On the Use of Voice Signals for Studying Sclerosis Disease

 ,
, 
Abstract
:1. Introduction
Phonetic Apparatus
- Lungs—these produce the airflow that enters into the bronchus and trachea.
- Larynx—this contains the vocal cords that vibrate to produce vowels. Vocal cords are folds of muscles located at the level of the glottis, which represents the space between the vocal cords. The vocal cords vibrate when they are closed to obstruct the airflow through the glottis.
- Oral cavity—this is composed by the tongue, palate, lips, and teeth. The tongue allows the articulation of consonants and vowels approaching the palate. The lips are involved in the production of several consonant sounds also affecting the sounds of vowels. The teeth are used to generate dental consonants.
- Nasal cavity—this is responsible for nasal sounds, particularly nasal consonants such as m and n. The nasal term means that the sound is produced by sending a stream of air through the nose but not through the mouth, as it is occluded by the lips or tongue.
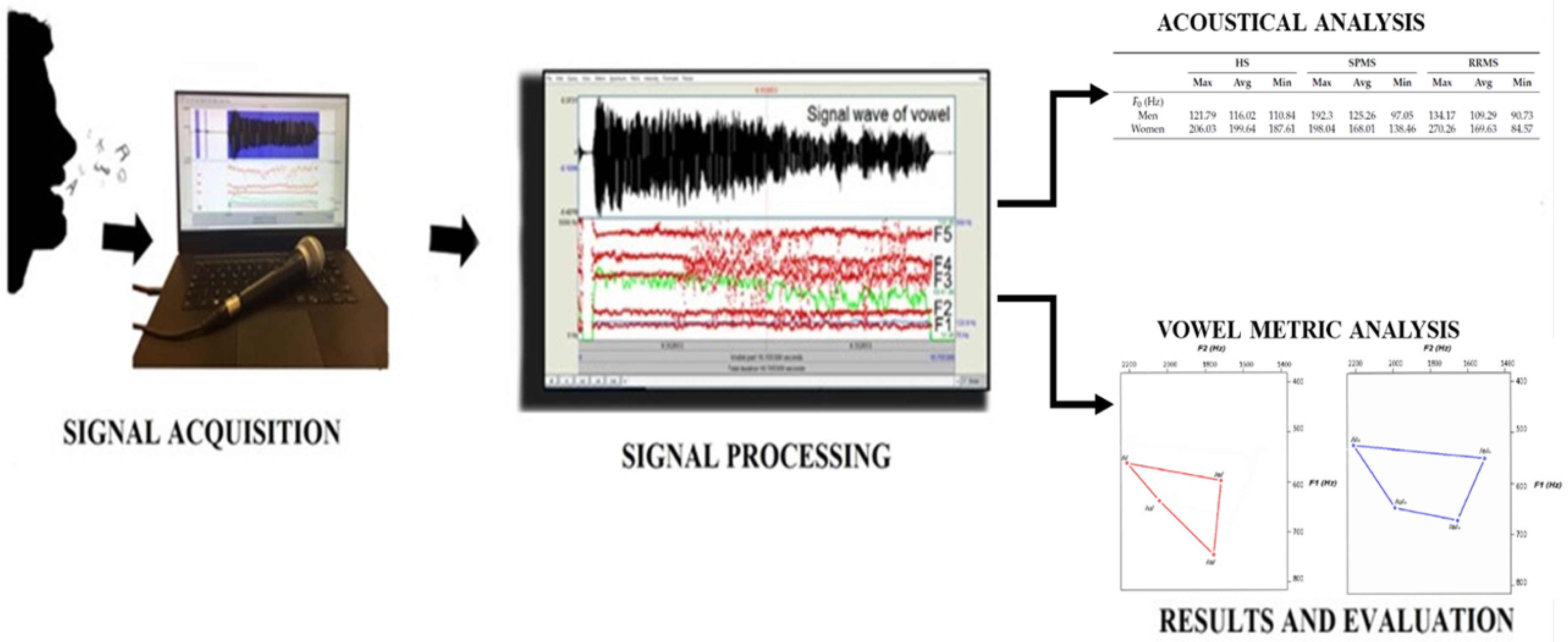
2. Methods
2.1. Acoustic Analysis
- Fundamental frequency ()—this represents the cycle of the wave.
- Jitter—this is a measure of frequency variability in the sound wave, expressed as a term (the term is used to distinguish the cycle of in the figure).
- Shimmer—this is a measure of amplitude variability in the sound wave.
- HNR—this estimates the level of additive noise in human voice signals associated to a leak of the glottal closure during phonation.
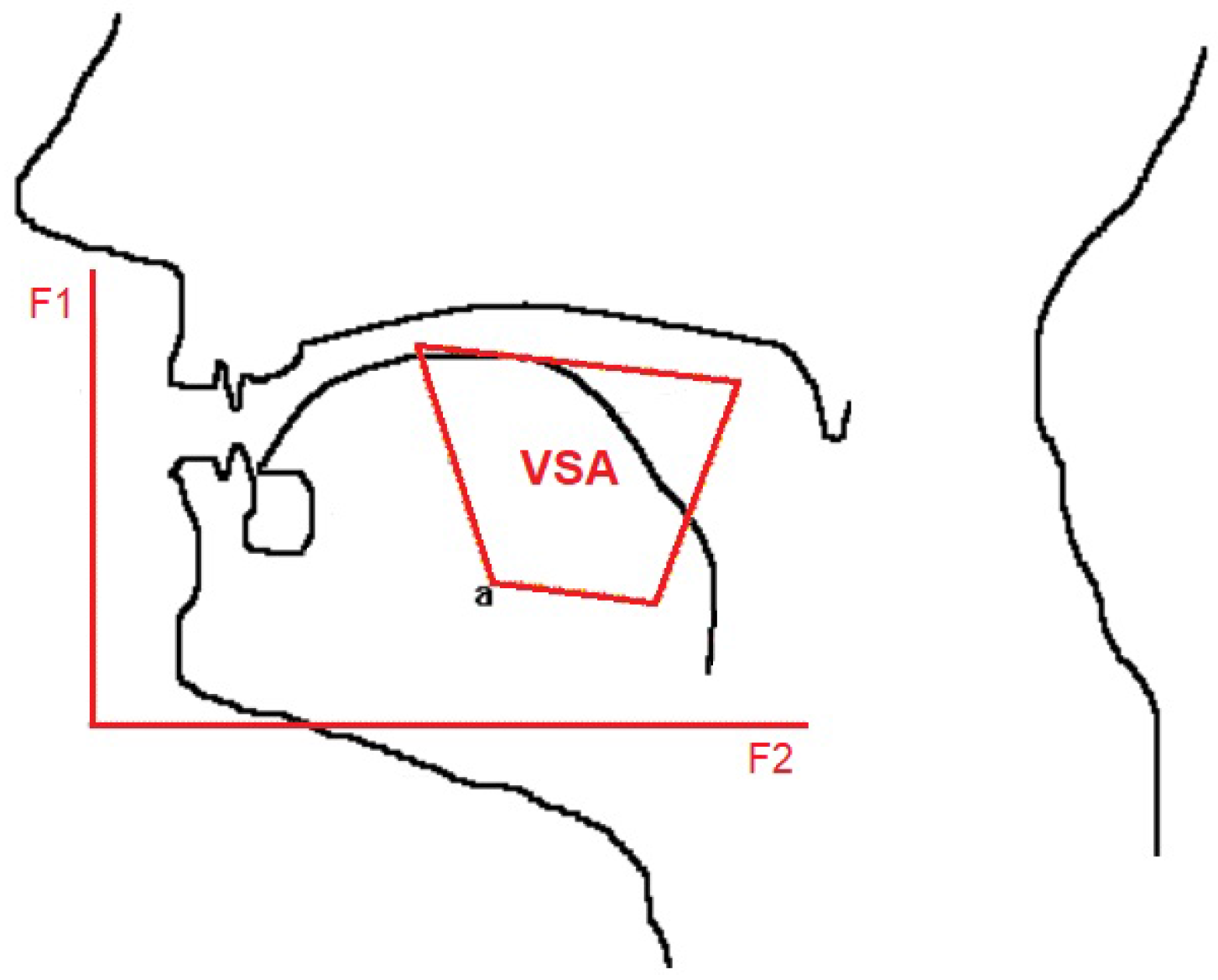
2.2. Vowel Metric
3. Results and Discussion
- 18 patients affected by SMSP (7 men and 11 women);
- 35 patients affected by SMRR (11 men and 24 women).
3.1. Results by Acoustical Analysis
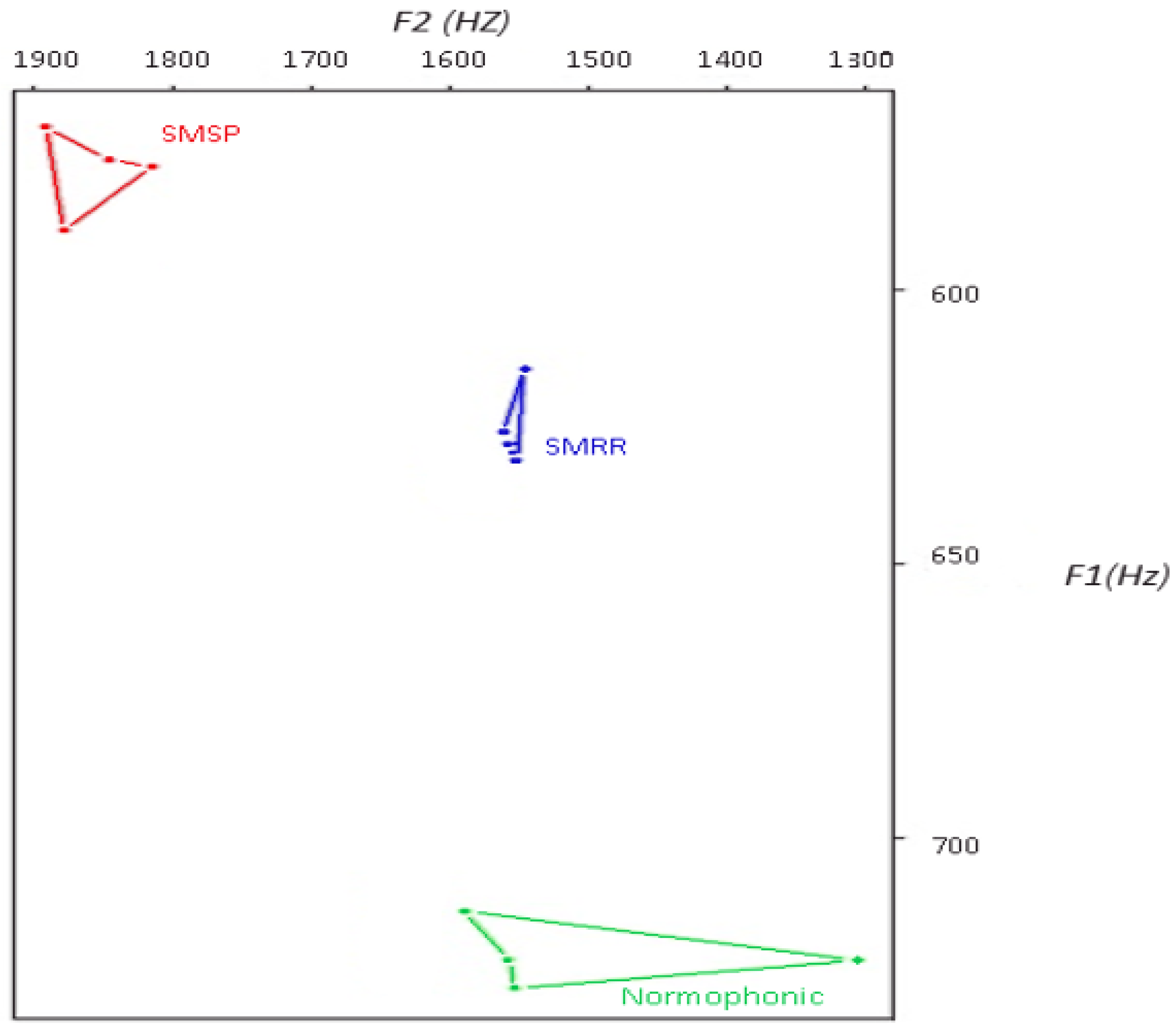
3.2. Results by Vowel Metric Analysis
3.3. Statistical Results
4. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Scarpini, E. Neurodegenerative Diseases: Clinical Aspects, Molecular Genetics and Biomarkers; Springer Science and Business: Berlin, Germany, 2014. [Google Scholar]
- Bethoux, F.; Robert, J.F. Multiple Sclerosis and Related Disorders: Diagnosis, Medical Management, and Rehabilitation; Demos Medical Publishing: New York, NY, USA, 2013. [Google Scholar]
- Lublin, F.D.; Reingold, S.C.; Cohen, J.A.; Cutter, G.R.; Sorensen, P.S.; Thompson, A.J. Defining the clinical course of multiple sclerosis, the 2013 revisions. Neurology 2014, 83, 278–286. [Google Scholar] [CrossRef] [PubMed]
- Murdoch, B.E. Acquired Speech and Language Disorders; John Wiley and Sons: Hoboken, NJ, USA, 2013. [Google Scholar]
- Campbell, W.W. Pocket Guide and Toolkit to Dejong’s Neurologic Examination; Lippincott Williams and Wilkins: Philadelphia, PA, USA, 2007. [Google Scholar]
- Rahimifar, P.; Soltani, M.; Moradi, N. Rehabilitation Treatment In Dysarthria Caused By Stroke. Adv. Biosci. Clin. Med. 2017, 26, 1–6. [Google Scholar] [CrossRef]
- Mirarchi, D.; Vizza, P.; Tradigo, G.; Lombardo, N.; Arabia, G.; Veltri, P. Signal Analysis for Voice Evaluation in Parkinson’s Disease. In Proceedings of the IEEE International Conference on Healthcare Informatics, Park City, UT, USA, 23–26 August 2017. [Google Scholar]
- Baghai-Eavary, L.; Beet, S.W. Automatic Speech Signal Analysis for Clinical Diagnosis and Assessment of Speech Disorders; Springer: Berlin, Germany, 2012. [Google Scholar]
- Shaoa, J.; MacCallumb, J.K.; Zhangb, Y.; Sprecherb, A.; Jianga, J.J. Acoustic analysis of the tremulous voice: Assessing the utility of the correlation dimension and perturbation parameters. J. Commun. Disord. 2010, 43, 35–44. [Google Scholar] [CrossRef] [PubMed]
- Barsties, B.; Bodt, M.D. Assessment of voice quality: Current state-of-the-art. Auris Nasus Larynx 2015, 42, 183–188. [Google Scholar] [CrossRef] [PubMed]
- Tjaden, K.; Wilding, G.E. Effect of Rate Reduction and Increased Loudness on Acoustic Measures of Anticipatory Coarticulation in Multiple Sclerosis and Parkinson’s Disease. J. Speech Lang. Hear. Res. 2005, 48, 261–277. [Google Scholar] [CrossRef]
- Sussman, J.E.; Tjaden, K. Perceptual measures of speech from individuals with Parkinson’s disease and multiple sclerosis: Intelligibility and beyond. J. Speech Lang. Hear. Res. 2012, 55, 1208–1219. [Google Scholar] [CrossRef]
- Rusz, J.; Cmejla, R.; Ruzickova, H.; Ruzicka, E. Quantitative acoustic measurements for characterization of speech and voice disorders in early untreated Parkinson’s disease. J. Acoust. Soc. Am. 2011, 129, 350–367. [Google Scholar] [CrossRef] [PubMed]
- Tjaden, K.; Lam, J.; Wilding, G. Vowel acoustics in Parkinson’s disease and multiple sclerosis: Comparison of clear, loud, and slow speaking conditions. J. Speech Lang. Hear. Res. 2013, 56, 1485–1502. [Google Scholar] [CrossRef]
- Sapir, S.; Ramig, L.; Fox, C. Speech and swallowing disorders in Parkinson disease. Curr. Opin. Otolaryngol. Head Neck Surg. 2008, 16, 205–210. [Google Scholar] [CrossRef] [PubMed]
- Teixeira, J.P.; Oliveira, C.; Lopes, C. Vocal Acoustic Analysis–Jitter, Shimmer and HNR Parameters. In Proceedings of the CENTERIS 2013 Conference on ENTERprise Information Systems/HCIST 2013, International Conference on Health and Social Care Information Systems and Technologies, Lisboa, Portugal, 23–25 October 2013; pp. 1112–1122. [Google Scholar]
- Lansford, K.L.; Liss, J.M. Vowel acoustics in dysarthria: Speech disorder diagnosis and classification. J. Speech Lang. Hear. Res. 2014, 57, 57–67. [Google Scholar] [CrossRef]
- Palumbo, A.; Veltri, P.; Calabrese, B.; Vizza, P.; Cannataro, M.; Garozzo, A.; Lombardo, N.; Amato, F. Experiences of Using a DSP Based Device for Vocal Signal Analysis. In MAVEBA: Models and Analysis of Vocal Emissions for Biomedical Applications; Firenze University Press: Florence, Italy, 2011; pp. 187–189. [Google Scholar]
- Rani, K.U.; Holi, M.S. Analysis of Speech Characteristics of Neurological Diseases and Their Classification. In Proceedings of the Third IEEE International Conference on Computing Communication and Networking Technologies, Karur, India, 26–28 July 2012; pp. 1–6. [Google Scholar]
- Bauer, V.; Aleric, Z.; Jancic, E. Comparing Voice Self-Assessment with Auditory Perceptual Analysis in Patients with Multiple Sclerosis. Int. Arch. Otorhinolaryngol. 2015, 19, 100–105. [Google Scholar] [PubMed]
- Hartelius, L.; Nord, L.; Buder, E.H. Acoustic analysis of dysarthria associated with multiple sclerosis. Clin. Linguist. Phon. 1995, 9, 95–120. [Google Scholar] [CrossRef]
- Feijó, A.V.; Parente, M.A.; Behlau, M.; Haussen, S.; de Veccino, M.C.; Martignago, B.C. Acoustic Analysis of Voice in Multiple Sclerosis Patients. J. Voice 2004, 18, 341–347. [Google Scholar] [CrossRef] [PubMed]
- García, M.J.V.; Cobeta, I.; Martín, G.; Alonso-Navarro, H.; Jimenez-Jimenez, F.J. Acoustic Analysis of Voice in Huntington’s Disease Patients. J. Voice 2011, 25, 208–217. [Google Scholar] [CrossRef] [PubMed]
- Maryn, Y.; Weenink, D. Objective Dysphonia Measures in the Program Praat: Smoothed Cepstral Peak Prominence and Acoustic Voice Quality Index. J. Voice 2015, 29, 35–43. [Google Scholar] [CrossRef] [PubMed]
- Manfredi, C.; Giordano, A.; Schoentgen, J.; Fraj, S.; Bocchi, L.; Dejonckere, P.H. Perturbation measurements in highly irregular voice signals: Performances/validity of analysis software tools. Biomed. Signal Process. Control 2012, 7, 409–416. [Google Scholar] [CrossRef]
- Sandoval, S.; Berisha, V.; Utianski, R.L.; Liss, J.M.; Spanias, A. Automatic assessment of vowel space area. J. Acoust. Soc. Am. 2013, 134, 477–483. [Google Scholar] [CrossRef] [PubMed]
- Sapir, S.; Ramig, L.O.; Spielman, J.L.; Fox, C. Acoustic metrics of vowel articulation in Parkinson’s disease: Vowel space area (VSA) vs. vowel articulation index (VAI). In MAVEBA: Models and Analysis of Vocal Emissions for Biomedical Applications; Firenze University Press: Florence, Italy, 2011; pp. 173–175. [Google Scholar]
- Mekyska, J.; Rektorova, I.; Smekal, Z. Objective Automatic Assessment of Rehabilitative Speech Treatment in Parkinson’s Disease. In Proceedings of the 34th IEEE International Conference on Telecommunications and Signal Processing, Budapest, Hungary, 18–20 August 2011. [Google Scholar]
- Veltri, P.; Cannataro, M.; Tradigo, G. Sharing mass spectrometry data in a grid-based distributed proteomics laboratory. Inf. Process. Manag. 2007, 43, 577–591. [Google Scholar] [CrossRef]
- Vizza, P.; Curcio, A.; Tradigo, G.; Indolfi, C.; Veltri, P. A framework for the atrial fibrillation prediction in electrophysiological studies. Comput. Methods Progr. Biomed. 2015, 120, 65–76. [Google Scholar] [CrossRef] [PubMed]
- Cannataro, M.; Guzzi, P.H.; Veltri, P. IMPRECO: Distributed prediction of protein complexes. Future Gener. Comput. Syst. 2010, 26, 434–440. [Google Scholar] [CrossRef]
- Dogan, M.; Midi, I.; Yazici, M.A.; Kocak, I.; Günal, D.; Sehitoglu, M.A. Objective and subjective evaluation of voice quality in multiple sclerosis. J. Voice 2007, 21, 735–740. [Google Scholar] [CrossRef] [PubMed]
- Murry, T.; Rosen, C.A. Outcome measurements and quality of life in voice disorders. Otolaryngol. Clin. N. Am. 2000, 33, 905–916. [Google Scholar] [CrossRef]
- Hardcastle, W.J.; Laver, J.; Gibbon, F.E. The Handbook of Phonetic Sciences; John Wiley and Sons: Hoboken, NJ, USA, 2010. [Google Scholar]
- Neuroscience News. Study Shows How the Nanog Protein Promotes Growth of Head and Neck Cancer. 2013. Available online: http://neurosciencenews.com (accessed on 26 November 2017).
- Scott, S.; McGettigan, C. The Voice: From Identity to Interactions. In APA Handbook of Nonverbal Communication; American Psychological Association: Washington, DC, USA, 2015. [Google Scholar]
- Vizza, P.; Mirarchi, D.; Tradigo, G.; Redavide, M.; Bossio, R.; Veltri, P. Vocal signal analysis in patients affected by Multiple Sclerosis. Procedia Comput. Sci. 2017, 108, 1205–1214. [Google Scholar] [CrossRef]
- Zwetsch, I.; Fagundes, R.; Russomano, T.; Scolari, D. Digital signal processing in the differential diagnosis of beningn larynx diseases. Sci. Med. 2006, 16, 109–114. [Google Scholar]
- Harrington, J.; Cassidy, S. Techniques in Speech Acoustics; Springer: Berlin, Germany, 2012. [Google Scholar]
- Williamson, G. Human Communication: A Linguistic Introduction; Speechmark Publishing: Brackley, UK, 2001. [Google Scholar]
- Farrus, M.H.; Ejarque, P. Jitter and Shimmer Measurements for Speaker Recognition. In Interspeech, Proceedings of the 8th Annual Conference of the International Speech Communication Association, Antwerp, Belgium, 27–31 August 2007; International Speech Communication Association (ISCA): Stockholm, Sweden, 2007; pp. 778–781. [Google Scholar]
- Casper, J.K.; Leonard, R. Understanding Voice Problems: A Physiological Perspective for Diagnosis and Treatment; Lippincott Williams and Wilkins: Philadelphia, PA, USA, 2006. [Google Scholar]
- Vorperian, H.K.; Kent, R.D. Vowel acoustic space development in children: A synthesis of acoustic and anatomic data. J. Speech Lang. Hear. Res. 2007, 50, 1510–1545. [Google Scholar] [CrossRef]
- Kewley-Port, D.; Burkle, T.Z.; Lee, J.H. Contribution of consonant versus vowel information to sentence intelligibility for young normal-hearing and elderly hearing-impaired listeners. J. Acoust. Soc. Am. 2007, 122, 2365–2375. [Google Scholar] [CrossRef] [PubMed]
- Sapir, S.; Ramig, L.O.; Spielman, J.L.; Fox, C. Formant centralization ratio: A proposal for a new acoustic measure of dysarthric speech. J. Speech Lang. Hear. Res. 2010, 53, 114–125. [Google Scholar] [CrossRef]
- Liu, H.M.; Tsao, F.M.; Kuhl, P.K. The effect of reduced vowel working space on speech intelligibility in Mandarin-speaking young adults with cerebral palsy. J. Acoust. Soc. Am. 2005, 117, 3879–3889. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| HS | SPMS | RRMS | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Max | Avg | Min | Max | Avg | Min | Max | Avg | Min | |
| (Hz) | |||||||||
| Men | 121.79 | 116.02 | 110.84 | 192.3 | 125.26 | 97.05 | 134.17 | 109.29 | 90.73 |
| Women | 206.03 | 199.64 | 187.61 | 198.04 | 168.01 | 138.46 | 270.26 | 169.63 | 84.57 |
| Jitter (%) | |||||||||
| Men | 0.42 | 0.36 | 0.29 | 1.83 | 0.7 | 0.19 | 4.57 | 0.79 | 0.21 |
| Women | 0.4 | 0.32 | 0.21 | 3.83 | 0.82 | 0.12 | 2.99 | 0.5 | 0.08 |
| Shimmer (%) | |||||||||
| Men | 15.16 | 8.46 | 3.98 | 13.54 | 8.7 | 4.67 | 22.06 | 8.13 | 2.31 |
| Women | 8.06 | 5.81 | 4.63 | 16 | 8 | 2 | 16.51 | 6.73 | 2.94 |
| Harmonic Noise Ratio (dB) | |||||||||
| Men | 20.25 | 13.44 | 9.6 | 18.15 | 14.29 | 11.23 | 21.01 | 14.39 | 4.25 |
| Women | 18.26 | 16.71 | 13.09 | 27.64 | 17.42 | 7.31 | 26.16 | 16.98 | 6.71 |
| Metric | HS | SPMS | RRMS |
|---|---|---|---|
| tVSA | 579.8 | 673.45 | 97.45 |
| qVSA | 674.23 | 525.89 | 108.56 |
| FCR | 1.95 | 1.96 | 1.98 |
| Parameter | Subjects | Number | Mean | Standard Deviation | p-Value |
|---|---|---|---|---|---|
| HS | 7 | 165.08 | 51.4 | 0.97 | |
| MS | 55 | 179.9 | 25.7 | ||
| Harmonic Noise Ratio | HS | 7 | 0.035 | 0.047 | 0.47 |
| MS | 55 | 0.057 | 0.069 | ||
| Jitter | HS | 7 | 0.341 | 0.0007 | 0.379 |
| MS | 55 | 0.65 | 0.0085 | ||
| Shimmer | HS | 7 | 6.9 | 0.3 | 0.027 |
| MS | 55 | 8.07 | 0.04 |
| Parameter | Subjects | Number | Mean | SD | p-Value |
|---|---|---|---|---|---|
| HS | 7 | 165.08 | 51.4 | 0.499 | |
| MS | 55 | 156.01 | 33.5 | ||
| Harmonic Noise Ratio | HS | 7 | 0.035 | 0.047 | 0.86 |
| MS | 55 | 0.05 | 0.069 | ||
| Jitter | HS | 7 | 0.26 | 0.71 | 0.04 |
| MS | 55 | 0.80 | 1.65 | ||
| Shimmer | HS | 7 | 5.89 | 3.64 | 0.31 |
| MS | 55 | 6.62 | 3.92 |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vizza, P.; Tradigo, G.; Mirarchi, D.; Bossio, R.B.; Veltri, P. On the Use of Voice Signals for Studying Sclerosis Disease. Computers 2017, 6, 30. https://doi.org/10.3390/computers6040030
Vizza P, Tradigo G, Mirarchi D, Bossio RB, Veltri P. On the Use of Voice Signals for Studying Sclerosis Disease. Computers. 2017; 6(4):30. https://doi.org/10.3390/computers6040030
Chicago/Turabian StyleVizza, Patrizia, Giuseppe Tradigo, Domenico Mirarchi, Roberto Bruno Bossio, and Pierangelo Veltri. 2017. "On the Use of Voice Signals for Studying Sclerosis Disease" Computers 6, no. 4: 30. https://doi.org/10.3390/computers6040030
APA StyleVizza, P., Tradigo, G., Mirarchi, D., Bossio, R. B., & Veltri, P. (2017). On the Use of Voice Signals for Studying Sclerosis Disease. Computers, 6(4), 30. https://doi.org/10.3390/computers6040030