
Effect of Fiber Reinforcement Type on the Performance of Large Posterior Restorations: A Review of In Vitro Studies

 ,
,  ,
, 

Abstract
: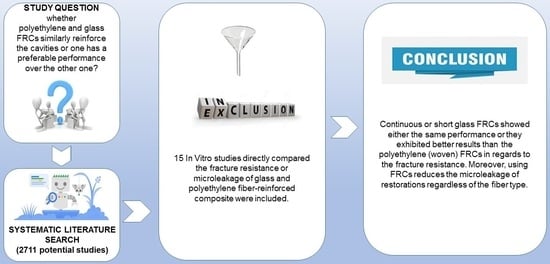
1. Introduction
2. Materials and Methods
2.1. Search Strategy and Data Collection Process
2.2. Eligibility Criteria
2.3. Selection Process
2.4. Data Synthesis
2.5. Quality Assessment
3. Results
4. Discussion
4.1. Fracture Resistance
4.2. Microleakage and Marginal Adaptation
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Soares, P.V.; Santos-Filho, P.C.; Martins, L.R.; Soares, C.J. Influence of restorative technique on the biomechanical behavior of endodontically treated maxillary premolars. Part I: Fracture resistance and fracture mode. J. Prosthet. Dent. 2008, 99, 30–37. [Google Scholar] [CrossRef]
- Hannig, C.; Westphal, C.; Becker, K.; Attin, T. Fracture resistance of endodontically treated maxillary premolars restored with CAD/CAM ceramic inlays. J. Prosthet. Dent. 2005, 94, 342–349. [Google Scholar] [CrossRef] [PubMed]
- Garoushi, S.; Vallittu, P.; Watts, D.C.; Lassila, L.V. Polymerization shrinkage of experimental short glass fiber-reinforced composite with semi-inter penetrating polymer network matrix. Dent. Mater. 2008, 24, 211–215. [Google Scholar] [CrossRef]
- Sáry, T.; Garoushi, S.; Braunitzer, G.; Alleman, D.; Volom, A.; Fráter, M. Fracture behaviour of MOD restorations reinforced by various fibre-reinforced techniques—An in vitro study. J. Mech. Behav. Biomed. Mater. 2019, 98, 348–356. [Google Scholar] [CrossRef] [Green Version]
- Braga, R.R.; Boaro, L.C.; Kuroe, T.; Azevedo, C.L.; Singer, J.M. Influence of cavity dimensions and their derivatives (volume and ’C’ factor) on shrinkage stress development and microleakage of composite restorations. Dent. Mater. 2006, 22, 818–823. [Google Scholar] [CrossRef]
- Dyer, S.; Lassila, L.; Vallittu, P. Effect of cross-sectional design on modulus of elasticity and toughness of fiber-reinforced composite materials. J. Prosthet. Dent. 2005, 94, 219–226. [Google Scholar] [CrossRef]
- Belli, S.; Erdemir, A.; Ozcopur, M.; Eskitascioglu, G. The effect of fibre insertion on fracture resistance of root filled molar teeth with MOD preparations restored with composite. Int. Endod. J. 2005, 38, 73–80. [Google Scholar] [CrossRef]
- Garlapati, T.G.; Krithikadatta, J.; Natanasabapathy, V. Fracture resistance of endodontically treated teeth restored with short fiber composite used as a core material-An in vitro study. J. Prosthodont. Res. 2017, 61, 464–470. [Google Scholar] [CrossRef]
- Belli, S.; Orucoglu, H.; Yildirim, C.; Eskitascioglu, G. The effect of fiber placement or flowable resin lining on microleakage in Class II adhesive restorations. J. Adhes. Dent. 2007, 9, 175–181. [Google Scholar]
- El-Mowafy, O.; El-Badrawy, W.; Eltanty, A.; Abbasi, K.; Habib, N. Gingival microleakage of Class II resin composite restorations with fiber inserts. Oper. Dent. 2007, 32, 298–305. [Google Scholar] [CrossRef]
- Ozel, E.; Soyman, M. Effect of fiber nets, application techniques and flowable composites on microleakage and the effect of fiber nets on polymerization shrinkage in class II MOD cavities. Oper. Dent. 2009, 34, 174–180. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tuloglu, N.; Bayrak, S.; Tunc, E.S. Different clinical applications of bondable reinforcement Ribbond in pediatric dentistry. Eur. J. Dent. 2009, 3, 329–334. [Google Scholar] [CrossRef] [Green Version]
- Vallittu, P.K. Ultra-high-modulus polyethylene ribbon as reinforcement for denture polymethyl methacrylate: A short communication. Dent. Mater. 1997, 13, 381–382. [Google Scholar] [CrossRef]
- Lastumaki, T.M.; Kallio, T.T.; Vallitu, P.K. The bond strength of light-curing composite resin to finally polymerized and aged glass fiber-reinforced composite substrate. Biomaterials 2002, 23, 4533–4639. [Google Scholar] [CrossRef]
- Belli, S.; Erdemir, A.; Yildirim, C. Reinforcement effect of polyethylene fibre in root-filled teeth: Comparison of two restoration techniques. Int. Endod. J. 2006, 39, 136–142. [Google Scholar] [CrossRef]
- Deliperi, S.; Bardwell, D.N.; Coiana, C. Reconstruction of devital teeth using direct fiber-reinforced composite resins: A case report. J. Adhes. Dent. 2005, 7, 165–171. [Google Scholar]
- Rudo, D.N.; Karbhari, V.M. Physical behaviors of fiber reinforcement as applied to tooth stabilization. Dent. Clin. N. Am. 1999, 43, 7–35. [Google Scholar]
- Visser, H.J.; Brandt, P.D.; de Wet, F.A. Fracture strength of cusp-replacing fibre-strengthened composite restorations. SADJ 2014, 69, 204–207. [Google Scholar]
- Vallittu, P. Flexural properties of acrylic polymers reinforced with unidirectional and woven glass fibers. J. Prosthet. Dent. 1999, 81, 318–326. [Google Scholar] [CrossRef]
- Vallittu, P. Strength and interfacial adhesion of FRC-tooth system. In Proceedings of the Second International Symposium on Fibre-Reinforced Plastics in Dentistry, Nijmegen, The Netherlands, 13 October 2001. [Google Scholar]
- Garoushi, S.; Vallittu, P.; Lassila, L. Short glass fiber reinforced restorative composite resin with semi-inter penetrating polymer network matrix. Dent. Mater. 2007, 23, 1356–1362. [Google Scholar] [CrossRef]
- Garoushi, S.; Mangoush, E.; Vallittu, P.; Lassila, L. Short fiber reinforced composite: A new alternative for direct onlay restorations. Open Dent. J. 2013, 30, 181–185. [Google Scholar] [CrossRef] [Green Version]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 29, 372. [Google Scholar]
- Bourgi, R.; Hardan, L.; Rivera-Gonzaga, A.; Cuevas-Suárez, C.E. Effect of warm-air stream for solvent evaporation on bond strength of adhesive systems: A systematic review and meta-analysis of in vitro studies. Int. J. Adhes. Adhes. 2021, 105, 102794. [Google Scholar] [CrossRef]
- Zarow, M.; Dominiak, M.; Szczeklik, K.; Hardan, L.; Bourgi, R.; Cuevas-Suárez, C.E.; Zamarripa-Calderón, J.E.; Kharouf, N.; Filtchev, D. Effect of composite core materials on fracture resistance of endodontically treated teeth: A systematic review and meta-analysis of in vitro studies. Polymers 2021, 9, 2251. [Google Scholar] [CrossRef]
- Hiremath, H.; Kulkarni, S.; Hiremath, V.; Kotipalli, M. Evaluation of different fibers and biodentine as alternates to crown coverage for endodontically treated molars: An in vitro study. J. Conserv. Dent. 2017, 20, 72–75. [Google Scholar] [CrossRef] [PubMed]
- Sah, S.P.; Datta, K.; Velmurugan, N.; Lakshmanan, G.; Karthik, L. Evaluation of Fracture Resistance of Endodontically Treated Maxillary Premolars Restored with Three Different Core Materials: An In Vitro Study. Int. J. Oral Health Med. Res. 2018, 5, 31–36. [Google Scholar]
- Kemaloglu, H.; Kaval, M.E.; Turkun, M.; Kurt, S.M. Effect of novel restoration techniques on the fracture resistance of teeth treated endodontically: An in vitro study. Dent. Mater. J. 2015, 34, 618–622. [Google Scholar] [CrossRef] [Green Version]
- Tekçe, N.; Pala, K.; Tuncer, S.; Demirci, M.; Serim, M.E. Influence of polymerisation method and type of fibre on fracture strength of endodontically treated teeth. Aust. Endod. J. 2017, 43, 115–122. [Google Scholar] [CrossRef]
- Khan, S.; Ramachandran, A.; Alfadley, A.; Baskaradoss, J.K. Ex vivo fracture resistance of teeth restored with glass and fiber reinforced composite resin. J. Mech. Behav. Biomed. Mater. 2018, 82, 235–238. [Google Scholar] [CrossRef]
- Ozsevik, A.S.; Yildirim, C.; Aydin, U.; Culha, E.; Surmelioglu, D. Effect of fibre-reinforced composite on the fracture resistance of endodontically treated teeth. Aust. Endod. J. 2016, 42, 82–87. [Google Scholar] [CrossRef]
- Shah, S.; Shilpa-Jain, D.P.; Velmurugan, N.; Sooriaprakas, C.; Krithikadatta, J. Performance of fibre reinforced composite as a post-endodontic restoration on different endodontic cavity designs- an in-vitro study. J. Mech. Behav. Biomed. Mater. 2020, 104, 103650. [Google Scholar] [CrossRef]
- Basavanna, R.; Garg, A.; Kapur, R. Evaluation of gingival microleakage of class II resin composite restorations with fiber inserts: An in vitro study. J. Conserv. Dent. 2012, 15, 166–169. [Google Scholar] [CrossRef]
- Ahmed, W.; El-Badrawy, W.; Kulkarni, G.; Prakki, A.; El-Mowafy, O. Gingival microleakage of class V composite restorations with fiber inserts. J. Contemp. Dent. Pract. 2013, 1, 622–628. [Google Scholar] [CrossRef]
- Kumar, M.; Bharath, M.J.; Sahadev, C.K.; Sandeep, R.; Santhosh, P.S.; George, V.M. Evaluation of gingival microleakage of composite restorations with glass fiber inserts, polyethylene fiber inserts and prepolymerized composite inserts: An in vitro study. IMP. J. Interdiscip. Res. 2016, 2, 627–630. [Google Scholar]
- Garoushi, S.; Lassila, L.; Vallittu, P.K. Fiber-reinforced Composite in Clinical Dentistry. Chin. J. Dent. Res. 2009, 12, 7–14. [Google Scholar]
- Mangoush, E.; Säilynoja, E.; Prinssi, R.; Lassila, L.; Vallittu, P.; Garoushi, S. Comparative evaluation between glass and polyethylene fiber reinforced composites: A review of the current literature. J. Clin. Exp. Dent. 2017, 9, 1408–1417. [Google Scholar] [CrossRef] [PubMed]
- Vallittu, P. Glass fiber reinforcement in repaired acrylic resin removable dentures: Preliminary results of a clinical study. Quintessence Int. 1997, 28, 39–44. [Google Scholar]
- Sengun, A.; Cobankara, F.K.; Orucoglu, H. Effect of a new restoration technique on fracture resistance of endodontically treated teeth. Dent. Traumatol. 2008, 24, 214–219. [Google Scholar] [CrossRef] [PubMed]
- Fráter, M.; Forster, A.; Keresztúri, M.; Braunitzer, G.; Nagy, K. In vitro fracture resistance of molar teeth restored with a short fiber-reinforced composite material. J. Dent. 2014, 42, 1143–1150. [Google Scholar] [CrossRef] [PubMed]
- Belli, S.; Dönmez, N.; Eskitaşcioğlu, G. The effect of c-factor and flowableresin or fiber use at the interface on microtensile bond strength to dentin. J. Adhesiv. Dent. 2006, 8, 247–253. [Google Scholar]
- Garoushi, S.; Vallittu, P.; Lassila, L. Fracture resistance of short, randomly oriented, glass fiber-reinforced composite premolar crowns. Sep. Acta Biomater. 2007, 3, 779–784. [Google Scholar] [CrossRef]
- Garoushi, S.; Vallittu, P.; Lassila, L. Direct restoration of severely damaged incisors using short fiber-reinforced composite resin. J. Dent. 2007, 35, 731–736. [Google Scholar] [CrossRef] [PubMed]
- Garoushi, S.; Lassila, L.; Tezvergil, A.; Vallittu, P. Load bearing capacity of fibre-reinforced and particulate filler composite resin combination. Mar. J. Dent. 2005, 34, 179–184. [Google Scholar] [CrossRef]
- Lassila, L.; Garoushi, S.; Vallittu, P.; Säilynoja, E. Mechanical properties of fiber reinforced restorative composite with two distinguished fiber length distribution. J. Mech. Behav. Biomed. Mater. 2016, 60, 331–338. [Google Scholar] [CrossRef] [PubMed]
- Vallittu, P.; Lassila, L.; Lappalainen, R. Transverse strength and fatigue of denture acrylic-glass fiber composite. Dent. Mater. 1994, 10, 116–121. [Google Scholar] [CrossRef]
- Foek, D.L.; Ozcan, M.; Krebs, E.; Sandham, A. Adhesive properties of bonded orthodontic retainers to enamel: Stainless steel wire vs. fiber-reinforced composites. J. Adhes. Dent. 2009, 11, 381–390. [Google Scholar] [PubMed]
- Kolbeck, C.; Rosentritt, M.; Behr, M.; Lang, R.; Handel, G. In vitro study of fracture strength and marginal adaptation of polyethylene-fibre-reinforced-composite versus glass-fibre reinforced-composite fixed partial dentures. J. Oral Rehabil. 2002, 29, 668–674. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| Study | Tested Parameter | Control Group | Type of Compared FRCs | FRCs Application Technique | Main Conclusion |
|---|---|---|---|---|---|
| Kmaloglu [28] | Fracture strength | MOD cavities of ETT restored with composite with no fiber reinforcement | Ribbond (Ribbond Inc., Seattle, WA, USA) and everX Posterior (GC Europe, Leuven, Belgium) | Ribbond was placed on the cavity floor BL; everX Posterior applied using bulk-fill (3 mm) technique. | Fiber reinforcement increased the fracture strength of teeth with large MOD cavities endodontically treated when compared to bulk-fill and nano-hybrid resin composites. |
| Ozsevik [31] | Fracture resistance | MOD cavities of ETT restored with composite with no fiber reinforcements | Ribbond and everX Posterior | Ribbond was placed on the cavity floor BL; everX Posterior applied using bulk-fill technique. | Using everX posterior under composite restorations resulted in fracture resistance similar to that of intact teeth. Furthermore, it reinforced root-filled teeth more than composite alone and ribbon and composite restorations. |
| Tekçe [29] | Fracture strength | No control | Ribbond and everX Posterior | Ribbond was placed on the cavity floor BL; everX Posterior applied using bulk-fill technique. | The polyethylene ribbon fibre-reinforced composite groups displayed similar fracture strength results with those of the short fibre-reinforced composite everX Posterior group. |
| Garlapati [8] | Fracture resistance | MOD cavities of ETT restored with composite with no fiber reinforcements | Ribbond and everX Posterior | Ribbond was placed on the cavity floor BL; everX Posterior applied using incremental technique. | Among the materials tested, endodontically treated teeth restored with everX posterior fiber reinforced composite showed superior fracture resistance. |
| Hiremath [26] | Fracture resistance | No control | Ribbond and everX Posterior | Ribbond was placed circumferentially against the entire inner surfaces; everX Posterior applied using bulk-fill technique. | Both FRC and polyethylene fibers (Ribbond) could be considered as an alternate to crown coverage, considering the insignificant difference in the values of fracture resistance when compared to that of natural tooth. |
| Khan [30] | Fracture resistance | MOD cavity of ETT restored with composite with no fiber reinforcements | Ribbond, everStick C&B (Stick Tech, GC member, Turku, Finland), Dentapreg (UFM, ADM AS, Brno, Czech Republic), and Bioctris fibers (Bio Composants Medicaux, Tullins, France) | Ribbond was placed on the cavity floor BL; two pieces of everStick C&B coated the cavity surface; Dentapreg coated the cavity surface; Bioctris coated the cavity surface. | Among the different fibers tested, Everstick and Bioctris demonstrated the highest fracture resistance. Thus, it can be inferred that E-glass system is able to reinforce teeth better than S2 glass or Polyethylene fibers. |
| Sah [27] | Fracture resistance | MOD cavities of ETT restored with composite with no fiber reinforcements | Ribbond and everX Posterior | Ribbond was placed on the cavity floor BL; everX Posterior applied using bulk-fill (3 mm) technique. | The mean load to fracture was highest for EverX posterior followed by Ribbond and Conventional Composite for different cavity configuration. |
| Sáry [4] | Fracture resistance | MOD cavities restored with composite with no fiber reinforcements | Ribbond, everX Posterior, and everStick NET (Stick Tech, GC member, Turku, Finland) | Ribbond was placed either on the base BL, on the top, as an occlusal splint, circumferentially or transcoronaly; everX Posterior applied using bulk-fill technique; everStick NET was applied with everX Posterior either on the cavity base BL, on the top BL, as an occlusal splint or circumferentially inside the cavity. | Incorporating polyethylene or a combination of short and bidirectional glass fibres in certain positions in direct restorations seems to be able to restore the fracture resistance of sound molar teeth. |
| Shah [32] | Fracture resistance | Cavities of ETT restored with composite with no fiber reinforcements | Ribbond and everX Posterior | Ribbond was placed on the cavity floor BL; everX Posterior applied using incremental technique. | Fibre reinforced composites when used in different cavity configurations of endodontically treated premolar yielded similar results. |
| Belli [9] | Microleakage | Class II cavities restored with composite with no fiber reinforcement | Ribbond and everX Posterior | Ribbond was placed on the cavity floor BL; everStick NET was placed on cavity floor | The use of flowable composite alone or in combination with polyethylene or glass fibers helps reduce occlusal leakage in class II adhesive cavities with enamel margins. |
| El. Mowafy [10] | Microleakage | Class II cavities restored with composite with no fiber reinforcement | Ribbond and everStick Post 0.9 mm (Stick Tech oy, GC member, Turku, Finland) | Ribbond was placed on the gingival floor; everStick Post was placed on the gingival floor. | The use of fiber inserts significantly reduced microleakage in Class II resin composite restorations with gingival margins on the root surface. |
| Ozel [11] | Microleakage and polymerization shrinkage | Class II cavities restored with composite with no fiber reinforcements | Ribbond and everStick NET | Ribbond was applied on the gingival and axial wall; everStick NET was applied on the gingival and axial wall. | Fiber nets in general decreased both microleakage and polymerization shrinkage. |
| Basavanna [33] | Microleakage | Class II cavities restored with composite with no fiber reinforcements | Ribbond and everStick NET | Ribbond was placed on the gingival floor; everStick NET was placed on the gingival floor. | The use of fiber inserts significantly reduces microleakage in class II resin composite restorationswith gigngival margins on the root surface, with no significant difference between the different fiber inserts groups. |
| Ahmed [34] | Microleakage | Class V cavities restored with composite with no fiber reinforcements | Ribbond and everStick Post 0.9 mm | Ribbond was positioned into the restoration at the gingival seat after polymerization of the first increment and before the application of the second increment; everStick Post was positioned as previously done with Ribbond. | Class V resin composite restorations bonded with a total etch adhesive had a significant reduction in mean microleakage scores when glass or polyethylene fibers were placed at the gingival cavo-surface margin |
| Kumar [35] | Microleakage | Class II cavities restored with composite with no fiber reinforcements | Ribbond and everStick NET | Ribbond was placed on the gingival floor; everStick NET was placed on the gingival floor. | Polyethylene fiber inserts group exhibited less reduction in microleakage when compared to Glass fiber inserts and Prepolymerized Composite fiber inserts. |
| Studies Evaluated | Control Group | Standardized Samples | Randomized Samples | Single Operator | Manufacture’s Instructions | Operator Blindness | Sample Size Calculation | Failure-mode Evaluation | Risk of Bias |
|---|---|---|---|---|---|---|---|---|---|
| Kemaloglu [28] | YES | YES | YES | NO | YES | NO | NO | YES | Medium |
| Ozsevik [31] | YES | YES | YES | NO | YES | NO | YES | NO | Medium |
| Tekce [29] | NO | YES | NO | NO | YES | NO | NO | YES | High |
| Garlapati [8] | YES | YES | YES | NO | YES | NO | NO | YES | Medium |
| Hiremath [26] | NO | YES | YES | NO | NO | NO | NO | NO | High |
| Khan [30] | YES | YES | NO | NO | YES | NO | NO | NO | High |
| Sah [27] | YES | YES | YES | NO | YES | NO | NO | YES | Medium |
| Sáry [4] | YES | YES | YES | YES | YES | NO | NO | YES | Medium |
| Shah [32] | YES | YES | NO | NO | YES | NO | NO | YES | Medium |
| Belli [9] | YES | YES | YES | NO | YES | YES | NO | NA | Medium |
| El. Mowafy [10] | YES | YES | YES | YES | NO | NO | NO | NA | Medium |
| Ozel [11] | YES | YES | YES | YES | YES | NO | NO | NA | Medium |
| Basavanna [33] | YES | YES | YES | NO | YES | NO | NO | NA | Medium |
| Ahmed [34] | YES | YES | YES | YES | YES | NO | NO | NA | Medium |
| Kumar [35] | YES | YES | YES | NO | YES | NO | NO | NA | Medium |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mangoush, E.; Garoushi, S.; Lassila, L.; Vallittu, P.K.; Säilynoja, E. Effect of Fiber Reinforcement Type on the Performance of Large Posterior Restorations: A Review of In Vitro Studies. Polymers 2021, 13, 3682. https://doi.org/10.3390/polym13213682
Mangoush E, Garoushi S, Lassila L, Vallittu PK, Säilynoja E. Effect of Fiber Reinforcement Type on the Performance of Large Posterior Restorations: A Review of In Vitro Studies. Polymers. 2021; 13(21):3682. https://doi.org/10.3390/polym13213682
Chicago/Turabian StyleMangoush, Enas, Sufyan Garoushi, Lippo Lassila, Pekka K. Vallittu, and Eija Säilynoja. 2021. "Effect of Fiber Reinforcement Type on the Performance of Large Posterior Restorations: A Review of In Vitro Studies" Polymers 13, no. 21: 3682. https://doi.org/10.3390/polym13213682
APA StyleMangoush, E., Garoushi, S., Lassila, L., Vallittu, P. K., & Säilynoja, E. (2021). Effect of Fiber Reinforcement Type on the Performance of Large Posterior Restorations: A Review of In Vitro Studies. Polymers, 13(21), 3682. https://doi.org/10.3390/polym13213682