
One-Year Clinical Performance of the Fast-Modelling Bulk Technique and Composite-Up Layering Technique in Class I Cavities

 ,
, 
 ,
,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Clinical Evaluation
2.3. Statistical Analysis
3. Results
3.1. Comparison of Biological Criteria
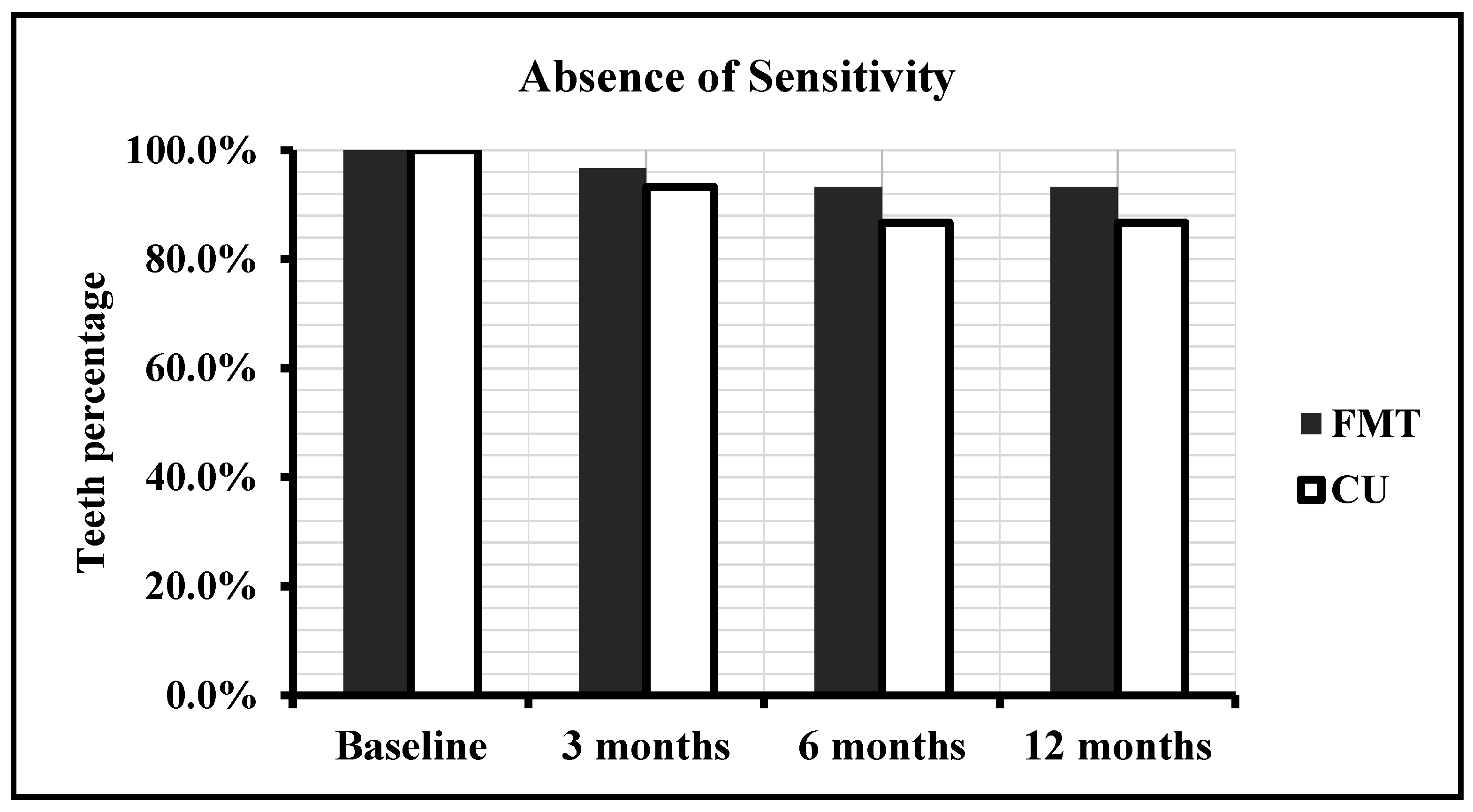
3.1.1. Sensitivity
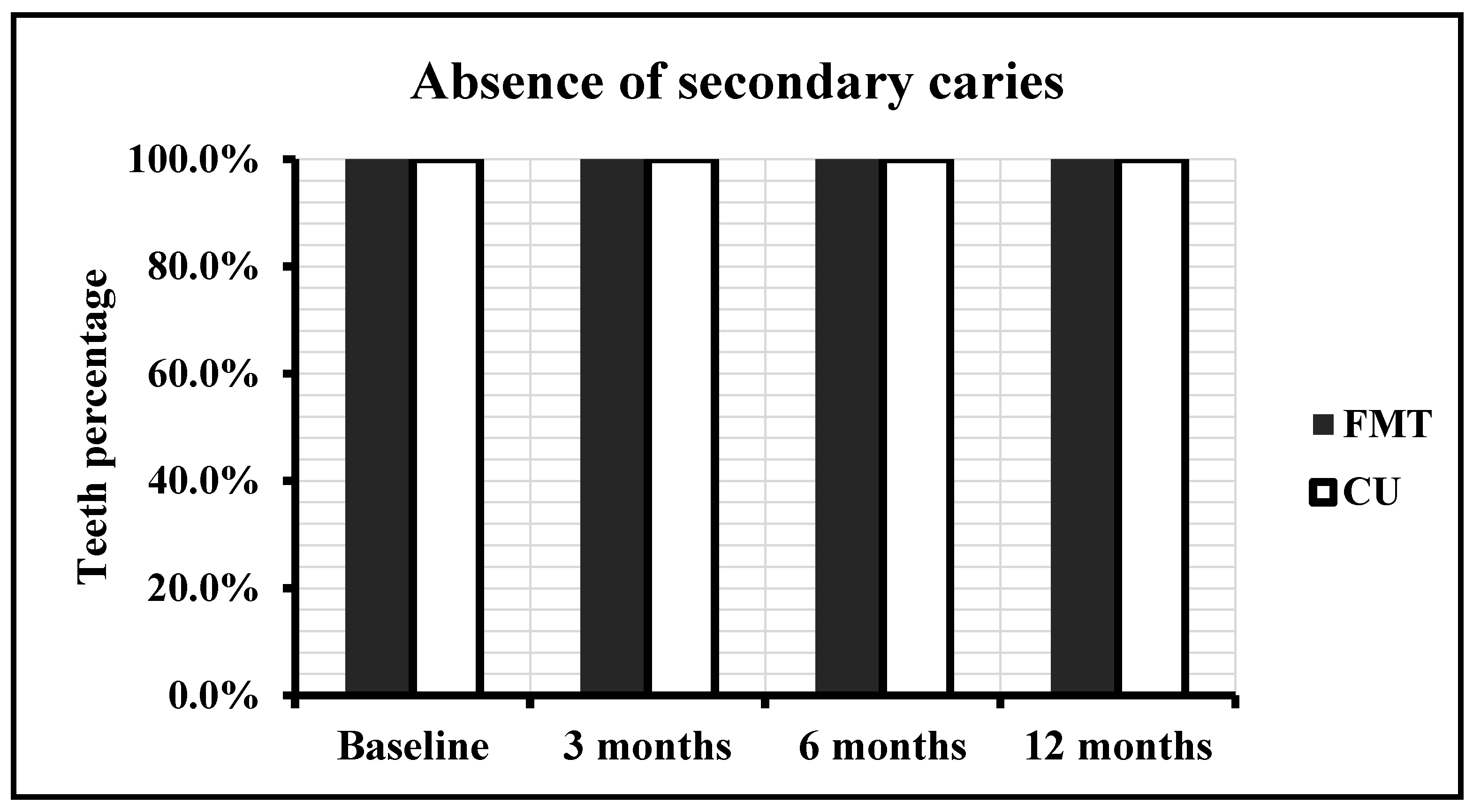
3.1.2. Secondary Caries
3.2. Comparison of Functional Criteria
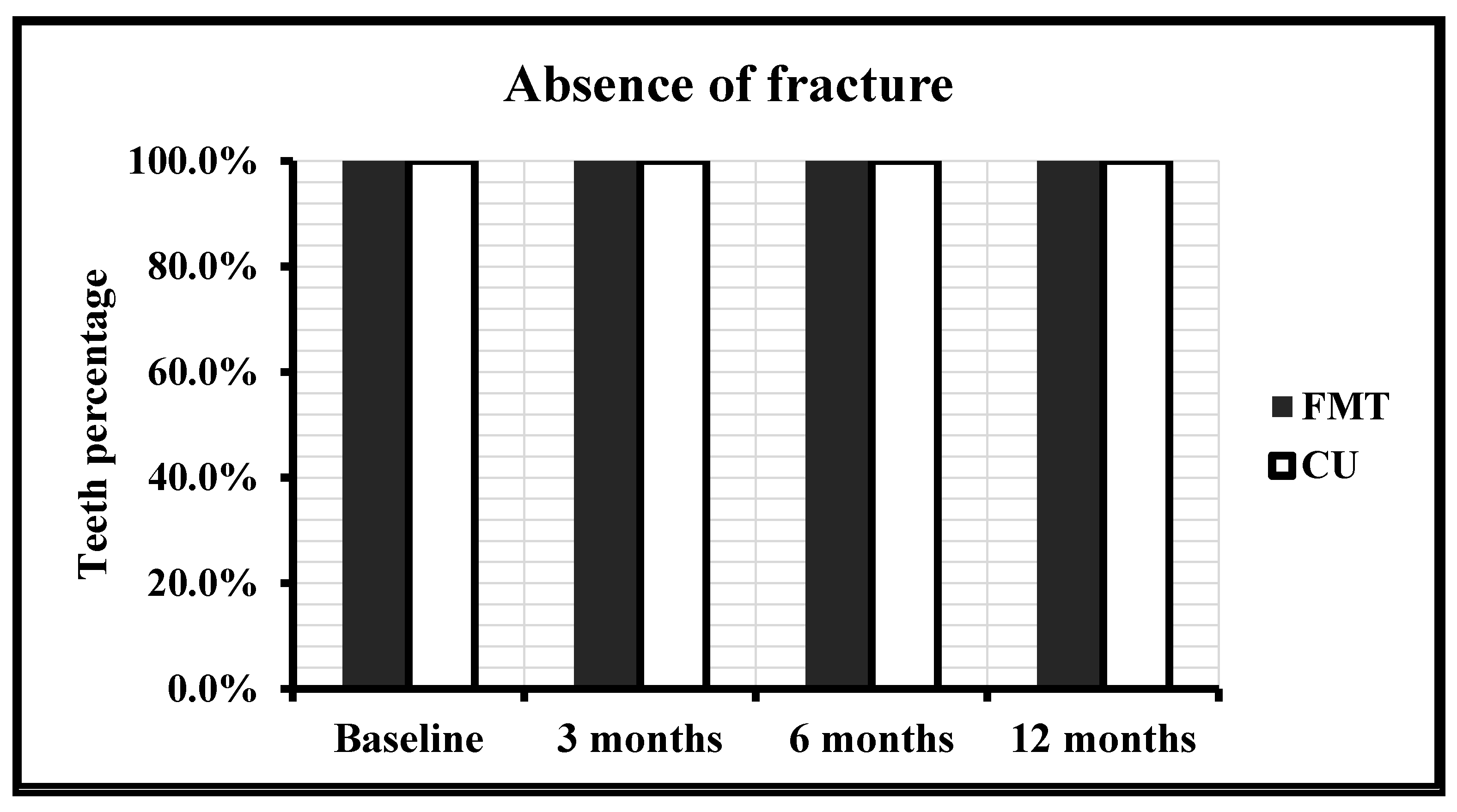
3.2.1. Fracture
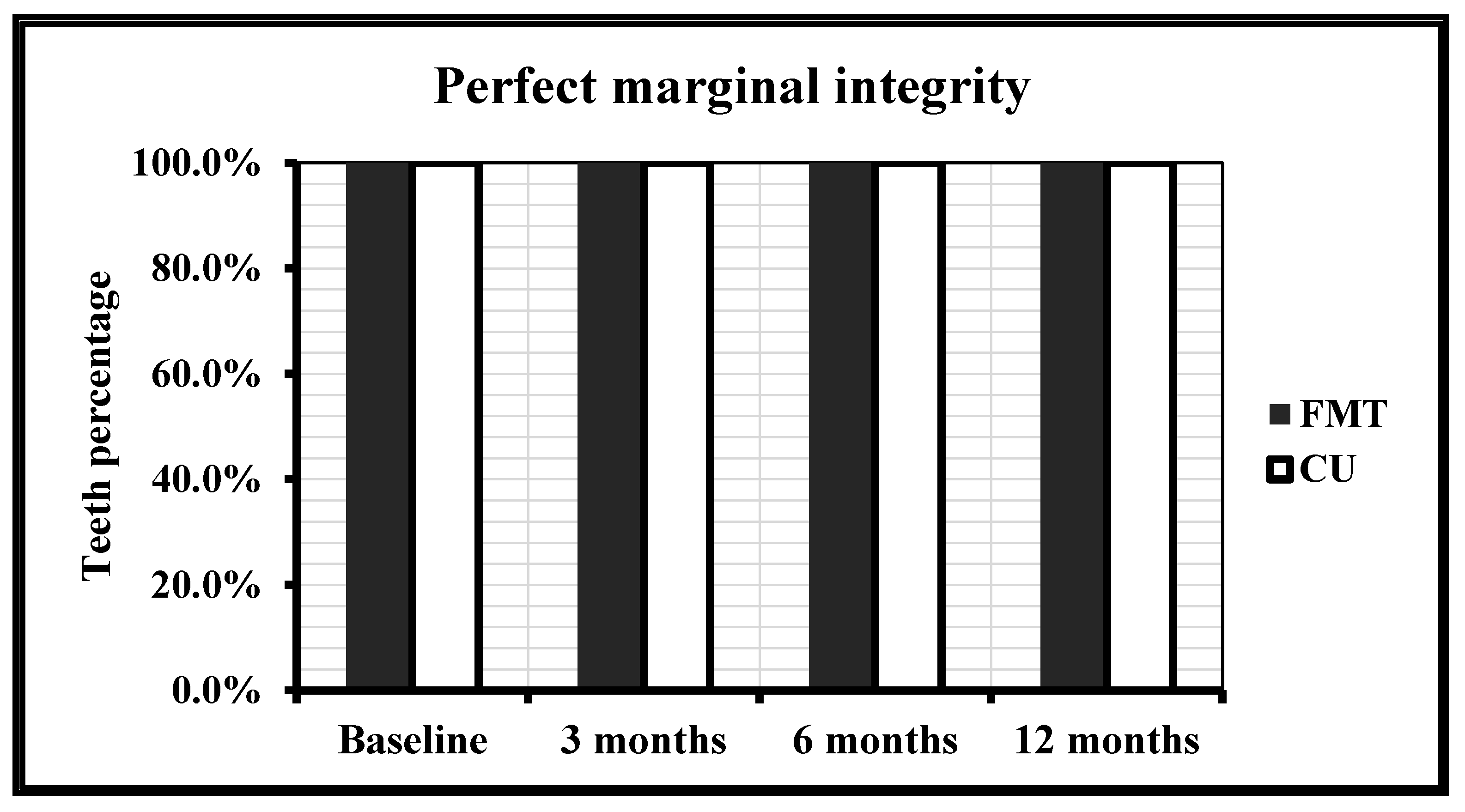
3.2.2. Marginal Integrity
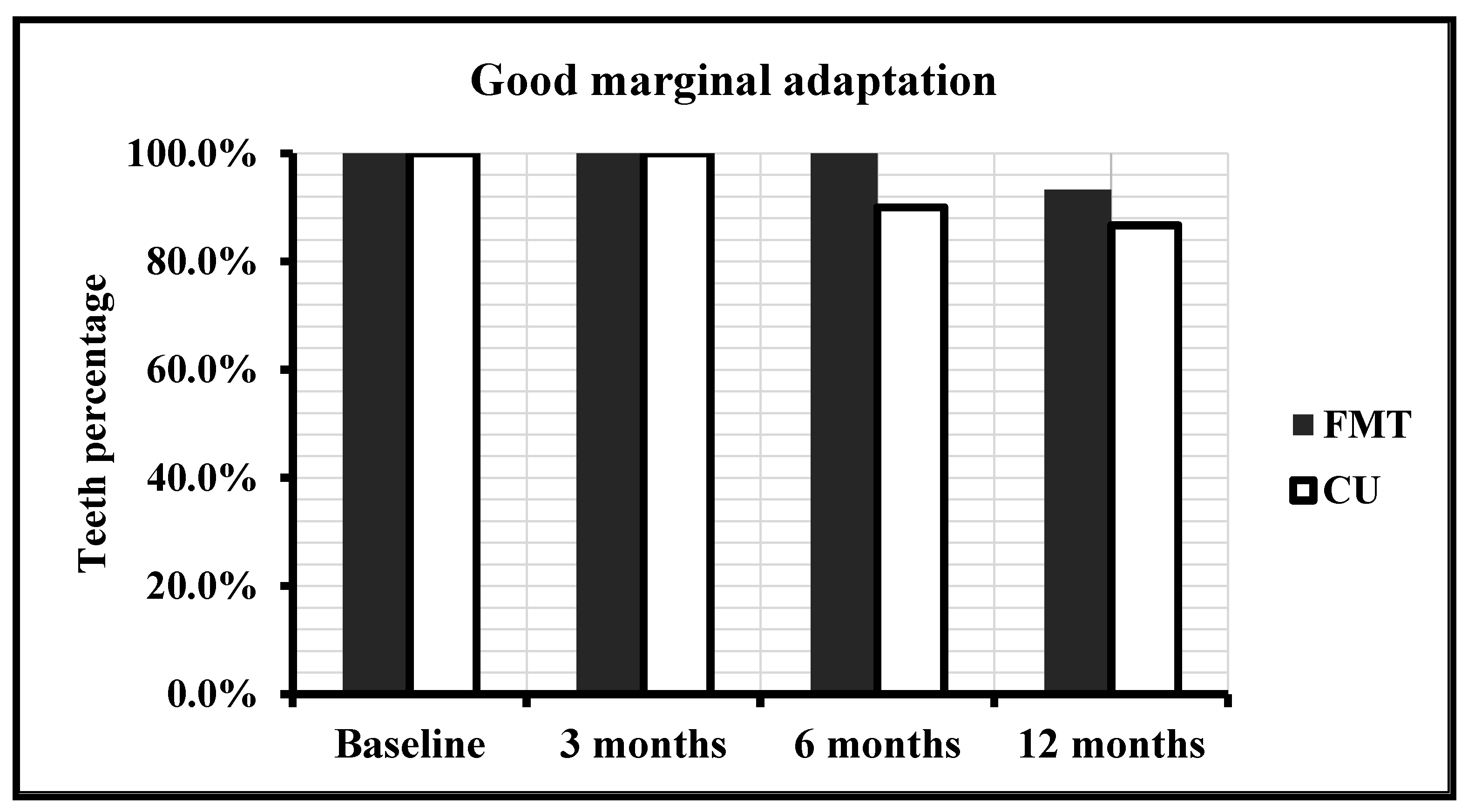
3.2.3. Comparison of Radiological Criteria
Marginal Adaptation
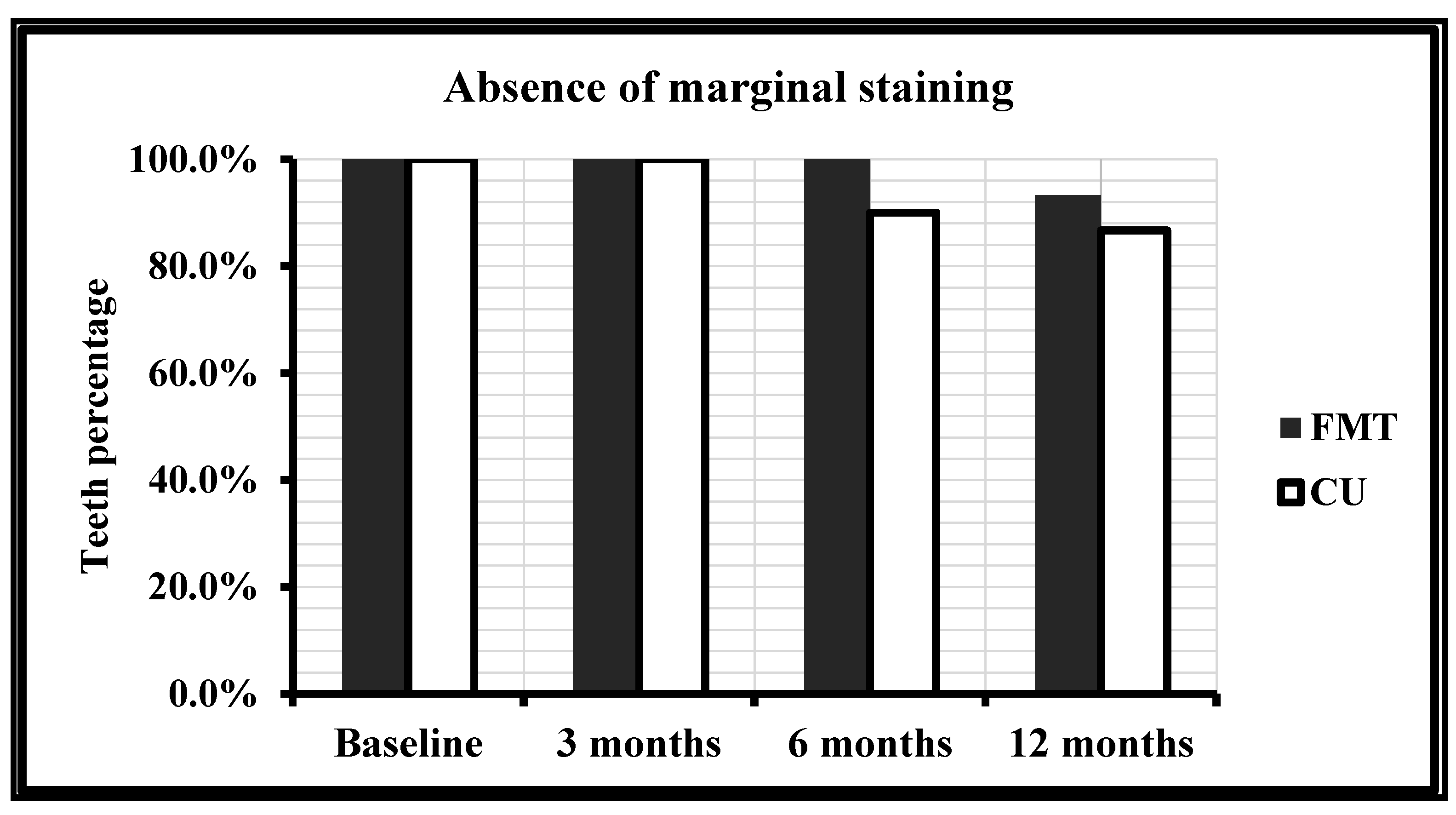
3.3. Comparison of Aesthetic Criteria
Marginal Discoloration
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Celik, C.; Arhun, N.; Yamanel, K. Clinical Evaluation of Resin-Based Composites in Posterior Restorations: 12-Month Results. Eur. J. Dent. 2010, 4, 057–065. [Google Scholar] [CrossRef] [Green Version]
- El-Banna, A.; Sherief, D.; Fawzy, A.S. Resin-based dental composites for tooth filling. In Advanced Dental Biomaterials; Woodhead Publishing: Cambridge, UK, 2019; pp. 127–173. [Google Scholar] [CrossRef]
- Miletic, V. Development of Dental Composites. In Dental Composite Materials for Direct Restorations; Springer: Cham, Switzerland, 2018; pp. 3–9. [Google Scholar]
- Soares, C.J.; Faria-E-Silva, A.L.; Rodrigues, M.D.P.; Vilela, A.B.F.; Pfeifer, C.S.; Tantbirojn, D.; Versluis, A. Polymerization shrinkage stress of composite resins and resin cements—What do we need to know? Braz. Oral Res. 2017, 31. [Google Scholar] [CrossRef] [Green Version]
- Arbildo-Vega, H.; Lapinska, B.; Panda, S.; Lamas-Lara, C.; Khan, A.; Lukomska-Szymanska, M. Clinical Effectiveness of Bulk-Fill and Conventional Resin Composite Restorations: Systematic Review and Meta-Analysis. Polymers 2020, 12, 1786. [Google Scholar] [CrossRef]
- Hardan, L.; Lukomska-Szymanska, M.; Zarow, M.; Cuevas-Suárez, C.E.; Bourgi, R.; Jakubowicz, N.; Sokolowski, K.; D’Arcangelo, C. One-Year Clinical Aging of Low Stress Bulk-Fill Flowable Composite in Class II Restorations: A Case Report and Literature Review. Coatings 2021, 11, 504. [Google Scholar] [CrossRef]
- Hardan, L.; Bourgi, R.; Kharouf, N.; Mancino, D.; Zarow, M.; Jakubowicz, N.; Haikel, Y.; Cuevas-Suárez, C. Bond Strength of Universal Adhesives to Dentin: A Systematic Review and Meta-Analysis. Polymers 2021, 13, 814. [Google Scholar] [CrossRef]
- Hardan, L.S.; Amm, E.W.; Ghayad, A. Effect of different modes of light curing and resin composites on microleakage of Class II restorations. Odontostomatol. Trop. 2008, 31, 27–34. [Google Scholar]
- Hardan, L.S.; Amm, E.W.; Ghayad, A.; Ghosn, C.; Khraisat, A. Effect of different modes of light curing and resin composites on microleakage of Class II restorations—Part II. Odontostomatol. Trop. 2009, 32, 29–37. [Google Scholar]
- Comba, A.; Scotti, N.; Maravić, T.; Mazzoni, A.; Carossa, M.; Breschi, L.; Cadenaro, M. Vickers Hardness and Shrinkage Stress Evaluation of Low and High Viscosity Bulk-Fill Resin Composite. Polymers 2020, 12, 1477. [Google Scholar] [CrossRef]
- Bucuta, S.; Ilie, N. Light transmittance and micro-mechanical properties of bulk fill vs. conventional resin based composites. Clin. Oral Investig. 2014, 18, 1991–2000. [Google Scholar] [CrossRef]
- Rudrapati, L.; Chandrasekhar, V.; Badami, V.; Tummala, M. Incremental techniques in direct composite restoration. J. Conserv. Dent. 2017, 20, 386–391. [Google Scholar] [CrossRef]
- Kim, M.; Park, S. Comparison of Premolar Cuspal Deflection in Bulk or in Incremental Composite Restoration Methods. Oper. Dent. 2011, 36, 326–334. [Google Scholar] [CrossRef]
- Yuan, J.-X.; Yang, K.-Y.; Ma, J.; Wang, Z.-Z.; Guo, Q.-Y.; Liu, F. Step-by-step teaching method: Improving learning outcomes of undergraduate dental students in layering techniques for direct composite resin restorations. BMC Med. Educ. 2020, 20, 300. [Google Scholar] [CrossRef] [PubMed]
- Purk, J.H.; Dusevich, V.; Glaros, A.; Eick, J.D. Adhesive analysis of voids in class II composite resin restorations at the axial and gingival cavity walls restored under in vivo versus in vitro conditions. Dent. Mater. 2007, 23, 871–877. [Google Scholar] [CrossRef] [Green Version]
- Kaisarly, D.; El Gezawi, M.; Keßler, A.; Rösch, P.; Kunzelmann, K.-H. Shrinkage vectors in flowable bulk-fill and conventional composites: Bulk versus incremental application. Clin. Oral Investig. 2021, 25, 1127–1139. [Google Scholar] [CrossRef]
- Boaro, L.C.C.; Lopes, D.P.; de Souza, A.S.C.; Nakano, E.L.; Perez, M.D.A.; Pfeifer, C.S.; Gonçalves, F. Clinical performance and chemical-physical properties of bulk fill composites resin —a systematic review and meta-analysis. Dent. Mater. 2019, 35, e249–e264. [Google Scholar] [CrossRef]
- Rosatto, C.; Bicalho, A.; Veríssimo, C.; Bragança, G.; Rodrigues, M.; Tantbirojn, D.; Versluis, A.; Soares, C. Mechanical properties, shrinkage stress, cuspal strain and fracture resistance of molars restored with bulk-fill composites and incremental filling technique. J. Dent. 2015, 43, 1519–1528. [Google Scholar] [CrossRef]
- Kim, Y.-J.; Kim, R.J.Y.; Ferracane, J.; Lee, I.-B. Influence of the Compliance and Layering Method on the Wall Deflection of Simulated Cavities in Bulk-fill Composite Restoration. Oper. Dent. 2016, 41, e183–e194. [Google Scholar] [CrossRef]
- Van Dijken, J.W.; Pallesen, U. Posterior bulk-filled resin composite restorations: A 5-year randomized controlled clinical study. J. Dent. 2016, 51, 29–35. [Google Scholar] [CrossRef]
- Azeem, R.A.; Sureshbabu, N.M. Clinical performance of direct versus indirect composite restorations in posterior teeth: A systematic review. J. Conserv. Dent. 2018, 21, 2–9. [Google Scholar]
- El-Damanhoury, H.; Platt, J.A. Polymerization Shrinkage Stress Kinetics and Related Properties of Bulk-fill Resin Composites. Oper. Dent. 2014, 39, 374–382. [Google Scholar] [CrossRef]
- De Assis, F.S.; Lima, S.N.L.; Tonetto, M.R.; Bhandi, S.H.; Pinto, S.C.S.; Malaquias, P.; Loguercio, A.D.; Bandéca, M.C. Evaluation of Bond Strength, Marginal Integrity, and Fracture Strength of Bulk- vs Incrementally-filled Restorations. J. Adhes. Dent. 2016, 18, 317–323. [Google Scholar]
- Veloso, S.R.M.; Lemos, C.A.A.; Moraes, S.; Vasconcelos, B.C.D.E.; Pellizzer, E.P.; Monteiro, G.Q.D.M. Clinical performance of bulk-fill and conventional resin composite restorations in posterior teeth: A systematic review and meta-analysis. Clin. Oral Investig. 2018, 23, 221–233. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sajnani, A.R.; Hegde, M.N. Leaching of monomers from bulk-fill composites: An in vitro study. J. Conserv. Dent. 2016, 19, 482–486. [Google Scholar] [CrossRef] [PubMed]
- Lazarchik, D.A.; Hammond, B.D.; Sikes, C.L.; Looney, S.W.; Rueggeberg, F.A. Hardness comparison of bulk-filled/transtooth and incremental-filled/occlusally irradiated composite resins. J. Prosthet. Dent. 2007, 98, 129–140. [Google Scholar] [CrossRef]
- Abbasi, M.; Moradi, Z.; Mirzaei, M.; Kharazifard, M.J.; Rezaei, S. Polymerization Shrinkage of Five Bulk-Fill Resin compo-sites in Comparison with a Conventional Resin composite. J. Dent. 2018, 15, 365–374. [Google Scholar]
- Tomaszewska, I.M.; Kearns, J.O.; Ilie, N.; Fleming, G.J. Bulk fill restoratives: To cap or not to cap—That is the question? J. Dent. 2015, 43, 309–316. [Google Scholar] [CrossRef]
- Hoseinifar, R.; Mortazavi-Lahijani, E.; Mollahassani, H.; Ghaderi, A. One Year Clinical Evaluation of a Low Shrinkage Composite Compared with a Packable Composite Resin: A Randomized Clinical Trial. J. Dent. 2017, 14, 84–91. [Google Scholar]
- Berkowitz, G.S.; Spielman, H.; Matthews, A.G.; Vena, D.; Craig, R.G.; Curro, F.A.; Thompson, V.P. Postoperative hypersensitivity and its rela-tionship to preparation variables in Class I resin-based composite restorations: Findings from the practitioners engaged in applied research and learning (PEARL) Network. Part 1. Compend. Contin. Educ. Dent. 2013, 34, e44–e52. [Google Scholar]
- Auschill, T.M.; Koch, C.A.; Wolkewitz, M.; Hellwig, E.; Arweiler, N.B. Occurrence and Causing Stimuli of Postoperative Sensitivity in Composite Restorations. Oper. Dent. 2009, 34, 3–10. [Google Scholar] [CrossRef]
- Perdigão, J. Current perspectives on dental adhesion: (1) Dentin adhesion—Not there yet. Jpn. Dent. Sci. Rev. 2020, 56, 190–207. [Google Scholar] [CrossRef]
- Sancakli, H.S.; Yildiz, E.; Bayrak, I.; Özel, S. Effect of different adhesive strategies on the post-operative sensitivity of class I composite restorations. Eur. J. Dent. 2014, 8, 15–22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Casselli, D.S.M.; Martins, L.R.M. Postoperative sensitivity in Class I composite resin restorations in vivo. J. Adhes. Dent. 2006, 8, 53–58. [Google Scholar]
- Costa, T.; Rezende, M.; Sakamoto, A.; Bittencourt, B.; Dalzochio, P.; Loguercio, A.D.; Reis, A. Influence of Adhesive Type and Placement Technique on Postoperative Sensitivity in Posterior Composite Restorations. Oper. Dent. 2017, 42, 143–154. [Google Scholar] [CrossRef]
- Opdam, N.; Roeters, F.; Feilzer, A.; Verdonschot, E. Marginal integrity and postoperative sensitivity in Class 2 resin composite restorations in vivo. J. Dent. 1998, 26, 555–562. [Google Scholar] [CrossRef]
- Plant, C.G.; Anderson, R.J. The effect of cavity depth on the pulpal response to restorative materials. Br. Dent. J. 1978, 144, 10–13. [Google Scholar] [CrossRef] [PubMed]
- Tantbirojn, D.; Versluis, A.; Pintado, M.R.; DeLong, R.; Douglas, W.H. Tooth deformation patterns in molars after composite restoration. Dent. Mater. 2004, 20, 535–542. [Google Scholar] [CrossRef]
- Sobral, M.; Luz, M.A.A.C.; Santos, A.P.; Garone-Netto, N. Prevention of postoperative tooth sensitivity: A preliminary clinical trial. J. Oral Rehabil. 2005, 32, 661–668. [Google Scholar] [CrossRef] [PubMed]
- Van Dijken, J.W.; Pallesen, U. A six-year prospective randomized study of a nano-hybrid and a conventional hybrid resin composite in Class II restorations. Dent. Mater. 2013, 29, 191–198. [Google Scholar] [CrossRef] [PubMed]
- Dennison, J.B.; Sarrett, D.C. Prediction and diagnosis of clinical outcomes affecting restoration margins. J. Oral Rehabil. 2011, 39, 301–318. [Google Scholar] [CrossRef] [Green Version]
- Wang, Y.; Li, C.; Yuan, H.; Wong, M.C.; Zou, J.; Shi, Z.; Zhou, X. Rubber dam isolation for restorative treatment in dental patients. Cochrane Database Syst. Rev. 2016, 9, CD009858. [Google Scholar] [CrossRef] [Green Version]
- Samet, N.; Kwon, K.-R.; Good, P.; Weber, H.-P. Voids and interlayer gaps in Class 1 posterior composite restorations: A comparison between a microlayer and a 2-layer technique. Quintessence Int. 2006, 37, 803–809. [Google Scholar]
- Orłowski, M.; Tarczydło, B.; Chałas, R. Evaluation of Marginal Integrity of Four Bulk-Fill Dental Composite Materials:In VitroStudy. Sci. World J. 2015, 2015, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Furness, A.; Tadros, M.Y.; Looney, S.W.; Rueggeberg, F. Effect of bulk/incremental fill on internal gap formation of bulk-fill composites. J. Dent. 2014, 42, 439–449. [Google Scholar] [CrossRef] [PubMed]
- Kwon, Y.; Ferracane, J.; Lee, I.-B. Effect of layering methods, composite type, and flowable liner on the polymerization shrinkage stress of light cured composites. Dent. Mater. 2012, 28, 801–809. [Google Scholar] [CrossRef] [PubMed]
- Abbas, G.; Fleming, G.; Harrington, E.; Shortall, A.; Burke, F. Cuspal movement and microleakage in premolar teeth restored with a packable composite cured in bulk or in increments. J. Dent. 2003, 31, 437–444. [Google Scholar] [CrossRef]
- Skałecka-Sądel, A.; Grzebieluch, W. The marginal sealing of class II resin composite restoration located in enam-el—Evaluation in vitro. Dent. Med. Prob. 2012, 49, 502–509. [Google Scholar]
- Yazici, A.R.; Antonson, S.A.; Kutuk, Z.B.; Ergin, E. Thirty-Six-Month Clinical Comparison of Bulk Fill and Nanofill Composite Restorations. Oper. Dent. 2017, 42, 478–485. [Google Scholar] [CrossRef]
- Van Ende, A.; De Munck, J.; Van Landuyt, K.L.; Poitevin, A.; Peumans, M.; Van Meerbeek, B. Bulk-filling of high C-factor posterior cavities: Effect on adhesion to cavity-bottom dentin. Dent. Mater. 2013, 29, 269–277. [Google Scholar] [CrossRef]
- Agarwal, R.S.; Hiremath, H.; Agarwal, J.; Garg, A. Evaluation of cervical marginal and internal adaptation using newer bulk fill composites: An in vitro study. J. Conserv. Dent. 2015, 18, 56–61. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roggendorf, M.J.; Krämer, N.; Appelt, A.; Naumann, M.; Frankenberger, R. Marginal quality of flowable 4-mm base vs. conventionally layered resin composite. J. Dent. 2011, 39, 643–647. [Google Scholar] [CrossRef]
- Nedeljkovic, I.; Teughels, W.; De Munck, J.; Van Meerbeek, B.; Van Landuyt, K.L. Is secondary caries with composites a material-based problem? Dent. Mater. 2015, 31, e247–e277. [Google Scholar] [CrossRef] [PubMed]
- Dukic, W.; Delija, B.; DeRossi, D.; Dadic, I. Radiopacity of composite dental materials using a digital X-ray system. Dent. Mater. J. 2012, 31, 47–53. [Google Scholar] [CrossRef] [Green Version]
- Finan, L.; Palin, W.M.; Moskwa, N.; McGinley, E.L.; Fleming, G.J. The influence of irradiation potential on the degree of conversion and mechanical properties of two bulk-fill flowable RBC base materials. Dent. Mater. 2013, 29, 906–912. [Google Scholar] [CrossRef]
- Yaşa, B.; Kucukyilmaz, E.; Yasa, E.; Ertas, E.T. Comparative study of radiopacity of resin-based and glass ionomer-based bulk-fill restoratives using digital radiography. J. Oral Sci. 2015, 57, 79–85. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koc-Vural, U.; Baltacioglu, I.; Altinci, P. Color stability of bulk-fill and incremental-fill resin-based composites polished with aluminum-oxide impregnated disks. Restor. Dent. Endod. 2017, 42, 118–124. [Google Scholar] [CrossRef]
- Barakah, H.M.; Taher, N.M. Effect of polishing systems on stain susceptibility and surface roughness of nanocomposite resin material. J. Prosthet. Dent. 2014, 112, 625–631. [Google Scholar] [CrossRef]
- Gönülol, N.; Yılmaz, F. The effects of finishing and polishing techniques on surface roughness and color stability of nanocomposites. J. Dent. 2012, 40, e64–e70. [Google Scholar] [CrossRef] [PubMed]
- Baroudi, K.; Kaminedi, R.R.; Penumatsa, N.V.; Priya, T. The influence of finishing/polishing time and cooling system on surface roughness and microhardness of two different types of composite resin restorations. J. Int. Soc. Prev. Community Dent. 2014, 4, S99–S104. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morgan, M. Finishing and polishing of direct posterior resin restorations. Pract. Proced. Aesthet. Dent. 2004, 16, 211–217. [Google Scholar]
- Loguercio, A.; Rezende, M.; Gutierrez, M.; Costa, T.; Armas-Vega, A.; Reis, A. Randomized 36-month follow-up of posterior bulk-filled resin composite restorations. J. Dent. 2019, 85, 93–102. [Google Scholar] [CrossRef]
- Hirata, R.; Kabbach, W.; De Andrade, O.S.; Bonfante, E.A.; Giannini, M.; Coelho, P.G. Bulk Fill Composites: An Anatomic Sculpting Technique. J. Esthet. Restor. Dent. 2015, 27, 335–343. [Google Scholar] [CrossRef] [PubMed]
- Brunthaler, A.; König, F.; Lucas, T.; Sperr, W.; Schedle, A. Longevity of direct resin composite restorations in posterior teeth: A review. Clin. Oral Investig. 2003, 7, 63–70. [Google Scholar] [CrossRef] [PubMed]
- Opdam, N.; Collares, K.; Hickel, R.; Bayne, S.; Loomans, B.; Cenci, M.; Lynch, C.; Correa, M.; Demarco, F.; Schwendicke, F.; et al. Clinical studies in restorative dentistry: New directions and new demands. Dent. Mater. 2018, 34, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Beck, F.; Lettner, S.; Graf, A.; Bitriol, B.; Dumitrescu, N.; Bauer, P.; Moritz, A.; Schedle, A. Survival of direct resin restorations in posterior teeth within a 19-year period (1996–2015): A meta-analysis of prospective studies. Dent. Mater. 2015, 31, 958–985. [Google Scholar] [CrossRef] [PubMed]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Material | Type | Manufacturer | Composition |
|---|---|---|---|
| Filtek Z250XT | Nanohybrid composite | 3M ESPE, St. Paul, MN, USA | Bis-GMA; UDMA; Bis-EMA; PEGDMA and TEGDMA. Surface-modified zirconia/silica with a median particle size of approximately 3 μm or less. Nonagglomerated/nonaggregated 20 nm surface-modified silica particles. The filler loading is 82% by weight (68% by volume) |
| Filtek bulk-fill Posterior Restorative | Bulk-fill composite | 3M ESPE, St. Paul, MN, USA | AUDMA; UDMA; and 1, 12-dodecane-DMA 20 nm silica filler, a non-agglomerated nonaggregated 4–11 nm zirconia filler, an aggregated zirconia/silica cluster filler (comprised of 20 nm silica and 4–11 nm zirconia particles), and a ytterbium trifluoride filler consisting of agglomerate 100 nm particles. Inorganic filler loading is about 76.5% by weight (58.4% by volume) |
| Scotchbond™ Universal Etchant | Low-viscosity etching gel | 3M ESPE, St. Paul, MN, USA | 34% H3PO4, water, synthetic amorphous silica, polyethylene glycol, aluminum oxide |
| Adper™ Single Bond | Two-step etch-and-rinse adhesive | 3M ESPE, St. Paul, MN, USA | Bis-GMA; HEMA, dimethacrylates, polyalkenes acid copolymer, initiators, water, and ethanol |
| Outcome Variables and Methods for the Evaluation of Restorations | Clinically Excellent | Clinically Good | Clinically Sufficient | Clinically Unsatisfactory | Clinically Poor | |
|---|---|---|---|---|---|---|
| Biological Properties | Sensitivity | Absence of pain | Low pain | Moderate pain | Intense pain | Extreme pain |
| Secondary caries | No secondary caries | Small and localized. Demineralization area | Larger areas of demineralization. Only preventive measures necessary | Caries with cavitation and suspected undermining caries. Localized and accessible can be repaired | Deep secondary caries or exposed dentine that is not accessible for repair of restoration | |
| Functional Properties | Fracture | Restoration in place, no fracture | Small hairline crack | Two or more or larger hairline cracks and/or chipping (not affecting the marginal integrity or approximal contact) | Material chip fractures which damage marginal quality and/or approximal contacts | (Partial or complete) loss of the restoration or multiple fractures |
| Marginal integrity | Continuity between restoration/tooth | Marginal gap (<150 μm), white lines. Small marginal fracture removable by polishing | Gap < 250 μm not removable. Several small marginal fractures | Gap > 250 μm or dentine/base exposed. Severe marginal fractures | Restoration (complete or partial) is loose but in situ. Generalized major gaps or irregularities | |
| Radiographic examination | No pathology, harmonious transition between restoration and tooth | Acceptable material excess present. Positive/negative step present at margin < 150 μm | Marginal gap < 250 μm. Negative steps visible < 250 μm. No adverse effects noticed. Poor radiopacity of filling material | Marginal gap > 250 μm. Material excess accessible but not removable. Negative steps > 250 μm and reparable | Secondary caries, large gaps, large overhangs. Apical pathology. Fracture/loss of restoration or tooth | |
| Aesthetic Property | Marginal discoloration | No marginal staining | Minor staining, easily removable | Moderate staining between restoration and tooth | Surface staining recognizable from speaking distance. Or severe localized marginal staining not removable by polishing | Significant (detectable) marginal staining between restoration and tooth |
| Sensitivity | Absence of Pain | Low Pain | Moderate Pain | Intense Pain | Extreme Pain | |
|---|---|---|---|---|---|---|
| FMBT | Baseline | 30 (100.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) |
| 3 months | 29 (96.7%) | 1 (3.3%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | |
| 6 months | 28 (93.3%) | 2 (6.7%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | |
| 12 months | 28 (93.3%) | 2 (6.7%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | |
| CULT | Baseline | 30 (100.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) |
| 3 months | 28 (93.3%) | 2 (6.7%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | |
| 6 months | 26 (86.7%) | 2 (6.7%) | 2 (6.7%) | 0 (0.0%) | 0 (0.0%) | |
| 12 months | 26 (86.7%) | 2 (6.7%) | 2 (6.7%) | 0 (0.0%) | 0 (0.0%) | |
| Secondary Caries | No Secondary Caries | Small and Localized. Demineralization Area | Larger Areas of Demineralization. Only Preventive Measures Necessary | Caries with Cavitation and Suspected Undermining Caries. Localized and Accessible Can Be Repaired | Deep Secondary Caries or Exposed Dentine that Is Not Accessible for Repair of Restoration | |
|---|---|---|---|---|---|---|
| FMBT | Baseline | 30 (100.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) |
| 3 months | 30 (100.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | |
| 6 months | 30 (100.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | |
| 12 months | 30 (100.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | |
| CULT | Baseline | 30 (100.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) |
| 3 months | 30 (100.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | |
| 6 months | 30 (100.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | |
| 12 months | 30 (100.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | |
| Fracture | Restoration in Place, No Fracture | Small Hairline Crack | Two or More or Larger Hairline Cracks and/or Chipping (Not Affecting the Marginal Integrity or Approximal Contact) | Material Chip Fractures Which Damage Marginal Quality and/or Approximal Contacts | (Partial or Complete) Loss of the Restoration or Multiple Fractures | |
|---|---|---|---|---|---|---|
| FMBT | Baseline | 30 (100.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) |
| 3 months | 30 (100.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | |
| 6 months | 30 (100.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | |
| 12 months | 30 (100.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | |
| CULT | Baseline | 30 (100.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) |
| 3 months | 30 (100.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | |
| 6 months | 30 (100.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | |
| 12 months | 30 (100.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | |
| Marginal Integrity | Continuity between Restoration/Tooth | Marginal Gap (<150 μm), White Lines. Small Marginal Fracture Removable by Polishing | Gap < 250 μm Not Removable. Several Small Marginal Fractures | Gap > 250 μm or Dentine/Base Exposed. Severe Marginal Fractures | Restoration (Complete or Partial) Is Loose but in Situ. Generalized Major Gaps or Irregularities | |
|---|---|---|---|---|---|---|
| FMBT | Baseline | 30 (100.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) |
| 3 months | 30 (100.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | |
| 6 months | 30 (100.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | |
| 12 months | 30 (100.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | |
| CULT | Baseline | 30 (100.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) |
| 3 months | 30 (100.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | |
| 6 months | 30 (100.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | |
| 12 months | 30 (100.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | |
| Marginal Adaptation | No Pathology, Harmonious Transition between Restoration and Tooth | Acceptable Material Excess Present. Positive/Negative Step Present at Margin < 150 μm | Marginal Gap < 250 μm. Negative Steps Visible < 250 μm. No Adverse Effects Noticed. Poor Radiopacity of Filling Material | Marginal Gap > 250 μm. Material Excess Accessible but Not Removable. Negative Steps > 250 μm and Reparable | Secondary Caries, Large Gaps, Large Overhangs. Apical Pathology. Fracture/Loss of Restoration or Tooth | |
|---|---|---|---|---|---|---|
| FMBT | Baseline | 30 (100.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) |
| 3 months | 30 (100.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | |
| 6 months | 30 (100.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | |
| 12 months | 30 (100.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | |
| CULT | Baseline | 29 (96.7%) | 0 (0.0%) | 1 (3.3%) | 0 (0.0%) | 0 (0.0%) |
| 3 months | 29 (96.7%) | 0 (0.0%) | 1 (3.3%) | 0 (0.0%) | 0 (0.0%) | |
| 6 months | 29 (96.7%) | 0 (0.0%) | 1 (3.3%) | 0 (0.0%) | 0 (0.0%) | |
| 12 months | 29 (96.7%) | 0 (0.0%) | 1 (3.3%) | 0 (0.0%) | 0 (0.0%) | |
| Marginal Discoloration No Marginal Staining | Minor Staining, Easily Removable | Moderate Staining between Restoration and Tooth | Surface Staining Recognizable from Speaking Distance. or Severe Localized Marginal Staining Not Removable by Polishing | Significant (Detectable) Marginal Staining between Restoration and Tooth | ||
|---|---|---|---|---|---|---|
| FMBT | Baseline | 30 (100.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) |
| 3 months | 30 (100.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | |
| 6 months | 30 (100.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | |
| 12 months | 28 (93.3%) | 2 (6.7%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | |
| CULT | Baseline | 30 (100.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) |
| 3 months | 30 (100.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | |
| 6 months | 27 (90.0%) | 3 (10.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | |
| 12 months | 26 (86.7%) | 4 (13.3%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hardan, L.; Sidawi, L.; Akhundov, M.; Bourgi, R.; Ghaleb, M.; Dabbagh, S.; Sokolowski, K.; Cuevas-Suárez, C.E.; Lukomska-Szymanska, M. One-Year Clinical Performance of the Fast-Modelling Bulk Technique and Composite-Up Layering Technique in Class I Cavities. Polymers 2021, 13, 1873. https://doi.org/10.3390/polym13111873
Hardan L, Sidawi L, Akhundov M, Bourgi R, Ghaleb M, Dabbagh S, Sokolowski K, Cuevas-Suárez CE, Lukomska-Szymanska M. One-Year Clinical Performance of the Fast-Modelling Bulk Technique and Composite-Up Layering Technique in Class I Cavities. Polymers. 2021; 13(11):1873. https://doi.org/10.3390/polym13111873
Chicago/Turabian StyleHardan, Louis, Layla Sidawi, Murad Akhundov, Rim Bourgi, Maroun Ghaleb, Sarah Dabbagh, Krzysztof Sokolowski, Carlos Enrique Cuevas-Suárez, and Monika Lukomska-Szymanska. 2021. "One-Year Clinical Performance of the Fast-Modelling Bulk Technique and Composite-Up Layering Technique in Class I Cavities" Polymers 13, no. 11: 1873. https://doi.org/10.3390/polym13111873
APA StyleHardan, L., Sidawi, L., Akhundov, M., Bourgi, R., Ghaleb, M., Dabbagh, S., Sokolowski, K., Cuevas-Suárez, C. E., & Lukomska-Szymanska, M. (2021). One-Year Clinical Performance of the Fast-Modelling Bulk Technique and Composite-Up Layering Technique in Class I Cavities. Polymers, 13(11), 1873. https://doi.org/10.3390/polym13111873