
Availability and Access to Orphan Drugs for Rare Cancers in Bulgaria: Analysis of Delays and Public Expenditures

 , and
, and
Abstract
:Simple Summary
Abstract
1. Introduction
1.1. Background
1.2. Rare Cancer Policies
1.3. Access to Orphan Cancer Therapies in the EU and Bulgaria
1.4. Rare Cancer Policies in Bulgaria
2. Materials and Methods
2.1. Study Design
2.2. Definitions
2.3. Data Collection
2.4. Data Analysis
3. Results
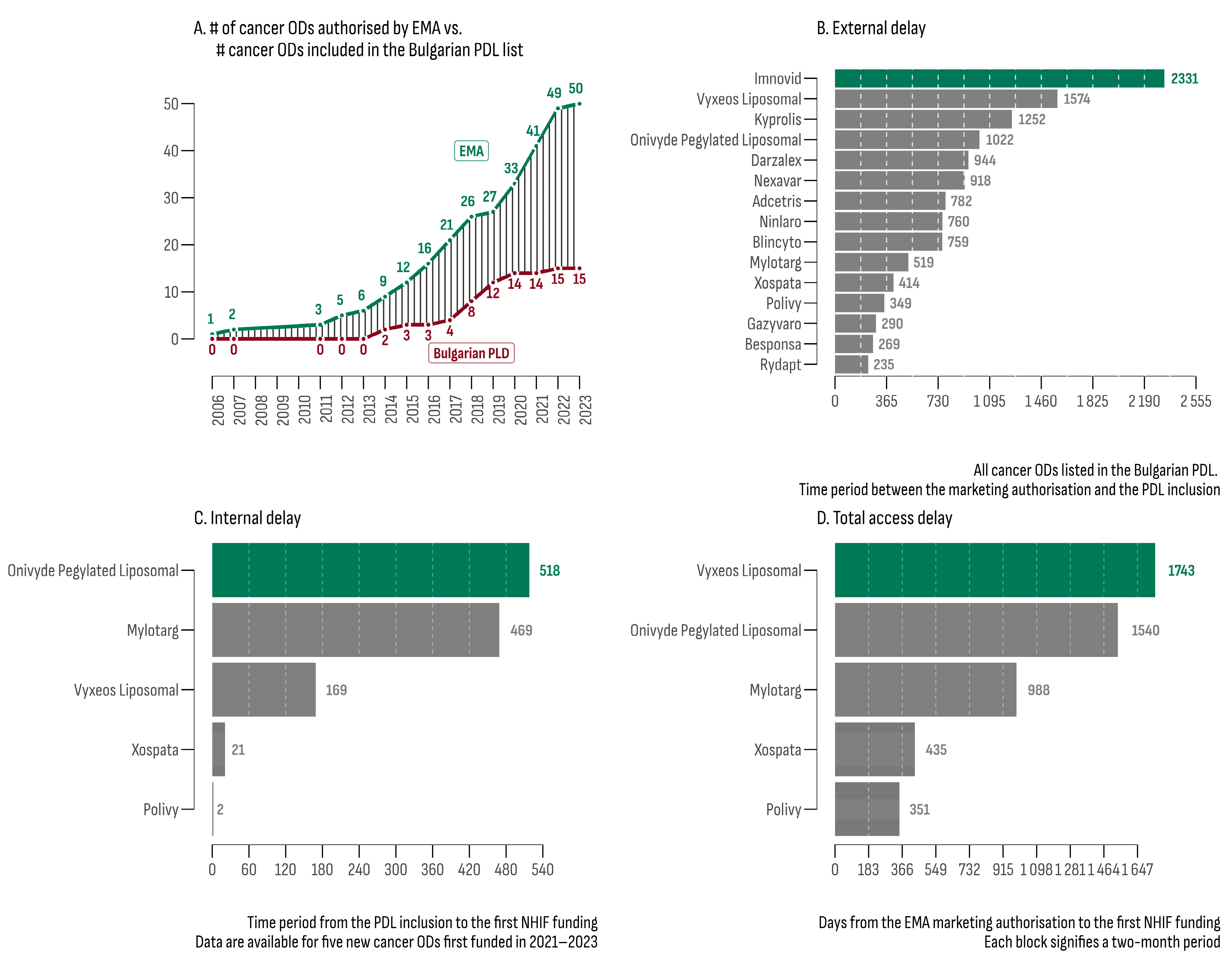
3.1. Number of Available Cancer ODs and Their Access Delay
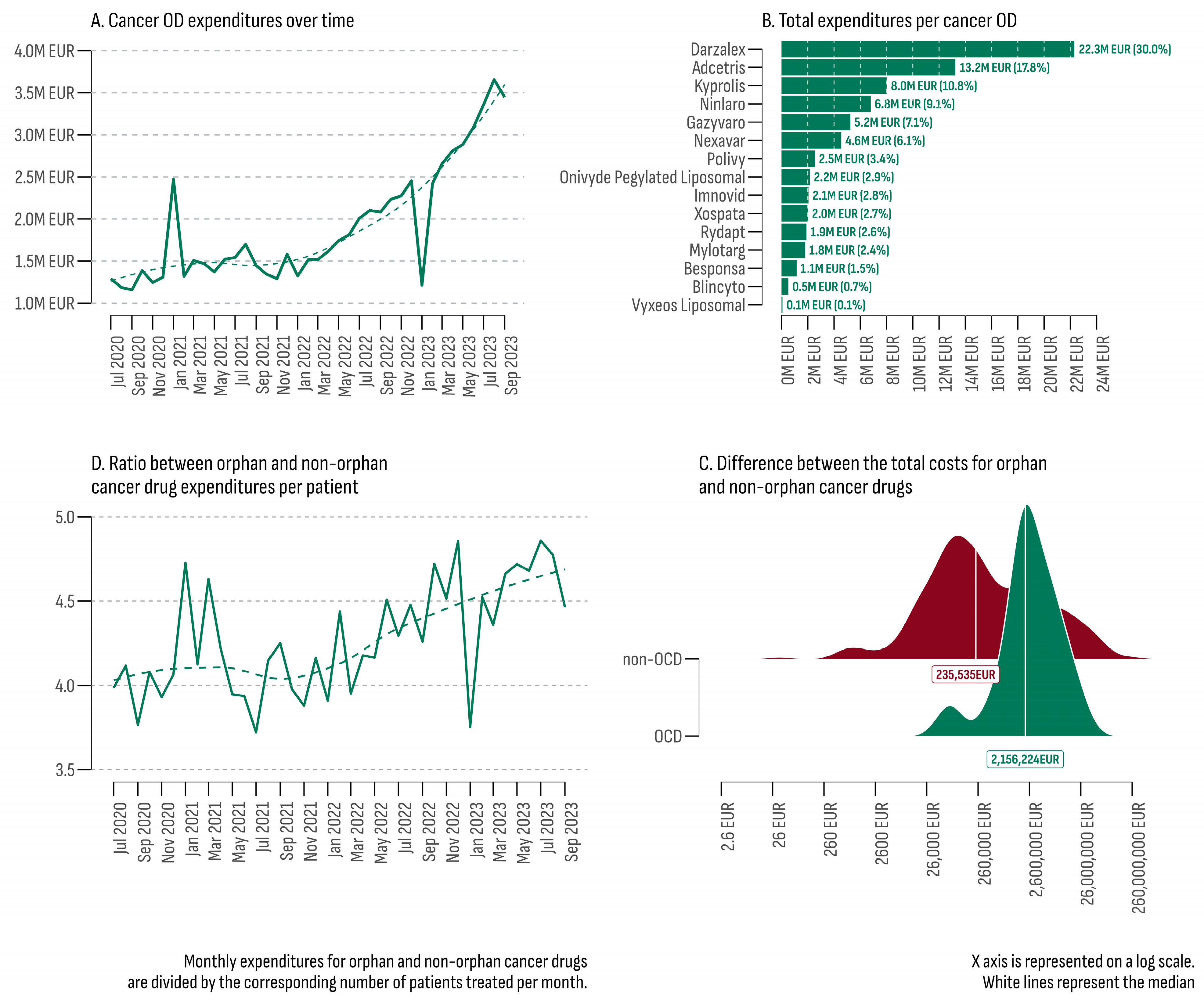
3.2. Expenditures of Accessible OD Cancer Drugs and Their Budgetary Impact
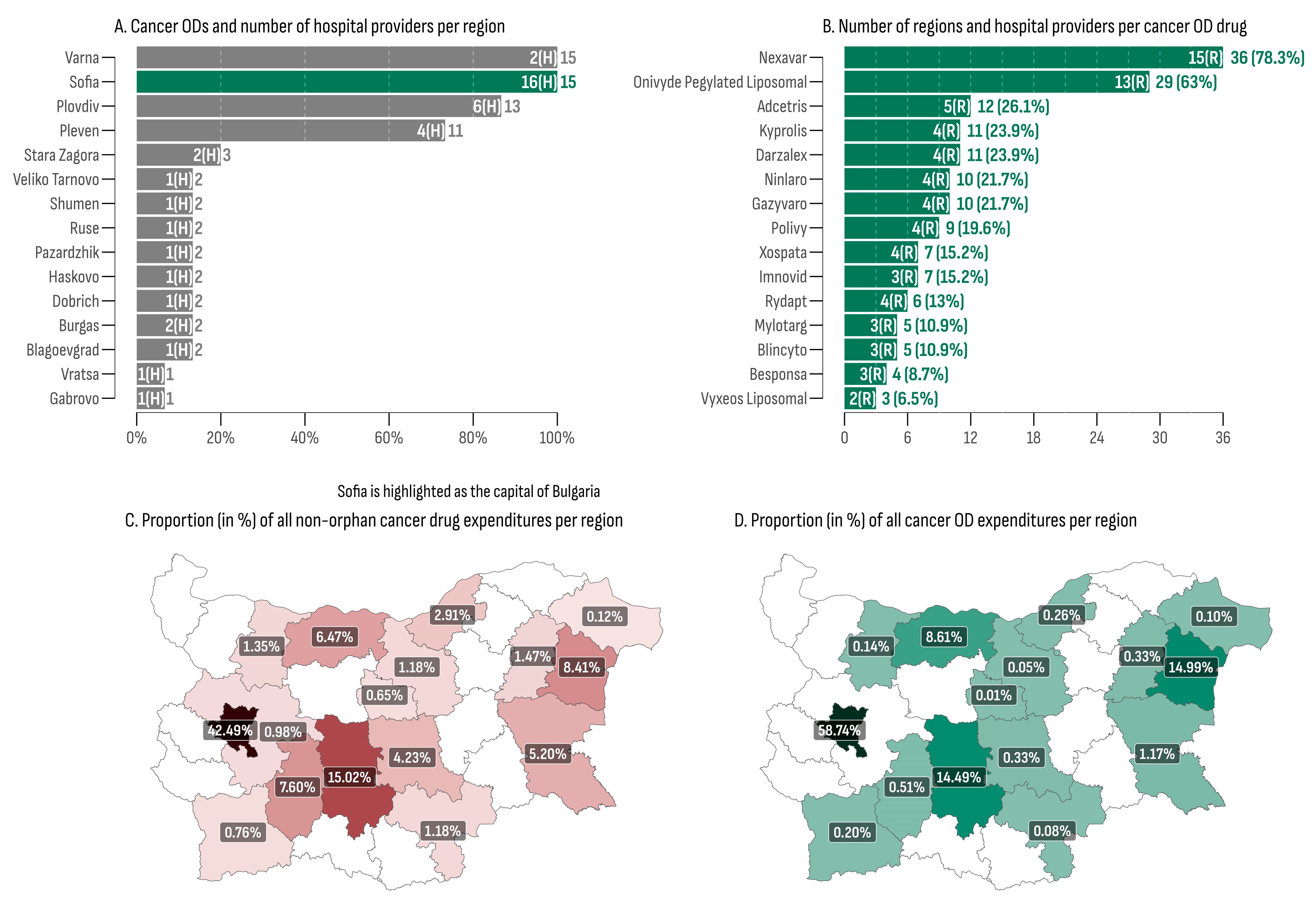
3.3. Regional Differences in Access and Expenditures for Cancer ODs
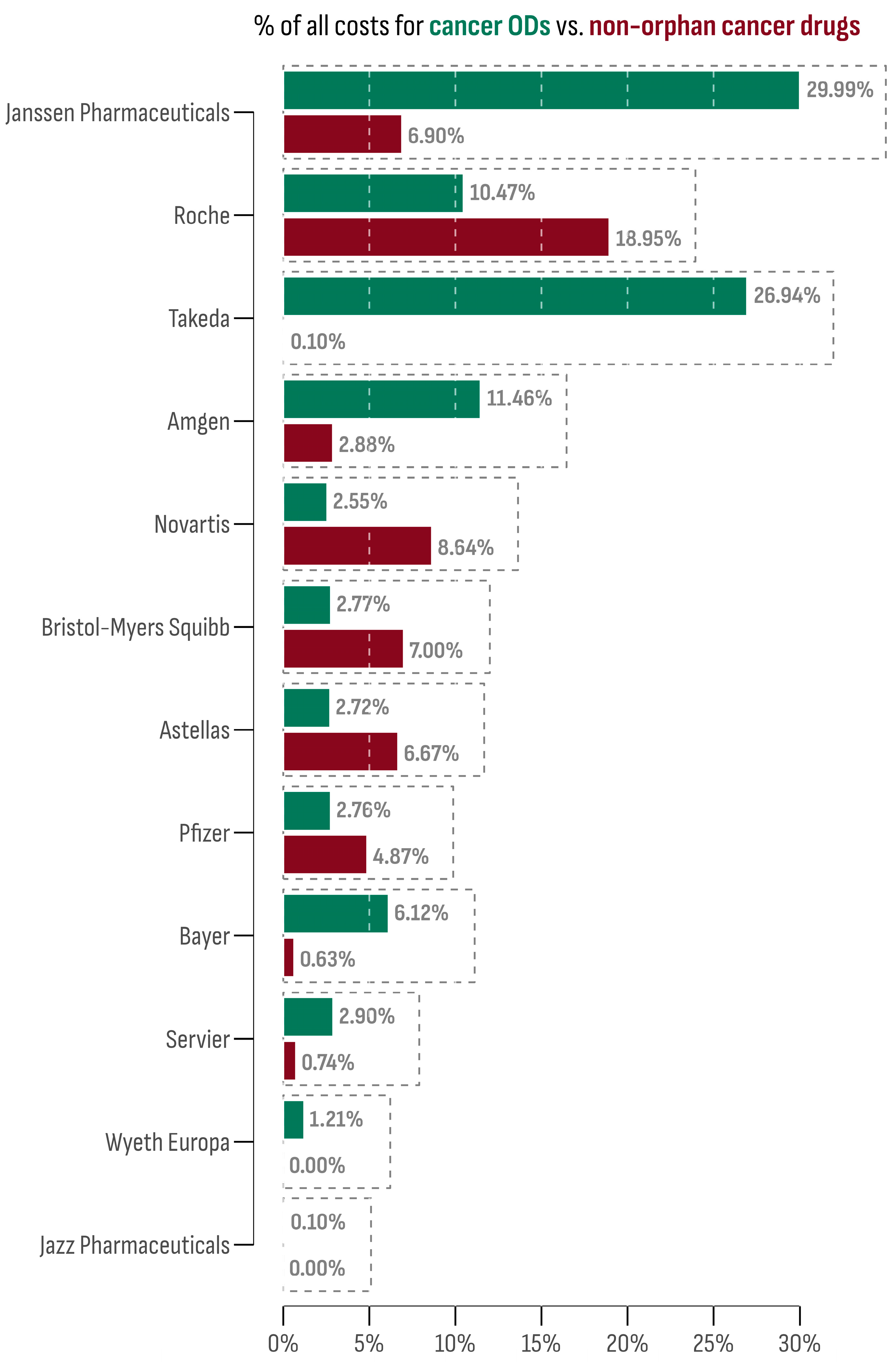
3.4. Comparative Profile of Market Authorization Holders
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- JARC—Joint Action on Rare Cancers Rare Cancer Agenda—2030. Rare Cancers Europe 2022. Available online: https://www.esmo.org/policy/rare-cancers-working-group/rare-cancers-in-europe/rare-cancer-agenda-2030 (accessed on 3 January 2024).
- European Society for Medical Oncology—ESMO. Available online: https://www.esmo.org/ (accessed on 3 January 2024).
- de la Paz, M.P.; Taruscio, D.; Groft, S.C. (Eds.) Rare Diseases Epidemiology: Update and Overview|SpringerLink; Advances in Experimental Medicine and Biology 686; Springer: Dordrecht, The Netherlands, 2010; ISBN 978-3-319-67144-4. Available online: https://link.springer.com/book/10.1007/978-3-319-67144-4 (accessed on 3 January 2024).
- Law of 10 November 2021/No. 175. Provisions for the Treatment of Rare Diseases and the Support of Research and Production of Orphan Drugs. (21G00189) [LEGGE 10 November 2021/n. 175. Disposizioni Per la Cura Delle Malattie Rare e Per il Sostegno Della Ricerca e Della Produzione Dei Farmaci Orfani. (21G00189)] 2021. Available online: https://www.gazzettaufficiale.it/eli/gu/2021/11/27/283/sg/pdf (accessed on 3 January 2024).
- Commission Staff Working Document EU Missions Two Years on: An Assessment of Progress in Shaping the Future We Want and Reporting on the Review of Mission Areas and Areas for Institutionalised Partnerships Based on Articles 185 and 187 TFEU Accompanying the Document Communication From the Commission to the European Parliament, the Council, the European Economic and Social Committee and the Committee of the Regions EU Missions Two Years on: Assessment of Progress and Way Forward 2023. Available online: https://eur-lex.europa.eu/legal-content/EN/ALL/?uri=CELEX:52023SC0260 (accessed on 3 January 2024).
- Gatta, G.; Capocaccia, R.; Botta, L.; Mallone, S.; De Angelis, R.; Ardanaz, E.; Comber, H.; Dimitrova, N.; Leinonen, M.K.; Siesling, S.; et al. Burden and centralised treatment in Europe of rare tumours: Results of RARECAREnet—A population-based study. Lancet Oncol. 2017, 18, 1022–1039. [Google Scholar] [CrossRef] [PubMed]
- Gatta, G.; van der Zwan, J.M.; Casali, P.G.; Siesling, S.; Dei Tos, A.P.; Kunkler, I.; Otter, R.; Licitra, L.; Mallone, S.; Tavilla, A.; et al. Rare cancers are not so rare: The rare cancer burden in europe. Eur. J. Cancer 2011, 47, 2493–2511. [Google Scholar] [CrossRef] [PubMed]
- Iskrov, G.; Stefanov, R. Rare tumors—Epidemiological and public health aspects. Rare Dis. Orphan Drugs J. 2018, 9, 9–13. (In Bulgarian) [Google Scholar] [CrossRef]
- Van Dongen, J.; de Heus, E.; Eickholt, L.; Schrieks, M.; Zantingh, I.; Brouwer, O.R.; Oonk, M.H.M.; Grotenhuis, B.A.; Ezendam, N.P.M.; Duijts, S.F.A. Challenges and controversies patients and (health care) professionals experience in managing vaginal, vulvar, penile or anal cancer: The SILENCE study. Eur. J. Cancer Care 2022, 31, e13676. [Google Scholar] [CrossRef] [PubMed]
- Gonzato, O. Could information improve patient access to new emerging drugs in rare cancer trials? J. Cancer Policy 2016, 8, 38–41. [Google Scholar] [CrossRef]
- Heus, E.; Zwan, J.M.; Husson, O.; Frissen, A.; Herpen, C.M.L.; Merkx, M.A.W.; Duijts, S.F.A. Unmet supportive care needs of patients with rare cancer: A systematic review. Eur. J. Cancer Care 2021, 30, e13502. [Google Scholar] [CrossRef]
- Miller, R.C. Problems in rare tumor study: A call for papers. Rare Tumors 2010, 2, 46–47. [Google Scholar] [CrossRef]
- Prades, J.; Weinman, A.; Le Cam, Y.; Trama, A.; Frezza, A.M.; Borras, J.M. Priorities on rare cancers? Policy in national cancer control plans (NCCPs): A review conducted within the framework of EU-JARC joint-action. J. Cancer Policy 2020, 24, 100222. [Google Scholar] [CrossRef]
- Drabbe, C.; Grünhagen, D.J.; Van Houdt, W.J.; Braam, P.M.; Soomers, V.L.M.N.; Van der Hage, J.A.; De Haan, J.J.; Keymeulen, K.B.M.I.; Husson, O.; Van der Graaf, W.T.A. Diagnosed with a rare cancer: Experiences of adult sarcoma survivors with the healthcare system—Results from the SURVSARC study. Cancers 2021, 13, 679. [Google Scholar] [CrossRef]
- Pierotti, M.A.; Negri, T.; Tamborini, E.; Perrone, F.; Pricl, S.; Pilotti, S. Targeted therapies: The rare cancer paradigm. Mol. Oncol. 2009, 4, 19–37. [Google Scholar] [CrossRef]
- Pillai, R.; Jayasree, K. Rare cancers: Challenges and issues. Indian J. Med. Res. 2017, 145, 17. [Google Scholar] [CrossRef] [PubMed]
- Ray-Coquard, I.; Lauraine, E.P.; Cesne, A.L.; Pautier, P.; Lavenue, M.C.V.; Trama, A.; Casali, P.; Coindre, J.M.; Blay, J.Y. Improving treatment results with reference centres for rare cancers: Where do we stand? Eur. J. Cancer 2017, 77, 90–98. [Google Scholar] [CrossRef] [PubMed]
- De Heus, E.; Engelen, V.; Dingemans, I.; Richel, C.; Schrieks, M.; van der Zwan, J.M.; Besselink, M.G.; van Berge Henegouwen, M.I.; van Herpen, C.M.L.; Duijts, S.F.A. Differences in health care experiences between rare cancer and common cancer patients: Results from a national cross-sectional survey. Orphanet J. Rare Dis. 2021, 16, 249. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues, R.; Trigg, L.; Schmidt, A.E.; Leichsenring, K. The public gets what the public wants: Experiences of public reporting in long-term care in europe. Health Policy 2014, 116, 84–94. [Google Scholar] [CrossRef]
- EU Health Union: Europe’s Beating Cancer Plan 2021. Available online: https://ec.europa.eu/commission/presscorner/detail/en/fs_20_341 (accessed on 3 January 2024).
- Blay, J.-Y.; Casali, P.; Bouvier, C.; Dehais, C.; Galloway, I.; Gietema, J.; Halámková, J.; Hindi, N.; Idbaih, A.; Kinloch, E.; et al. European reference network for rare adult solid cancers, statement, and integration to health care systems of member states: A position paper of the ERN EURACAN. ESMO Open 2021, 6, 100174. [Google Scholar] [CrossRef] [PubMed]
- Frezza, A.M.; Trama, A.; Blay, J.-Y.; Casali, P.G. Networking in rare cancers: What was done, what is next? Eur. J. Surg. Oncol. 2019, 45, 16–18. [Google Scholar] [CrossRef]
- Prades, J.; Trama, A.; Casali, P.G.; Emile, J.-F.; Gaspar, N.; Janavicius, R.; Jančiauskienė, R.; Karjalainen, S.; Kopeckova, K.; Pylkkänen, L.; et al. Is rare cancer care organized at national health system level? Multiple case study in six EU countries. Eur. J. Public Health 2022, 32, 852–857. [Google Scholar] [CrossRef]
- Regulation (EC) No 141/2000 of the European Parliament and of the Council of 16 December 1999 on Orphan Medicinal Products. Off. J. Eur. Communities 2000, 18, 15. Available online: https://eur-lex.europa.eu/legal-content/EN/TXT/PDF/?uri=CELEX:32000R0141 (accessed on 3 January 2024).
- Commission delegated decision of 10 March 2014 setting out criteria and conditions that European Reference Networks and healthcare providers wishing to join a European Reference Network must fulfil. Off. J. Eur. Union 2014, 17, 71–78. Available online: https://eur-lex.europa.eu/legal-content/EN/TXT/PDF/?uri=CELEX:32014D0286 (accessed on 3 January 2024).
- Blay, J.-Y.; Fenaux, P.; Ladenstein, R.; Hoogerbrugge, N. Continue rare cancers collaboration with european reference networks after brexit. Lancet 2021, 397, 793. [Google Scholar] [CrossRef]
- Tan, S.-B.; Dear, K.B.G.; Bruzzi, P.; Machin, D. Strategy for randomised clinical trials in rare cancers. BMJ Br. Med. J. 2003, 327, 47–49. [Google Scholar] [CrossRef] [PubMed]
- Baker, L.H.; Crowley, J.J.; Maki, R.G. Randomization and statistical power: Paramount in trial reproducibility (even for rare cancers). Oncologist 2012, 17, 1129–1132. [Google Scholar] [CrossRef] [PubMed]
- Gronchi, A.; Haas, R.L.; Bonvalot, S. Cancer registries and randomised clinical trials in rare tumours: At the two extremes of daily clinical practice. Eur. J. Cancer 2016, 64, 113–115. [Google Scholar] [CrossRef] [PubMed]
- Schuller, Y.; Biegstraaten, M.; Hollak, C.E.M.; Klümpen, H.-J.; Gispen-de Wied, C.C.; Stoyanova-Beninska, V. Oncologic orphan drugs approved in the EU—Do clinical trial data correspond with real-world effectiveness? Orphanet J. Rare Dis. 2018, 13, 214. [Google Scholar] [CrossRef]
- Korchagina, D.; Jaroslawski, S.; Jadot, G.; Toumi, M. Orphan drugs in oncology. In Regulatory and Economic Aspects in Oncology; Recent Results in Cancer Research; Springer: Cham, Switzerland, 2018; pp. 109–142. [Google Scholar] [CrossRef]
- Schey, C.; Milanova, T.; Hutchings, A. Estimating the budget impact of orphan medicines in europe: 2010–2020. Orphanet J. Rare Dis. 2011, 6, 62. [Google Scholar] [CrossRef] [PubMed]
- Kirk, R. Genetics: New classification for endometrial cancer puts genes in POLE position. Nat. Rev. Clin. Oncol. 2013, 10, 304. [Google Scholar] [CrossRef] [PubMed]
- Eliyatkın, N.; Yalçın, E.; Zengel, B.; Aktaş, S.; Vardar, E. Molecular classification of breast carcinoma: From traditional, old-fashioned way to a new age, and a new way. J. Breast Health 2015, 11, 59–66. [Google Scholar] [CrossRef]
- Loughnot, D. Potential interactions of the orphan drug act and pharmacogenomics: A flood of orphan drugs and abuses? Am. J. Law Med. 2005, 31, 365–380. [Google Scholar] [CrossRef]
- Côté, A.; Keating, B. What is wrong with orphan drug policies? Value Health 2012, 15, 1185–1191. [Google Scholar] [CrossRef]
- Simoens, S. Pricing and reimbursement of orphan drugs: The need for more transparency. Orphanet J. Rare Dis. 2011, 6, 42. [Google Scholar] [CrossRef]
- Vokinger, K.N.; Daniore, P.; Kesselheim, A.S. 1586MO pivotal trial endpoints of drugs for rare and non-rare cancers in the US and europe. Ann. Oncol. 2020, 31, S1197. [Google Scholar] [CrossRef]
- Nagase, F.N.I.; Stafinski, T.; Sun, J.; Jhangri, G.; Menon, D. Factors associated with positive and negative recommendations for cancer and non-cancer drugs for rare diseases in canada. Orphanet J. Rare Dis. 2019, 14, 127. [Google Scholar] [CrossRef] [PubMed]
- Pauwels, K.; Huys, I.; Casteels, M.; Larsson, K.; Voltz, C.; Penttila, K.; Morel, T.; Simoens, S. Are products with an orphan designation for oncology indications different from products for other rare indications? A retrospective analysis of european orphan designations granted between 2002–2012. Orphanet J. Rare Dis. 2017, 12, 36. [Google Scholar] [CrossRef] [PubMed]
- Fermaglich, L.J.; Miller, K.L. A comprehensive study of the rare diseases and conditions targeted by orphan drug designations and approvals over the forty years of the orphan drug act. Orphanet J. Rare Dis. 2023, 18, 163. [Google Scholar] [CrossRef] [PubMed]
- Martin, N.; Doulet, N.; Hivert, V.; Aymé, S. Rare diseases research in europe: An overview based on data from the orphanet database. Orphanet J. Rare Dis. 2010, 5, P5. [Google Scholar] [CrossRef]
- Barrenho, E.; Halmai, R.; Miraldo, M.; Tzintzun, I.; Raïs Ali, S.; Toulemon, L.; Dupont, J.-C.K.; Rochaix, L. Inequities in cancer drug development in terms of unmet medical need. Soc. Sci. Med. 2022, 302, 114953. [Google Scholar] [CrossRef] [PubMed]
- Korchagina, D.; Millier, A.; Vataire, A.-L.; Aballea, S.; Falissard, B.; Toumi, M. Determinants of orphan drugs prices in France: A regression analysis. Orphanet J. Rare Dis. 2017, 12, 75. [Google Scholar] [CrossRef] [PubMed]
- Bouslouk, M. G-BA benefit assessment of new orphan drugs in Germany: The first five years. Expert Opin. Orphan Drugs 2016, 4, 453–455. [Google Scholar] [CrossRef]
- Adkins, E.; Nicholson, L.; Floyd, D.; Ratcliffe, M.; Chevrou-Severac, H. Oncology drugs for orphan indications: How are HTA processes evolving for this specific drug category? Clin. Outcomes Res. 2017, 9, 327–342. [Google Scholar] [CrossRef]
- Nicod, E.; Kanavos, P. Commonalities and differences in HTA outcomes: A comparative analysis of five countries and implications for coverage decisions. Health Policy 2012, 108, 167–177. [Google Scholar] [CrossRef]
- Medicinal Products in Human Medicine Act. State Gazette 2007. Available online: https://www.bda.bg/images/stories/documents/legal_acts/20210208_ZLPHM_English.pdf (accessed on 3 January 2024).
- Ministry of Health. Ordinance on the Terms, Rules and Procedure for Regulation and Registration of Prices for Medicinal Products 2013. Available online: https://www.ncpr.bg/images/REGULATIONS/2017/20.02.2017/Naredba_tseni_NCPR_24.01.2017-eng.pdf (accessed on 3 January 2024).
- Regulation (EU) 2021/2282 of the European Parliament and of the Council of 15 December 2021 on health technology assessment and amending Directive 2011/24/EU. Off. J. Eur. Union 2021, 458, 1–32. Available online: https://eur-lex.europa.eu/legal-content/EN/TXT/?uri=CELEX:32021R2282 (accessed on 3 January 2024).
- Health Insurance Act. State Gazette, No. 16/23.02.2024. 1998. Available online: https://www.minfin.bg/upload/36670/Health_Insurance_Act.pdf (accessed on 3 January 2024).
- Council of Ministers. Decision No. 3/04.01.2023 on the Adoption of the National Cancer Control Plan in the Republic of Bulgaria 2027. State Gazette; 2022. Available online: https://www.mh.government.bg/media/filer_public/2022/07/08/bg_national_cancer_plan_2030_-_site.pdf (accessed on 3 January 2024).
- Wepner, B.; Giesecke, S. Drivers, trends and scenarios for the future of health in Europe. Impressions from the FRESHER project. Eur. J. Futures Res. 2018, 6, 2. [Google Scholar] [CrossRef]
- Iskrov, G.; Miteva-Katrandzhieva, T.; Stefanov, R. Challenges to orphan drugs access in eastern europe: The case of Bulgaria. Health Policy 2012, 108, 10–18. [Google Scholar] [CrossRef]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2021; Available online: https://www.r-project.org/ (accessed on 3 January 2024).
- Wickham, H.; Averick, M.; Bryan, J.; Chang, W.; McGowan, L.D.; François, R.; Grolemund, G.; Hayes, A.; Henry, L.; Hester, J.; et al. Welcome to the tidyverse. J. Open Source Softw. 2019, 4, 1686. [Google Scholar] [CrossRef]
- Wickham, H. ggplot2: Elegant Graphics for Data Analysis; Springer: New York, NY, USA, 2016; ISBN 978-3-319-24277-4. [Google Scholar]
- Hartmann, M.; Mayer-Nicolai, C.; Pfaff, O. Approval probabilities and regulatory review patterns for anticancer drugs in the european union. Crit. Rev. Oncol./Hematol. 2013, 87, 112–121. [Google Scholar] [CrossRef] [PubMed]
- Salcher-Konrad, M.; Naci, H.; Davis, C. Approval of cancer drugs with uncertain therapeutic value: A comparison of regulatory decisions in europe and the United States. Milbank Q. 2020, 98, 1219–1256. [Google Scholar] [CrossRef] [PubMed]
- Sandman, L.; Liliemark, J. From evidence-based to hope-based medicine? Ethical aspects on conditional market authorization of and early access to new cancer drugs. Semin. Cancer Biol. 2017, 45, 58–63. [Google Scholar] [CrossRef]
- Grössmann, N.; Robausch, M.; Rosian, K.; Wild, C.; Simon, J. Monitoring evidence on overall survival benefits of anticancer drugs approved by the european medicines agency between 2009 and 2015. Eur. J. Cancer 2019, 110, 1–7. [Google Scholar] [CrossRef]
- Wilking, N.; Bucsics, A.; Kandolf Sekulovic, L.; Kobelt, G.; Laslop, A.; Makaroff, L.; Roediger, A.; Zielinski, C. Achieving equal and timely access to innovative anticancer drugs in the european union (EU): Summary of a multidisciplinary CECOG-driven roundtable discussion with a focus on eastern and south-eastern EU countries. ESMO Open 2019, 4, e000550. [Google Scholar] [CrossRef]
- Raycheva, R.; Kostadinov, K. HTA69 delay of innovative oncology treatments—Case from Bulgaria. Value Health 2022, 25, S309–S310. [Google Scholar] [CrossRef]
- Raycheva, R.; Kostadinov, K. HTA7 the price of innovation—Oncology treatments expenditures: Case from Bulgaria. Value Health 2023, 26, S260. [Google Scholar] [CrossRef]
- Post, H.C.; Schutte, T.; van Oijen, M.G.H.; van Laarhoven, H.W.M.; Hollak, C.E.M. Time to reimbursement of novel anticancer drugs in europe: A case study of seven european countries. ESMO Open 2023, 8, 101208. [Google Scholar] [CrossRef] [PubMed]
- Schoot, R.A.; Otth, M.A.; Frederix, G.W.J.; Leufkens, H.G.M.; Vassal, G. Market access to new anticancer medicines for children and adolescents with cancer in europe. Eur. J. Cancer 2022, 165, 146–153. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.T.; Klempner, S.J.; Park, S.H.; Park, J.O.; Park, Y.S.; Lim, H.Y.; Kang, W.K.; Kim, K.-M.; Lee, J. Correlating programmed death ligand 1 (PD-L1) expression, mismatch repair deficiency, and outcomes across tumor types: Implications for immunotherapy. Oncotarget 2017, 8, 77415–77423. [Google Scholar] [CrossRef] [PubMed]
- Skorupan, N.; Ghabra, S.; Maldonado, J.A.; Zhang, Y.; Alewine, C. Two rare cancers of the exocrine pancreas: To treat or not to treat like ductal adenocarcinoma? J. Cancer Metastasis Treat. 2023, 9, 5. [Google Scholar] [CrossRef] [PubMed]
- Mincarone, P.; Leo, C.G.; Sabina, S.; Sarriá-Santamera, A.; Taruscio, D.; Serrano-Aguilar, P.G.; Kanavos, P. Reimbursed price of orphan drugs: Current strategies and potential improvements. Public Health Genom. 2017, 20, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Czech, M.; Baran-Kooiker, A.; Atikeler, K.; Demirtshyan, M.; Gaitova, K.; Holownia-Voloskova, M.; Turcu-Stiolica, A.; Kooiker, C.; Piniazhko, O.; Konstandyan, N.; et al. A review of rare disease policies and orphan drug reimbursement systems in 12 Eurasian countries. Front. Public Health 2020, 7, 416. [Google Scholar] [CrossRef] [PubMed]
- Rachev, B.; Uyei, J.; Singh, R.; Kowal, S.; Johnson, C.E. Stakeholder point of view on prescription drug affordability—A systematic literature review and content analysis. Health Policy 2021, 125, 1158–1165. [Google Scholar] [CrossRef]
- Graf von der Schulenburg, J.-M.; Pauer, F. Rare cancers—Rarity as a cost and value argument. J. Cancer Policy 2017, 11, 54–59. [Google Scholar] [CrossRef]
- Zlatareva, A.; Petrova, G. National health insurance fund cost analysis for rare cancer diseases and orphan drugs. Gen. Med. 2015, 17, 13–18. [Google Scholar]
- Barron, A.; Wilsdon, T. Challenging perceptions about oncology product pricing in breast and colorectal cancer. Pharm. Med. 2016, 30, 321–326. [Google Scholar] [CrossRef] [PubMed]
- Latimer, N.R.; Pollard, D.; Towse, A.; Henshall, C.; Sansom, L.; Ward, R.L.; Bruce, A.; Deakin, C. Challenges in valuing and paying for combination regimens in oncology: Reporting the perspectives of a multi-stakeholder, international workshop. BMC Health Serv. Res. 2021, 21, 412. [Google Scholar] [CrossRef] [PubMed]
- Jayasundara, K.; Krahn, M.; Mamdani, M.; Hoch, J.S.; Grootendorst, P. Differences in incremental cost-effectiveness ratios for common versus rare conditions: A case from oncology. PharmacoEconomics-Open 2017, 1, 167–173. [Google Scholar] [CrossRef] [PubMed]
- Vancoppenolle, J.M.; Franzen, N.; Koole, S.N.; Retèl, V.P.; van Harten, W.H. Differences in time to patient access to innovative cancer medicines in six european countries. Int. J. Cancer 2023, 154, 886–894. [Google Scholar] [CrossRef] [PubMed]
- Jain, R.; Menzin, J.; Lachance, K.; McBee, P.; Phatak, H.; Nghiem, P.T. Travel burden associated with rare cancers: The example of merkel cell carcinoma. Cancer Med. 2019, 8, 2580–2586. [Google Scholar] [CrossRef] [PubMed]
- Onega, T.; Alford-Teaster, J.; Leggett, C.; Loehrer, A.; Weiss, J.E.; Moen, E.L.; Pollack, C.C.; Wang, F. The interaction of rurality and rare cancers for travel time to cancer care. J. Rural Health 2022, 39, 426–433. [Google Scholar] [CrossRef]
- Mixich, V.; Voinea, S.A.; Mardale, S. PDG61 Cancer drugs shortages in Romania: Magnitude, causes and solutions. Value Health 2019, 22, S607. [Google Scholar] [CrossRef]
- Cherny, N.; Sullivan, R.; Torode, J.; Saar, M.; Eniu, A. ESMO european consortium study on the availability, out-of-pocket costs and accessibility of antineoplastic medicines in europe. Ann. Oncol. 2016, 27, 1423–1443. [Google Scholar] [CrossRef] [PubMed]
- Gavel, S.J. The oncology pipeline: Maturing, competitive, and growing. Oncol. Bus. Rev. 2008, 14–16. [Google Scholar]
- Karanyotova, S.; Topova, B.; Petrova, E.; Doychev, P.; Kapitanska, E.; Petrova, G.; Mitkova, Z.; Dimitrova, M. Treatment patterns, adherence to international guidelines, and financial mechanisms of the market access of advanced breast cancer therapy in Bulgaria. Front. Public Health 2023, 11, 1073733. [Google Scholar] [CrossRef]
- Mitkova, Z.; Doneva, M.; Gerasimov, N.; Tachkov, K.; Dimitrova, M.; Kamusheva, M.; Petrova, G. Analysis of Healthcare Expenditures in Bulgaria. Healthcare 2022, 10, 274. [Google Scholar] [CrossRef] [PubMed]
- Lebanova, H.; Stoev, S.; Naseva, E.; Getova, V.; Wang, W.; Sabale, U.; Petrova, E. Economic burden of cervical cancer in bulgaria. Int. J. Environ. Res. Public Health 2023, 20, 2746. [Google Scholar] [CrossRef] [PubMed]
- Vekic, B.; Dragojevic-Simic, V.; Jakovljevic, M.; Pilipovic, F.; Simic, R.; Zivic, R.; Radovanovic, D.; Rancic, N. Medical cost of colorectal cancer services in serbia between 2014 and 2017: National data report. Front. Pharmacol. 2019, 10, 526. [Google Scholar] [CrossRef] [PubMed]
- Tomić, Z.; Tomas, A.; Benšova, Z.; Tomić, L.; Horvat, O.; Varga, I.; Paut Kusturica, M.; Sabo, A. Challenges of providing access to cutting-edge cancer medicines in the countries of Eastern Europe. Front. Public Health 2018, 6, 193. [Google Scholar] [CrossRef] [PubMed]
- Pejcic, A.V.; Iskrov, G.; Jakovljevic, M.M.; Stefanov, R. Access to orphan drugs—Comparison across Balkan countries. Health Policy 2018, 122, 583–589. [Google Scholar] [CrossRef]
- Kandolf Sekulovic, L.; Guo, J.; Agarwala, S.; Hauschild, A.; McArthur, G.; Cinat, G.; Wainstein, A.; Caglevic, C.; Lorigan, P.; Gogas, H.; et al. Access to innovative medicines for metastatic melanoma worldwide: Melanoma World Society and European Association of Dermato-oncology survey in 34 countries. Eur. J. Cancer 2018, 104, 201–209. [Google Scholar] [CrossRef]
- Martinalbo, J.; Bowen, D.; Camarero, J.; Chapelin, M.; Démolis, P.; Foggi, P.; Jonsson, B.; Llinares, J.; Moreau, A.; O’Connor, D.; et al. Early market access of cancer drugs in the EU. Ann. Oncol. 2016, 27, 96–105. [Google Scholar] [CrossRef]
- Horgan, D.; Koeva-Balabanova, J.; Capoluongo, E.; Jagielska, B.; Cattaneo, I.; Kozaric, M.; Tumiene, B.; El Ahl, J.-P.; Lal, J.A.; Kalra, D.; et al. Making sure that orphan incentives tip the right way in Europe. Healthcare 2022, 10, 1600. [Google Scholar] [CrossRef] [PubMed]
- Dimitrova, M.; Jakab, I.; Mitkova, Z.; Kamusheva, M.; Tachkov, K.; Nemeth, B.; Zemplenyi, A.; Dawoud, D.; Delnoij, D.M.J.; Houýez, F.; et al. Potential barriers of patient involvement in health technology assessment in central and eastern european countries. Front. Public Health 2022, 10, 922708. [Google Scholar] [CrossRef]
- Jakab, I.; Dimitrova, M.; Houÿez, F.; Bereczky, T.; Fövényes, M.; Maravic, Z.; Belina, I.; Andriciuc, C.; Tóth, K.; Piniazhko, O.; et al. Recommendations for patient involvement in health technology assessment in central and Eastern European countries. Front. Public Health 2023, 11, 1176200. [Google Scholar] [CrossRef]
- Husereau, D.; Bombard, Y.; Stockley, T.; Carter, M.; Davey, S.; Lemaire, D.; Nohr, E.; Park, P.; Spatz, A.; Williams, C.; et al. Future role of health technology assessment for genomic medicine in oncology: A Canadian laboratory perspective. Curr. Oncol. 2023, 30, 9660–9669. [Google Scholar] [CrossRef] [PubMed]
- Normanno, N.; Apostolidis, K.; Wolf, A.; Al Dieri, R.; Deans, Z.; Fairley, J.; Maas, J.; Martinez, A.; Moch, H.; Nielsen, S.; et al. Access and quality of biomarker testing for precision oncology in europe. Eur. J. Cancer 2022, 176, 70–77. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Data Source | Description | Extracted Variables | Link 1 |
|---|---|---|---|
| EMA | List of all authorized medicinal products | Product name, ATC code, therapeutic indication, orphan designation status, date of market authorization | https://www.ema.europa.eu/en/medicines/download-medicine-data |
| NCPRMP | Positive Drug List (PDL) database | Reimbursement status, date of inclusion in the PDL | https://data.egov.bg/resource/download/ba1ab4be-8695-4377-9edf-464233e2fc39/csv |
| NHIF | Annual budget reports | Total expenses related to all medicinal treatments | https://www.nhif.bg/bg |
| NHIF | Monthly expenditures for all medicinal treatments | Product (market) name, number of treated patients, ATC, INN, region, hospital, ICD code | https://www.nhif.bg/bg/nzok/medicine/5 |
| EMA | List of all authorized medicinal products | Product name, ATC code, therapeutic indication, orphan designation status, date of market authorization | https://www.ema.europa.eu/en/medicines/download-medicine-data |
| NCPRMP | Positive Drug List (PDL) database | Reimbursement status, date of inclusion in the PDL | https://data.egov.bg/resource/download/ba1ab4be-8695-4377-9edf-464233e2fc39/csv |
| Trade Name | INN | Indication |
|---|---|---|
| Adcetris | Brentuximab Vedotin | Hodgkin’s lymphoma |
| Blincyto | Blinatumomab | Precursor Cell Lymphoblastic Leukemia Lymphoma |
| Darzalex | Daratumumab | Multiple Myeloma |
| Gazyvaro | Obinutuzumab | Leukemia, Lymphocytic, Chronic, B-Cell |
| Kyprolis | Carfilzomib | Multiple Myeloma |
| Nexavar | Sorafenib | Carcinoma, Hepatocellular and Carcinoma, Renal Cell |
| Ninlaro | Ixazomib | Multiple Myeloma |
| Rydapt | Midostaurin | Leukemia, Myeloid, Acute and Mastocytosis |
| Besponsa | Inotuzumab ozogamicin | Precursor Cell Lymphoblastic Leukemia Lymphoma |
| Imnovid | Pomalidomide | Multiple Myeloma |
| Mylotarg | Gemtuzumab ozogamicin | Leukemia, Myeloid, Acute |
| Onivyde Pegylated Liposomal | Irinotecan | Pancreatic Neoplasms |
| Polivy | Polatuzumab vedotin | Lymphoma, B-Cell |
| Xospata | Gilteritinib | Leukemia, Myeloid, Acute |
| Vyxeos Liposomal | Daunorubicin/Cytarabine | Leukemia, Myeloid, Acute |
| Indicator/Year | 2020 | 2021 | 2022 | 2023 |
|---|---|---|---|---|
| Months | July–December (6) | January–December (12) | January–December (12) | January–September (9) |
| Total expenditures | 7,573,302 | 18,564,033 | 22,680,446 | 25,535,712 |
| % of all cancer drugs expenditures | 4.75% | 5.17% | 5.47% | 6.71% |
| % of NHIF medicinal expenditures | 0.24% | 2.73% | 2.93% | 3.77% |
| Median monthly treated patients | 270 | 287 | 334 | 432 |
| Increase in median monthly treated patients Δ% | - | 6% | 16% | 29% |
| Median monthly cancer OD expenditures (in EUR) | 1,267,187 | 1,487,890 | 1,910,242 | 2,884,393 |
| Increase in median monthly cancer OD expenditures Δ% | base | 17% | 28% | 51% |
| Median monthly expenditure per patient (in EUR) | 4701.99 | 5184.29 | 5719.29 | 6676.84 |
| Year | ||||
|---|---|---|---|---|
| Region | 2020 | 2021 | 2022 | 2023 |
| Blagoevgrad | 3 (9607) | 1 (1354) | 1 (3043) | 1 (2302) |
| Burgas | 14 (46,398) | 14 (24,281) | 4 (11,419) | 3 (6812) |
| Dobrich | 1 (3200) | 1 (3190) | 2 (1817) | 1 (3698) |
| Gabrovo | 1 (1716) | 1 (871) | — | — |
| Haskovo | 1 (3202) | 2 (3200) | 2 (3033) | 1 (2980) |
| Pazardzhik | 6 (18,538) | 6 (9670) | 2 (5093) | 2 (3125) |
| Pleven | 23 (107,143) | 18 (93,392) | 25 (150,814) | 53 (309,897) |
| Plovdiv | 38 (169,954) | 40 (194,117) | 42 (230,639) | 62 (432,887) |
| Ruse | 4 (12,809) | 3 (5418) | 1 (2767) | 1 (2767) |
| Shumen | 4 (9608) | 4 (5418) | 1 (3043) | 2 (6452) |
| Sofia | 128 (693,117) | 158 (917,017) | 202 (1,166,230) | 231 (1,568,788) |
| Stara Zagora | 4 (14,338) | 4 (7365) | 1 (1851) | 2 (5011) |
| Varna | 38 (158,481) | 38 (188,040) | 60 (298,279) | 81 (523,459) |
| Veliko Tarnovo | 1 (3143) | 1 (1354) | — | 1 (1611) |
| Vratsa | 5 (9435) | 2 (4720) | 1 (97) | 3 (6004) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kostadinov, K.; Popova-Sotirova, I.; Marinova, Y.; Musurlieva, N.; Iskrov, G.; Stefanov, R. Availability and Access to Orphan Drugs for Rare Cancers in Bulgaria: Analysis of Delays and Public Expenditures. Cancers 2024, 16, 1489. https://doi.org/10.3390/cancers16081489
Kostadinov K, Popova-Sotirova I, Marinova Y, Musurlieva N, Iskrov G, Stefanov R. Availability and Access to Orphan Drugs for Rare Cancers in Bulgaria: Analysis of Delays and Public Expenditures. Cancers. 2024; 16(8):1489. https://doi.org/10.3390/cancers16081489
Chicago/Turabian StyleKostadinov, Kostadin, Ivelina Popova-Sotirova, Yuliyana Marinova, Nina Musurlieva, Georgi Iskrov, and Rumen Stefanov. 2024. "Availability and Access to Orphan Drugs for Rare Cancers in Bulgaria: Analysis of Delays and Public Expenditures" Cancers 16, no. 8: 1489. https://doi.org/10.3390/cancers16081489
APA StyleKostadinov, K., Popova-Sotirova, I., Marinova, Y., Musurlieva, N., Iskrov, G., & Stefanov, R. (2024). Availability and Access to Orphan Drugs for Rare Cancers in Bulgaria: Analysis of Delays and Public Expenditures. Cancers, 16(8), 1489. https://doi.org/10.3390/cancers16081489