
Impact of Pre-Liver Transplant Treatments on the Imaging Accuracy of HCC Staging and Their Influence on Outcomes

 , , , and
, , , and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
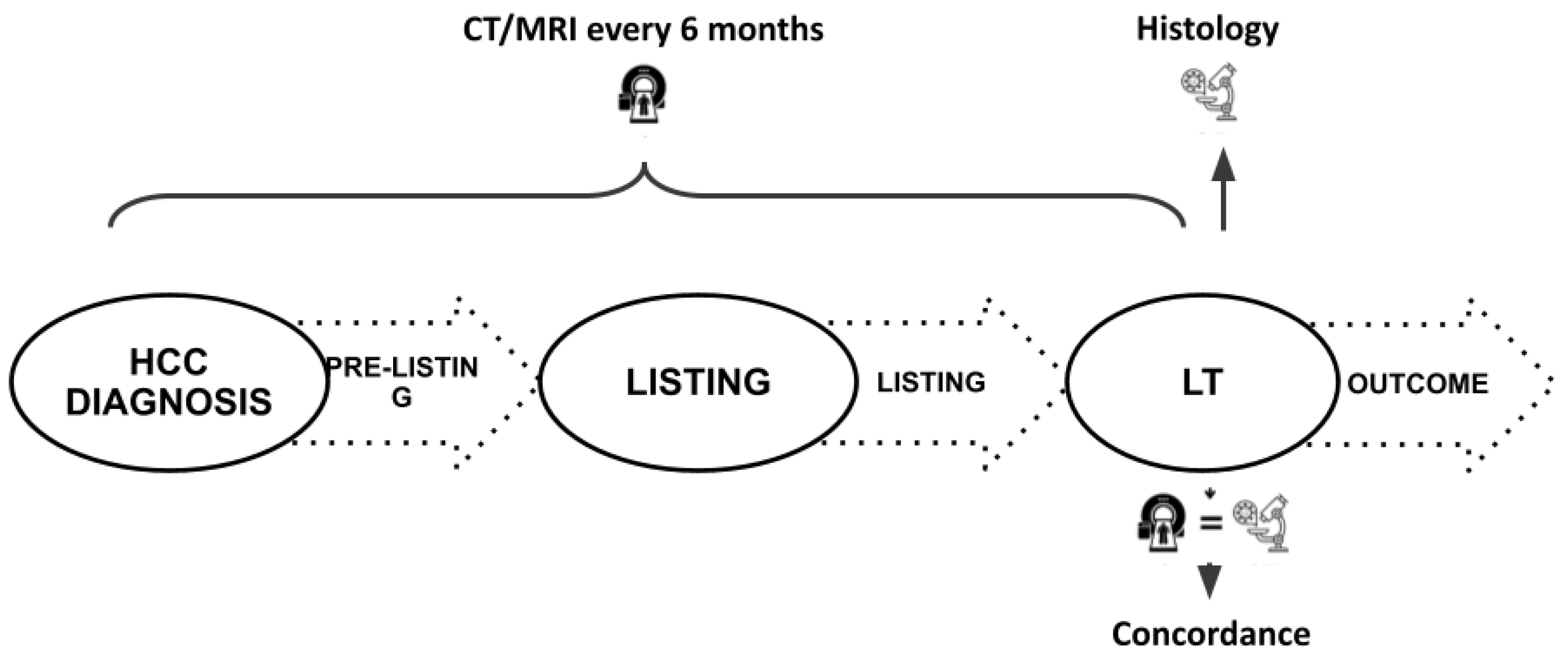
2.1. Study Design
2.2. Patients Management
2.3. Technical Details
2.4. Downstaging and Bridge Therapies
2.5. Statistical Analysis
3. Results
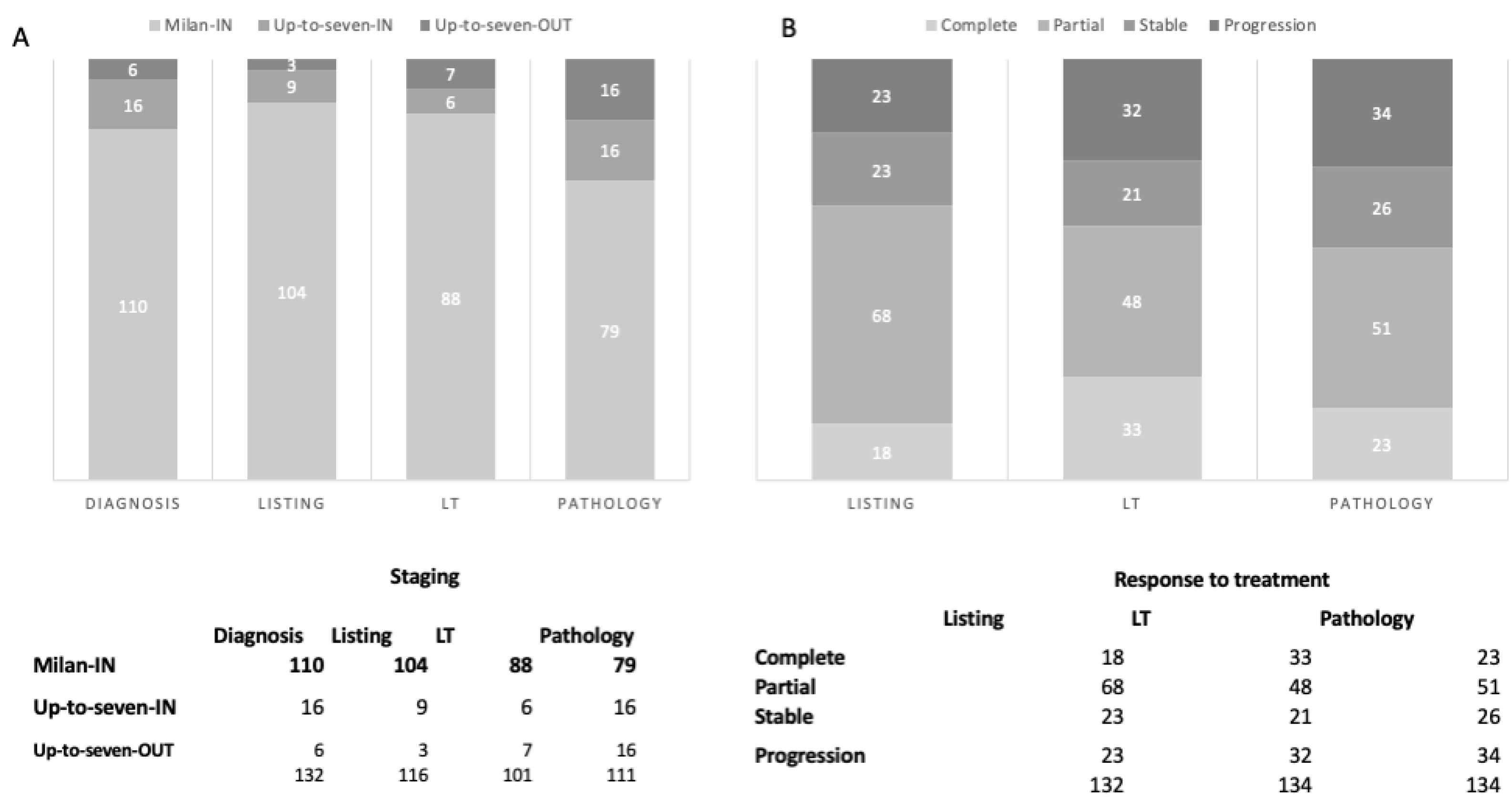
3.1. Comparison between Imaging and Pathology
3.2. Role of Downstaging/Bridging Procedures
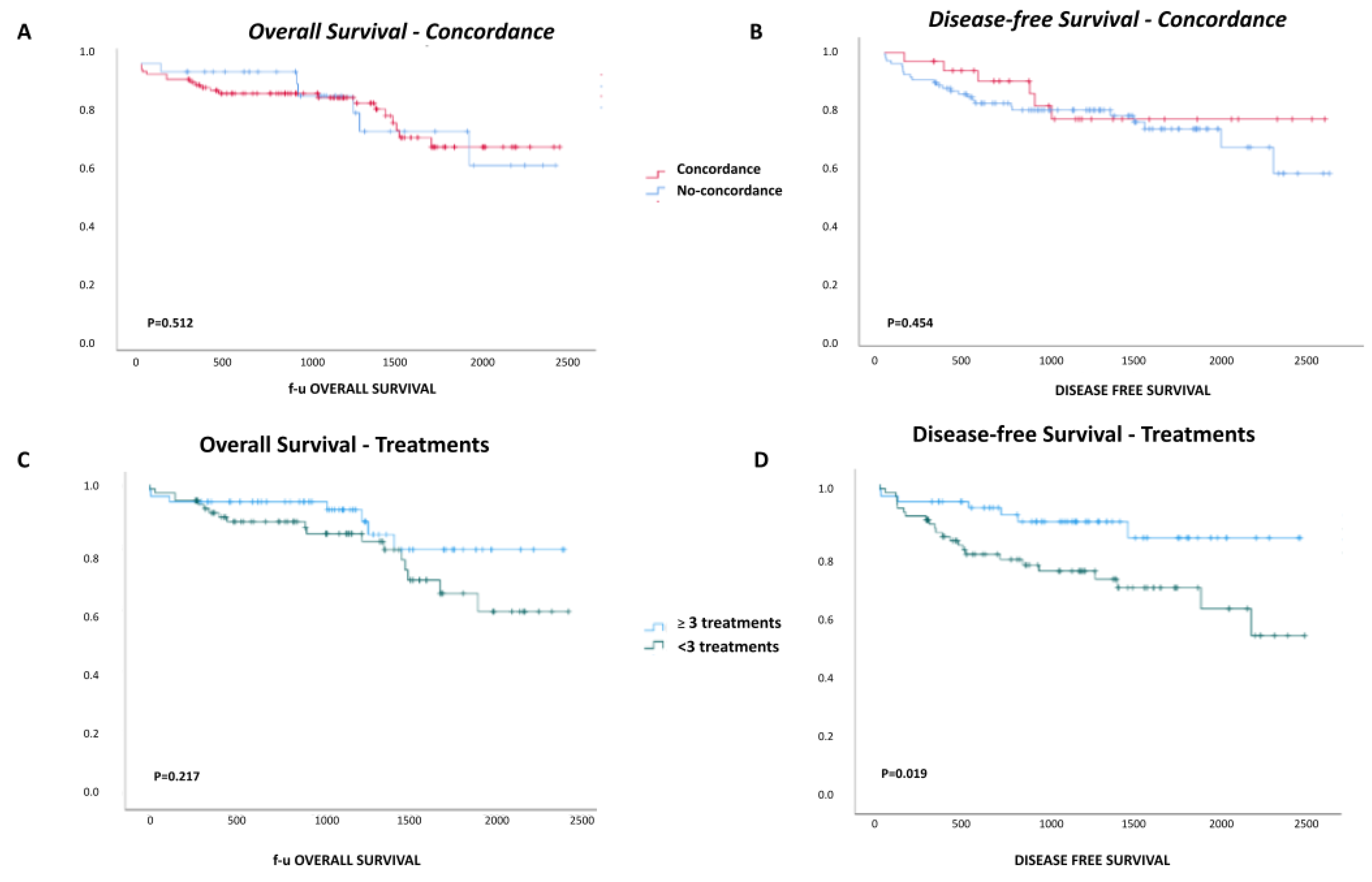
3.3. Impact of HCC Staging
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Adam, R.; Karam, V.; Cailliez, V.; Grady, J.G.O.; Mirza, D.; Cherqui, D.; Klempnauer, J.; Salizzoni, M.; Pratschke, J.; Jamieson, N.; et al. 2018 Annual Report of the European Liver Transplant Registry (ELTR)—50-Year Evolution of Liver Transplantation. Transpl. Int. 2018, 31, 1293–1317. [Google Scholar] [CrossRef] [PubMed]
- Belghiti, J.; Fuks, D. Liver Resection and Transplantation in Hepatocellular Carcinoma. Liver Cancer 2012, 1, 71–82. [Google Scholar] [CrossRef] [PubMed]
- Cunha, G.M.; Hosseini, M.; Furlan, A.; Fowler, K.J. Hepatocellular Carcinoma Staging: Differences Between Radiologic and Pathologic Systems and Relevance to Patient Selection and Outcomes in Liver Transplantation. AJR Am. J. Roentgenol. 2022, 218, 77–86. [Google Scholar] [CrossRef]
- Yao, F.Y.; Ferrell, L.; Bass, N.M.; Bacchetti, P.; Ascher, N.L.; Roberts, J.P. Liver Transplantation for Hepatocellular Carcinoma: Comparison of the Proposed UCSF Criteria with the Milan Criteria and the Pittsburgh Modified TNM Criteria. Liver Transplant. 2002, 8, 765–774. [Google Scholar] [CrossRef]
- Llovet, J.M.; Pavel, M.; Rimola, J.; Diaz, M.A.; Colmenero, J.; Saavedra-Perez, D.; Fondevila, C.; Ayuso, C.; Fuster, J.; Ginès, P.; et al. Pilot Study of Living Donor Liver Transplantation for Patients with Hepatocellular Carcinoma Exceeding Milan Criteria (Barcelona Clinic Liver Cancer Extended Criteria). Liver Transplant. 2018, 24, 369–379. [Google Scholar] [CrossRef] [PubMed]
- Halazun, K.J.; Sapisochin, G.; von Ahrens, D.; Agopian, V.G.; Tabrizian, P. Predictors of Outcome after Liver Transplantation for Hepatocellular Carcinoma (HCC) beyond Milan Criteria. Int. J. Surg. 2020, 82S, 61–69. [Google Scholar] [CrossRef]
- Mazzaferro, V.; Llovet, J.M.; Miceli, R.; Bhoori, S.; Schiavo, M.; Mariani, L.; Camerini, T.; Roayaie, S.; Schwartz, M.E.; Grazi, G.L.; et al. Predicting Survival after Liver Transplantation in Patients with Hepatocellular Carcinoma beyond the Milan Criteria: A Retrospective, Exploratory Analysis. Lancet Oncol. 2009, 10, 35–43. [Google Scholar] [CrossRef]
- Lencioni, R.; Llovet, J.M. Modified RECIST (mRECIST) Assessment for Hepatocellular Carcinoma. Semin. Liver Dis. 2010, 30, 52–60. [Google Scholar] [CrossRef]
- Kamath, P.S.; Kim, W.R. The Model for End-Stage Liver Disease (MELD). Hepatology 2007, 45, 797–805. [Google Scholar] [CrossRef]
- Mazzaferro, V.; Sposito, C.; Zhou, J.; Pinna, A.D.; De Carlis, L.; Fan, J.; Cescon, M.; Di Sandro, S.; Yi-Feng, H.; Lauterio, A.; et al. Metroticket 2.0 Model for Analysis of Competing Risks of Death After Liver Transplantation for Hepatocellular Carcinoma. Gastroenterology 2018, 154, 128–139. [Google Scholar] [CrossRef]
- Belghiti, J.; Panis, Y.; Sauvanet, A.; Gayet, B.; Fékété, F. A New Technique of Side to Side Caval Anastomosis during Orthotopic Hepatic Transplantation without Inferior Vena Caval Occlusion. Surg. Gynecol. Obstet. 1992, 175, 270–272. [Google Scholar] [PubMed]
- Eisenhauer, E.A.; Verweij, J. 11 New Response Evaluation Criteria in Solid Tumors: RECIST GUIDELINE VERSION 1.1. EJC Suppl. 2009, 7, 5. [Google Scholar] [CrossRef]
- Ruch, B.; Wagler, J.; Kumm, K.; Zhang, C.; Katariya, N.N.; Garcia-Saenz-de-Sicilia, M.; Giorgakis, E.; Mathur, A.K. Hepatocellular Carcinoma, Alpha Fetoprotein, and Liver Allocation for Transplantation: Past, Present and Future. Curr. Oncol. 2022, 29, 7537–7551. [Google Scholar] [CrossRef] [PubMed]
- Sotiropoulos, G.C.; Paul, A.; Molmenti, E.; Lang, H.; Frilling, A.; Napieralski, B.P.; Nadalin, S.; Treckmann, J.; Brokalaki, E.I.; Gerling, T.; et al. Liver Transplantation for Hepatocellular Carcinoma in Cirrhosis within the Eurotransplant Area: An Additional Option with “Livers That Nobody Wants”. Transplantation 2005, 80, 897–902. [Google Scholar] [CrossRef] [PubMed]
- Tovoli, F.; Renzulli, M.; Negrini, G.; Brocchi, S.; Ferrarini, A.; Andreone, A.; Benevento, F.; Golfieri, R.; Morselli-Labate, A.M.; Mastroroberto, M.; et al. Inter-Operator Variability and Source of Errors in Tumour Response Assessment for Hepatocellular Carcinoma Treated with Sorafenib. Eur. Radiol. 2018, 28, 3611–3620. [Google Scholar] [CrossRef]
- Vicentin, I.; Mosconi, C.; Garanzini, E.; Sposito, C.; Serenari, M.; Buscemi, V.; Verna, M.; Spreafico, C.; Golfieri, R.; Mazzaferro, V.; et al. Inter-Center Agreement of mRECIST in Transplanted Patients for Hepatocellular Carcinoma. Eur. Radiol. 2021, 31, 8903–8912. [Google Scholar] [CrossRef] [PubMed]
- Ecker, B.L.; Hoteit, M.A.; Forde, K.A.; Hsu, C.C.; Reddy, K.R.; Furth, E.E.; Siegelman, E.S.; Habibollahi, P.; Ben-Josef, E.; Porrett, P.M.; et al. Patterns of Discordance Between Pretransplant Imaging Stage of Hepatocellular Carcinoma and Posttransplant Pathologic Stage: A Contemporary Appraisal of the Milan Criteria. Transplantation 2018, 102, 648–655. [Google Scholar] [CrossRef]
- Vigano, L.; Terrone, A.; Costa, G.; Franchi, E.; Cimino, M.; Procopio, F.; Del Fabbro, D.; Torzilli, G. Effect of Chemotherapy on Tumour-Vessel Relationship in Colorectal Liver Metastases. Br. J. Surg. 2022, 109, 401–404. [Google Scholar] [CrossRef]
- Lee Cheah, Y.; Chow, P.K.H. Liver Transplantation for Hepatocellular Carcinoma: An Appraisal of Current Controversies. Liver Cancer 2012, 1, 183–189. [Google Scholar] [CrossRef]
- Nadarevic, T.; Giljaca, V.; Colli, A.; Fraquelli, M.; Casazza, G.; Miletic, D.; Štimac, D. Computed Tomography for the Diagnosis of Hepatocellular Carcinoma in Adults with Chronic Liver Disease. Cochrane Database Syst. Rev. 2021, 10, CD013362. [Google Scholar] [CrossRef]
- Roberts, L.R.; Sirlin, C.B.; Zaiem, F.; Almasri, J.; Prokop, L.J.; Heimbach, J.K.; Murad, M.H.; Mohammed, K. Imaging for the Diagnosis of Hepatocellular Carcinoma: A Systematic Review and Meta-Analysis. Hepatology 2018, 67, 401–421. [Google Scholar] [CrossRef] [PubMed]
- Moura Cunha, G.; Chernyak, V.; Fowler, K.J.; Sirlin, C.B. Up-to-Date Role of CT/MRI LI-RADS in Hepatocellular Carcinoma. J. Hepatocell. Carcinoma 2021, 8, 513–527. [Google Scholar] [CrossRef] [PubMed]
- Ayuso, C.; Rimola, J.; Vilana, R.; Burrel, M.; Darnell, A.; García-Criado, Á.; Bianchi, L.; Belmonte, E.; Caparroz, C.; Barrufet, M.; et al. Diagnosis and Staging of Hepatocellular Carcinoma (HCC): Current Guidelines. Eur. J. Radiol. 2018, 101, 72–81. [Google Scholar] [CrossRef] [PubMed]
- Krinsky, G.A.; Lee, V.S.; Theise, N.D.; Weinreb, J.C.; Morgan, G.R.; Diflo, T.; John, D.; Teperman, L.W.; Goldenberg, A.S. Transplantation for Hepatocellular Carcinoma and Cirrhosis: Sensitivity of Magnetic Resonance Imaging. Liver Transplant. 2002, 8, 1156–1164. [Google Scholar] [CrossRef] [PubMed]
- Grąt, K.; Grąt, M.; Rowiński, O.; Patkowski, W.; Zieniewicz, K.; Pacho, R. Accuracy of Computed Tomography in the Assessment of Milan Criteria in Liver Transplantation for Hepatocellular Carcinoma. Transplant. Proc. 2018, 50, 2002–2005. [Google Scholar] [CrossRef] [PubMed]
- Jeng, K.-S.; Huang, C.-C.; Lin, C.-K.; Lin, C.-C.; Huang, C.-T.; Chung, C.-S.; Weng, M.-T.; Chen, K.-H. Reappraisal of Failures in Downstaging Treatment of Hepatocellular Carcinoma Prior to Liver Transplant-Preliminary Report on the Impact of Underestimations of Tumor Numbers and Tumor Sizes as Measured From Imaging Before Transplant. Transplant. Proc. 2019, 51, 1428–1434. [Google Scholar] [CrossRef]
- Agopian, V.G.; Harlander-Locke, M.P.; Ruiz, R.M.; Klintmalm, G.B.; Senguttuvan, S.; Florman, S.S.; Haydel, B.; Hoteit, M.; Levine, M.H.; Lee, D.D.; et al. Impact of Pretransplant Bridging Locoregional Therapy for Patients With Hepatocellular Carcinoma Within Milan Criteria Undergoing Liver Transplantation: Analysis of 3601 Patients From the US Multicenter HCC Transplant Consortium. Ann. Surg. 2017, 266, 525–535. [Google Scholar] [CrossRef]
- Shimada, S.; Shamaa, T.; Ivanics, T.; Kitajima, T.; Adhnan, M.; Collins, K.; Rizzari, M.; Yoshida, A.; Abouljoud, M.; Salgia, R.; et al. Multiple Pretransplant Treatments for Patients Without Pathological Complete Response May Worsen Posttransplant Outcomes in Patients with Hepatocellular Carcinoma. Ann. Surg. Oncol. 2022, 30, 1408–1419. [Google Scholar] [CrossRef]
- Rana, A.; Hardy, M.A.; Halazun, K.J.; Woodland, D.C.; Ratner, L.E.; Samstein, B.; Guarrera, J.V.; Brown, R.S., Jr.; Emond, J.C. Survival Outcomes Following Liver Transplantation (SOFT) Score: A Novel Method to Predict Patient Survival Following Liver Transplantation. Am. J. Transpl. 2008, 8, 2537–2546. [Google Scholar] [CrossRef]
- Cucchetti, A.; Serenari, M.; Sposito, C.; Di Sandro, S.; Mosconi, C.; Vicentin, I.; Garanzini, E.; Mazzaferro, V.; De Carlis, L.; Golfieri, R.; et al. Including mRECIST in the Metroticket 2.0 Criteria Improves Prediction of Hepatocellular Carcinoma-Related Death after Liver Transplant. J. Hepatol. 2020, 73, 342–348. [Google Scholar] [CrossRef]
- Parfitt, J.R.; Marotta, P.; Alghamdi, M.; Wall, W.; Khakhar, A.; Suskin, N.G.; Quan, D.; McAllister, V.; Ghent, C.; Levstik, M.; et al. Recurrent Hepatocellular Carcinoma after Transplantation: Use of a Pathological Score on Explanted Livers to Predict Recurrence. Liver Transplant. 2007, 13, 543–551. [Google Scholar] [CrossRef]
- Iwatsuki, S.; Dvorchik, I.; Marsh, J.W.; Madariaga, J.R.; Carr, B.; Fung, J.J.; Starzl, T.E. Liver Transplantation for Hepatocellular Carcinoma: A Proposal of a Prognostic Scoring system11No Competing Interests Declared. J. Am. Coll. Surg. 2000, 191, 389–394. [Google Scholar] [CrossRef]
- Decaens, T.; Roudot-Thoraval, F.; Badran, H.; Wolf, P.; Durand, F.; Adam, R.; Boillot, O.; Vanlemmens, C.; Gugenheim, J.; Dharancy, S.; et al. Impact of Tumour Differentiation to Select Patients before Liver Transplantation for Hepatocellular Carcinoma. Liver Int. 2011, 31, 792–801. [Google Scholar] [CrossRef] [PubMed]
- Mehta, N.; Heimbach, J.; Harnois, D.M.; Sapisochin, G.; Dodge, J.L.; Lee, D.; Burns, J.M.; Sanchez, W.; Greig, P.D.; Grant, D.R.; et al. Validation of a Risk Estimation of Tumor Recurrence After Transplant (RETREAT) Score for Hepatocellular Carcinoma Recurrence After Liver Transplant. JAMA Oncol. 2017, 3, 493–500. [Google Scholar] [CrossRef] [PubMed]
- Mehta, N.; Dodge, J.L.; Roberts, J.P.; Yao, F.Y. Validation of the Prognostic Power of the RETREAT Score for Hepatocellular Carcinoma Recurrence Using the UNOS Database. Am. J. Transpl. 2018, 18, 1206–1213. [Google Scholar] [CrossRef]
- Mehta, N.; Yao, F.Y. What Are the Optimal Liver Transplantation Criteria for Hepatocellular Carcinoma? Clin. Liver Dis. 2019, 13, 20–25. [Google Scholar] [CrossRef] [PubMed]
- Costentin, C.; Piñero, F.; Degroote, H.; Notarpaolo, A.; Boin, I.F.; Boudjema, K.; Baccaro, C.; Podestá, L.G.; Bachellier, P.; Ettorre, G.M.; et al. R3-AFP Score Is a New Composite Tool to Refine Prediction of Hepatocellular Carcinoma Recurrence after Liver Transplantation. JHEP Rep. 2022, 4, 100445. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Patients (n = 134) | |
|---|---|
| FEATURES | |
| Age, years | 59 (36–71) |
| Gender, M, n (%) | 113 (84.3) |
| HCV RNA positive, n (%) | 29 (21.6) |
| Donor age, years | 64 (17–88) |
| N° (%) of patients treated at least one time with: | |
| - TACE | 95 (70.9) |
| - TARE | 1 (0.7) |
| - RFTA/MWTA | 53 (39.6) |
| - Liver resection, open | 11 (8.2) |
| - Liver resection, laparoscopic | 6 (4.5) |
| - PEI | 7 (5.2) |
| AT LISTING | |
| AFP, ng/mL | 10 (1–3721) |
| MELD | 11 (2–31) |
| HCC, n (%) | 132 (98.5) |
| Time from diagnosis to listing, days | 379 (−74–5673) |
| AT LIVER TRANSPLANTATION | |
| AFP, ng/mL | 9 (1–60500) |
| MELD | 11 (3–31) |
| Imaging, n (%) | |
| - TC | 123 (91.8) |
| - RM | 11 (8.2) |
| HCC, n (%) | 101 (75.4) |
| Active nodules, n | 2 (1–7) |
| Larger active nodule, diameter, mm | 16 (4–45) |
| Active nodules, total diameter, mm | 25 (4–108) |
| Macrovascular invasion, n (%) * | 1 (1.0) |
| Metroticket 2.0 | 94.1 (42.4–97.6) |
| Last imaging–LT interval, days | 52 (1–154) |
| Presentation–LT interval, days | 499.5 (41–5769) |
| Waiting time, days | 73 (2–1328) |
| AT PATHOLOGICAL EXAMINATION | |
| HCC nodules, n. (%) | 111 (82.8) |
| Active nodules, n. | 2 (1–22) |
| Larger active nodule, diameter, mm | 22 (6–78) |
| Actrive nodules, total diameter, mm | 38 (8–239) |
| Microvascular invasion, n (%) ° | 29 (26.1) |
| Edmondson grade, n (%) ° | |
| - 1 | 7 (6.3) |
| - 2 | 32 (28.8) |
| - 3 | 66 (59.5) |
| - 4 | 6 (5.4) |
| Metroticket original | 72.1 (41.1–78.4) |
| Concordant (n = 32) | Non Concordant (n = 102) | p Value | |
|---|---|---|---|
| Age, years | 59.5 (49–71) | 59 (36–71) | 0.581 |
| Gender, M, n (%) | 26 (81.2) | 87 (85.3) | 0.584 |
| MELD at listing | 11 (6–26) | 11 (2–31) | 0.297 |
| AFP level at listing, ng/mL | 9 (1–864) | 11.5 (1–3721) | 0.581 |
| MELD at LT | 10 (6–30) | 11 (3–31) | 0.899 |
| AFP at LT, ng/mL | 9.5 (2–755) | 9 (1–60500) | 0.581 |
| Donor age, years | 60 (18–80) | 65 (17–88) | 0.074 |
| Waiting time, days | 73 (6–1328) | 73 (2–1170) | 0.512 |
| LT–HCC recurrence interval, days | 510 (107–820) | 360 (96–2124) | 0.835 |
| Last imaging–LT interval, days | 54 (12–154) | 50 (1–147) | 0.308 |
| Treatment ≥ 3, n (%) | 13 (40.6) | 66 (64.7) | 0.014 |
| Everolimus, n (%) | 4 (12.5) | 24 (23.5) | 0.107 |
| HCC recurrence, n (%) | 5 (15.6) | 13 (12.7) | 0.437 |
| Time from HCC diagnosis to LT, days | 455.5 (63–1572) | 591.5 (4–5769) | 0.062 |
| Overall patients’ survival, n (%) | |||
| - 1 year | 31 (96.9) | 93 (91.1) | 0.945 |
| - 3 years | 29 (87.6) | 90 (87.3) | |
| - 5 years | 27 (74.4) | 83 (69.2) | |
| Disease-free survival, n (%) | |||
| - 1 year | 30 (93.5) | 88 (86.2) | 0.454 |
| - 3 years | 26 (76.1) | 82 (79.3) | |
| - 5 years | 26 (76.1) | 79 (72.5) | |
| AT PATHOLOGICAL EXAMINATION | |||
| Nodules, n. | 2 (1–4) | 3 (1–29) | 0.004 |
| Nodules, total diameter, mm | 35 (8–61) | 59 (8–271) | 0.001 |
| Large nodule, diameter, mm | 22 (8–45) | 25 (8–78) | 0.066 |
| Active nodules, n. | 2 (1–3) | 2 (1–22) | 0.019 |
| Active nodules, diameter, mm | 32 (8–61) | 40.5 (8–239) | 0.026 |
| Larger active nodule, diameter, mm | 21 (8–45) | 22.5 (6–78) | 0.348 |
| Active nodules, total diameter, mm | 23 (3–34) | 26 (1–78) | 0.097 |
| Metroticket original, % | 73.8 (48.7–78.4) | 70.4 (41.1–78.4) | 0.081 |
| TNM, n (%) ** | |||
| - ≤1 | 10 (37.0) | 20 (23.8) | 0.108 |
| - >1 | 17 (63.0) | 64 (76.2) | |
| Edmondson grade, n (%) ** | |||
| - ≤2 | 7 (25.9) | 32 (38.1) | 0.149 |
| - >2 | 20 (74.1) | 52 (61.9) | |
| Microsatellite, n (%) | 2 (6.3) | 19 (18.6) | 0.054 |
| Microvascular invasion, n (%) | 6 (18.8) | 23 (22.5) | 0.427 |
| Staging, n (%) | |||
| - Milan-in | 31 (96.9) | 71 (69.6) | 0.002 |
| - Up-to-Seven-in | 1 (3.1) | 15 (14.7) | |
| - Up-to-Seven-out | 0 (0.0) | 16 (15.7) | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Franchi, E.; Dondossola, D.E.; Marini, G.M.F.; Iavarone, M.; Del Prete, L.; Di Benedetto, C.; Donato, M.F.; Antonelli, B.; Lampertico, P.; Caccamo, L. Impact of Pre-Liver Transplant Treatments on the Imaging Accuracy of HCC Staging and Their Influence on Outcomes. Cancers 2024, 16, 1043. https://doi.org/10.3390/cancers16051043
Franchi E, Dondossola DE, Marini GMF, Iavarone M, Del Prete L, Di Benedetto C, Donato MF, Antonelli B, Lampertico P, Caccamo L. Impact of Pre-Liver Transplant Treatments on the Imaging Accuracy of HCC Staging and Their Influence on Outcomes. Cancers. 2024; 16(5):1043. https://doi.org/10.3390/cancers16051043
Chicago/Turabian StyleFranchi, Eloisa, Daniele Eliseo Dondossola, Giulia Maria Francesca Marini, Massimo Iavarone, Luca Del Prete, Clara Di Benedetto, Maria Francesca Donato, Barbara Antonelli, Pietro Lampertico, and Lucio Caccamo. 2024. "Impact of Pre-Liver Transplant Treatments on the Imaging Accuracy of HCC Staging and Their Influence on Outcomes" Cancers 16, no. 5: 1043. https://doi.org/10.3390/cancers16051043
APA StyleFranchi, E., Dondossola, D. E., Marini, G. M. F., Iavarone, M., Del Prete, L., Di Benedetto, C., Donato, M. F., Antonelli, B., Lampertico, P., & Caccamo, L. (2024). Impact of Pre-Liver Transplant Treatments on the Imaging Accuracy of HCC Staging and Their Influence on Outcomes. Cancers, 16(5), 1043. https://doi.org/10.3390/cancers16051043