Systematic Review and Meta-Analysis. Radiol. Medica 2017, 122, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Koumpa, F.S.; Xylas, D.; Konopka, M.; Galea, D.; Veselkov, K.; Antoniou, A.; Mehta, A.; Mirnezami, R. Colorectal Peritoneal Metastases: A Systematic Review of Current and Emerging Trends in Clinical and Translational Research. Gastroenterol. Res. Pract. 2019, 2019, 1–30. [Google Scholar] [CrossRef] [PubMed]
- Bootsma, S.; Bijlsma, M.F.; Vermeulen, L. The Molecular Biology of Peritoneal Metastatic Disease. EMBO Mol. Med. 2023, 15, e15914. [Google Scholar] [CrossRef] [PubMed]
- Kok, H.P.; Cressman, E.N.K.; Ceelen, W.; Brace, C.L.; Ivkov, R.; Grüll, H.; Ter Haar, G.; Wust, P.; Crezee, J. Heating Technology for Malignant Tumors: A Review. Int. J. Hyperth. 2020, 37, 711–741. [Google Scholar] [CrossRef] [PubMed]
- Leopoldo, S.; Lorena, B.; Cinzia, A.; Gabriella, D.C.; Angela Luciana, B.; Renato, C.; Antonio, M.; Carlo, S.; Cristina, P.; Stefano, C.; et al. Two Subtypes of Mucinous Adenocarcinoma of The Colorectum: Clinicopathological and Genetic Features. Ann. Surg. Oncol. 2008, 15, 1429–1439. [Google Scholar] [CrossRef]
- Hugen, N.; Verhoeven, R.H.A.; Radema, S.A.; de Hingh, I.H.J.T.; Pruijt, J.F.M.; Nagtegaal, I.D.; Lemmens, V.E.P.P.; de Wilt, J.H.W. Prognosis and Value of Adjuvant Chemotherapy in Stage III Mucinous Colorectal Carcinoma. Ann. Oncol. 2013, 24, 2819–2824. [Google Scholar] [CrossRef]
- Maisano, R.; Azzarello, D.; Maisano, M.; Mafodda, A.; Bottari, M.; Egitto, G.; Nardi, M. Mucinous Histology of Colon Cancer Predicts Poor Outcomes with FOLFOX Regimen in Metastatic Colon Cancer. J. Chemother. 2012, 24, 212–216. [Google Scholar] [CrossRef]
- Park, J.S.; Huh, J.W.; Park, Y.A.; Cho, Y.B.; Yun, S.H.; Kim, H.C.; Lee, W.Y.; Chun, H.-K. Prognostic Comparison between Mucinous and Nonmucinous Adenocarcinoma in Colorectal Cancer. Medicine 2015, 94, e658. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Hirano, Y.; Heng, G.; Ishii, T.; Kondo, H.; Hara, K.; Obara, N.; Asari, M.; Kato, T.; Yamaguchi, S. Mucinous Adenocarcinoma as a High-Risk Factor in Stage II Colorectal Cancer: A Propensity Score-Matched Study from Japan. Anticancer Res. 2020, 40, 1651–1659. [Google Scholar] [CrossRef] [PubMed]
- Franko, J.; Shi, Q.; Meyers, J.P.; Maughan, T.S.; Adams, R.A.; Seymour, M.T.; Saltz, L.; Punt, C.J.A.; Koopman, M.; Tournigand, C.; et al. Prognosis of Patients with Peritoneal Metastatic Colorectal Cancer given Systemic Therapy: An Analysis of Individual Patient Data from Prospective Randomised Trials from the Analysis and Research in Cancers of the Digestive System (ARCAD) Database. Lancet Oncol. 2016, 17, 1709–1719. [Google Scholar] [CrossRef] [PubMed]
- Rovers, K.P.; Bakkers, C.; Nienhuijs, S.W.; Burger, J.W.A.; Creemers, G.-J.M.; Thijs, A.M.J.; Brandt-Kerkhof, A.R.M.; Madsen, E.V.E.; van Meerten, E.; Tuynman, J.B.; et al. Perioperative Systemic Therapy vs. Cytoreductive Surgery and Hyperthermic Intraperitoneal Chemotherapy Alone for Resectable Colorectal Peritoneal Metastases. JAMA Surg. 2021, 156, 710. [Google Scholar] [CrossRef]
- Rovers, K. Perioperative Systemic Therapy for Isolated Resectable Colorectal Peritoneal Metastases (CAIRO6)-ClinicalTrial.Gov ID: NCT02758951. Available online: https://clinicaltrials.gov/study/NCT02758951 (accessed on 20 December 2023).
- Sullivan, B.G.; Lo, A.; Yu, J.; Gonda, A.; Dehkordi-Vakil, F.; Dayyani, F.; Senthil, M. Circulating Tumor DNA Is Unreliable to Detect Somatic Gene Alterations in Gastrointestinal Peritoneal Carcinomatosis. Ann. Surg. Oncol. 2023, 30, 278–284. [Google Scholar] [CrossRef]
- Zhou, S.; Jiang, Y.; Liang, J.; Pei, W.; Zhou, Z. Neoadjuvant Chemotherapy Followed by Hyperthermic Intraperitoneal Chemotherapy for Patients with Colorectal Peritoneal Metastasis: A Retrospective Study of Its Safety and Efficacy. World J. Surg. Oncol. 2021, 19, 151. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Variable | Patients with Synchronous PM n = 181 | Patients with Metachronous PM n = 129 | p-Value | Total n = 310 |
|---|---|---|---|---|
| Sex (n, %) Male Female | 83 (45.9) 98 (54.1) | 57 (44.2) 72 (55.8) | 0.77 | 140 (45.2) 170 (54.8) |
| Age (median, IQR) | 62 (17) | 64 (15) | 0.35 | 63 (16) |
| ASA score (n, %) 1 2 3 | 68 (37.6) 103 (56.9) 10 (5.5) | 35 (27.1) 88 (68.2) 6 (4.7) | 0.13 | 103 (33.2) 191 (61.6) 16 (5.2) |
| Previous cancer-related surgery (n, %) None Colonic resection • Right-sided • Left-sided • Colectomy Rectal resection Laparoscopy only 1 Laparotomy only Alleviating surgery 2 Gynaecologic surgery N/A | 44 (24.3) 72 (39.8) 49 (68.1) 20 (27.8) 3 (4.2) 7 (3.9) 19 (10.5) 5 (2.8) 31 (17.1) 3 (1.6) 0 (0.0) | 0 (0.0) 114 (88.4) 51 (44.7) 60 (52.6) 3 (2.6) 14 (10.9) 0 (0.0) 0 (0.0) 0 (0.0) 0 (0.0) 1 (0.7) | <0.01 | 44 (14.2) 186 (60.0) 100 (53.8) 80 (43.0) 6 (3.2) 21 (6.8) 19 (6.1) 5 (1.6) 31 (10.0) 3 (1.0) 1 (0.3) |
| Histology of CRS (n, %) Adenocarcinoma, CRC Mucinous adenocarcinoma No malignancy 3 | 122 (67.4) 31 (17.1) 28 (15.5) | 105 (81.4) 10 (7.7) 14 (10.9) | 0.02 | 227 (71.6) 41 (12.9) 42 (13.6) |
| Extraperitoneal metastases prior to CRS+HIPEC (n, %) No 4 Yes | 162 (89.5) 19 (10.5) | 95 (73.6) 34 (26.4) | <0.01 | 257 (82.9) 53 (17.1) |
| Preoperative chemotherapy (n, %) No Yes | 78 (43.1) 103 (56.9) | 88 (68.2) 41 (31.8) | <0.01 | 166 (53.6) 144 (45.4) |
| Year of CRS+HIPEC (n, %) 2006–2010 2011–2015 2016–2020 | 12 (6.6) 42 (23.2) 127 (70.2) | 5 (3.9) 26 (20.1) 98 (76.0) | 0.32 | 17 (5.5) 68 (21.9) 225 (75.6) |
| Median time from resection of primary tumor to CRS+HIPEC (months, IQR) | 4.2 (4.8) 5 n = 159 | 19.5 (16.1) 5 n = 127 | <0.01 | 6.2 (13.4) 5 n = 286 |
| PCI score <6 6–10 >10 Missing 6 | 58 (32.0) 42 (23.2) 32 (17.7) 49 (27.1) | 40 (31.0) 40 (31.0) 19 (14.7) 30 (23.3) | 0.46 | 98 (31.6) 82 (26.5) 51 (16.4) 79 (25.5) |
| Hyperthermic chemotherapy Mitomycin Oxaliplatin None | 88 (48.6) 92 (50.8) 1 (0.6) | 74 (57.4) 55 (42.6) 0 (0.0) | 0.24 | 162 (52.3) 147 (47.4) 1 (0.3) |
| Completeness of cancer resection (CCR) CC0 | 178 (98.3) | 127 (98.5) | 0.94 | 305 (98.4) |
| Pattern of Recurrence | Synchronous PM n = 181 | Metachronous PM n = 129 | p-Value | Total n = 310 |
|---|---|---|---|---|
| Median follow-up (months, IQR) | 11.7 (14.2) | 7.6 (11.2) | - | 10.3 (12.9) |
| Recurrence, n (%) | ||||
| No Yes | 40 (22.1) 141 (77.9) | 23 (17.8) 106 (82.2) | 0.68 0.41 | 63 (20.3) 247 (79.7) |
| Diagnostic modality, n (%) | ||||
| Clinical Computer tomography Perioperatively Lab incl. pathology | 5 (3.5) 119 (84.4) 10 (7.1) 7 (5.0) | 6 (5.7) 95 (89.6) 2 (1.9) 3 (2.8) | - | 11 (4.4) 214 (86.6) 12 (4.9) 10 (4.0) |
| Location of recurrence, n (%) | ||||
| Isolated peritoneal Peritoneal and extraperitoneal Isolated extraperitoneal • Liver • Lungs • Other 1 | 50 (35.5) 26 (18.4) 65 (46.1) 26 (40.0) 16 (24.6) 23 (35.4) | 30 (28.3) 30 (28.3) 46 (43.4) 18 (39.1) 10 (21.7) 18 (39.1) | 0.51 0.38 0.78 - - - | 80 (32.4) 56 (22.7) 111 (44.9) 44 (39.6) 26 (23.4) 41 (36.9) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nielsen, M.F.; Ravn, S.; Sørensen, M.M.; Funder, J.A.; Iversen, L.H. Recurrence and Survival Following Cytoreductive Surgery and Hyperthermic Intraperitoneal Chemotherapy for Synchronous and Metachronous Peritoneal Metastases of Colorectal Origin. Cancers 2024, 16, 631. https://doi.org/10.3390/cancers16030631
Nielsen MF, Ravn S, Sørensen MM, Funder JA, Iversen LH. Recurrence and Survival Following Cytoreductive Surgery and Hyperthermic Intraperitoneal Chemotherapy for Synchronous and Metachronous Peritoneal Metastases of Colorectal Origin. Cancers. 2024; 16(3):631. https://doi.org/10.3390/cancers16030631
Chicago/Turabian StyleNielsen, Mette Fugleberg, Sissel Ravn, Mette Møller Sørensen, Jonas Amstrup Funder, and Lene Hjerrild Iversen. 2024. "Recurrence and Survival Following Cytoreductive Surgery and Hyperthermic Intraperitoneal Chemotherapy for Synchronous and Metachronous Peritoneal Metastases of Colorectal Origin" Cancers 16, no. 3: 631. https://doi.org/10.3390/cancers16030631
APA StyleNielsen, M. F., Ravn, S., Sørensen, M. M., Funder, J. A., & Iversen, L. H. (2024). Recurrence and Survival Following Cytoreductive Surgery and Hyperthermic Intraperitoneal Chemotherapy for Synchronous and Metachronous Peritoneal Metastases of Colorectal Origin. Cancers, 16(3), 631. https://doi.org/10.3390/cancers16030631