Cobalt–Chromium Dental Alloys: Metal Exposures, Toxicological Risks, CMR Classification, and EU Regulatory Framework



Abstract
:
1. Introduction
2. Co–Cr Dental Alloys: Metal Ions and Wear Particles Release
2.1. Corrosion and Metal Ions Release
2.2. Wear of Dental Materials
- (1)
- Mean primary particle size by volume was 35 nm (under normal wear, range = 9–152 nm) and 95 nm (under edge-loading conditions, range = 6–573 nm).
- (2)
- Hydrodynamic diameter analysis by volume gave mixed results, namely particles from normal wear ranged from nano- (<100 nm) to submicron (<1000 nm) in size; from edge-loading conditions, the size range of particles was comprised between <100 nm and up to 3000–6000 nm.
- (3)
- The nature of the isolated particles also varied according to the study conditions, the vast majority of particles under normal use was Cr (98.5%).
- (4)
- Under edge-loading conditions, wear particles contained more Co (≈640-fold) than Cr.
2.3. Toolbox to Detect Metals
3. Toxicological Risks of Co–Cr Dental Alloys
3.1. Recent Toxicological Studies
3.2. Carcinogenicity, Mutagenicity and Toxicity for Reproduction of Co and Cr Metals
3.3. Year 2017, a Pivotal Year for Co–Cr Dental Alloys
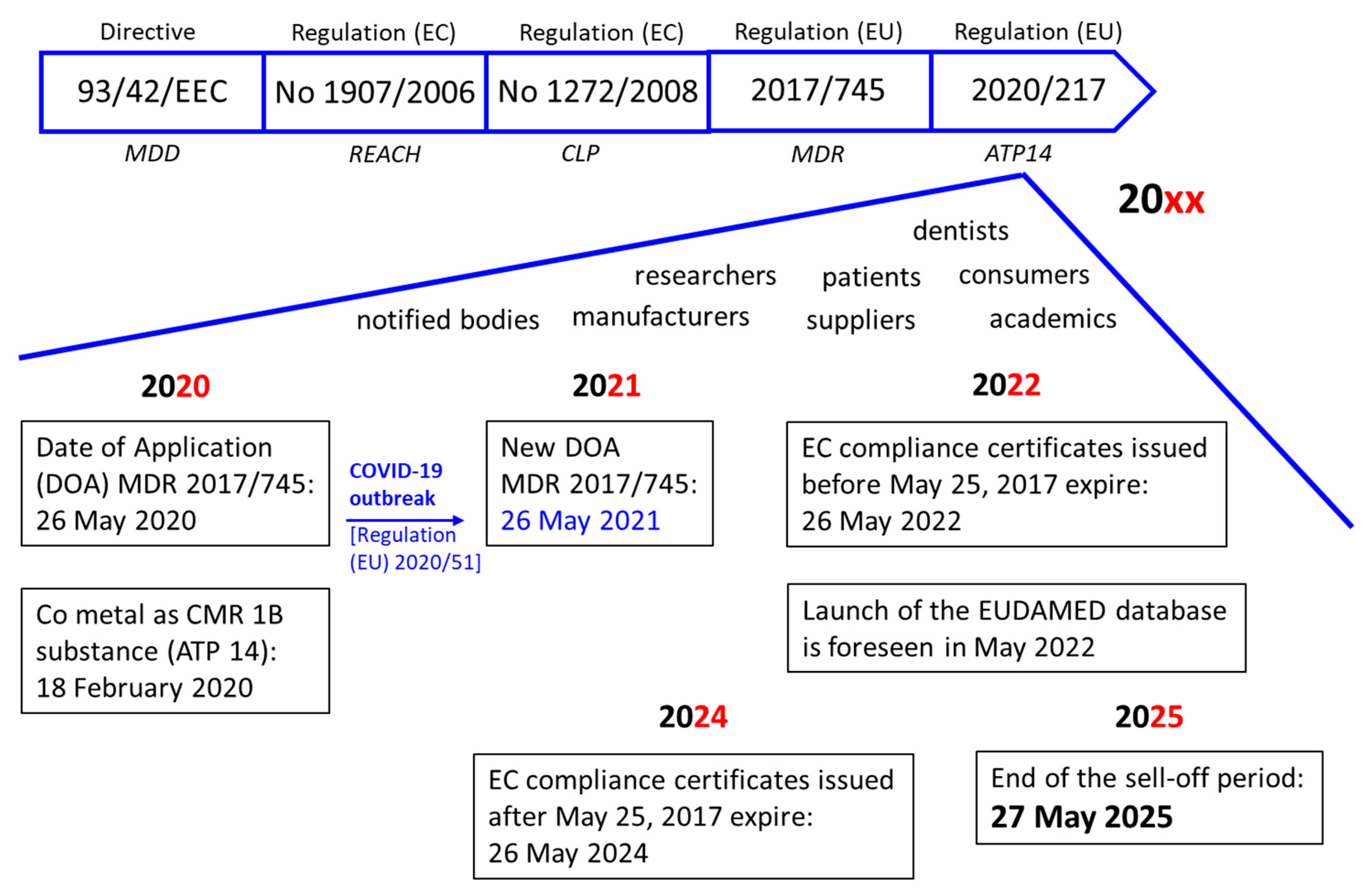
4. European Union (EU) Regulatory Framework
4.1. Medical Device Regulatory Requirements—Period 1990–2020
4.2. Chemicals Legislation—Period 2007–2020
4.3. Co-Existence and Grace Period 2017–2025
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Marti, A. Cobalt-base alloys used in bone surgery. Injury 2000, 31, D18–D21. [Google Scholar] [CrossRef]
- Al Jabbari, Y.S. Physico-mechanical properties and prosthodontic applications of Co–Cr dental alloys: A review of the literature. J. Adv. Prosthodont. 2014, 6, 138–145. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Iglesias, J.F.; Roffi, M.; Degrauwe, S.; Secco, G.G.; Aminian, A.; Windecker, S.; Pilgrim, T. Orsiro cobalt-chromium sirolimus-eluting stent: Present and future perspectives. Expert Rev. Med. Devices 2017, 14, 773–788. [Google Scholar] [CrossRef] [PubMed]
- Gherbesi, E.; Natalini, G. The Ultimaster coronary stent system: 5-year worldwide experience. Future Cardiol. 2020, 16, 251–261. [Google Scholar] [CrossRef]
- Louwerens, J.K.; Hockers, N.; Achten, G.; Sierevelt, I.N.; Nolte, P.A.; Van Hove, R.P. No clinical difference between TiN-coated versus uncoated cementless CoCrMo mobile-bearing total knee arthroplasty; 10-year follow-up of a randomized controlled trial. Knee Surg. Sports Traumatol. Arthrosc. 2020, 1–7. [Google Scholar] [CrossRef]
- Liu, G.; Wang, X.; Zhou, X.; Zhang, L.; Mi, J.; Shan, Z.; Huang, B.; Chen, Z.; Chen, Z. Modulating the cobalt dose range to manipulate multisystem cooperation in bone environment: A strategy to resolve the controversies about cobalt use for orthopedic applications. Theranostics 2020, 10, 1074–1089. [Google Scholar] [CrossRef]
- Buser, D.; Sennerby, L.; De Bruyn, H. Modern implant dentistry based on osseointegration: 50 years of progress, current trends and open questions. Periodontology 2000 2017, 73, 7–21. [Google Scholar] [CrossRef]
- Lee, B.W.; Alsenz, R.; Ignatiev, A.; Van Hove, M.A. Surface structures of the two allotropic phases of cobalt. Phys. Rev. B 1978, 17, 1510–1520. [Google Scholar] [CrossRef]
- Lin, W.-C.; Chuang, C.; Yao, C.; Tang, C.-M. Effect of cobalt precursors on cobalt-hydroxyapatite used in bone regeneration and MRI. J. Dent. Res. 2020, 99, 277–284. [Google Scholar] [CrossRef]
- Scharf, B.; Clement, C.C.; Zolla, V.; Perino, G.; Yan, B.; Elci, S.G.; Purdue, E.; Goldring, S.R.; Macaluso, F.; Cobelli, N.; et al. Molecular analysis of chromium and cobalt-related toxicity. Sci. Rep. 2015, 4, 5729. [Google Scholar] [CrossRef] [Green Version]
- Anderson, R.A. Chromium as an essential nutrient for humans. Regul. Toxicol. Pharmacol. 1997, 26, S35–S41. [Google Scholar] [CrossRef] [Green Version]
- McGregor, D.; Baan, R.; Partensky, C.; Rice, J.; Wilbourn, J. Evaluation of the carcinogenic risks to humans associated with surgical implants and other foreign bodies—A report of an IARC monographs programme meeting. Eur. J. Cancer 2000, 36, 307–313. [Google Scholar] [CrossRef]
- Meek, R.D.; Afolaranmi, G.A.; Tettey, J.; Grant, M.H. Release of chromium from orthopaedic arthroplasties. Open Orthop. J. 2008, 2, 10–18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Overview on the Medical Devices Legislation in the EU. Available online: https://www.ema.europa.eu/en/human-regulatory/overview/medical-devices#medical-devices-legislation-section (accessed on 21 November 2020).
- Hussein, M.A.; Mohammed, A.S.; Al-Aqeeli, N. Wear characteristics of metallic biomaterials: A review. Materials 2015, 8, 2749–2768. [Google Scholar] [CrossRef]
- Chitra, P.; Prashantha, G.S.; Rao, A. Long-term evaluation of metal ion release in orthodontic patients using fluoridated oral hygiene agents: An in vivo study. J. World Fed. Orthod. 2019, 8, 107–111. [Google Scholar] [CrossRef]
- Mikulewicz, M.; Chojnacka, K.; Woźniak, B.; Downarowicz, P. Release of metal ions from orthodontic appliances: An in vitro study. Biol. Trace Elem. Res. 2011, 146, 272–280. [Google Scholar] [CrossRef] [Green Version]
- De Aguiar, S.R.M.M.; Nicolai, M.; Almeida, M.; Gomes, A. Electrochemical behaviour of a cobalt–chromium–molybdenum dental alloy in artificial salivas. Bio-Med. Mater. Eng. 2015, 25, 53–66. [Google Scholar] [CrossRef]
- Gibon, E.; Amanatullah, D.F.; Loi, F.; Pajarinen, J.; Nabeshima, A.; Yao, Z.; Hamadouche, M.; Goodman, S.B. The biological response to orthopaedic implants for joint replacement: Part I: Metals. J. Biomed. Mater. Res. Part B Appl. Biomater. 2017, 105, 2162–2173. [Google Scholar] [CrossRef]
- Forssten, S.D.; Björklund, M.; Ouwehand, A.C. Streptococcus mutans, caries and simulation models. Nutrition 2010, 2, 290–298. [Google Scholar] [CrossRef] [Green Version]
- Upadhyay, D.; Panchal, M.A.; Dubey, R.; Srivastava, V. Corrosion of alloys used in dentistry: A review. Mater. Sci. Eng. A 2006, 432, 1–11. [Google Scholar] [CrossRef]
- Ciszewski, A.; Baraniak, M.; Urbanekbrychczynska, M. Corrosion by galvanic coupling between amalgam and different chromium-based alloys. Dent. Mater. 2007, 23, 1256–1261. [Google Scholar] [CrossRef]
- Liu, Y.; Chen, B. In vivo corrosion of CoCrMo alloy and biological responses: A review. Mater. Technol. 2018, 33, 127–134. [Google Scholar] [CrossRef]
- Mercieca, S.; Conti, M.C.; Buhagiar, J.; Camilleri, J. Assessment of corrosion resistance of cast cobalt- and nickel-chromium dental alloys in acidic environments. J. Appl. Biomater. Funct. Mater. 2017, 16, 47–54. [Google Scholar] [CrossRef] [Green Version]
- IARC Monographs on the Evaluation of Carcinogenic Risks to Humans. Chromium, Nickel and Welding. Volume 49. Available online: https://publications.iarc.fr/67 (accessed on 27 September 2020).
- Uggowitzer, P.J.; Magdowski, R.; Speidel, M.O. High nitrogen steels. Nickel free high nitrogen austenitic steels. ISIJ Int. 1996, 36, 901–908. [Google Scholar] [CrossRef] [Green Version]
- Posada, O.M.; Gilmour, D.; Tate, R.J.; Grant, M.H. CoCr wear particles generated from CoCr alloy metal-on-metal hip replacements, and cobalt ions stimulate apoptosis and expression of general toxicology-related genes in monocyte-like U937 cells. Toxicol. Appl. Pharmacol. 2014, 281, 125–135. [Google Scholar] [CrossRef] [Green Version]
- Madl, A.K.; Kovochich, M.; Liong, M.; Finley, B.L.; Paustenbach, D.J.; Oberdörster, G. Toxicology of wear particles of cobalt-chromium alloy metal-on-metal hip implants Part II: Importance of physicochemical properties and dose in animal and in vitro studies as a basis for risk assessment. Nanomedicine 2015, 11, 1285–1298. [Google Scholar] [CrossRef]
- Kovochich, M.; Finley, B.L.; Novick, R.; Monnot, A.D.; Donovan, E.; Unice, K.; Fung, E.S.; Fung, D.; Paustenbach, D.J. Understanding outcomes and toxicological aspects of second generation metal-on-metal hip implants: A state-of-the-art review. Crit. Rev. Toxicol. 2018, 48, 839–887. [Google Scholar] [CrossRef]
- Cuiabc, G.; Liu, H.; Li, S.; Gao, G.; Hassani, M.; Kou, Z. Effect of Ni, W and Mo on the microstructure, phases and high-temperature sliding wear performance of CoCr matrix alloys. Sci. Technol. Adv. Mater. 2020, 21, 229–241. [Google Scholar] [CrossRef] [Green Version]
- Heintze, S.D.; Reichl, F.-X.; Hickel, R. Wear of dental materials: Clinical significance and laboratory wear simulation methods -A review. Dent. Mater. J. 2019, 38, 343–353. [Google Scholar] [CrossRef] [Green Version]
- Kovochich, M.; Fung, E.S.; Donovan, E.; Unice, K.M.; Paustenbach, D.J.; Finley, B.L. Characterization of wear debris from metal-on-metal hip implants during normal wear versus edge-loading conditions. J. Biomed. Mater. Res. Part B Appl. Biomater. 2018, 106, 986–996. [Google Scholar] [CrossRef]
- Di Laura, A.; Quinn, P.D.; Panagiotopoulou, V.C.; Hothi, H.S.; Henckel, J.; Powell, J.J.; Berisha, F.; Amary, F.; Mosselmans, J.F.W.; Skinner, J.A.; et al. The chemical form of metal species released from corroded taper junctions of hip implants: Synchrotron analysis of patient tissue. Sci. Rep. 2017, 7, 10952. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Crothers, A. Tooth wear and facial morphology. J. Dent. 1992, 20, 333–341. [Google Scholar] [CrossRef]
- Hsu, H.C.; Yen, S.-K. Evaluation of metal ion release and corrosion resistance of ZrO2 thin coatings on the dental Co–Cr alloys. Dent. Mater. 1998, 14, 339–346. [Google Scholar] [CrossRef]
- Lucchetti, M.C.; Fratto, G.; Valeriani, F.; De Vittori, E.; Giampaoli, S.; Papetti, P.; Spica, V.R.; Manzon, L. Cobalt-chromium alloys in dentistry: An evaluation of metal ion release. J. Prosthet. Dent. 2015, 114, 602–608. [Google Scholar] [CrossRef]
- Haugli, K.H.; Syverud, M.; Samuelsen, J.T. Ion release from three different dental alloys—Effect of dynamic loading and toxicity of released elements. Biomater. Investig. Dent. 2020, 7, 71–79. [Google Scholar] [CrossRef]
- Tuna, S.H.; Karaca, E.; Aslan, I.; Pekkan, G.; Pekmez, N. Özçiçek Evaluation of corrosion resistance of Co–Cr alloys fabricated with different metal laser sintering systems. J. Adv. Prosthodont. 2020, 12, 114–123. [Google Scholar] [CrossRef]
- Ramirez-Ledesma, A.L.; Barrera, P.R.; Álvarez-Pérez, M.A.; Lopez, H.; Juárez-Islas, J.A. Corrosion assessment of an implantable dental Co–Cr alloy in artificial saliva and biocompatibility behavior. J. Mater. Eng. Perform. 2020, 29, 1657–1670. [Google Scholar] [CrossRef]
- Kassapidou, M.; Hjalmarsson, L.; Johansson, C.B.; Johansson, P.H.; Morisbak, E.; Wennerberg, A.; Stenport, V.F. Cobalt–chromium alloys fabricated with four different techniques: Ion release, toxicity of released elements and surface roughness. Dent. Mater. 2020, 36, e352–e363. [Google Scholar] [CrossRef]
- Kim, T.-W.; Kim, W.-I.; Mun, J.-H.; Song, M.; Kim, H.-S.; Kim, B.-S.; Kim, M.-B.; Ko, H.C. Patch Testing with dental screening series in oral disease. Ann. Dermatol. 2015, 27, 389–393. [Google Scholar] [CrossRef] [Green Version]
- Kettelarij, J.A.B.; Lidén, C.; Axén, E.; Julander, A. Cobalt, nickel and chromium release from dental tools and alloys. Contact Dermat. 2013, 70, 3–10. [Google Scholar] [CrossRef]
- Kettelarij, J.A.B.; Nilsson, S.; Midander, K.; Lidén, C.; Julander, A. Snapshot of cobalt, chromium and nickel exposure in dental technicians. Contact Dermat. 2016, 75, 370–376. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maruyama, N.; Kawasaki, H.; Yamamoto, A.; Hiromoto, S.; Imai, H.; Hanawa, T. Friction-wear properties of nickel-free Co–Cr–Mo alloy in a simulated body fluid. Mater. Trans. 2005, 46, 1588–1592. [Google Scholar] [CrossRef] [Green Version]
- Lewis, R.; Dwyer-Joyce, R.S. Wear of human teeth: A tribological perspective. Proc. Inst. Mech. Eng. Part J J. Eng. Tribol. 2005, 219, 2–19. [Google Scholar] [CrossRef]
- Pourzal, R.; Catelas, I.; Theissmann, R.; Kaddick, C.; Fischer, A. Characterization of wear particles generated from CoCrMo alloy under sliding wear conditions. Wear 2011, 271, 1658–1666. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koronfel, M.A.; Goode, A.E.; Weker, J.N.; Tay, S.E.R.; Stitt, C.A.; Simões, T.A.; Mosselmans, J.F.W.; Quinn, P.; Brydson, R.; Hart, A.J.; et al. Understanding the reactivity of CoCrMo-implant wear particles. NPJ Mater. Degrad. 2018, 2, 8. [Google Scholar] [CrossRef] [Green Version]
- Addy, M.; Hughes, J.; Pickles, M.J.; Joiner, A.; Huntington, E. Development of a method in situ to study toothpaste abrasion of dentine. J. Clin. Periodontol. 2002, 29, 896–900. [Google Scholar] [CrossRef] [PubMed]
- Vaicelyte, A.; Janssen, C.; Le Borgne, M.; Grosgogeat, B. Toxicological risks of the cobalt—Chromium alloys used in dentistry: A systematic review. J. Dent. 2020. in preparation. [Google Scholar]
- Chitturi, R.; Baddam, V.R.; Prasad, L.; Prashanth, L.; Kattapagari, K. A review on role of essential trace elements in health and disease. J. Dr. NTR Univ. Health Sci. 2015, 4, 75. [Google Scholar] [CrossRef]
- Han, X.; Sawada, T.; Schille, C.; Schweizer, E.; Scheideler, L.; Geis-Gerstorfer, J.; Rupp, F.; Spintzyk, S. Comparative analysis of mechanical properties and metal-ceramic bond strength of Co–Cr dental alloy fabricated by different manufacturing processes. Materials 2018, 11, 1801. [Google Scholar] [CrossRef] [Green Version]
- Kassapidou, M.; Stenport, V.F.; Hjalmarsson, L.; Johansson, C.B. Cobalt-chromium alloys in fixed prosthodontics in Sweden. Acta Biomater. Odontol. Scand. 2017, 3, 53–62. [Google Scholar] [CrossRef]
- Julander, A.; Hindsén, M.; Skare, L.; Lidén, C. Cobalt-containing alloys and their ability to release cobalt and cause dermatitis. Contact Dermat. 2009, 60, 165–170. [Google Scholar] [CrossRef] [PubMed]
- Ebadian, B.; Razavi, M.; Soleimanpour, S.; Mosharraf, R. Evaluation of tissue reaction to some denture-base materials: An animal study. J. Contemp. Dent. Pract. 2008, 9, 67–74. [Google Scholar] [CrossRef]
- Thyssen, J.; Menné, T.; Møller, P.; Jellesen, M.S.; Johansen, J.D. A cobalt spot test was useful in the diagnostic work-up of a cobalt allergic patient suffering from oral hypersensitivity to cobalt. J. Am. Acad. Dermatol. 2011, 65, 659–660. [Google Scholar] [CrossRef] [PubMed]
- Song, H.; Yin, W.; Ma, Q. Allergic palmoplantar pustulosis caused by cobalt in cast dental crowns: A case report. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2011, 111, e8–e10. [Google Scholar] [CrossRef] [PubMed]
- Arafa, K.A. Comparing the effects of titanium alloy and chrome cobalt in removable partial denture connectors on tooth mobility, bone loss and tissue reaction. Saudi J. Dent. Res. 2016, 7, 112–117. [Google Scholar] [CrossRef] [Green Version]
- Linauskienė, K.; Malinauskienė, L.; Blažienė, A. Metals are important contact sensitizers: An experience from Lithuania. BioMed Res. Int. 2017, 2017, 3964045. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Al-Imam, H.; Benetti, A.R.; Øzhayat, E.B.; Pedersen, A.M.L.; Johansen, J.D.; Thyssen, J.; Jellesen, M.S.; Gotfredsen, K. Cobalt release and complications resulting from the use of dental prostheses. Contact Dermat. 2016, 75, 377–383. [Google Scholar] [CrossRef]
- Olms, C.; Yahiaoui-Doktor, M.; Remmerbach, T.W. Contact allergies to dental materials. Swiss Dent. J. 2019, 129, 571–579. [Google Scholar]
- Drynda, A.; Drynda, S.; Kekow, J.; Lohmann, C.H.; Bertrand, J. Differential effect of cobalt and chromium ions as well as CoCr particles on the expression of osteogenic markers and osteoblast function. Int. J. Mol. Sci. 2018, 19, 3034. [Google Scholar] [CrossRef] [Green Version]
- IARC Monographs. Available online: https://monographs.iarc.fr/cards_page/publications-monographs/ (accessed on 16 August 2020).
- National Toxicology Program. Available online: https://ntp.niehs.nih.gov/pubhealth/roc/index-1.html (accessed on 16 August 2020).
- Suh, M.; Wikoff, D.; Lipworth, L.; Goodman, M.; Fitch, S.; Mittal, L.; Ring, C.; Proctor, D. Hexavalent chromium and stomach cancer: A systematic review and meta-analysis. Crit. Rev. Toxicol. 2019, 49, 140–159. [Google Scholar] [CrossRef] [Green Version]
- Christian, W.V.; Oliver, L.D.; Paustenbach, D.J.; Kreider, M.L.; Finley, B.L. Toxicology-based cancer causation analysis of CoCr-containing hip implants: A quantitative assessment of genotoxicity and tumorigenicity studies. J. Appl. Toxicol. 2014, 34, 939–967. [Google Scholar] [CrossRef]
- Biological Responses to Metal Implants. FDA Report Published on September 2019. Available online: https://www.fda.gov/media/132446/download (accessed on 28 August 2020).
- Leonard, A.; Lauwerys, R. Carcinogenicity and mutagenicity of chromium. Mutat. Res. Genet. Toxicol. 1980, 76, 227–239. [Google Scholar] [CrossRef]
- Léonard, A.; Lauwerys, R. Mutagenicity, carcinogenicity and teratogenicity of cobalt metal and cobalt compounds. Mutat. Res. Genet. Toxicol. 1990, 239, 17–27. [Google Scholar] [CrossRef]
- Rusu, L.C.; Bortun, C.M.; Tănăsie, G.; Podariu, A.C.; Baderca, F.; Solovan, C.; Ardelean, L. The cytotoxicity of dental alloys studied on cell culture. Rom. J. Morphol. Embryol. 2014, 55, 111–115. [Google Scholar]
- Yan, T. The study of cytocompatibility of Co–Cr alloy and Ti alloy. Tianjin Med. J. 2015, 43, 526–528. [Google Scholar] [CrossRef]
- Fernández-Miñano, E.; Ortiz, C.; Vicente, A.; Calvo, J.L.; Ortiz, A.J. Metallic ion content and damage to the DNA in oral mucosa cells of children with fixed orthodontic appliances. BioMetals 2011, 24, 935–941. [Google Scholar] [CrossRef]
- Annangi, B.; Bonassi, S.; Marcos, R.; Hernández, A. Biomonitoring of humans exposed to arsenic, chromium, nickel, vanadium, and complex mixtures of metals by using the micronucleus test in lymphocytes. Mutat. Res. Mutat. Res. 2016, 770, 140–161. [Google Scholar] [CrossRef]
- RAC Opinion on Cobalt. ECHA Document Published on 22 September 2017. Available online: https://echa.europa.eu/documents/10162/b7316b11-ae65-1dd0-2e64-bb6ad3efbd82 (accessed on 28 August 2020).
- Regulation (EU) 2017/745 of the European Parliament and of the Council of 5 April 2017 on Medical Devices. Available online: http://data.europa.eu/eli/reg/2017/745/oj (accessed on 11 November 2020).
- Cogliano, V.J.; Baan, R.; Straif, K.; Grosse, Y.; Lauby-Secretan, B.; El Ghissassi, F.; Bouvard, V.; Benbrahim-Tallaa, L.; Guha, N.; Freeman, C.; et al. Preventable exposures associated with human cancers. J. Natl. Cancer Inst. 2011, 103, 1827–1839. [Google Scholar] [CrossRef]
- Council Directive 93/42/EEC of 14 June 1993 Concerning Medical Devices. Available online: http://data.europa.eu/eli/dir/1993/42/oj (accessed on 11 November 2020).
- Regulation (EU) 2020/561 of the European Parliament and of the Council of 23 April 2020. Available online: http://data.europa.eu/eli/reg/2020/561/oj (accessed on 11 November 2020).
- Commission Implementing Regulation (EU) 2017/2185 of 23 November 2017. Available online: http://data.europa.eu/eli/reg_impl/2017/2185/oj (accessed on 11 November 2020).
- Regulation (EC) No 1907/2006 of 18 December 2006 Concerning the Registration, Evaluation, Authorisation and Restriction of Chemicals (REACH). Available online: http://data.europa.eu/eli/reg/2006/1907/2014-04-10 (accessed on 11 November 2020).
- Regulation (EC) No 1272/2008 of the European Parliament and of the Council of 16 December 2008 on Classification, Labelling and Packaging of Substances and Mixtures. Available online: http://data.europa.eu/eli/reg/2008/1272/oj (accessed on 15 November 2020).
- Registered Substances ECHA. Available online: https://echa.europa.eu/information-on-chemicals/registered-substances (accessed on 15 November 2020).
- Table of Harmonised Entries in annex VI to CLP. Available online: https://echa.europa.eu/documents/10162/13626/annex_vi_clp_table_atp14_en.xlsx/c767afd2-4d53-b8d5-de2b-0820680cac95 (accessed on 15 November 2020).
- Sonofuchi, K.; Hagiwara, Y.; Koizumi, Y.; Chiba, A.; Kawano, M.; Nakayama, M.; Ogasawara, K.; Yabe, Y.; Itoi, E. Quantitative in vivo biocompatibility of new ultralow-nickel cobalt-chromium-molybdenum alloys. J. Orthop. Res. 2016, 34, 1505–1513. [Google Scholar] [CrossRef]
- Mertová, K.; Palán, J.; Németh, G.; Fintová, S.; Duchek, M.; Studecký, T.; Veselý, J.; Máthis, K.; Džugan, J.; Trojanová, Z. Optimization of the mechanical performance of titanium for biomedical applications by advanced, high-gain SPD technology. Crystals 2020, 10, 422. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Type | Trademark Mfr. 1 (Country) | Composition (Mass%) | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Co | Cr | Mo | Si 2 | Mn 2 | C 2 | Fe | W | Other | ||
| Alloys for removable partial denture | Wironit® extrahart Bego (Germany) | 63.0 | 30.0 | 5.0 | 1.0 | 1.0 | <1.0 | |||
| Remanium® GM 800+ Dentaurum (Germany) | 58.3 | 32.0 | 6.5 | 1.0 | <1.0 | 1.5 | N 2 < 1.0 | |||
| Orthodontic wires | Alloy CoCr 3.002 Dentaurum (Germany) | 31.0–35.0 | 28.0–32.0 | 4.0–6.0 | ≤0.1 | ≤0.1 | ≤0.35 | 27.0–31.0 | ||
| Remaloy® Dentaurum (Germany) | rest | 18.0–22.0 | 3.0–5.0 | ≤0.5 | ≤1.0 | ≤0.03 | 4.0–6.0 | 3.0–5.0 | Ni 19–23 Ti 2 0.1–2 S 2 ≤ 0.1 | |
| Alloys for fixed prostheses | CoCr Biostar ERNST HINRICHS Dental (Germany) | 61.65 | 27.75 | 1.61 | <1.0 | <1.0 | 8.45 | |||
| Vi-comp II® Dentsply Sirona (USA) | 52.5 | 27.4 | <1.0 | 1.0 | 12.1 | Ga 2.5 Ru 2.4 Cu 2 1.0 Nb 2 < 1.0 Ta 2 < 1.0 | ||||
| Metal Ions Release and Corrosion | Methods and Techniques | Remarks |
|---|---|---|
| Testing methods | alloys shaped into discs/cylinders and polished static immersion test (chemical corrosion) | variation of parameters: artificial saliva solution, presence or absence of bacteria (e.g., Eikenella corrodens), pH, time, altered conditions, etc. |
| dynamic immersion test (biocorrosion) | ||
| Release of ions | atomic absorption spectroscopy (AAS) electrochemical impedance spectroscopy (EIS) inductively coupled plasma optical emission spectrometry (ICP-OES) | to identify released elements, to determine ion concentrations |
| inductively coupled plasma mass spectrometry (ICP–MS) | ||
| polarization test by potentiostat | ||
| Characterization techniques | energy dispersive spectroscopy (EDS) optical interferometry scanning electron microscopy (SEM) | to compare the corrosion resistance, to evaluate porosity, to analyze surface topography |
| X-ray diffraction (XRD) |
| Wear of Metallic Biomaterials | Methods and Techniques | Remarks |
|---|---|---|
| Testing methods | alloys shaped into discs/cylinders and polished ball and crater, ball-on-disc block-on-disc one-way slide and static end load | variation of parameters: temperature, magnitude of biting force, simulated body fluids, etc. |
| pin-on-disc, pin-on-flat | ||
| Surface roughness | optical profilometer 3D-profilometer | to test the cross-sectional profile, to calculate the wear volume |
| atomic force microscope (AFM) | ||
| X-ray photoelectron spectroscopy (XPS) | ||
| Characterization techniques | energy dispersive spectroscopy (EDS) scanning electron microscopy (SEM) transmission electron microscopy (TEM) | for particles and/or surface |
| X-ray absorption spectroscopy (XRAS) | ||
| X-ray diffraction (XRD) |
| Element | Total Average Quantity (g) | Daily Requirement (mg/day) |
|---|---|---|
| Co | 1.1 | 0.0001 |
| Cr | 0.006 | 0.0050 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vaicelyte, A.; Janssen, C.; Le Borgne, M.; Grosgogeat, B. Cobalt–Chromium Dental Alloys: Metal Exposures, Toxicological Risks, CMR Classification, and EU Regulatory Framework. Crystals 2020, 10, 1151. https://doi.org/10.3390/cryst10121151
Vaicelyte A, Janssen C, Le Borgne M, Grosgogeat B. Cobalt–Chromium Dental Alloys: Metal Exposures, Toxicological Risks, CMR Classification, and EU Regulatory Framework. Crystals. 2020; 10(12):1151. https://doi.org/10.3390/cryst10121151
Chicago/Turabian StyleVaicelyte, Alina, Christine Janssen, Marc Le Borgne, and Brigitte Grosgogeat. 2020. "Cobalt–Chromium Dental Alloys: Metal Exposures, Toxicological Risks, CMR Classification, and EU Regulatory Framework" Crystals 10, no. 12: 1151. https://doi.org/10.3390/cryst10121151
APA StyleVaicelyte, A., Janssen, C., Le Borgne, M., & Grosgogeat, B. (2020). Cobalt–Chromium Dental Alloys: Metal Exposures, Toxicological Risks, CMR Classification, and EU Regulatory Framework. Crystals, 10(12), 1151. https://doi.org/10.3390/cryst10121151