Development of Poly(HEMA-Am) Polymer Hydrogel Filler for Soft Tissue Reconstruction by Facile Polymerization

 , , and
, , and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Materials
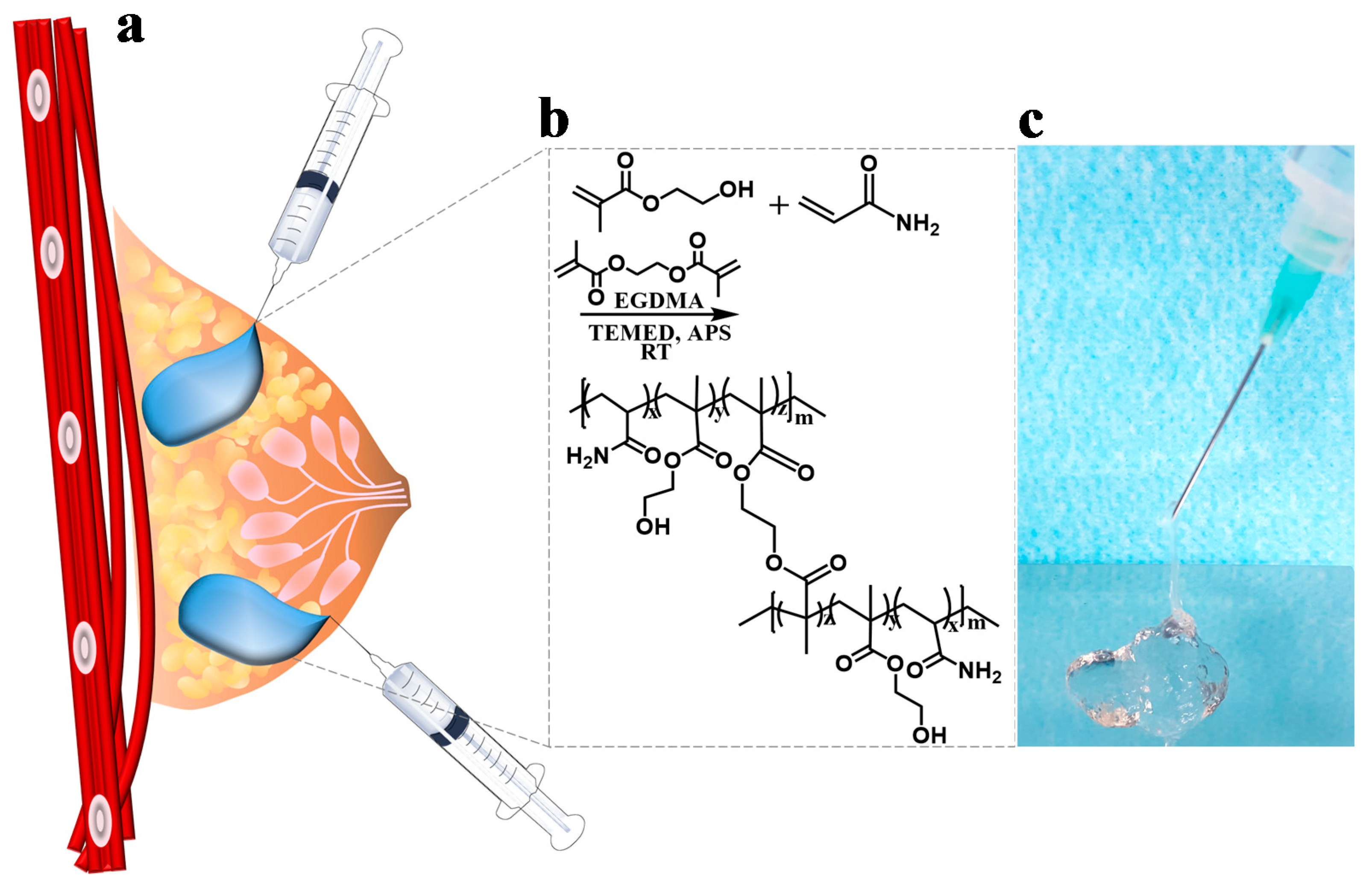
2.2. Synthesis of the Poly(HEMA-Am)
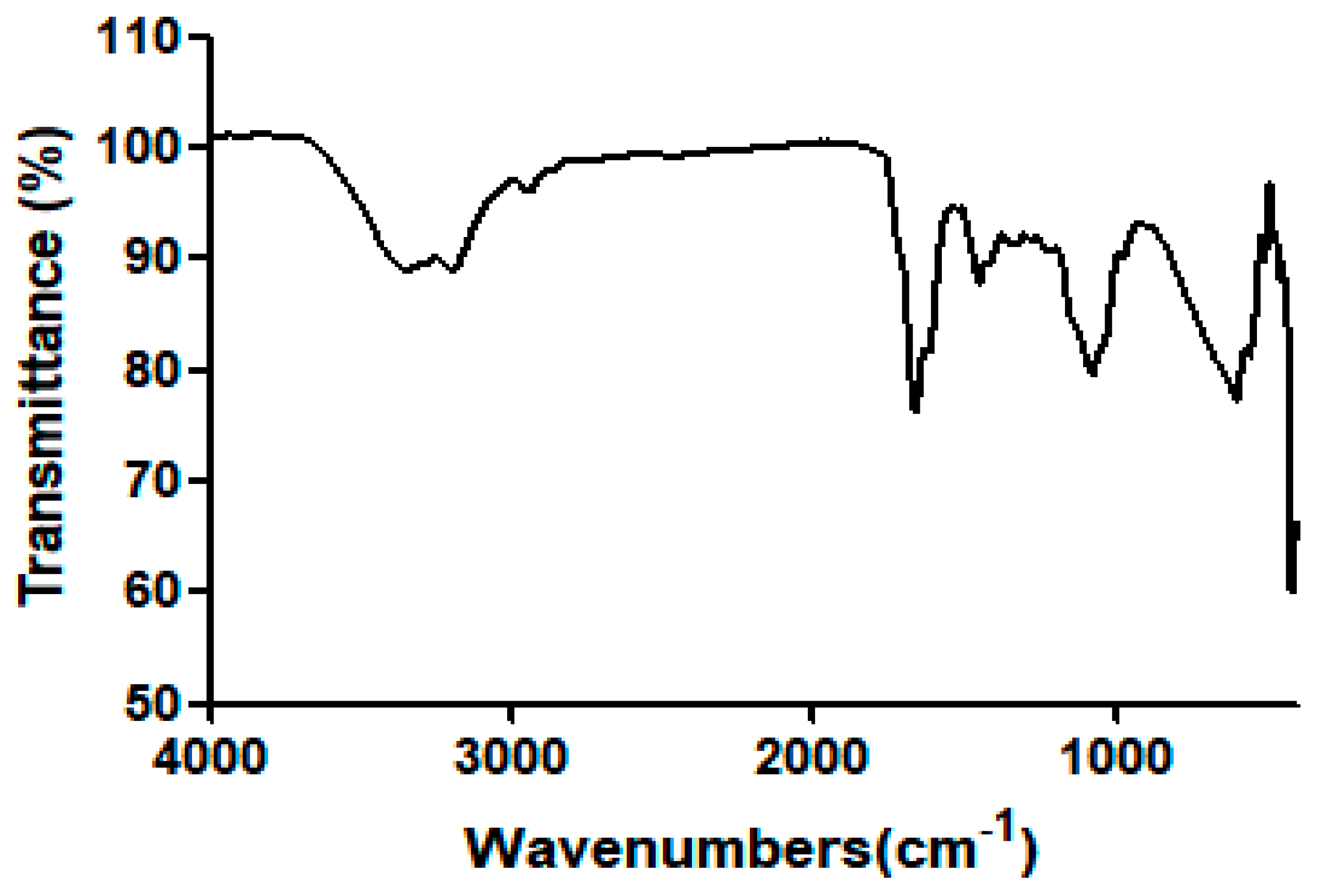
2.3. Fourier Transform Infrared Spectroscopy (FT-IR) of the Poly(HEMA-Am)
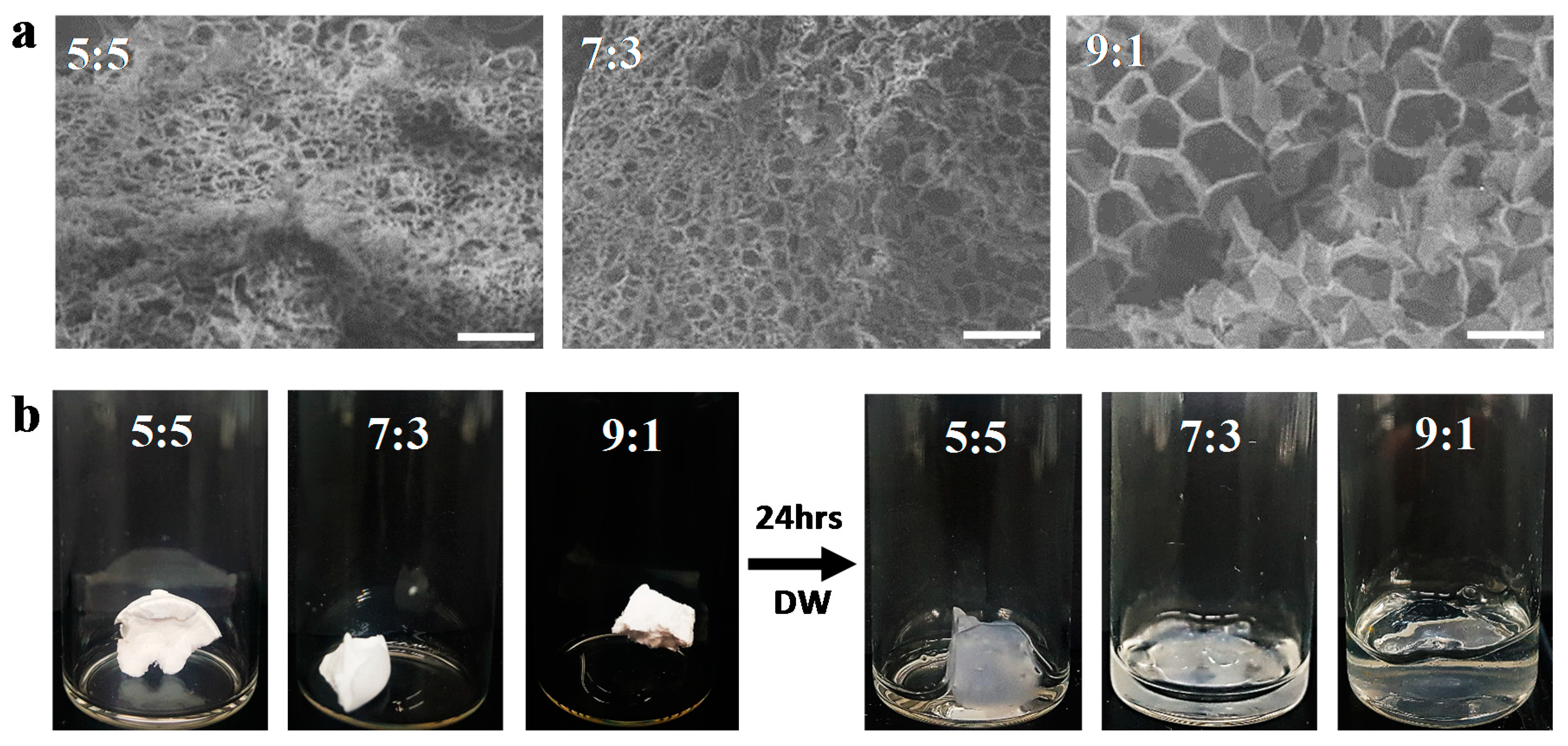
2.4. Scanning Electron Microscopy (SEM) of the Poly(HEMA-Am)
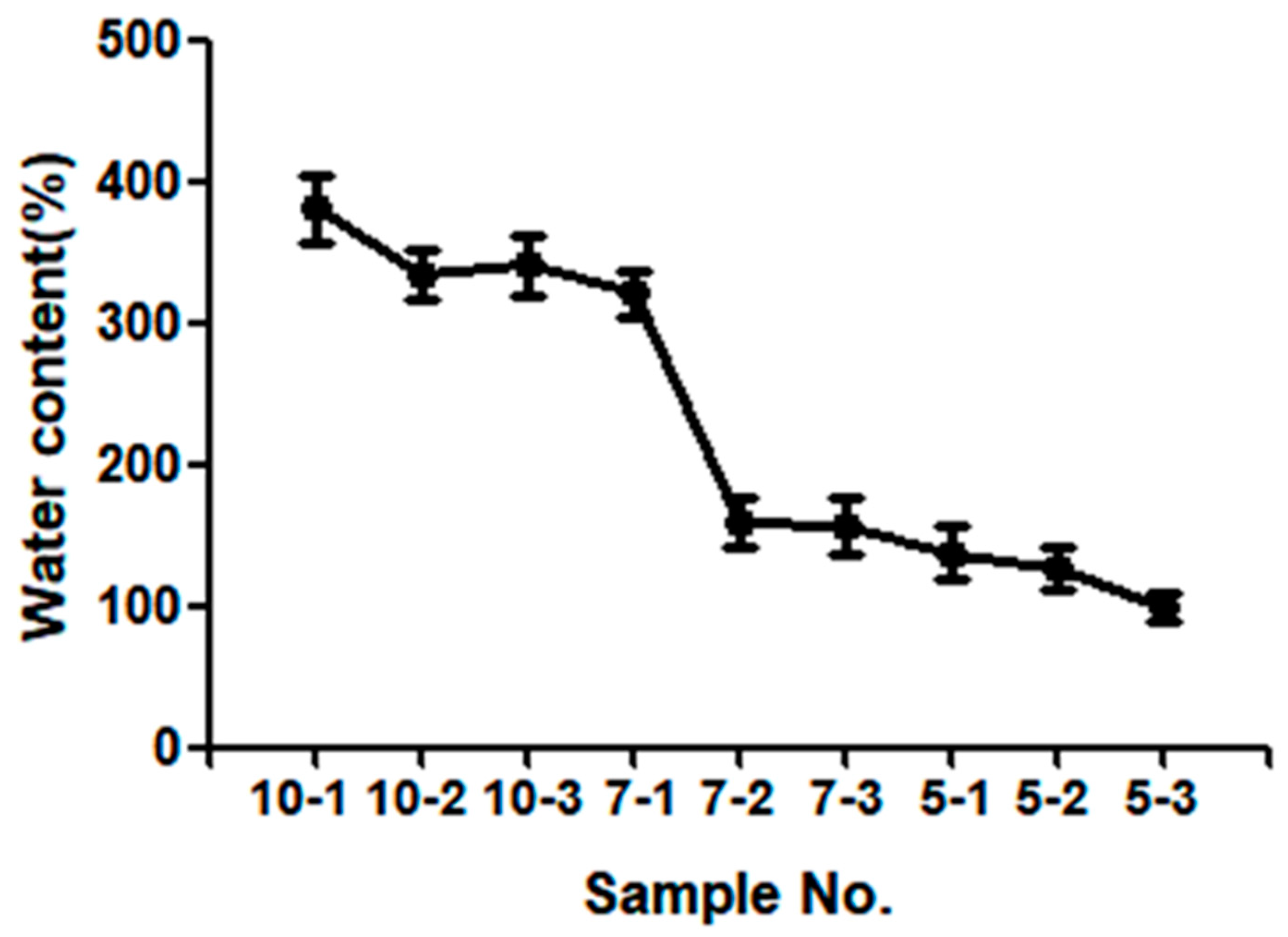
2.5. Swelling Properties
2.6. Measurements of the Mechanical Properties
2.7. In Vitro Test
2.8. Statistical Analysis
3. Results and Discussion
3.1. Synthesis of the Poly(HEMA-Am)
3.2. Characterization of the Poly(HEMA-Am)
3.2.1. FT-IR Spectroscopy
3.2.2. Scanning Electron Microscope
3.3. Equilibrium Water Content of the Poly(HEMA-Am)
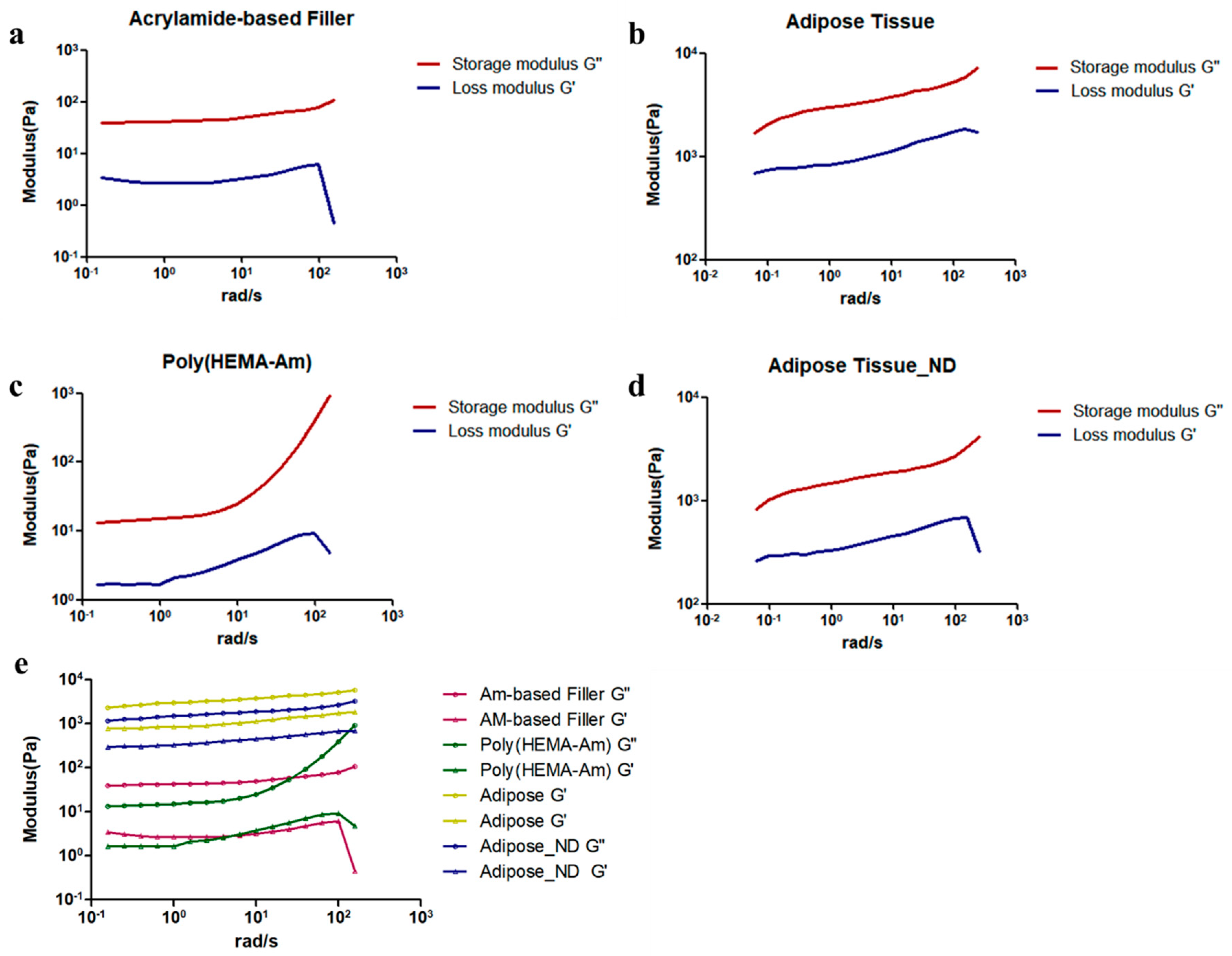
3.4. Mechanical Properties of the Poly(HEMA-Am) Hydrogel
3.5. In Vitro Cytotoxicity Assay
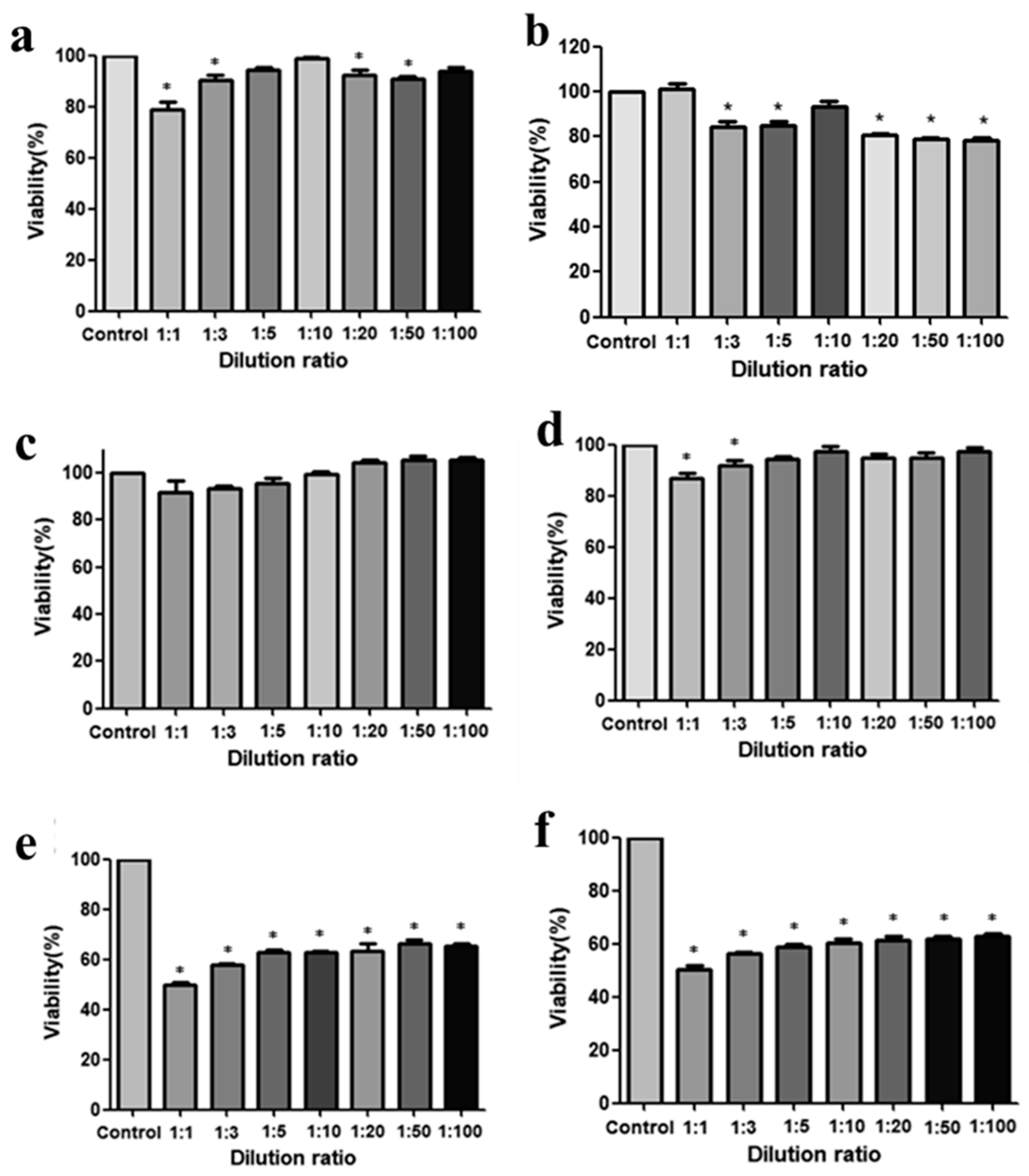
3.5.1. Cell Viability Assay
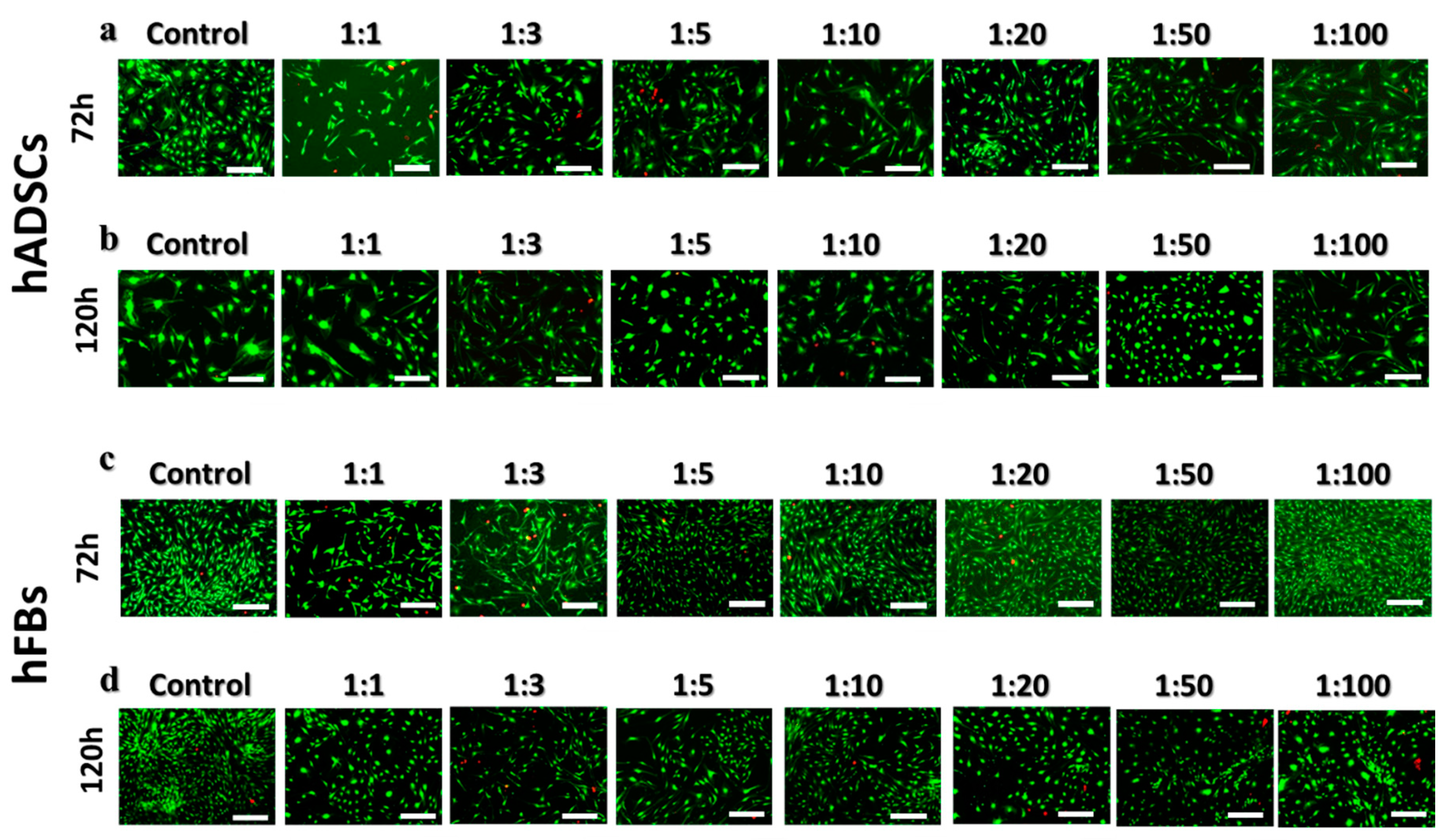
3.5.2. Live and Dead Assay
4. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Engelman, D.E.; Bloom, B.; Goldberg, D.J. Dermal fillers: Complications and informed consent. J. Cosmet. Laser Ther. 2005, 7, 29–32. [Google Scholar] [CrossRef] [PubMed]
- Pittet, B.; Montandon, D.; Pittet, D. Infection in breast implants. Lancet Infect. Dis. 2005, 5, 94–106. [Google Scholar] [CrossRef]
- Schmauss, D.; Machens, H.-G.; Harder, Y. Breast Reconstruction after Mastectomy. Front. Surg. 2015, 2, 71. [Google Scholar] [CrossRef] [PubMed]
- Roh, T.S. Letter: Position Statement of Korean Academic Society of Aesthetic and Reconstructive Breast Surgery: Concerning the Use of Aquafilling® for Breast Augmentation. Arch. Aesthetic Plast. Surg. 2016, 22, 45–46. [Google Scholar] [CrossRef]
- Broder, K.W.; Cohen, S.R. An overview of permanent and semipermanent fillers. Plast. Reconstr.Surg. 2006, 118, 7S–14S. [Google Scholar] [CrossRef] [PubMed]
- Bergeret-Galley, C. Comparison of resorbable soft tissue fillers. Aesthetic Surg. J. 2004, 24, 33–46. [Google Scholar] [CrossRef] [PubMed]
- Christensen, L.; Breiting, V.; Janssen, M.; Vuust, J.; Hoqdall, E. Adverse Reactions to Injectable Soft Tissue Permanent Fillers. Aesthetic Plast. Surg. 2005, 29, 34–48. [Google Scholar] [CrossRef] [PubMed]
- Ellis, D.A.; Makdessian, A.S.; Brown, D.J. Survey of future injectables. Facial Plast. Surg. Clin. N. Am. 2001, 9, 405–411. [Google Scholar] [CrossRef]
- Van Nieuwenhove, I.; Tytgat, L.; Ryx, M.; Blondeel, P.; Stillaert, F.; Thrienpont, H.; Ottevaere, H.; Dubruel, P.; Van Vlierberghe, S. Soft tissue fillers for adipose tissue regeneration: From hydrogel development toward clinical applications. Acta Biomater. 2017, 63, 37–49. [Google Scholar] [CrossRef] [PubMed]
- Lemperle, G.; Morhenn, V.; Charrier, U. Human Histology and Persistence of Various Injectable Filler Substances for Soft Tissue Augmentation. Aesthetic Plast. Surg. 2003, 27, 354–366. [Google Scholar] [CrossRef] [PubMed]
- Alcalay, J.; Alkalay, R.; Gat, A.; Yorav, S. Late-onset granulomatous reaction to Artecoll. Dermatol. Surg. 2003, 29, 859–862. [Google Scholar] [PubMed]
- Funt, D.; Pavicic, T. Dermal fillers in aesthetics: An overview of adverse events and treatment approaches. Clin. Cosmet. Investig. Dermatol. 2013, 6, 295–316. [Google Scholar] [CrossRef] [PubMed]
- Smith, E.A.; Oehme, F.W. Acrylamide and Polyacrylamide: A Review of Production, Use, Environmental Fate and Neurotoxicity; De Gruyter: Berlin, Germany, 1991. [Google Scholar]
- Lafaille, P.; Benedetto, A. Fillers: Contraindications, Side Effects and Precautions. J. Cutan. Aesthetic Surg. 2010, 3, 16–19. [Google Scholar] [CrossRef] [PubMed]
- Sclafani, A.P.; Romo, T. III. Injectable fillers for facial soft tissue enhancement. Facial Plast. Surg. 2000, 16, 29–34. [Google Scholar] [CrossRef] [PubMed]
- Andre, P.; Lowe, N.J.; Parc, A.; Clerici, T.H.; Zimmermann, U. Adverse reactions to dermal fillers: A review of European experiences. J. Cosmet. Laser Ther. 2005, 7, 171–176. [Google Scholar] [CrossRef] [PubMed]
- Bergeret-Galley, C.; Latouche, X.; Illouz, Y.-G. The value of a new filler material in corrective and cosmetic surgery: DermaLive and DermaDeep. Aesthetic Plast. Surg. 2001, 25, 249–255. [Google Scholar] [CrossRef] [PubMed]
- Alijotas-Reig, J.; Garcia-Gimenez, V. Delayed immune-mediated adverse effects related to hyaluronic acid and acrylic hydrogel dermal fillers: Clinical findings, long-term follow-up and review of the literature. J. Eur. Acad. Dermatol. Venereol. 2008, 22, 150–161. [Google Scholar] [CrossRef] [PubMed]
- Pitaru, S.; Noff, M.; Blok, L.; Nir, E.; Pitaru, S.; Goldlust, A.; Savion, N. Long-Term Efficacy of a Novel Ribose–Cross-linked Collagen Dermal Filler: A Histologic and Histomorphometric Study in an Animal Model. Dermatol. Surg. 2007, 33, 1045–1054. [Google Scholar] [CrossRef] [PubMed]
- Duranti, F.; Salti, G.; Bovani, B.; Calandra, M.; Rosati, M.L. Injectable hyaluronic acid gel for soft tissue augmentation. Dermatol. Surg. 1998, 24, 1317–1325. [Google Scholar] [CrossRef] [PubMed]
- Peters, W.; Fornasier, V. Complications from injectable materials used for breast augmentation. Canadian J. Plast. Surg. 2009, 17, 89–96. [Google Scholar] [CrossRef] [Green Version]
- Luo, Y.; Dalton, P.D.; Shoichet, M.S. Shoichet, Investigating the properties of novel poly(2-hydroxyethyl methacrylate-co-methyl methacrylate) hydrogel hollow fiber membranes. Chem. Mater. 2001, 13, 4087–4093. [Google Scholar] [CrossRef]
- Schwanninger, M.; Rodrigues, J.; Pereira, H.; Hinterstoisser, B. Effects of short-time vibratory ball milling on the shape of FT-IR spectra of wood and cellulose. Vib. Spectrosc. 2004, 36, 23–40. [Google Scholar] [CrossRef] [Green Version]
- Katime, I.; Mendizábal, E. Swelling properties of new hydrogels based on the dimethyl amino ethyl acrylate methyl chloride quaternary salt with acrylic acid and 2-methylene butane-1,4-dioic acid monomers in aqueous solutions. Mater. Sci. Appl. 2010, 1, 162–167. [Google Scholar] [CrossRef]
- Meyvis, T.K.; Stubbe, B.G.; Van Steenbergen, M.J.; Hennink, W.E.; De Smedt, S.C.; Demeester, J. A comparison between the use of dynamic mechanical analysis and oscillatory shear rheometry for the characterisation of hydrogels. Int. J. Pharm. 2002, 244, 163–168. [Google Scholar] [CrossRef]
- Araña, M.; Mazo, M.; Aranda, P.; Pelacho, B.; Prosper, F. Adipose tissue-derived mesenchymal stem cells: Isolation, expansion, and characterization. In Cellular Cardiomyoplasty; Springer: Berlin, Germany, 2013; pp. 47–61. [Google Scholar]
- ISO. 10993-12: 2008–Biological Evaluation of Medical Devices–Part 12: Sample Preparation and Reference Materials, ISO 10993-12:2007, German version: DIN EN ISO; ISO: Geneva, Switzerland, 2008; pp. 10912–10993. [Google Scholar]
- Zhou, S.; Cui, Z.; Urban, J. Dead cell counts during serum cultivation are underestimated by the fluorescent live/dead assay. Biotechnol. J. 2011, 6, 513–518. [Google Scholar] [CrossRef] [PubMed]
- Dalton, P.D.; Shoichet, M.S. Creating porous tubes by centrifugal forces for soft tissue application. Biomaterials 2001, 22, 2661–2669. [Google Scholar] [CrossRef]
- Finlay, J.A.; Callow, M.E. The toxicity of alkyl amines: The effects of pH. Biofouling 1997, 11, 19–30. [Google Scholar] [CrossRef]
- Arslan, G.; Celik, L.; Atasoy, M.M.; Cubuk, R. Complication of non-US guided procedure of aquafilling breast gel. Med. Ultrasonography 2017, 19, 236–237. [Google Scholar] [CrossRef] [PubMed]
- Lynch, I.; Dawson, K.A. Effect of a Polymeric Additive on the Pore-Size Distribution and Shrinking Process of a Hydrogel Network. Macromol. Chem. Phys. 2003, 204, 443–450. [Google Scholar] [CrossRef]
- Moon, N.G.; Pekkanen, A.M.; Long, T.E.; Showalter, T.N.; Libby, B. Thiol-Michael ‘click’ hydrogels as an imageable packing material for cancer therapy. Polymer 2017, 125, 66–75. [Google Scholar] [CrossRef]
- Banerjee, A.; Arha, M.; Choudhary, S.; Ashton, R.S.; Bhatia, S.R.; Schaffer, D.V.; Kane, R.S. The influence of hydrogel modulus on the proliferation and differentiation of encapsulated neural stem cells. Biomaterials 2009, 30, 4695–4699. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Agache, P.; Monneur, C.; Leveque, J.; De Rigal, J. Mechanical properties and Young's modulus of human skin in vivo. Arch. Dermatol. Res. 1980, 269, 221–232. [Google Scholar] [CrossRef] [PubMed]
- Patel, P.N.; Smith, C.K.; Patrick, C.W. Rheological and recovery properties of poly(ethylene glycol) diacrylate hydrogels and human adipose tissue. J. Biomed. Mater. Res. Part A 2005, 73, 313–319. [Google Scholar] [CrossRef] [PubMed]
- Jeong, M.; Cho, J.; Shin, J.-I.; Jeon, Y.-J.; Kim, J.-H.; Lee, S.-J.; Kim, E.-S.; Lee, K. Hempseed oil induces reactive oxygen species-and C/EBP homologous protein-mediated apoptosis in MH7A human rheumatoid arthritis fibroblast-like synovial cells. J. Ethnopharmacol. 2014, 154, 745–752. [Google Scholar] [CrossRef] [PubMed]
- Saunders, R.E.; Gough, J.E.; Derby, B. Delivery of human fibroblast cells by piezoelectric drop-on-demand inkjet printing. Biomaterials 2008, 29, 193–203. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| DI Water (mL) | Sample No. | HEMA (wt % of monomer) | EGDMA (wt % of monomer) | APS/TEMED (wt % of monomer) | Am (wt % of monomer) |
|---|---|---|---|---|---|
| 10 | 10-1 | 18 | 3.2 | 1.7/1.7 | 80 |
| 10-2 | 31 | 2.7 | 1.4/1.4 | 71 | |
| 10-3 | 40 | 2.2 | 1.2/1.2 | 59 | |
| 7 | 7-1 | 18 | 3.2 | 1.7/1.7 | 80 |
| 7-2 | 31 | 2.7 | 1.4/1.4 | 71 | |
| 7-3 | 40 | 2.2 | 1.2/1.2 | 59 | |
| 5 | 5-1 | 18 | 3.2 | 1.7/1.7 | 80 |
| 5-2 | 31 | 2.7 | 1.4/1.4 | 71 | |
| 5-3 | 40 | 2.2 | 1.2/1.2 | 59 |
| Type of Bond | IR Bands (cm−1) |
|---|---|
| Primary amine (CONH2) | 3346.71, 3194.65 |
| Amide C=O stretch peak | 1660.68 |
| Amide N–H bonding peak | 1450.72 |
| Secondary amine stretch peak | - |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, S.; Shin, B.H.; Yang, C.; Jeong, S.; Shim, J.H.; Park, M.H.; Choy, Y.B.; Heo, C.Y.; Lee, K. Development of Poly(HEMA-Am) Polymer Hydrogel Filler for Soft Tissue Reconstruction by Facile Polymerization. Polymers 2018, 10, 772. https://doi.org/10.3390/polym10070772
Kim S, Shin BH, Yang C, Jeong S, Shim JH, Park MH, Choy YB, Heo CY, Lee K. Development of Poly(HEMA-Am) Polymer Hydrogel Filler for Soft Tissue Reconstruction by Facile Polymerization. Polymers. 2018; 10(7):772. https://doi.org/10.3390/polym10070772
Chicago/Turabian StyleKim, Sujin, Byung Ho Shin, Chungmo Yang, Soohyun Jeong, Jung Hee Shim, Min Hee Park, Young Bin Choy, Chan Yeong Heo, and Kangwon Lee. 2018. "Development of Poly(HEMA-Am) Polymer Hydrogel Filler for Soft Tissue Reconstruction by Facile Polymerization" Polymers 10, no. 7: 772. https://doi.org/10.3390/polym10070772
APA StyleKim, S., Shin, B. H., Yang, C., Jeong, S., Shim, J. H., Park, M. H., Choy, Y. B., Heo, C. Y., & Lee, K. (2018). Development of Poly(HEMA-Am) Polymer Hydrogel Filler for Soft Tissue Reconstruction by Facile Polymerization. Polymers, 10(7), 772. https://doi.org/10.3390/polym10070772