
Medical-Waste Chain: A Medical Waste Collection, Classification and Treatment Management by Blockchain Technology

 , ,
, , {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
- We look at the critical opportunities that blockchain technology offers for the handling and classifying of medical equipment and supplies to improve operational transparency, traceability, security, and accountability in waste management processes. It will be clarified in the section Medical-Waste Chain Architecture.
- We present a case-study implementation (i.e., proof-of-concept) based on Hyperledger Fabric. To advance extensive research into waste collection, segregation, and treatment systems, we share our implementation of Medical-Waste Chain at https://github.com/Masquerade0127/medical-blockchain accessed on 12 June 2022, which will be analyzed in the Implementation section.
- We measure and evaluate Medical-Waste Chain based on many different scenarios. The evaluation results are outlined in detail in the Evaluation section.
2. Background
2.1. Blockchain Technology
- Ledger [27,28] is a data storage on a blockchain that uses a consensus algorithm to store immutable, sequential entries in blocks. For each channel, each node keeps a copy of the ledger. For efficient processing, the shared ledger encapsulates the whole transaction history for each channel and adds query capabilities.
- Cryptography [28] is one of the essential components of blockchain, which allows relevant access, and stores data in immutable blocks with a fixed sequential order, and establishes identity and authenticity.
- Consensus [28] is another crucial component of blockchain that is connected to how data submissions are accepted onto the distributed ledger. Consensus algorithms [29] are used in blockchain technology to maintain a single history of blocks by synchronizing the data inside the chain of blocks to ensure that no contradicted or invalid transactions exist. There are many existing types of consensus rules, such as Proof of Work (PoW), Proof of Stake (PoS), Proof of Authority (PoA), and Proof of Elapsed Time (PoET). According to these algorithms, all participating nodes must prove something for someone to be granted permission to add a block to the current blockchain.
2.2. Smart Contract
2.2.1. Ethereum
2.2.2. Hyperledger Fabric
2.3. Hyperledger Caliper
3. Related Work
3.1. Blockchain-Based Management Systems
3.2. Blockchain-Based Medical Systems
3.3. Blockchain-Based Waste Management System
3.4. Limitation of Existing Research
4. Materials and Methods
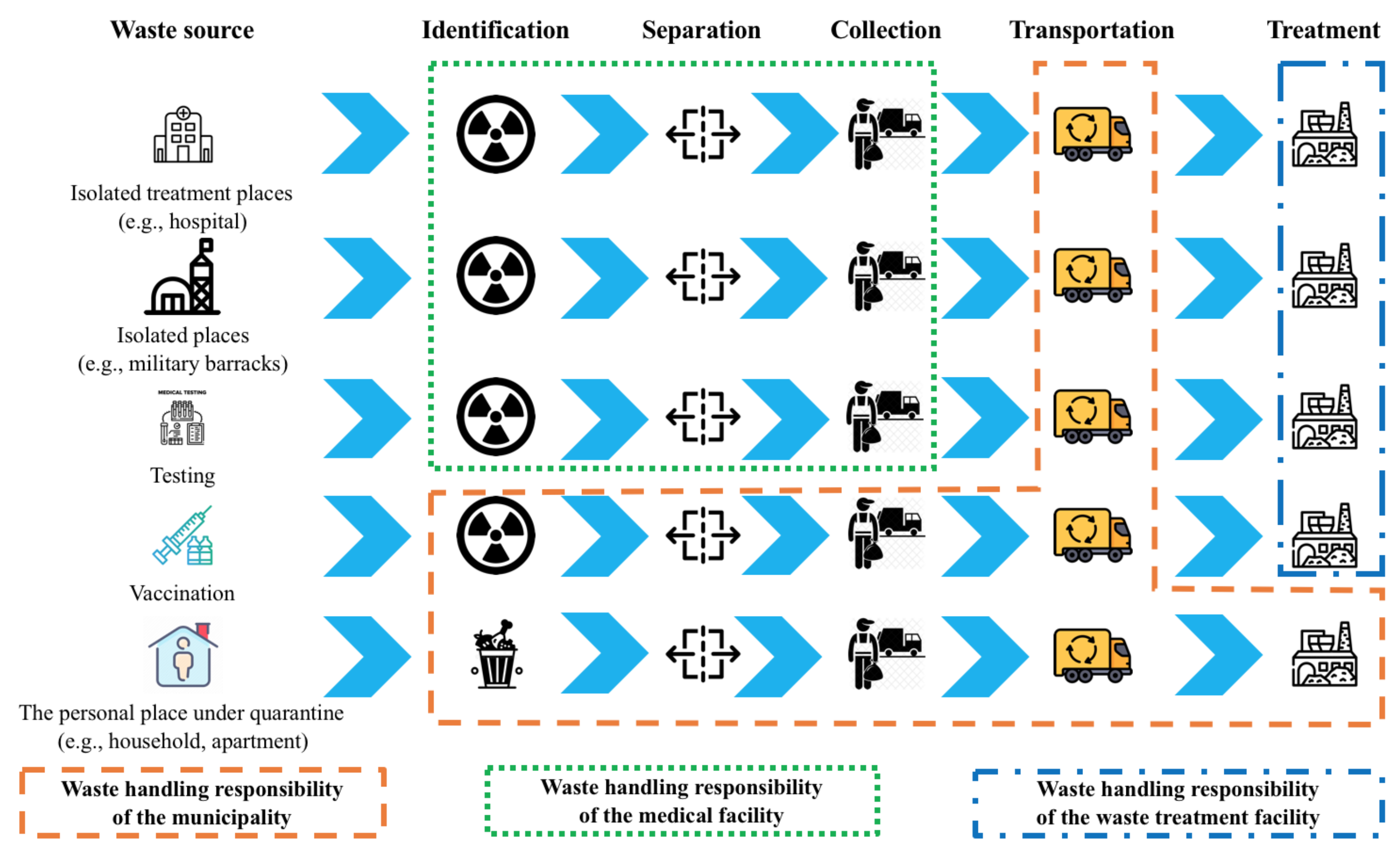
4.1. COVID-19 Waste Treatment Process in Vietnam
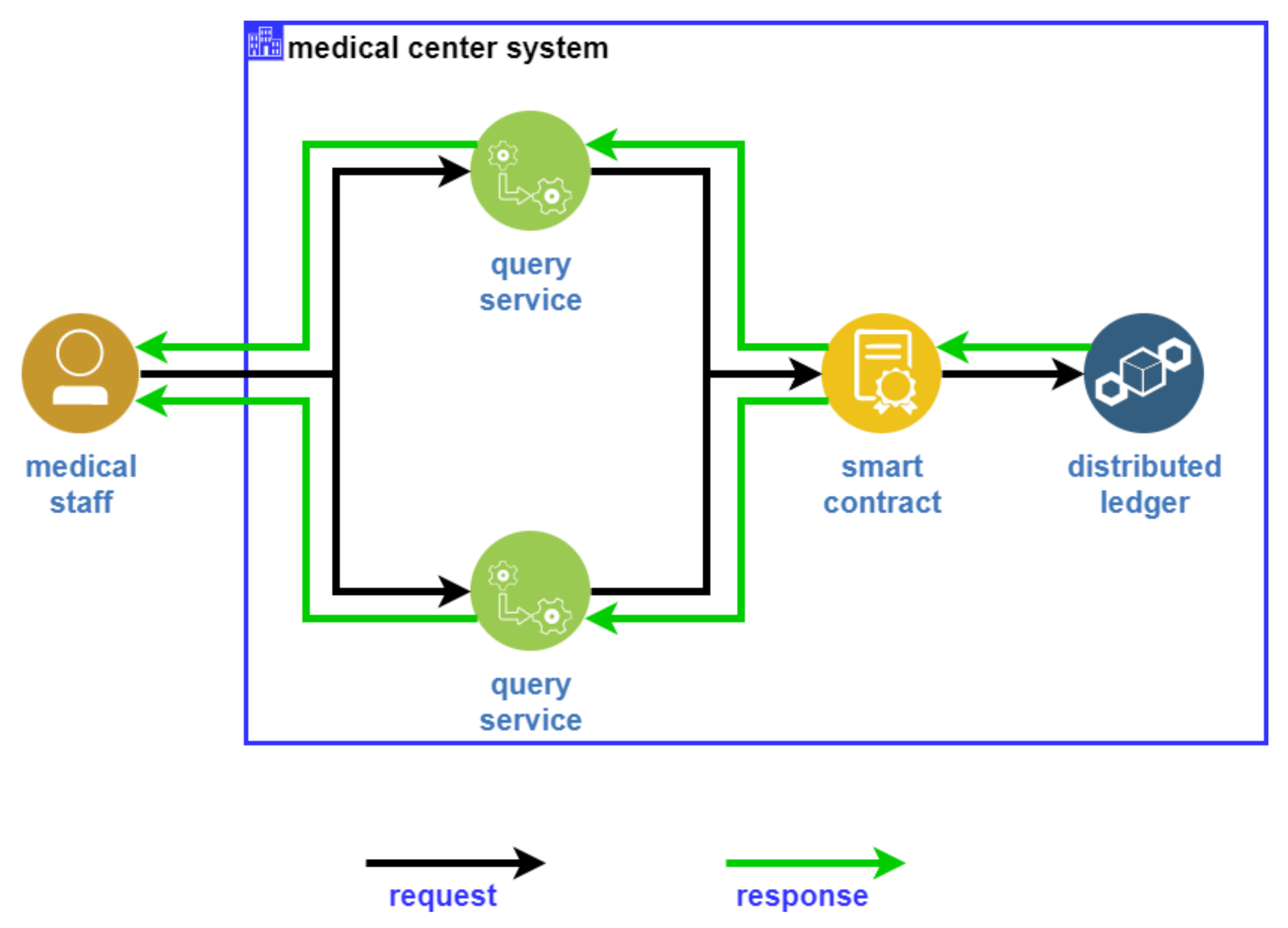
4.2. Medical-Waste Chain Architecture
5. Implementation
5.1. Data Creation
| Algorithm 1 Create data |
|
5.2. Query Data
| Algorithm 2 Query data |
|
5.3. Modify Data
| Algorithm 3 Query data |
|
6. Evaluation Scenarios
6.1. Environment Setting
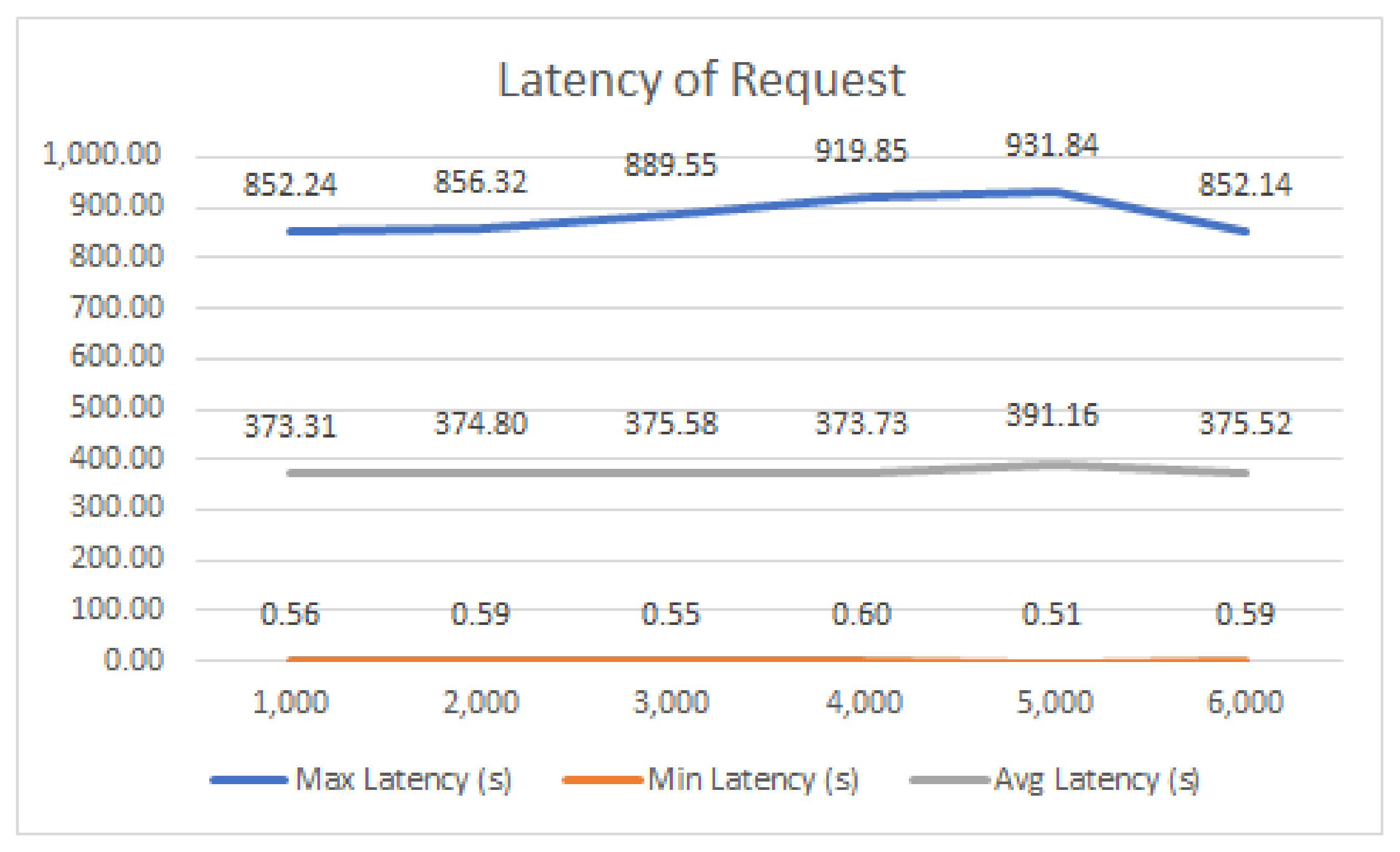
6.2. First Scenario
6.3. Second Scenario
6.4. Third Scenario
6.5. Security and Privacy Discussion
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ahmad, R.W.; Salah, K.; Jayaraman, R.; Yaqoob, I.; Omar, M.; Ellahham, S. Blockchain-based forward supply chain and waste management for COVID-19 medical equipment and supplies. IEEE Access 2021, 9, 44905–44927. [Google Scholar] [CrossRef] [PubMed]
- Zand, A.D.; Heir, A.V. Emanating challenges in urban and healthcare waste management in Isfahan, Iran after the outbreak of COVID-19. Environ. Technol. 2021, 42, 329–336. [Google Scholar] [CrossRef] [PubMed]
- Klemeš, J.J.; Jiang, P.; Van Fan, Y.; Bokhari, A.; Wang, X.C. COVID-19 pandemics Stage II–energy and environmental impacts of vaccination. Renew. Sustain. Energy Rev. 2021, 150, 111400. [Google Scholar] [CrossRef] [PubMed]
- Van Fan, Y.; Jiang, P.; Hemzal, M.; Klemeš, J.J. An update of COVID-19 influence on waste management. Sci. Total Environ. 2021, 754, 142014. [Google Scholar] [CrossRef] [PubMed]
- Jiang, P.; Klemeš, J.J.; Fan, Y.V.; Fu, X.; Bee, Y.M. More is not enough: A deeper understanding of the COVID-19 impacts on healthcare, energy and environment is crucial. Int. J. Environ. Res. Public Health 2021, 18, 684. [Google Scholar] [CrossRef]
- Steenmans, K.; Taylor, P.; Steenmans, I. Blockchain Technology for Governance of Plastic Waste Management: Where Are We? Soc. Sci. 2021, 10, 434. [Google Scholar] [CrossRef]
- Thanh, L.N.T.; Phien, N.N.; Vo, H.K.; Luong, H.H.; Anh, T.D.; Tuan, K.N.H.; Son, H.X. UIP2SOP: A unique IoT network applying single sign-on and message queue protocol. Int. J. Adv. Comput. Sci. Appl. 2021, 12, 19–30. [Google Scholar] [CrossRef]
- Luong, H.H.; Anh, T.D.; Tuan, K.N.H.; Son, H.X. IoHT-MBA: An Internet of Healthcare Things (IoHT) Platform based on Microservice and Brokerless Architecture. Int. J. Adv. Comput. Sci. Appl. 2021, 12, 591–601. [Google Scholar] [CrossRef]
- Nguyen, T.T.L.; Vo, H.K.; Luong, H.H.; Nguyen, H.T.K.; Dao, A.T.; Ha, X.S. Toward a unique IoT network via single sign-on protocol and message queue. In Proceedings of the International Conference on Computer Information Systems and Industrial Management, Elk, Poland, 24–26 September 2021; pp. 270–284. [Google Scholar]
- Thanh, L.N.T.; Vo, H.K.; Luong, H.H.; Tuan, K.N.H.; Dao, A.T.; Son, H.X. Toward a Security IoT Platform with High Rate Transmission and Low Energy Consumption. In Proceedings of the International Conference on Computational Science and Its Applications, Cagliari, Italy, 13–16 September 2021; pp. 647–662. [Google Scholar]
- Lam, N.T.T.; Son, H.X.; Le, T.H.; Nguyen, T.A.; Vo, H.K.; Luong, H.H.; Anh, T.D.; Tuan, K.N.H.; Nguyen, H.V.K. BMDD: A novel approach for IoT platform (Broker-less and Microservice architecture, Decentralized identity, and Dynamic transmission messages). Int. J. Adv. Comput. Sci. Appl. 2022, 8, e950. [Google Scholar]
- Thanh, L.N.T.; Phien, N.N.; Vo, H.K.; Luong, H.H.; Anh, T.D.; Tuan, K.N.H.; Son, H.X. SIP-MBA: A secure IoT platform with brokerless and micro-service architecture. Int. J. Adv. Comput. Sci. Appl. 2021, 12, 586–593. [Google Scholar] [CrossRef]
- Gupta, N.; Bedi, P. E-waste management using blockchain based smart contracts. In Proceedings of the 2018 International Conference on Advances in Computing, Communications and Informatics (ICACCI), Bangalore, India, 19–22 September 2018; pp. 915–921. [Google Scholar]
- Poongodi, M.; Hamdi, M.; Vijayakumar, V.; Rawal, B.S.; Maode, M. An effective electronic waste management solution based on blockchain smart contract in 5G communities. In Proceedings of the 2020 IEEE 3rd 5G World Forum (5GWF), Bangalore, India, 10–12 September 2020; pp. 1–6. [Google Scholar]
- Laouar, M.R.; Hamad, Z.T.; Eom, S. Towards blockchain-based urban planning: Application for waste collection management. In Proceedings of the 9th International Conference on Information Systems and Technologies, Cairo, Egypt, 24–26 March 2019; pp. 1–6. [Google Scholar]
- Dasaklis, T.K.; Casino, F.; Patsakis, C. A traceability and auditing framework for electronic equipment reverse logistics based on blockchain: The case of mobile phones. In Proceedings of the 2020 11th International Conference on Information, Intelligence, Systems and Applications (IISA), Piraeus, Greece, 15–17 July 2020; pp. 1–7. [Google Scholar]
- Le, H.T.; Thanh, L.N.T.; Vo, H.K.; Luong, H.H.; Tuan, K.N.H.; Anh, T.D.; Vuong, K.H.N.; Son, H.X. Patient-Chain: Patient-centered Healthcare System a Blockchain-based Technology in Dealing with Emergencies. In Proceedings of the International Conference on Parallel and Distributed Computing: Applications and Technologies, London, UK, 30–31 July 2022; pp. 576–583. [Google Scholar]
- Vujičić, D.; Jagodić, D.; Ranđić, S. Blockchain technology, bitcoin, and Ethereum: A brief overview. In Proceedings of the 2018 17th International Symposium Infoteh-Jahorina (Infoteh), East Sarajevo, Bosnia and Herzegovina, 21–23 March 2018; pp. 1–6. [Google Scholar]
- Duong-Trung, N.; Ha, X.S.; Phan, T.T.; Trieu, P.N.; Nguyen, Q.N.; Pham, D.; Huynh, T.T.; Le, H.T. Multi-sessions mechanism for decentralized cash on delivery system. Int. J. Adv. Comput. Sci. Appl. 2019, 10, 553–560. [Google Scholar] [CrossRef]
- Nakamoto, S. Bitcoin: A Peer-to-Peer Electronic Cash System. Bitcoin.org. Disponible. 2009. Available online: https://bitcoin.org/en/bitcoin-paper (accessed on 25 November 2021).
- Uddin, M.A.; Stranieri, A.; Gondal, I.; Balasubramanian, V. A survey on the adoption of blockchain in iot: Challenges and solutions. Blockchain Res. Appl. 2021, 2, 100006. [Google Scholar] [CrossRef]
- Alharby, M.; Van Moorsel, A. Blockchain-based smart contracts: A systematic mapping study. arXiv 2017, arXiv:1710.06372. [Google Scholar]
- Androulaki, E.; Barger, A.; Bortnikov, V.; Cachin, C.; Christidis, K.; De Caro, A.; Enyeart, D.; Ferris, C.; Laventman, G.; Manevich, Y. Hyperledger fabric: A distributed operating system for permissioned blockchains. In Proceedings of the Thirteenth EuroSys Conference, Porto, Portugal, 23–26 April 2018; pp. 1–15. [Google Scholar]
- Shi, S.; He, D.; Li, L.; Kumar, N.; Khan, M.K.; Choo, K.K.R. Applications of blockchain in ensuring the security and privacy of electronic health record systems: A survey. Comput. Secur. 2020, 97, 101966. [Google Scholar] [CrossRef]
- Casino, F.; Dasaklis, T.K.; Patsakis, C. A systematic literature review of blockchain-based applications: Current status, classification and open issues. Telemat. Inform. 2019, 36, 55–81. [Google Scholar] [CrossRef]
- Monrat, A.A.; Schelén, O.; Andersson, K. A survey of blockchain from the perspectives of applications, challenges, and opportunities. IEEE Access 2019, 7, 117134–117151. [Google Scholar] [CrossRef]
- Alketbi, A.; Nasir, Q.; Talib, M.A. Blockchain for government services—Use cases, security benefits and challenges. In Proceedings of the 2018 15th Learning and Technology Conference (L&T), Jeddah, Saudi Arabia, 25–26 February 2018; pp. 112–119. [Google Scholar]
- Jaradat, A.; Ali, O.; AlAhmad, A. Blockchain Technology: A Fundamental Overview. In Blockchain Technologies for Sustainability; Springer: Berlin/Heidelberg, Germany, 2022; pp. 1–24. [Google Scholar]
- Mamun, Q. Blockchain technology in the future of healthcare. Smart Health 2022, 23, 100223. [Google Scholar] [CrossRef]
- Zheng, Z.; Xie, S.; Dai, H.N.; Chen, W.; Chen, X.; Weng, J.; Imran, M. An overview on smart contracts: Challenges, advances and platforms. Future Gener. Comput. Syst. 2020, 105, 475–491. [Google Scholar] [CrossRef] [Green Version]
- Díaz-Santiso, J.; Fraga-Lamas, P. E-Voting System Using Hyperledger Fabric Blockchain and Smart Contracts. Eng. Proc. 2021, 7, 11. [Google Scholar] [CrossRef]
- Crosby, M.; Nachiappan; Pattanayak, P.; Verma, S.; Kalyanaraman, V. Blockchain technology: Beyond bitcoin. Appl. Innov. 2016, 2, 71. [Google Scholar]
- Son, H.X.; Nguyen, M.H.; Phien, N.N.; Le, H.T.; Nguyen, Q.N.; Dinh, V.; Tru, P.; Nguyen, P. Towards a mechanism for protecting seller’s interest of cash on delivery by using smart contract in hyperledger. Int. J. Adv. Comput. Sci. Appl. 2019, 10, 45–50. [Google Scholar] [CrossRef]
- Kim, D. An integrated supply chain management system: A case study in healthcare sector. In Proceedings of the International Conference on Electronic Commerce and Web Technologies, Copenhagen, Denmark, 23–26 August 2005; pp. 218–227. [Google Scholar]
- Shahbaz, M.S.; Raja Zuraidah, R.M.; Bin, M.F.; Rehman, F. What is supply chain risk management? A review. Adv. Sci. Lett. 2017, 23, 9233–9238. [Google Scholar] [CrossRef]
- Lavastre, O.; Gunasekaran, A.; Spalanzani, A. Effect of firm characteristics, supplier relationships and techniques used on supply chain risk management (SCRM): An empirical investigation on French industrial firms. Int. J. Prod. Res. 2014, 52, 3381–3403. [Google Scholar] [CrossRef]
- Douladiris, K.; Dasaklis, T.; Casino, F.; Douligeris, C. A Blockchain framework for reverse logistics of used medical equipment. In Proceedings of the 24th Pan-Hellenic Conference on Informatics, Athens, Greece, 20–22 November 2020; pp. 148–151. [Google Scholar]
- Subramanian, N.; Chaudhuri, A.; Kayıkcı, Y. Blockchain Applications in Reverse Logistics. In Blockchain and Supply Chain Logistics; Springer: Berlin/Heidelberg, Germany, 2020; pp. 67–81. [Google Scholar]
- Farouk, M.; Darwish, S.M. Reverse logistics solution in e-supply chain management by blockchain technology. Egypt. Comput. Sci. J. 2020, 44, 22–34. [Google Scholar]
- Le, N.T.T.; Nguyen, Q.N.; Phien, N.N.; Duong-Trung, N.; Huynh, T.T.; Nguyen, T.P.; Son, H.X. Assuring Non-fraudulent Transactions in Cash on Delivery by Introducing Double Smart Contracts. Int. J. Adv. Comput. Sci. Appl. 2019, 10, 677–684. [Google Scholar] [CrossRef]
- Le, H.T.; Le, N.T.T.; Phien, N.N.; Duong-Trung, N. Introducing multi shippers mechanism for decentralized cash on delivery system. Int. J. Adv. Comput. Sci. Appl. 2019, 10, 590–597. [Google Scholar] [CrossRef]
- Ha, X.S.; Le, H.T.; Metoui, N.; Duong-Trung, N. Dem-cod: Novel access-control-based cash on delivery mechanism for decentralized marketplace. In Proceedings of the 2020 IEEE 19th International Conference on Trust, Security and Privacy in Computing and Communications (TrustCom), Guangzhou, China, 10–13 November 2020; pp. 71–78. [Google Scholar]
- Ha, X.S.; Le, T.H.; Phan, T.T.; Nguyen, H.H.D.; Vo, H.K.; Duong-Trung, N. Scrutinizing trust and transparency in cash on delivery systems. In Proceedings of the International Conference on Security, Privacy and Anonymity in Computation, Communication and Storage, Nanjing, China, 18–20 December 2020; pp. 214–227. [Google Scholar]
- Kumar, T.; Ramani, V.; Ahmad, I.; Braeken, A.; Harjula, E.; Ylianttila, M. Blockchain utilization in healthcare: Key requirements and challenges. In Proceedings of the 2018 IEEE 20th International Conference on e-Health Networking, Applications and Services (Healthcom), Ostrava, Czech Republic, 17–20 September 2018; pp. 1–7. [Google Scholar]
- De Oliveira, M.T.; Reis, L.H.; Carrano, R.C.; Seixas, F.L.; Saade, D.C.; Albuquerque, C.V.; Fernandes, N.C.; Olabarriaga, S.D.; Medeiros, D.S.; Mattos, D.M. Towards a blockchain-based secure electronic medical record for healthcare applications. In Proceedings of the ICC 2019-2019 IEEE International Conference on Communications (ICC), Shanghai, China, 20–24 May 2019; pp. 1–6. [Google Scholar]
- Wilber, K.; Vayansky, S.; Costello, N.; Berdik, D.; Jararweh, Y. A Survey on Blockchain for Healthcare Informatics and Applications. In Proceedings of the 2020 7th International Conference on Internet of Things: Systems, Management and Security (IOTSMS), Paris, France, 14–16 December 2020; pp. 1–9. [Google Scholar]
- Shynu, P.; Menon, V.G.; Kumar, R.L.; Kadry, S.; Nam, Y. Blockchain-based secure healthcare application for diabetic-cardio disease prediction in fog computing. IEEE Access 2021, 9, 45706–45720. [Google Scholar] [CrossRef]
- Torky, M.; Hassanien, A.E. COVID-19 blockchain framework: Innovative approach. arXiv 2020, arXiv:2004.06081. [Google Scholar]
- Hölbl, M.; Kompara, M.; Kamišalić, A.; Nemec Zlatolas, L. A systematic review of the use of blockchain in healthcare. Symmetry 2018, 10, 470. [Google Scholar] [CrossRef] [Green Version]
- FarmaTrust Report 2022. Available online: https://farmatrust.com (accessed on 17 May 2022).
- Organ Tree 2022. Available online: https://organ-tree.com (accessed on 17 May 2022).
- Yaga, D.; Mell, P.; Roby, N.; Scarfone, K. Blockchain technology overview. arXiv 2019, arXiv:1906.11078. [Google Scholar]
- Wüst, K.; Gervais, A. Do you need a blockchain? In Proceedings of the 2018 Crypto Valley Conference on Blockchain Technology (CVCBT), Zug, Switzerland, 20–22 June 2018; pp. 45–54. [Google Scholar]
- Quynh, N.T.T.; Son, H.X.; Le, T.H.; Huy, H.N.D.; Vo, K.H.; Luong, H.H.; Tuan, K.N.H.; Anh, T.D.; Duong-Trung, N. Toward a Design of Blood Donation Management by Blockchain Technologies. In Proceedings of the International Conference on Computational Science and Its Applications, Cagliari, Italy, 13–16 September 2021; pp. 78–90. [Google Scholar]
- Son, H.X.; Le, T.H.; Quynh, N.T.T.; Huy, H.N.D.; Duong-Trung, N.; Luong, H.H. Toward a Blockchain-Based Technology in Dealing with Emergencies in Patient-Centered Healthcare Systems. In Proceedings of the International Conference on Mobile, Secure, and Programmable Networking, Paris, France, 28–29 October 2020; pp. 44–56. [Google Scholar]
- Duong-Trung, N.; Son, H.X.; Le, H.T.; Phan, T.T. On Components of a Patient-Centered Healthcare System Using Smart Contract. In Proceedings of the 2020 4th International Conference on Cryptography, Security and Privacy, Nanjing, China, 10–12 January 2020; pp. 31–35. [Google Scholar] [CrossRef] [Green Version]
- Duong-Trung, N.; Son, H.X.; Le, H.T.; Phan, T.T. Smart Care: Integrating Blockchain Technology into the Design of Patient-Centered Healthcare Systems. In Proceedings of the 2020 4th International Conference on Cryptography, Security and Privacy, ICCSP, Nanjing, China, 10–12 January 2020; pp. 105–109. [Google Scholar] [CrossRef] [Green Version]
- Jiang, P.; Fu, X.; Van Fan, Y.; Klemeš, J.J.; Chen, P.; Ma, S.; Zhang, W. Spatial-temporal potential exposure risk analytics and urban sustainability impacts related to COVID-19 mitigation: A perspective from car mobility behaviour. J. Clean. Prod. 2021, 279, 123673. [Google Scholar] [CrossRef] [PubMed]
- Leonard, A. The Story of Stuff: How Our Obsession with Stuff Is Trashing the Planet, Our Communities, and Our Health-and a Vision for Change; Simon and Schuster: New York, NY, USA, 2010. [Google Scholar]
- Morseletto, P. Targets for a circular economy. Resour. Conserv. Recycl. 2020, 153, 104553. [Google Scholar] [CrossRef]
- The Circular Economy in Detail. Available online: https://archive.ellenmacarthurfoundation.org/explore/the-circular-economy-in-detail (accessed on 30 March 2022).
- How Amazon is Investing in a Circular Economy. Available online: https://www.aboutamazon.com/news/sustainability/how-amazon-is-investing-in-a-circular-economy (accessed on 30 March 2022).
- Korhonen, J.; Honkasalo, A.; Seppälä, J. Circular economy: The concept and its limitations. Ecol. Econ. 2018, 143, 37–46. [Google Scholar] [CrossRef]
- Sheehan, J.R.; Lyons, B.; Holt, F. The use of Lean Methodology to reduce personal protective equipment wastage in children undergoing congenital cardiac surgery, during the COVID-19 pandemic. Pediatr. Anesth. 2021, 31, 213–220. [Google Scholar] [CrossRef] [PubMed]
- The Circular Economy in Detail. Available online: https://www.cdc.gov/vaccines/covid-19/hcp/wastage-operational-summary.html#vaccine-wastage-best-practices (accessed on 30 March 2022).
- Manninen, K.; Koskela, S.; Antikainen, R.; Bocken, N.; Dahlbo, H.; Aminoff, A. Do circular economy business models capture intended environmental value propositions? J. Clean. Prod. 2018, 171, 413–422. [Google Scholar] [CrossRef] [Green Version]
- Nandi, S.; Sarkis, J.; Hervani, A.A.; Helms, M.M. Redesigning supply chains using blockchain-enabled circular economy and COVID-19 experiences. Sustain. Prod. Consum. 2021, 27, 10–22. [Google Scholar] [CrossRef]
- Govindan, K.; Mina, H.; Alavi, B. A decision support system for demand management in healthcare supply chains considering the epidemic outbreaks: A case study of coronavirus disease 2019 (COVID-19). Transp. Res. Part E Logist. Transp. Rev. 2020, 138, 101967. [Google Scholar] [CrossRef]
- Schmelz, D.; Pinter, K.; Strobl, S.; Zhu, L.; Niemeier, P.; Grechenig, T. Technical mechanics of a trans-border waste flow tracking solution based on blockchain technology. In Proceedings of the 2019 IEEE 35th International Conference on Data Engineering Workshops (ICDEW), Macao, 8–12 April 2019; pp. 31–36. [Google Scholar]
- LaGrega, M.D.; Buckingham, P.L.; Evans, J.C. Hazardous Waste Management; Waveland Press: Long Grove, IL, USA, 2010. [Google Scholar]
- Nguyen, T.D.; Kawai, K.; Nakakubo, T. Estimation of COVID-19 waste generation and composition in Vietnam for pandemic management. Waste Manag. Res. 2021, 39, 1356–1364. [Google Scholar] [CrossRef]
- Hoang, N.M.; Son, H.X. A dynamic solution for fine-grained policy conflict resolution. In Proceedings of the 3rd International Conference on Cryptography, Security and Privacy, Kuala Lumpur, Malaysia, 19–21 January 2019; pp. 116–120. [Google Scholar]
- Son, H.X.; Hoang, N.M. A novel attribute-based access control system for fine-grained privacy protection. In Proceedings of the 3rd International Conference on Cryptography, Security and Privacy, Kuala Lumpur, Malaysia, 19–21 January 2019; pp. 76–80. [Google Scholar]
- Son, H.X.; Dang, T.K.; Massacci, F. REW-SMT: A new approach for rewriting xacml request with dynamic big data security policies. In Proceedings of the International Conference on Security, Privacy and Anonymity in Computation, Communication and Storage, Guangzhou, China, 12–15 December 2017; pp. 501–515. [Google Scholar]
- Xuan, S.H.; Tran, L.K.; Dang, T.K.; Pham, Y.N. Rew-xac: An approach to rewriting request for elastic abac enforcement with dynamic policies. In Proceedings of the 2016 International Conference on Advanced Computing and Applications (ACOMP), Can Tho City, Vietnam, 23–25 November 2016; pp. 25–31. [Google Scholar]
- Son, H.X.; Chen, E. Towards a fine-grained access control mechanism for privacy protection and policy conflict resolution. Int. J. Adv. Comput. Sci. Appl. 2019, 10, 507–516. [Google Scholar] [CrossRef] [Green Version]
- Thi, Q.N.T.; Dang, T.K.; Van, H.L.; Son, H.X. Using json to specify privacy preserving-enabled attribute-based access control policies. In Proceedings of the International Conference on Security, Privacy and Anonymity in Computation, Communication and Storage, Guangzhou, China, 12–15 December 2017; pp. 561–570. [Google Scholar]











Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Le, H.T.; Quoc, K.L.; Nguyen, T.A.; Dang, K.T.; Vo, H.K.; Luong, H.H.; Le Van, H.; Gia, K.H.; Cao Phu, L.V.; Nguyen Truong Quoc, D.; et al. Medical-Waste Chain: A Medical Waste Collection, Classification and Treatment Management by Blockchain Technology. Computers 2022, 11, 113. https://doi.org/10.3390/computers11070113
Le HT, Quoc KL, Nguyen TA, Dang KT, Vo HK, Luong HH, Le Van H, Gia KH, Cao Phu LV, Nguyen Truong Quoc D, et al. Medical-Waste Chain: A Medical Waste Collection, Classification and Treatment Management by Blockchain Technology. Computers. 2022; 11(7):113. https://doi.org/10.3390/computers11070113
Chicago/Turabian StyleLe, Hai Trieu, Khoi Le Quoc, The Anh Nguyen, Khoa Tran Dang, Hong Khanh Vo, Huong Hoang Luong, Hieu Le Van, Khiem Huynh Gia, Loc Van Cao Phu, Duy Nguyen Truong Quoc, and et al. 2022. "Medical-Waste Chain: A Medical Waste Collection, Classification and Treatment Management by Blockchain Technology" Computers 11, no. 7: 113. https://doi.org/10.3390/computers11070113
APA StyleLe, H. T., Quoc, K. L., Nguyen, T. A., Dang, K. T., Vo, H. K., Luong, H. H., Le Van, H., Gia, K. H., Cao Phu, L. V., Nguyen Truong Quoc, D., Huyen Nguyen, T., Son, H. X., & Duong-Trung, N. (2022). Medical-Waste Chain: A Medical Waste Collection, Classification and Treatment Management by Blockchain Technology. Computers, 11(7), 113. https://doi.org/10.3390/computers11070113