
Imaging in Colorectal Cancer: Progress and Challenges for the Clinicians

Abstract
:1. Introduction
2. Imaging Modalities for Treatment Optimisation
2.1. Assessment beyond RECIST
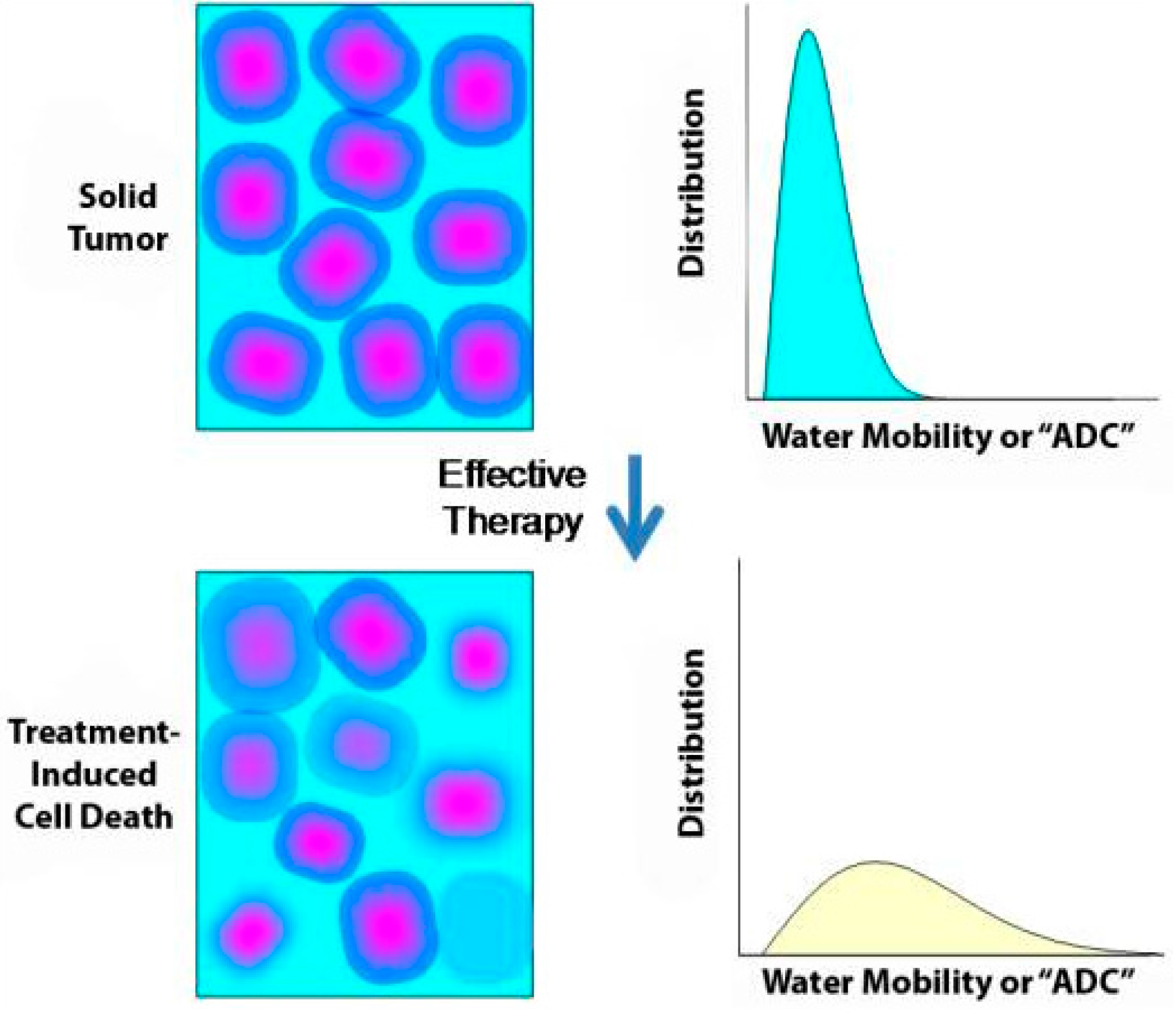
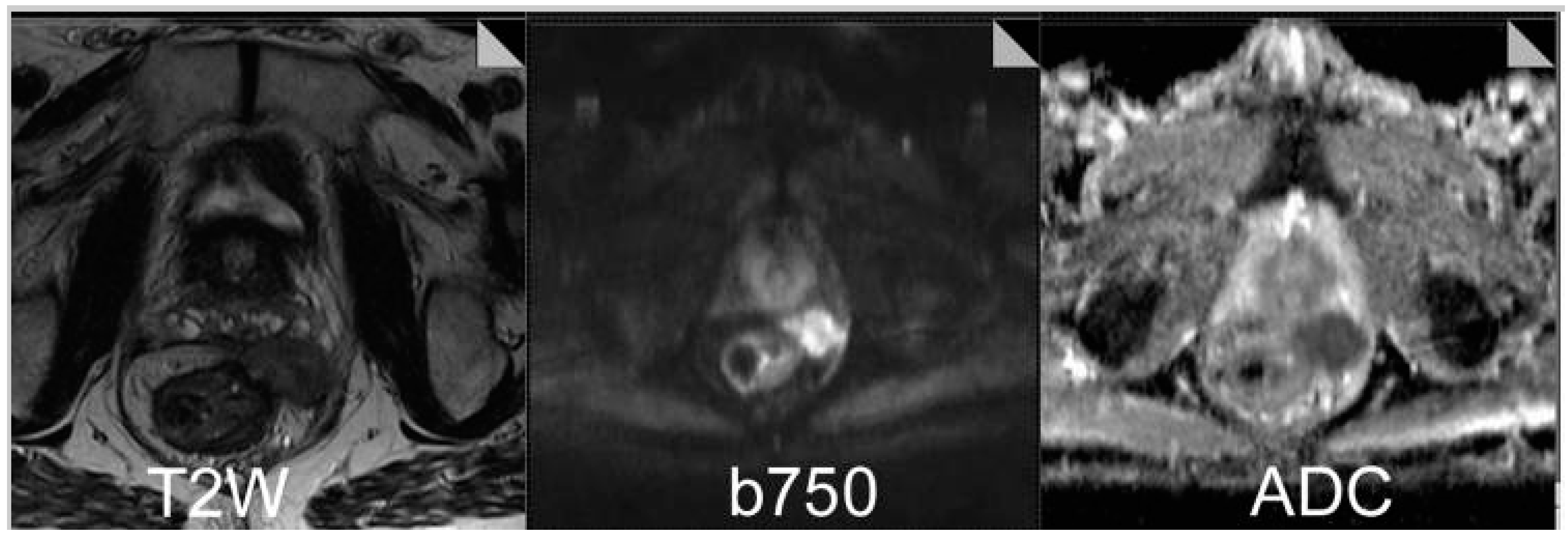
2.2. Functional Imaging with MRI
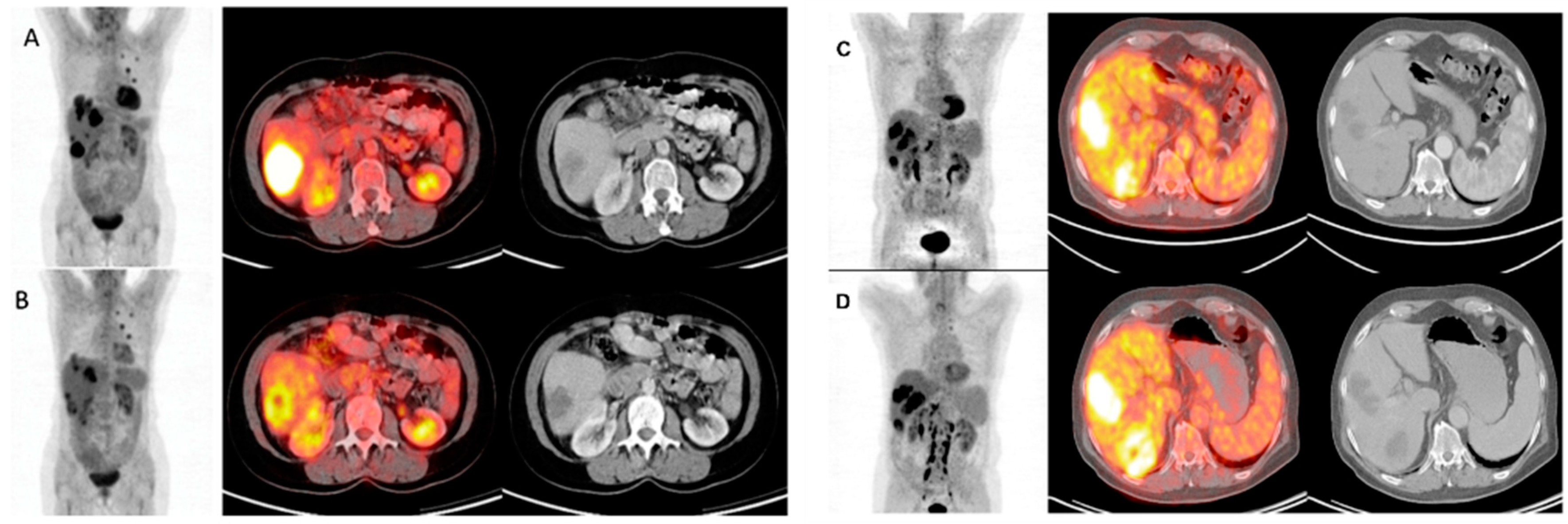
2.3. Metabolic Imaging with FDG-PET/CT
3. Rectal Cancer
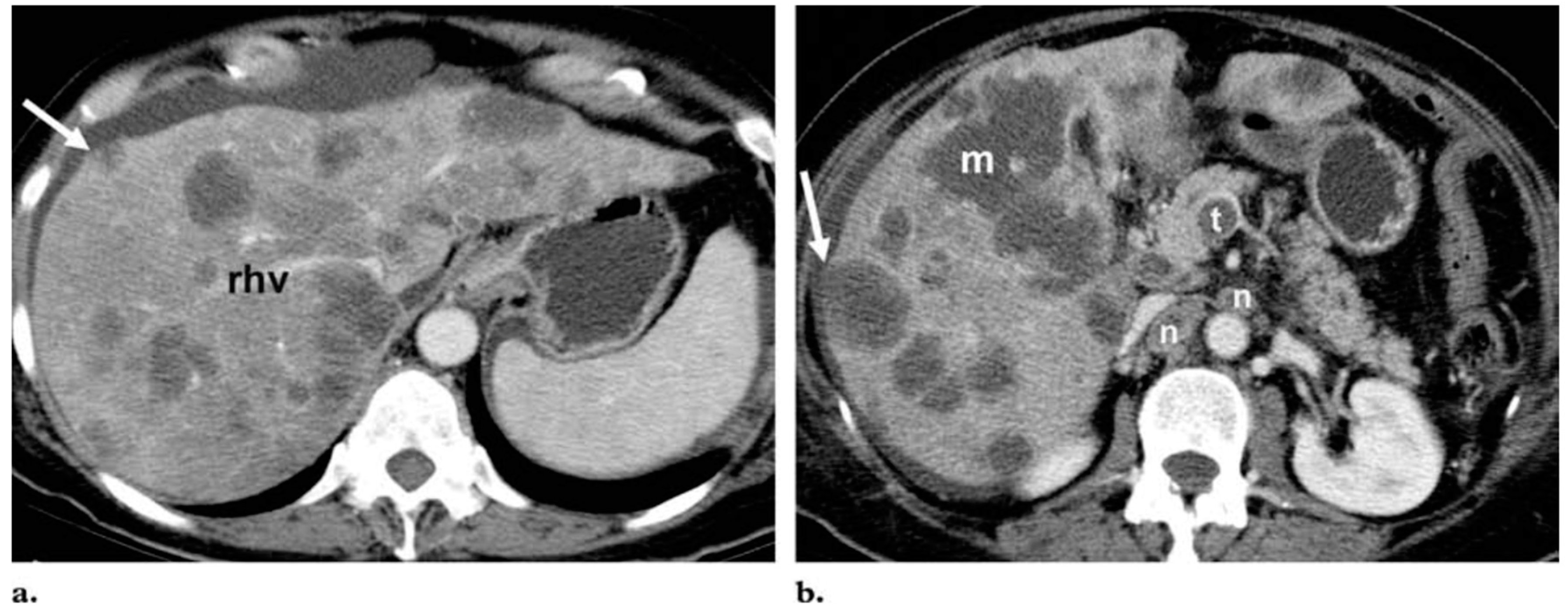
4. Hepatic Metastatic Disease
5. Limitations and Challenges of Assessing Treatment Response
6. Summary and Conclusions
Acknowledgments
Conflicts of Interest
References
- Globocan, F.S. Colorectal Cancer: Estimated Incidence, Mortality and Prevalence Worldwide in 2012. Available online: http://globocan.iarc.fr/Pages/fact_sheets_cancer.aspx (accessed on 30 August 2015).
- Ferlay, J.; Steliarova-Foucher, E.; Lortet-Tieulent, J.; Rosso, S.; Coebergh, J.W.W.; Comber, H.; Forman, D.; Bray, B. Cancer incidence and mortality patterns in Europe: Estimates for 40 countries in 2012. Eur. J. Cancer 2013, 49, 1374–1403. [Google Scholar] [CrossRef] [PubMed]
- Iyer, R.; Silverman, P.M.; DuBrow, R.A.; Charnsangavej, C. Imaging in the diagnosis, staging, and follow-up of colorectal cancer. Am. J. Roentgenol. 2002, 179, 3–13. [Google Scholar] [CrossRef]
- Kelloff, G.; Schilsky, R.L.; Alberts, D.S.; Day, R.W.; Guyton, K.Z.; Pearce, H.L. Colorectal adenomas: A prototype for the use of surrogate end points in the development of cancer prevention drugs. Clin. Cancer Res. 2004, 10, 3908–3918. [Google Scholar] [CrossRef] [PubMed]
- Gollub, M.; Schwartz, L.H.; Akhurst, T. Update on colorectal cancer imaging. Radiol. Clin. N. Am. 2007, 45, 85–118. [Google Scholar] [CrossRef] [PubMed]
- Johnston, P. Identification of clinically relevant molecular subtypes in colorectal cancer: The dawning of a New Era. Oncologist 2014, 19, 568–573. [Google Scholar] [CrossRef] [PubMed]
- McKeown, E.; Nelson, D.W.; Johnson, E.K.; Maykel, J.A.; Stojadinovic, A.; Nissan, A. Current approaches and challenges for monitoring treatment response in colon and rectal cancer. J. Cancer 2014, 5, 31–43. [Google Scholar] [CrossRef] [PubMed]
- De Geus-Oei, L.; Vriens, D.; van Laarhoven, H.W.M.; van der Graaf, W.T.A.; Oyen, W.J.G. Monitoring and predicting response to therapy with 18F-FDG PET in colorectal cancer: A Systematic Review. J. Nucl. Med. 2009, 50, 43S–54S. [Google Scholar] [CrossRef] [PubMed]
- Thoeny, H.; Ross, B. Predicting and monitoring cancer treatment response with DW-MRI. J. Magn. Reson. Imaging 2010, 32, 2–16. [Google Scholar] [CrossRef] [PubMed]
- Herbertson, R.; Scarsbrook, A.F.; Lee, S.T.; Tebbutt, N.; Scott, A.M. Established, emerging and future roles of PET/CT in the management of colorectal cancer. Clin. Radiol. 2009, 64, 225–237. [Google Scholar] [CrossRef] [PubMed]
- Kekelidze, M.; D’Errico, L.; Pansini, M.; Tyndall, A.; Hohmann, J. Colorectal cancer: Current imaging methods and future perspectives for the diagnosis, staging and therapeutic response evaluation. World J. Gastroenterol. 2013, 19, 8502–8514. [Google Scholar] [CrossRef] [PubMed]
- Therasse, P.; Arbuck, S.G.; Eisenhauer, E.A.; Wanders, J.; Kaplan, R.S.; Rubinstein, L. New guidelines to evaluate the response to treatment in solid tumors. J. Natl. Cancer Inst. 2000, 92, 205–216. [Google Scholar] [CrossRef] [PubMed]
- Eisenhauer, E.; Therasse, P.; Bogaerts, J.; Schwartz, L.H.; Sargent, D.; Ford, R. New response evaluation criteria in solid tumours: Revised RECIST guideline (version 1.1). Eur. J. Cancer 2009, 45, 228–247. [Google Scholar] [CrossRef] [PubMed]
- Wolchok, J.; Hoos, A.; O’Day, S.; Weber, J.S.; Hamid, O.; Lebbé, C.; Maio, M. Guidelines for the evaluation of immune therapy activity in solid tumors: Immune-related response criteria. Clin. Cancer Res. 2009, 15, 7412–7420. [Google Scholar] [CrossRef] [PubMed]
- Tirumani, S.; Kim, K.W.; Nishino, M.; Howard, S.A.; Krajewski, K.M.; Jagannathan, J.P. Update on the role of imaging in management of metastatic colorectal cancer. Radiographics 2014, 34, 1908–1928. [Google Scholar] [CrossRef] [PubMed]
- Lind, J.S.; Meijerink, M.R.; Dingemans, A.M.; van Kuijk, C.; Ollers, M.C.; de Ruysscher, D.; Postmus, P.E.; Smit, E.F. Dynamic contrast-enhanced CT in patients treated with sorafenib and erlotinib for non-small cell lung cancer: A new method of monitoring treatment? Eur. Radiol. 2010, 20, 2890–2898. [Google Scholar] [CrossRef] [PubMed]
- Cao, N.; Cao, M.; Chin-Sinex, H.; Mendonca, M.; Ko, S.C.; Stantz, K.M. Monitoring the effects of anti-angiogenesis on the radiation sensitivity of pancreatic cancer xenografts using dynamic contrast-enhanced computed tomography. Int. J. Radiat. Oncol. Biol. Phys. 2014, 88, 412–418. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nishino, M.; Giobbie-Hurder, A.; Gargano, M.; Suda, M.; Ramaiya, N.H.; Hodi, F.S. Developing a Common Language for Tumor Response to Immunotherapy: Immune-related Response Criteria using Unidimentional measurements. Clin. Cancer Res. 2013, 19, 3936–3943. [Google Scholar] [CrossRef] [PubMed]
- Zaniboni, A.; Savelli, G.; Pizzocaro, C.; Basile, P.; Massetti, V. Positron emission tomography for the response evaluation following treatment with chemotherapy in patients affected by colorectal liver metastases: A selected review. Gastroenterol. Res. Pract. 2015. [Google Scholar] [CrossRef] [PubMed]
- De Bruyne, S.; van Damme, N.; Smeets, P.; Ferdinande, L.; Ceelen, W.; Mertens, J. Value of DCE-MRI and FDG-PET/CT in the prediction of response to preoperative chemotherapy with bevacizumab for colorectal liver metastases. Br. J. Cancer 2012, 106, 1926–1933. [Google Scholar] [CrossRef] [PubMed]
- Chun, Y.; Vauthey, J.; Boonsirikamchai, P.; Maru, D.M.; Kopetz, S.; Palavecino, M. Association of computed tomography morphological criteria with pathologic response and survival in patients treated with bevacizumab for colorectal liver metastases. JAMA 2009, 302, 2338–2344. [Google Scholar] [CrossRef] [PubMed]
- Ricotta, R.; Vanzulli, A.; Moroni, M.; Colnago, B.; Oriani, M.; Nichelatti, M. Magnetic resonance imaging as an early indicator of clinical outcome in patients With metastatic colorectal carcinoma treated With cetuximab or panitumumab. Clin. Colorectal Cancer 2013, 12, 45–53. [Google Scholar] [CrossRef] [PubMed]
- O’Connor, J.; Rose, C.J.; Jackson, A.; Watson, Y.; Cheung, S.; Maders, F. DCE-MRI biomarkers of tumour heterogeneity predict CRC liver metastasis shrinkage following bevacizumab and FOLFOX-6. Br. J. Cancer 2011, 105, 139–145. [Google Scholar] [CrossRef] [PubMed]
- Padhani, A.; Liu, G.; Koh, D.M.; Chenevert, T.L.; Thoeny, H.C.; Takahara, T.; Dzik-Jurasz, A.; Ross, B.D.; van Cauteren, M.; Collins, D.; et al. Diffusion-weighted magnetic resonance imaging as a cancer biomarker: Consensus and recommendations. Neoplasia 2009, 11, 102–125. [Google Scholar] [CrossRef] [PubMed]
- Koh, D.; Blackledge, M.; Padhani, A.R.; Takahara, T.; Kwee, T.C.; Leach, M.O. Whole-Body Diffusion-weighted MRI: Tips, tricks, and pitfalls. Am. J. Roentgenol. 2012, 199, 252–262. [Google Scholar] [CrossRef] [PubMed]
- Lambregts, D.; Vandecaveye, V.; Barbaro, B.; Bakers, F.C.H.; Lambrecht, M.; Maas, M. Diffusion-weighted MRI for selection of complete responders after chemoradiation for locally advanced rectal cancer: A multicenter study. Ann. Surg. Oncol. 2011, 18, 2224–2231. [Google Scholar] [CrossRef] [PubMed]
- Koh, D.; Scurr, E.; Collins, D.; Kanber, B.; Norman, A.; Leach, M.O. Predicting response of colorectal hepatic metastasis: Value of pretreatment apparent diffusion coefficients. Am. J. Roentgenol. 2007, 188, 1001–1008. [Google Scholar] [CrossRef] [PubMed]
- Walker, A.; Zwintscher, N.P.; Johnson, E.K.; Maykel, J.A.; Stojadinovic, A.; Nissan, A. Future directions for monitoring treatment response in colorectal cancer. J. Cancer 2014, 5, 44–57. [Google Scholar] [CrossRef] [PubMed]
- Van den Abbeele, A.D. The lessons of GIST—PET and PET/CT: A new paradigm for imaging. Oncologist 2008, 13, 8–13. [Google Scholar] [CrossRef] [PubMed]
- Gauthé, M.; Richard-Molard, M.; Cacheux, W.; Michel, P.; Jouve, J.; Mitry, E. Role of fluorine 18 fluorodeoxyglucose positron emission tomography/computed tomography in gastrointestinal cancers. Dig. Liver Dis. 2015, 47, 443–454. [Google Scholar] [CrossRef] [PubMed]
- Hendlisz, A.; Golfinopoulos, V.; Garcia, C.; Covas, A.; Emonts, P.; Ameye, L. Serial FDG–PET/CT for early outcome prediction in patients with metastatic colorectal cancer undergoing chemotherapy. Ann. Oncol. 2012, 23, 1687–1693. [Google Scholar] [CrossRef] [PubMed]
- Skougaard, K.; Nielsen, D.; Jensen, B.V.; Hendel, H.W. Comparison of EORTC criteria and PERCIST for PET/CT response evaluation of patients with metastatic colorectal cancer treated with irinotecan and cetuximab. J. Nucl. Med. 2013, 54, 1026–1031. [Google Scholar] [CrossRef] [PubMed]
- Deleporte, A.; Hendlisz, A.; Garcia, C.; Delaunoit, T.; Maréchal, R.; Peeters, M. SoMore trial: Early metabolic response assessment of a sorafenib (SOR) and capecitabine (CAP) combination in chemorefractory metastatic colorectal cancer (mCRC). J. Clin. Oncol. 2014, 32, 524. [Google Scholar]
- Hendlisz, A.; Deleporte, A.; Delaunoit, T.; Maréchal, R.; Peeters, M.; Holbrechts, S.; van den Eynde, M.; Houbiers, G.; Filleul, B.; van Laethem, J.L.; et al. The prognostic significance of metabolic response heterogeneity in metastatic colorectal cancer. PLoS ONE 2015, 10, e0138341. [Google Scholar] [CrossRef] [PubMed]
- Sabet, A.; Meyer, C.; Aouf, A.; Sabet, A.; Ghamari, S.; Pieper, C.C. Early post-treatment FDG PET predicts survival after 90Y microsphere radioembolization in liver-dominant metastatic colorectal cancer. Eur. J. Nucl. Med. Mol. Imaging 2015, 42, 370–376. [Google Scholar] [CrossRef] [PubMed]
- Chinot, O.L.; Macdonald, D.R.; Abrey, L.E.; Zahlmann, G.; Kerloeguen, Y.; Cloughesy, T.F. Response assessment criteria for glioblastoma: Practical adaptation and implementation in clinical trials of antiangiogenic therapy. Curr. Neurol. Neurosci. Rep. 2013, 13, 347. [Google Scholar] [CrossRef] [PubMed]
- Smith, A.D.; Shah, S.N.; Rini, B.I.; Lieber, M.L.; Remer, E.M. Morphology, attenuation, size, and structure (MASS) criteria: Assessing response and predicting clinical outcome in metastatic renal cell carcinoma on antiangiogenic targeted therapy. Am. J. Roentgenol. 2010, 194, 1470–1478. [Google Scholar] [CrossRef] [PubMed]
- Arora, A.; Kumar, A. Treatment response evaluation and follow-up in hepatocellular carcinoma. J. Clin. Exp. Hepatol. 2014, 4, S126–S129. [Google Scholar]
- Makris, N.; Boellaard, R.; vanLingen, A.; Lammertsma, A.A.; vanDongen, G.A.M.S.; Verheul, H.M. PET/CT-derived whole-body and bone marrow dosimetry of 89Zr-Cetuximab. J. Nucl. Med. 2015, 56, 249–254. [Google Scholar] [CrossRef] [PubMed]
- Willemien Menke-van der Houven van Oordt, C.; Gootjes, E.C.; Huisman, M.C.; Vugts, D.J.; Roth, C.; Marije Luik, A.; Mulder, E.R. 89Zr-cetuximab PET imaging in patients with advanced colorectal cancer. Oncotarget 2014, 6, 30384–30393. [Google Scholar]
- NCT01691391. Treatment Optimization of Cetuximab in Patients With Metastatic Colorectal Cancer Based on Tumor Uptake of 89Zr-labeled Cetuximab Assessed by PET. Available online: https://clinicaltrials.gov/ct2/show/NCT01691391 (accessed on 30 August 2015).
- NCT02117466. Image Guided Treatment Optimization with Cetuximab for Patients with Metastatic Colorectal Cancer (IMPACT-CRC). Available online: https://clinicaltrials.gov/ct2/show/NCT02117466 (accessed on 30 August 2015).
- Haggar, F.; Boushey, R. Colorectal cancer epidemiology: Incidence, mortality, survival, and risk factors. Clin. Colon Rectal Surg. 2009, 22, 191–197. [Google Scholar] [CrossRef] [PubMed]
- Liu, Z.; Zhou, T.; Liang, X.B.; Ma, J.J.; Zhang, G.J. Learning curve of endorectal ultrasonography in preoperative staging of rectal carcinoma. Mol. Clin. Oncol. 2014, 2, 1085–1090. [Google Scholar] [CrossRef] [PubMed]
- Beets-Tan, R.G.; Beets, G.L.; Vliegen, R.F.; Kessels, A.G.; van Boven, H.; De Bruine, A.; von Meyenfeldt, M.F.; Baeten, C.G.; van Engelshoven, J.M. Accuracy of magnetic resonance imaging in prediction of tumour-free resection margin in rectal cancer surgery. Lancet 2001, 357, 497–504. [Google Scholar] [CrossRef]
- Kwok, H.; Bissett, I.P.; Hill, G.L. Preoperative staging of rectal cancer. Int. J. Colorectal Dis. 2000, 15, 9–20. [Google Scholar] [CrossRef] [PubMed]
- Brown, G.; Richards, C.J.; Bourne, M.W.; Newcombe, R.G.; Radcliffe, A.G.; Dallimore, N.S. Morphologic predictors of lymph node status in rectal cancer with use of high-spatial-resolution MR imaging with histopathologic comparison. Radiology 2003, 227, 371–377. [Google Scholar] [CrossRef] [PubMed]
- Beets-Tan, R.G.; Lambregts, D.M.; Maas, M.; Bipat, S.; Barbaro, B.; Caseiro-Alves, F.; Curvo-Semedo, L.; Fenlon, H.M.; Gollub, M.J.; Gourtsoyianni, S.; et al. Magnetic resonance imaging for the clinical management of rectal cancer patients: Recommendations from the 2012 European Society of Gastrointestinal and Abdominal Radiology (ESGAR) consensus meeting. Eur. Radiol. 2013, 23, 2522–2531. [Google Scholar] [CrossRef] [PubMed]
- Legou, F.; Chiaradia, M.; Baranes, L.; Pigneur, F.; Zegai, B.; Djabbari, M. Imaging strategies before beginning treatment of colorectal liver metastases. Diagn. Interv. Imaging 2014, 95, 505–512. [Google Scholar] [CrossRef] [PubMed]
- Cantisani, V.; Grazhdani, H.; Fioravanti, C.; Rosignuolo, M.; Calliada, F.; Messineo, D. Liver metastases: Contrast-enhanced ultrasound compared with computed tomography and magnetic resonance. World J. Gastroenterol. 2014, 7, 9998–10007. [Google Scholar] [CrossRef] [PubMed]
- Postema, M.; Gilja, O.H. Contrast-enhanced and targeted ultrasound. World J. Gastroenterol. 2011, 17, 28–41. [Google Scholar]
- Maruyama, H.; Takahashi, M.; Ishibashi, H.; Yoshikawa, M.; Yokosuka, O. Contrast-enhanced ultrasound for characterisation of hepatic lesions appearing non-hypervascular on CT in chronic liver diseases. Br. J. Radiol. 2012, 85, 351–357. [Google Scholar] [CrossRef] [PubMed]
- Bipat, S.; Niekel, M.C.; Comans, E.F.I.; Nio, C.Y.; Bemelman, W.A.; Verhoef, C. Imaging modalities for the staging of patients with colorectal cancer. Neth. J. Med. 2012, 70, 26–34. [Google Scholar] [PubMed]
- Oliva, M.; Saini, S. Liver cancer imaging: Role of CT, MRI, US and PET. Cancer Imaging 2004, 4, S42–S46. [Google Scholar]
- Hamer, O.W.; Aguirre, D.A.; Casola, G.; Lavine, J.E.; Woenckhaus, M.; Sirlin, C.B. Fatty liver: Imaging patterns and pitfalls. Radiographics 2006, 26, 1637–1653. [Google Scholar] [CrossRef] [PubMed]
- Selzner, M.; Hany, T.F.; Wildbrett, P.; McCormack, L.; Kadry, Z.; Clavien, P.A. Does the novel PET/CT imaging modality impact on the treatment of patients with metastatic colorectal cancer of the liver? Ann. Surg. 2004, 240, 1027–1034. [Google Scholar] [CrossRef] [PubMed]
- Ruers, T.J.; Wiering, B.; van der Sijp, J.R.; Roumen, R.M.; de Jong, K.P.; Comans, E.F.; Pruim, J.; Dekker, H.M.; Krabbe, P.F.; Oyen, W.J. Improved selection of patients for hepatic surgery of colorectal liver metastases with (18)F-FDG PET: A randomized study. J. Nucl. Med. 2009, 50, 1036–1041. [Google Scholar] [CrossRef] [PubMed]
- Hicks, R.J.; Ware, R.E.; Lau, E.W. PET/CT: Will it change the way that we use CT in cancer imaging? Cancer Imaging 2006, 6, S52–S62. [Google Scholar] [CrossRef] [PubMed]
- Culverwell, A.D.; Chowdhury, F.U.; Scarsbrook, A.F. Optimizing the role of FDG PET-CT for potentially operable metastatic colorectal cancer. Abdom. Imaging 2012, 37, 1021–1031. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Grade | Response Criteria |
|---|---|
| Complete response | Disappearance of all target lesions. Any pathological lymph nodes (whether target or non-target) must have reduction in short axis to <10 mm. |
| Partial response | At least a 30% decrease in the sum of diameters of target lesions, taking as reference the baseline sum diameters. |
| Progressive disease | At least a 20% increase in the sum of diameters of target lesions, the appearance of one or more new lesions is also considered progression |
| Stable disease | Neither sufficient shrinkage to qualify for partial response nor sufficient increase to qualify for progressive disease |
| WHO | irRC * | |
|---|---|---|
| New, measurable lesions (i.e., ≥5 × 5 mm) | Always represent PD | Incorporated into tumor burden |
| New, nonmeasurable lesions (i.e., < 5 × 5 mm) | Always represent PD | Do not define progression (but preclude irCR) |
| Non-index lesions | Changes contribute to defining BOR of CR, PR, SD, and PD | Contribute to defining irCR (complete disappearance required) |
| Complete response | Disappearance of all lesions in two consecutive observations not less than 4 wk apart | Disappearance of all lesions in two consecutive observations not less than 4 weeks apart |
| Partial response | ≥50% decrease in SPD of all index lesions compared with baseline in two observations at least 4 weeks apart, in absence of new lesions or unequivocal progression of non-index lesions | ≥50% decrease in tumor burden compared with baseline in two observations at least 4 weeks apart |
| Stable disease | 50% decrease in SPD compared with baseline cannot be established nor 25% increase compared with nadir, in absence of new lesions or unequivocal progression of non-index lesions | 50% decrease in tumour burden compared with baseline cannot be established nor 25% increase compared with nadir |
| Progressive disease | At least 25% increase in SPD compared with nadir and/or unequivocal progression of non-index lesions and/or appearance of new lesions (at any single time point) | At least 25% increase in tumour burden compared with nadir (at any single time point) in two consecutive observations at least 4 weeks apart |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Van Cutsem, E.; Verheul, H.M.W.; Flamen, P.; Rougier, P.; Beets-Tan, R.; Glynne-Jones, R.; Seufferlein, T. Imaging in Colorectal Cancer: Progress and Challenges for the Clinicians. Cancers 2016, 8, 81. https://doi.org/10.3390/cancers8090081
Van Cutsem E, Verheul HMW, Flamen P, Rougier P, Beets-Tan R, Glynne-Jones R, Seufferlein T. Imaging in Colorectal Cancer: Progress and Challenges for the Clinicians. Cancers. 2016; 8(9):81. https://doi.org/10.3390/cancers8090081
Chicago/Turabian StyleVan Cutsem, Eric, Henk M. W. Verheul, Patrik Flamen, Philippe Rougier, Regina Beets-Tan, Rob Glynne-Jones, and Thomas Seufferlein. 2016. "Imaging in Colorectal Cancer: Progress and Challenges for the Clinicians" Cancers 8, no. 9: 81. https://doi.org/10.3390/cancers8090081
APA StyleVan Cutsem, E., Verheul, H. M. W., Flamen, P., Rougier, P., Beets-Tan, R., Glynne-Jones, R., & Seufferlein, T. (2016). Imaging in Colorectal Cancer: Progress and Challenges for the Clinicians. Cancers, 8(9), 81. https://doi.org/10.3390/cancers8090081