
Caregiving and Its Resulting Effects—The Care Study to Evaluate the Effects of Caregiving on Caregivers of Patients with Advanced Cancer in Singapore

Abstract
:1. Introduction
2. Materials and Methods
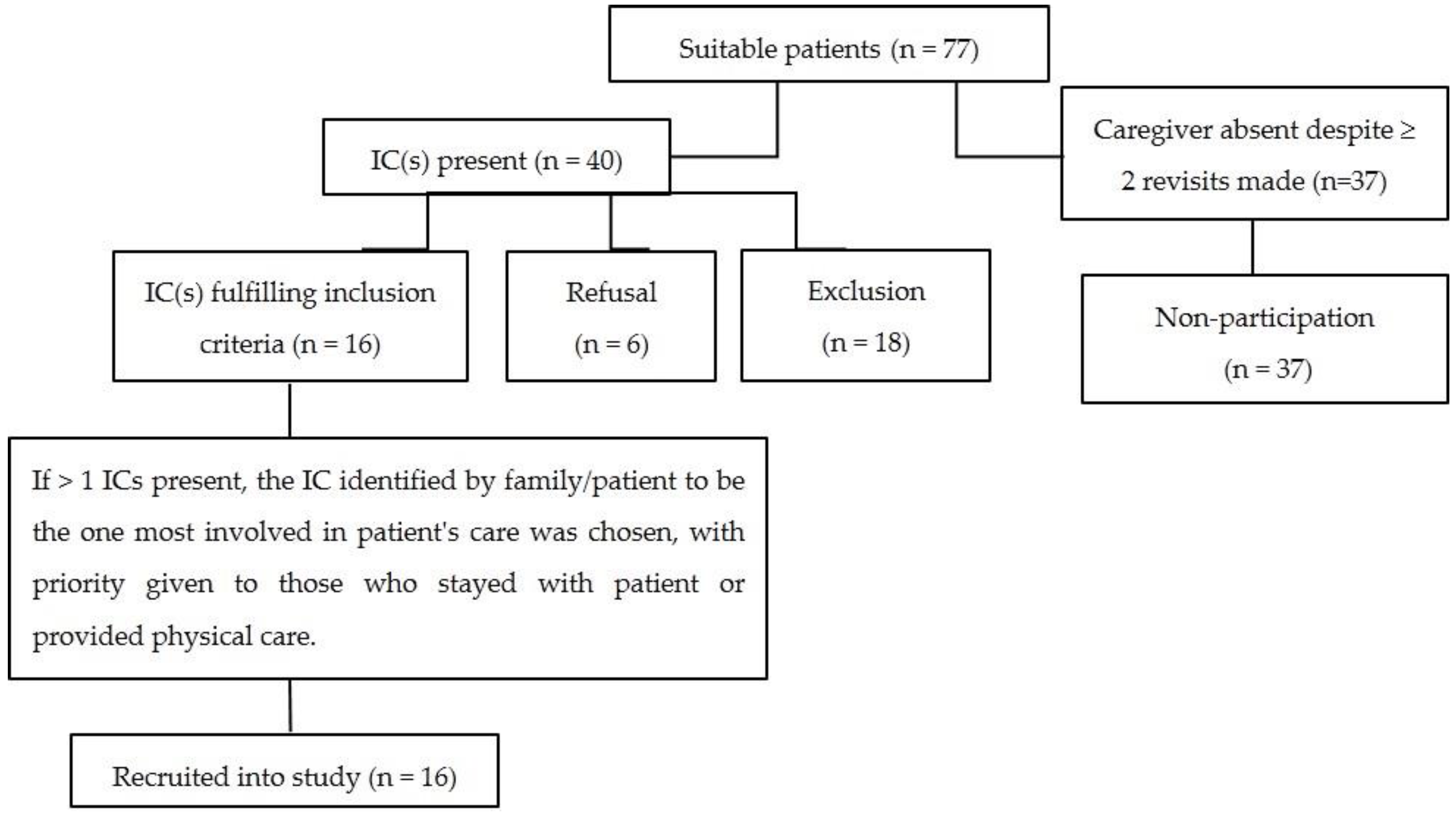
2.1. Eligibility Criteria
- ICs of advanced cancer patients admitted to Singapore General Hospital (SGH) within 3 weeks of the interview date and receiving care from the National Cancer Centre Singapore (NCCS) palliative care service.
- Significant involvement in at least one of four care roles: physical care, financial support, emotional support and decision making, with significant involvement defined as undertaking at least 50% of the care role as determined by the IC.
- Singaporeans or Singapore permanent residents.
- Aged 21 years old and above.
- Able to communicate in English.
- Intact cognition.
2.2. Surveys Administered
- Palliative care Outcomes Scale (POS)—Carer questionnaire. The POS is a 10-item scale with scores varying proportionately to the level of patients’ physical symptoms, psychological, emotional, spiritual, information and support needs. The outcome measure is developed for patients with advanced cancer and has been validated in various palliative care settings (both inpatient and outpatient). Its construct has been validated against other appropriate palliative care measures such as the European Organisation for Research on Cancer Treatment and the Support Team Assessment Schedule [14].
- Zarit Burden Interview (ZBI)—short-form 12-item version. In this 12-item short version of the original 22-item ZBI, higher scores represent higher burden. The ZBI is a widely used tool to describe caregiver burden and has been well validated in various caregiving samples. The scores from the 12-item version have previously been assessed to have good correlation with the original version in caregivers of advanced cancer patients. A score of 17 or more has been recommended as an indicator for high caregiver burden [15,16].
- Caregiver Quality of Life Index—Cancer (CQOLC). Higher scores correspond to better QOL in this 35-item questionnaire. Psychometric properties have previously been reported with test-retest reliability of 0.95, good internal consistency and demonstration of face, content, concurrent, convergent as well as discriminant validity among family caregivers of cancer patients [16,17,18].
- Center for Epidemiologic Studies Depression Scale—Revised (CESD-R). A score of 16 or above has been considered clinically significant in this 20-item depression scale reflecting the Fourth Edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-IV) criteria for depression [19].
- Work Productivity and Activity Impairment Questionnaire (WPAI). The proportion of work and activity impairment is assessed through 6 questions pertaining to work and non-work activities. The WPAI has previously reported to have high convergent validity with the Caregiver Strain Index and the Centre for Epidemiologic Studies Depression Scale in ICs [20].
3. Results
3.1. Participants
3.2. Burden of Caregiving
4. Discussion
Strengths and Limitations
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
Abbreviations
| IC | Informal caregiverQOL: Quality of life |
| SGH | Singapore General Hospital |
| NCCS | National Cancer Centre Singapore |
| POS | Palliative care Outcome Scale |
| ZBI | Zarit Burden Interview |
| CQOLC | Caregiver Quality of Life Index—Cancer |
| CESD-R | Center for Epidemiologic Studies Depression Scale—Revised |
| DSM-IV | Fourth Edition of the Diagnostic and Statistical Manual of Mental Disorders |
| WPAI | Work Productivity and Activity Impairment Questionnaire |
| SD | Standard deviation |
| KPS | Karnofsky Performance Status |
| EOL | End-of-life |
| DNR | Do-not-resuscitate |
| ACP | Advanced care planning |
References
- Chan, S.W. Family caregiving in dementia: The Asian perspective of a global problem. Dement. Geriatr. Cogn. Disord. 2010, 30, 469–478. [Google Scholar] [CrossRef] [PubMed]
- Hebert, R.S.; Schulz, R. Caregiving at the end of life. J. Palliat. Med. 2006, 9, 1174–1187. [Google Scholar] [CrossRef] [PubMed]
- Turkoglu, N.; Kilic, D. Effects of care burdens of caregivers of cancer patients on their quality of life. Asian Pac. J. Cancer Prev. 2012, 13, 4141–4145. [Google Scholar] [CrossRef] [PubMed]
- Goren, A.; Gilloteau, I.; Lees, M.; DaCosta Dibonaventura, M. Quantifying the burden of informal caregiving for patients with cancer in Europe. Support Care Cancer 2014, 22, 1637–1646. [Google Scholar] [CrossRef] [PubMed]
- Lee, K.C.; Chang, W.C.; Chou, W.C.; Su, P.J.; Hsieh, C.H.; Chen, J.S.; Tang, S.T. Longitudinal changes and predictors of caregiving burden while providing end-of-life care for terminally ill cancer patients. J. Palliat. Med. 2013, 16, 632–637. [Google Scholar] [CrossRef] [PubMed]
- Ng, H.Y.; Griva, K.; Lim, H.A.; Tan, J.Y.; Mahendran, R. The burden of filial piety: A qualitative study on caregiving motivations amongst family caregivers of patients with cancer in Singapore. Psychol. Health 2016, 31, 1293–1310. [Google Scholar] [CrossRef] [PubMed]
- Tang, S.T.; Li, C.Y.; Liao, Y.C. Factors associated with depressive distress among Taiwanese family caregivers of cancer patients at the end of life. Palliat. Med. 2007, 21, 249–257. [Google Scholar] [CrossRef] [PubMed]
- Leow, M.Q.; Chan, M.F.; Chan, S.W. Predictors of change in quality of life of family caregivers of patients near the end of life with advanced cancer. Cancer Nurs. 2014, 37, 391–400. [Google Scholar] [CrossRef] [PubMed]
- Searight, H.R.; Gafford, J. Cultural diversity at the end of life: Issues and guidelines for family physicians. Am. Fam. Physician 2005, 71, 515–522. [Google Scholar] [PubMed]
- Households and Housing. Available online: http://www.singstat.gov.sg/statistics/latest-data#22 (accessed on 20 September 2016).
- Out-of-Pocket Health Expenditure (% of Private Expenditure on Health). Available online: http://data.worldbank.org/indicator/SH.XPD.OOPC.ZS (accessed on 10 September 2016).
- WHO Guide to Identifying the Economic Consequences of Disease and Injury. Available online: http://www.who.int/choice/publications/d_economic_impact_guide.pdf (accessed on 10 September 2016).
- Ng, G.T. Study Report of Singapore Family Caregiving Survey. Available online: http://www.fas.nus.edu.sg/rg/doc/family/family_wp.pdf (accessed on 10 September 2016).
- Hearn, J.; Higginson, I.J. Development and validation of a core outcome measure for palliative care: The palliative care outcome scale. Palliative Care Core Audit Project Advisory Group. Qual. Health Care 1999, 8, 219–227. [Google Scholar] [CrossRef] [PubMed]
- Higginson, I.J.; Gao, W.; Jackson, D.; Murray, J.; Harding, R. Short-form Zarit Caregiver Burden Interviews were valid in advanced conditions. J. Clin. Epidemiol. 2010, 63, 535–542. [Google Scholar] [CrossRef] [PubMed]
- Whalen, K.J.; Buchholz, S.W. The reliability, validity and feasibility of tools used to screen for caregiver burden: A systematic review. J. Adv. Nurs. 2010. [Google Scholar] [CrossRef]
- Weitzner, M.A.; Jacobsen, P.B.; Wagner, H.J.; Friedland, J.; Cox, C. The Caregiver Quality of Life Index-Cancer (CQOLC) scale: Development and validation of an instrument to measure quality of life of the family caregiver of patients with cancer. Qual. Life Res. 1999, 8, 55–63. [Google Scholar] [CrossRef] [PubMed]
- Weitzner, M.A.; McMillan, S.C. The Caregiver Quality of Life Index-Cancer (CQOLC) Scale: Revalidation in a home hospice setting. J. Palliat. Med. 1999, 15, 13–20. [Google Scholar]
- Van Dam, N.T.; Earleywine, M. Validation of the Center for Epidemiologic Studies Depression Scale—Revised (CESD-R): Pragmatic depression assessment in the general population. Psychiatry Res. 2011, 186, 128–132. [Google Scholar] [CrossRef] [PubMed]
- Giovannetti, E.R.; Wolff, J.L.; Frick, K.D.; Boult, C. Construct validity of the Work Productivity and Activity Impairment questionnaire across informal caregivers of chronically ill older patients. Value Health 2009, 12, 1011–1017. [Google Scholar] [CrossRef] [PubMed]
- Glajchen, M. The emerging role and needs of family caregivers in cancer care. J. Support Oncol. 2004, 2, 145–155. [Google Scholar] [PubMed]
- Lim, H.A.; Tan, J.Y.S.; Chua, J.; Yoong, R.K.L.; Lim, S.E.; Kua, E.H.; Mahendran, R. Quality of life of family caregivers of cancer patients in Singapore and globally. Singapore Med. J. 2016. [Google Scholar] [CrossRef] [PubMed]
- Chong, S.A.; Abdin, E.; Vaingankar, J.A.; Heng, D.; Sherbourne, C.; Yap, M.; Lim, Y.W.; Wong, H.B.; Ghosh-Dastidar, B.; Kwok, K.W.; et al. A population-based survey of mental disorders in Singapore. Ann. Acad. Med. Singapore 2012, 41, 49–66. [Google Scholar] [PubMed]
- Rhee, Y.S.; Yun, Y.H.; Park, S.; Shin, D.O.; Lee, K.M.; Yoo, H.J.; Kim, J.H.; Kim, S.O.; Lee, R.; Lee, Y.O.; et al. Depression in family caregivers of cancer patients: The feeling of burden as a predictor of depression. J. Clin. Oncol. 2008, 26, 5890–5895. [Google Scholar] [CrossRef] [PubMed]
- Lai, Y.M.; Hong, C.P.H.; Chee, C.Y.I. Stigma of Mental Illness. Singapore Med. J. 2000, 42, 111–114. [Google Scholar]
- National Mental Health Literacy Study. Available online: https://www.imh.com.sg/uploadedFiles/Newsroom/News_Releases/6Oct15_Mind%20Matters%20Media%20Release (accessed on 12 September 2016).
- Chang, H.Y.; Chiou, C.J.; Chen, N.S. Impact of mental health and caregiver burden on family caregivers’ physical health. Arch. Gerontol. Geriatr. 2010, 50, 267–271. [Google Scholar] [CrossRef] [PubMed]
- Mazanec, S.R.; Daly, B.J.; Douglas, S.L.; Lipson, A.R. Work productivity and health of informal caregivers of persons with advanced cancer. Res. Nurs. Health 2011, 34, 483–495. [Google Scholar] [CrossRef] [PubMed]
- Labour Force in Singapore, 2014. Available online: http://stats.mom.gov.sg/Pages/Labour-Force-In-Singapore-2014.aspx (accessed on 12 September 2016).
- McGuire, J.F.; Kenney, K.; Brashler, P. Flexible Work Arrangements: The Fact Sheet. Available online: http://scholarship.law.georgetown.edu/cgi/viewcontent.cgi?article=1012&context=legal (accessed on 12 September 2016).
- Xue, J.Y. More companies offering flexible work arrangements: MOM survey. Available online: http://www.todayonline.com/singapore/more-companies-offering-flexible-work-arrangements-mom-survey (accessed on 17 March 2016).
- Dumont, S.; Turgeon, J.; Allard, P.; Gagnon, P.; Charbonneau, C.; Vézina, L. Caring for a loved one with advanced cancer: Determinants of psychological distress in family caregivers. J. Palliat. Med. 2006, 9, 912–921. [Google Scholar] [CrossRef] [PubMed]
- Chan, A.; Ostbye, T.; Malhotra, R.; Hu, A.J. The Survey on Informal Caregiving; Ministry of Social and Family Development: Singapore, 2013; p. 35.
- Ng, R.; Chan, S.; Ng, T.; Chiam, A.; Lim, S. An exploratory study of the knowledge, attitudes and perceptions of advance care planning in family caregivers of patients with advanced illness in Singapore. BMJ Support. Palliat. Care 2013, 3, 343–348. [Google Scholar] [CrossRef] [PubMed]
- Romito, F.; Goldzweig, G.; Cormio, C.; Hagedoorn, M.; Anderson, B.L. Informal caregiving for cancer patients. Cancer 2013, 119, 2160–2169. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.; Given, B.A. Quality of life of family caregivers of cancer survivors: Across the trajectory of the illness. Cancer 2008, 112, 2556–2568. [Google Scholar] [CrossRef] [PubMed]
- Census of population 2010 Statistical Release 1: Demographic Characteristics, Education, Language and Religion. Available online: https://www.singstat.gov.sg/docs/default-source/default-document-library/publications/publications_and_papers/cop2010/census_2010_release1/cop2010sr1.pdf (accessed on 22 September 2016).


{kind=link}
| Socio-Demographics | Caregivers | Patients | |
|---|---|---|---|
| Mean age in years (S.D.) | 43.8 (14.80) | 63.0 (17.51) | |
| Gender | Male, n (%) | 7 (43.8%) | 8 (50%) |
| Female | 9 (56.3%) | 8 (50%) | |
| Ethnicity | Chinese | 11 (68.8%) | |
| Malay | 1 (6.3%) | ||
| Indian | 3 (18.8%) | ||
| Others | 1 (6.3%) | ||
| Marital status | Single | 6 (37.5%) | |
| Married | 10 (62.5%) | ||
| Number of children <16 years | 0 | 13 (81.3%) | |
| 1 | 1 (6.3%) | ||
| 2 | 2 (12.5%) | ||
| Employment status | Employed | 8 (50%) | |
| Professional, managerial | 5 (31.3%) | ||
| Clerical, service, sales | 2 (12.5%) | ||
| Manual skilled or unskilled | 1 (6.3%) | ||
| Unemployed | 8 (50%) | ||
| Caregiving Variables | n (%) | |
|---|---|---|
| Caregiver-patient relationship | Spouse | 4 (25.0) |
| Child | 7 (43.8) | |
| Sibling | 2 (12.5) | |
| Extended family | 3 (18.8) | |
| Duration of care | <6 months | 5 (31.3) |
| 6 months–1 year | 1 (6.3) | |
| 1–2 years | 2 (12.5) | |
| ≥2 years | 8 (50) | |
| Amount of involvement in daily care | No | 3 (18.8) |
| Yes | 13 (81.3) | |
| <4 h | 0 | |
| 4–8 h | 1 (7.7) | |
| 8–12 h | 2 (15.4) | |
| ≥12 h | 10 (76.9) | |
| Number of caregiving roles | 1 | 2 (12.5) |
| 2 | 5 (31.3) | |
| 3 | 4 (25.0) | |
| 4 | 5 (31.3) | |
| Physical caregiving | No | 2 (12.5) |
| Yes 1 | 8 (50.0) | |
| Partially 2 | 1 (6.3) | |
| N/A 3 | 5 (31.3) | |
| Hours spent on physical caregiving | <4 h | 1 (11.1) |
| 4–8 h | 3 (33.3) | |
| 8–12 h | 0 | |
| ≥12 h | 5 (55.6) | |
| Financial caregiving | No | 3 (18.8) |
| Yes 1 | 5 (31.3) | |
| Partially 2 | 5 (31.3) | |
| N/A 3 | 3 (18.8) | |
| Emotional caregiving | No | 1 (6.3) |
| Yes 1 | 12 (75.0) | |
| Partially 2 | 3 (18.8) | |
| Decision-making | No | 1 (6.3) |
| Yes 1 | 6 (37.5) | |
| Partially 2 | 4 (25.0) | |
| N/A 3 | 5 (31.3) | |
| Employment of foreign domestic worker | No | 11 (68.8) |
| Yes | 5 (31.3) | |
| <6 months | 1 (20.0) | |
| 6 months–1 year | 1 (20.0) | |
| 1–2 years | 1 (20.0) | |
| ≥2 years | 2 (40.0) | |
| Home care service | No | 13 (81.3) |
| Yes | 3 (18.8) | |
| Financial assistance | No | 12 (75.0) |
| Yes | 4 (25.0) | |
| Attended caregiver training | No | 15 (93.8) |
| Yes | 1 (6.3) | |
| Previous experience in caring for someone sick | No | 11 (68.8) |
| Yes | 5 (31.3) | |
| Variables | n (%) | |
|---|---|---|
| Cancer type | Breast | 3 (18.8) |
| Digestive or gastrointestinal (gastric, colorectal, liver) | 6 (37.5) | |
| Head and neck (thyroid) | 1 (6.3) | |
| Genitourinary (bladder, prostate, renal) | 3 (18.8) | |
| Gynecological (ovarian) | 1 (6.3) | |
| Hematological (blood, lymphoma) | 1 (6.3) | |
| Respiratory (lung) | 1 (6.3) | |
| Time since diagnosis | <6 months | 5 (31.3) |
| 6 months–1 year | 1 (6.3) | |
| 1–2 years | 2 (12.5) | |
| ≥2 years | 8 (50) | |
| Distant metastasis | Yes | 15 (93.8) |
| No | 1 (6.3) | |
| Time since admission | <1 week | 12 (75.0) |
| 1–2 weeks | 3 (18.8) | |
| 2–3 weeks | 1 (6.3) | |
| Caregiver rated KPS 1 | 80–100 | 3 (18.8) |
| 50–70 | 8 (50.0) | |
| 0–40 | 5 (31.3) | |
| POS—Carer 2 total score | ≤10 | 1 (6.3) |
| 10–20 | 7 (43.8) | |
| >20 | 8 (50.0) | |
| Caregiving Outcomes | Possible Range | Mean (SD) | |||
|---|---|---|---|---|---|
| All, n = 16 | ZBI < 17, n = 8 | ZBI ≥ 17, n = 8 | |||
| Caregiver burden | ZBI 1 total score | 0–48 | 17.81 (9.98) | ||
| ZBI 1 domains | Burden in relationship | 0–8 | 3.56 (1.93) | ||
| Emotional well-being | 0–20 | 7.19 (4.79) | |||
| Social and family life | 0–12 | 4.19 (2.64) | |||
| Loss of control over one’s life | 0–8 | 2.88 (2.25) | |||
| Personal strain | 0–24 | 10.63 (5.27) | |||
| Role strain | 0–20 | 6.5 (4.07) | |||
| Caregiver QOL | CQOLC 2 total score | 0–140 | 81.19 (25.24) | 100.13 (14.42) | 62.5 (18.38) |
| CQOLC 2 subscales | Burden | 0–40 | 16.25 (10.10) | ||
| Disruptiveness | 0–28 | 18.44 (6.48) | |||
| Positive adaptation | 0–28 | 20.38 (4.76) | |||
| Financial concerns | 0–12 | 8.63 (3.32) | |||
| Caregiver depression | CESD-R 3 total score | 0–60 | 18.69 (12.65) | 10.13 (7.02) | 27.25 (11.24) |
| WPAI 4 | Proportion of absenteeism, % | 0–100 | 41.04 (37.21) | ||
| Proportion of presenteeism-related impairment, % | 0–100 | 41.25 (38.71) | |||
| Overall work impairment, % | 0–100 | 57.85 (35.24) | 45.00 (38.40) | 79.00 (18.10) | |
| Activity impairment, % | 0–100 | 47.5 (27.45) | 32.50 (27.12) | 62.50 (19.01) | |
| Characteristics of Caregivers | |||
| Balancing multiple responsibilities | Physical caregiving demands | Non-physical aspects of caregiving | Social support |
| Aged 31–50 years Had a child/children <16 years Involved in all 4 caregiving roles | Physical caregiving ≥12 h spent on physical caregiving | Spousal relationship with patient Caring for ≥2 years Providing financial care Making decisions pertaining to the care of the patient | Lack of: |
| Foreign domestic helper | |||
| Home care service | |||
| Financial assistance | |||
| Patient Characteristics | |||
| Physical demands | Symptoms | ||
| Male patients | High caregiver-rated POS score of >20 Distant metastasis to bones and/or lungs | ||
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chua, C.K.T.; Wu, J.T.; Wong, Y.Y.; Qu, L.; Tan, Y.Y.; Neo, P.S.H.; Pang, G.S. Caregiving and Its Resulting Effects—The Care Study to Evaluate the Effects of Caregiving on Caregivers of Patients with Advanced Cancer in Singapore. Cancers 2016, 8, 105. https://doi.org/10.3390/cancers8110105
Chua CKT, Wu JT, Wong YY, Qu L, Tan YY, Neo PSH, Pang GS. Caregiving and Its Resulting Effects—The Care Study to Evaluate the Effects of Caregiving on Caregivers of Patients with Advanced Cancer in Singapore. Cancers. 2016; 8(11):105. https://doi.org/10.3390/cancers8110105
Chicago/Turabian StyleChua, Cheryl Kai Ting, Jun Tian Wu, Yin Yee Wong, Limin Qu, Yung Ying Tan, Patricia Soek Hui Neo, and Grace Suyin Pang. 2016. "Caregiving and Its Resulting Effects—The Care Study to Evaluate the Effects of Caregiving on Caregivers of Patients with Advanced Cancer in Singapore" Cancers 8, no. 11: 105. https://doi.org/10.3390/cancers8110105
APA StyleChua, C. K. T., Wu, J. T., Wong, Y. Y., Qu, L., Tan, Y. Y., Neo, P. S. H., & Pang, G. S. (2016). Caregiving and Its Resulting Effects—The Care Study to Evaluate the Effects of Caregiving on Caregivers of Patients with Advanced Cancer in Singapore. Cancers, 8(11), 105. https://doi.org/10.3390/cancers8110105