
Shear Bond Strength of Veneered Zirconia Repaired Using Various Methods and Adhesive Systems: A Comparative Study

 , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
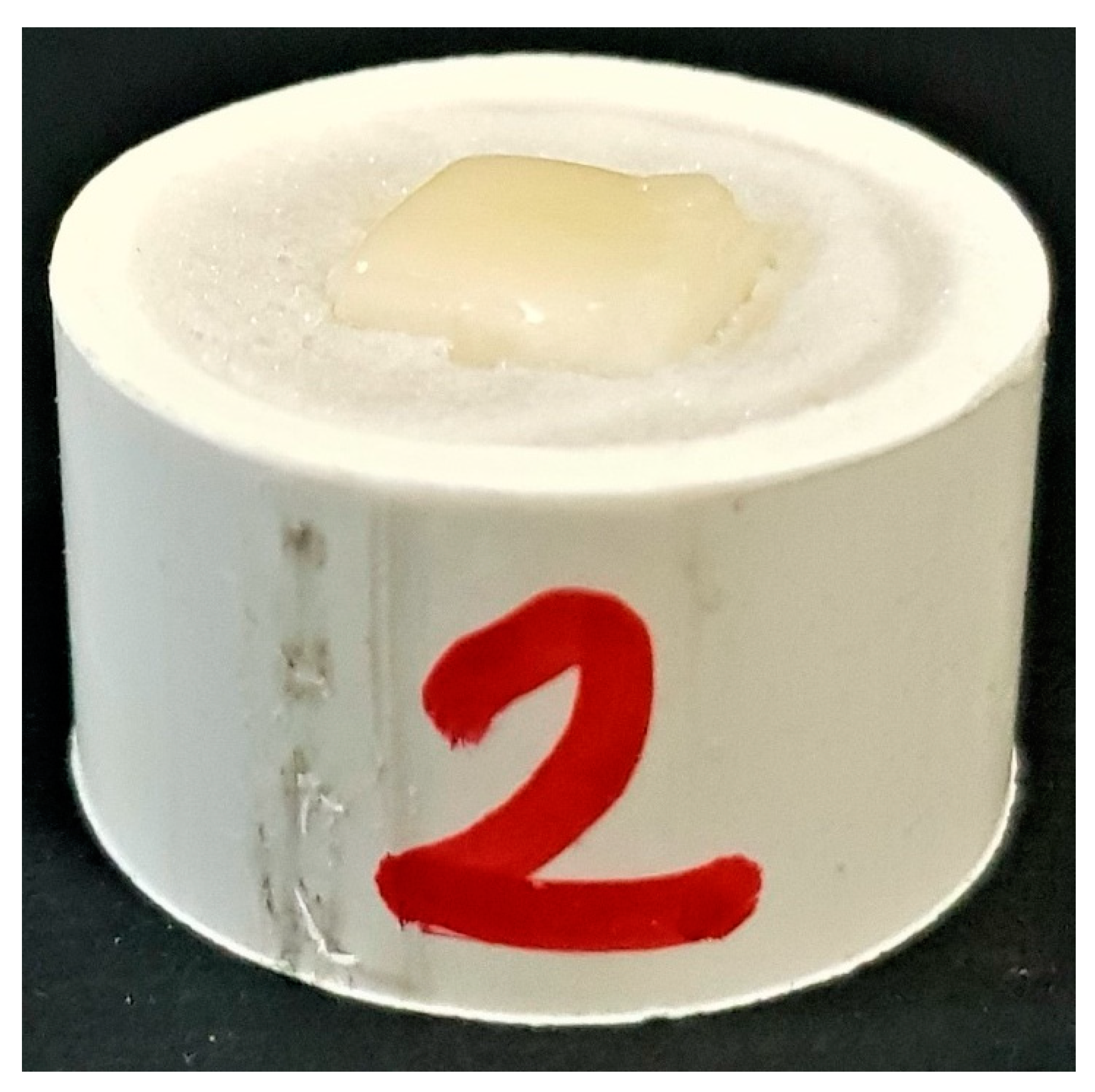
2.1. Zirconia Block Preparation
2.2. Veneering Porcelain Application
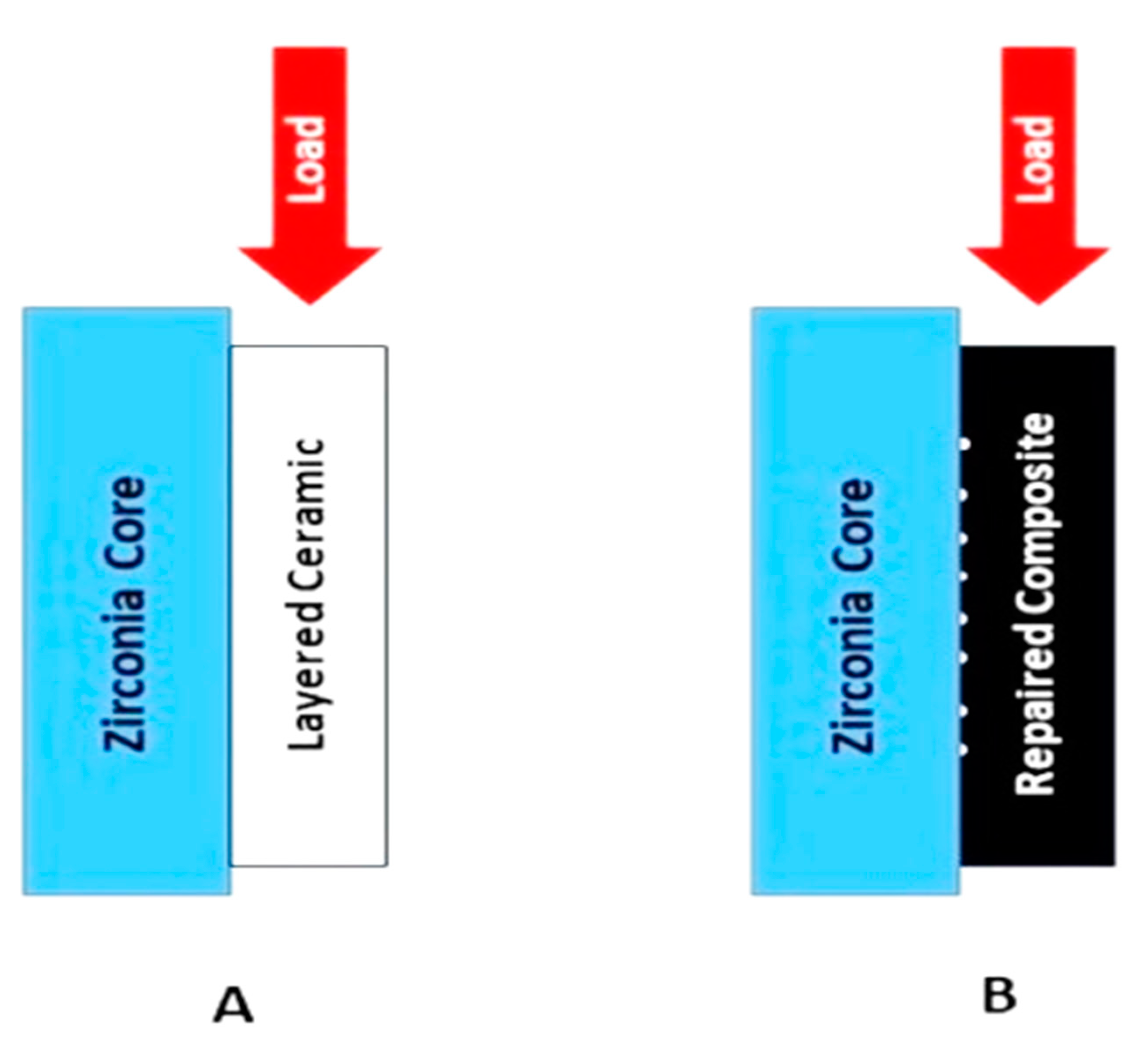
2.3. Shear Bond Strength Testing of The Specimens With Ceramic Built Up
2.4. Thermocycling of Specimens
2.5. Application of the Porcelain Repair System
2.6. Shear Bond Strength Testing of the Specimens with Composite Built Up
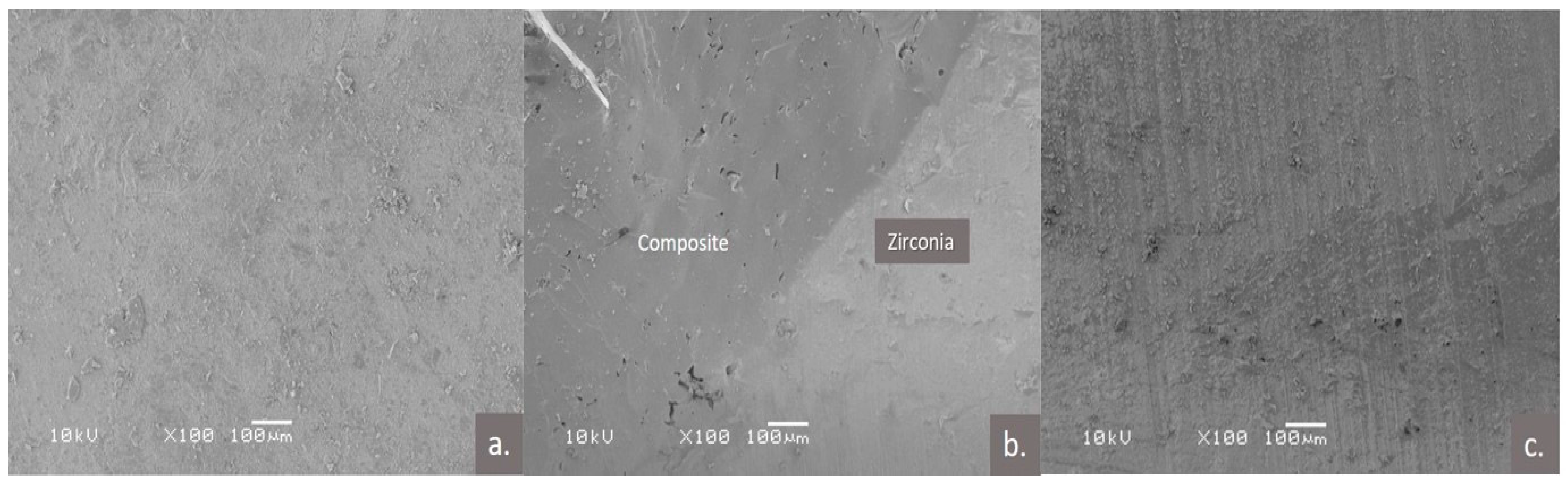
2.7. Scanning Electron Microscopic Examination
2.8. Data Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Brunton, P.A.; Ratnayake, J.; Loch, C.; Veerasamy, A.; Cathro, P.; Lee, R. Indirect restorations and fixed prosthodontics: Materials and techniques used by general dentists of New Zealand. Int. J. Dent. 2019, 2019, 5210162. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Varlan, C.; Dimitriu, B.; Varlan, V.; Bodnar, D.; Suciu, I. Current opinions concerning the restoration of endodontically treated teeth: Basic principles. J. Med. Life. 2009, 2, 165–172. [Google Scholar]
- Carvalho, M.A.D.; Lazari, P.C.; Gresnigt, M.; Del Bel Cury, A.A.; Magne, P. Current options concerning the endodontically-treated teeth restoration with the adhesive approach. Braz. Oral Res. 2018, 32, 147–158. [Google Scholar] [CrossRef] [Green Version]
- Madfa, A.A.; Al-Sanabani, F.A.; Al-Qudami, N.H.; Al-Sanabani, J.S.; Amran, A.G. Use of zirconia in dentistry: An overview. Open Biomater. J. 2014, 5, 1–7. [Google Scholar] [CrossRef]
- Daou, E.E. The zirconia ceramic: Strengths and weaknesses. Open Dent. J. 2014, 8, 33–42. [Google Scholar] [CrossRef] [PubMed]
- Ghodsi, S.; Jafarian, Z. A Review on Translucent Zirconia. Eur. J. Prosthodont. Restor. Dent. 2018, 26, 62–74. [Google Scholar] [PubMed]
- Urapepon, S.; Taenguthai, P. The effect of zirconia framework design on the failure of all-ceramic crown under static loading. J. Adv. Prosthodont. 2015, 7, 146–150. [Google Scholar] [CrossRef] [Green Version]
- Konstantinidis, I.; Trikka, D.; Gasparatos, S.; Mitsias, M.E. Clinical outcomes of monolithic zirconia crowns with CAD/CAM technology. a 1-year follow-up prospective clinical study of 65 patients. Int. J. Environ. Res. Public Health 2018, 15, 2523. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Worni, A.; Katsoulis, J.; Kolgeci, L.; Worni, M.; Mericske-Stern, R. Monolithic zirconia reconstructions supported by teeth and implants: 1-to 3-year results of a case series. Quintessence Int. 2017, 48, 459–467. [Google Scholar]
- Konstantinidis, I.K.; Jacoby, S.; Rädel, M.; Böning, K. Prospective evaluation of zirconia based tooth-and implant-supported fixed dental prostheses: 3-year results. J. Dent. 2015, 43, 87–93. [Google Scholar] [CrossRef]
- Pihlaja, J.; Näpänkangas, R.; Raustia, A. Early complications and short-term failures of zirconia single crowns and partial fixed dental prostheses. J. Prosthet. Dent. 2014, 112, 778–783. [Google Scholar] [CrossRef]
- Raigrodski, A.J.; Hillstead, M.B.; Meng, G.K.; Chung, K. Survival and complications of zirconia-based fixed dental prostheses: A systematic review. J. Prosthet. Dent. 2012, 107, 170–177. [Google Scholar] [CrossRef]
- Macura, A.; Kasperski, J.; Urbaniak, M.; Klimek, A. Materials and methods used for repairing damaged veneering porcelain in permanent complex prosthetic restorations-review of literature. J. Stoma 2013, 66, 221–230. [Google Scholar] [CrossRef]
- Kimmich, M.; Stappert, C.F. Intraoral treatment of veneering porcelain chipping of fixed dental restorations: A review and clinical application. J. Am. Dent. Assoc. 2013, 144, 31–44. [Google Scholar] [CrossRef] [Green Version]
- Lee, S.J.; Cheong, C.W.; Wright, R.F.; Chang, B.M. Bond strength of the porcelain repair system to all-ceramic copings and porcelain. J. Prosthodont. 2014, 23, 112–116. [Google Scholar] [CrossRef] [PubMed]
- Mumcu, E.; Erdemir, U.; Özsoy, A.; Tekbas-Atay, M.; Özcan, M. Effect of surface conditioning methods on the microtensile bond strength of repair composite to indirect restorative materials. J. Adhes. Sci. Technol. 2019, 33, 2369–2384. [Google Scholar] [CrossRef]
- Gargari, M.; Gloria, F.; Napoli, E.; Pujia, A.M. Zirconia: Cementation of prosthetic restorations. Literature review. Oral Implantol. 2010, 3, 25–29. [Google Scholar]
- Agingu, C.; Zhang, C.; Jiang, N.; Cheng, H.; Özcan, M.; Yu, H. Intraoral repair of chipped or fractured veneered zirconia crowns and fixed dental prosthesis: Clinical guidelines based on literature review. J. Adhes. Sci. Technol. 2018, 32, 1711–1723. [Google Scholar] [CrossRef]
- Layton, D. A critical appraisal of the survival and complication rates of tooth-supported all-ceramic and metal-ceramic fixed dental prostheses: The application of evidence-based dentistry. Int. J. Prosthodont. 2011, 24. [Google Scholar]
- Pjetursson, B.E.; Sailer, I.; Zwahlen, M.; Hämmerle, C.H. A systematic review of the survival and complication rates of all-ceramic and metal–ceramic reconstructions after an observation period of at least 3 years. Part I: Single crowns. Clin. Oral Implant. Res. 2007, 18, 73–85. [Google Scholar] [CrossRef]
- Komine, F.; Strub, J.R.; Matsumura, H. Bonding between layering materials and zirconia frameworks. Jpn. Dent. Sci. Rev. 2012, 48, 153–161. [Google Scholar] [CrossRef] [Green Version]
- Aboushelib, M.N.; Kleverlaan, C.J.; Feilzer, A.J. Effect of zirconia type on its bond strength with different veneer ceramics. J. Prosthodont. 2008, 17, 401–408. [Google Scholar] [CrossRef]
- Saito, A.; Komine, F.; Blatz, M.B.; Matsumura, H. A comparison of bond strength of layered veneering porcelains to zirconia and metal. J. Prosthet. Dent. 2010, 104, 247–257. [Google Scholar] [CrossRef]
- Passia, N.; Mitsias, M.; Lehmann, F.; Kern, M. Bond strength of a new generation of universal bonding systems to zirconia ceramic. J. Mech. Behav. Biomed. Mater. 2016, 62, 268–274. [Google Scholar] [CrossRef] [PubMed]
- Reston, E.; Filho, S.; Arossi, G.; Cogo, R.B.; Rocha, C.; Closs, L. Repairing ceramic restorations: Final solution or alternative procedure? Oper. Dent. 2008, 33, 461–466. [Google Scholar] [CrossRef]
- Özcan, M.; Van Der Sleen, J.M.; Kurunmäki, H.; Vallittu, P.K. Comparison of repair methods for ceramic-fused-to-metal crowns. J. Prosthodont. 2006, 15, 283–288. [Google Scholar] [CrossRef] [PubMed]
- Wady, A.F.; Paleari, A.G.; Queiroz, T.P.; Margonar, R. Repair technique for fractured implant-supported metal-ceramic restorations: A clinical report. J. Oral Implantol. 2014, 40, 589–592. [Google Scholar] [CrossRef] [PubMed]
- Han, I.; Kang, D.; Chung, C.; Choe, H.; Son, M. Effect of various intraoral repair systems on the shear bond strength of composite resin to zirconia. J. Adv. Prosthodont. 2013, 5, 248–255. [Google Scholar] [CrossRef] [Green Version]
- Carvalho, R.M.; Manso, A.P.; Geraldeli, S.; Tay, F.R.; Pashley, D.H. Durability of bonds and clinical success of adhesive restorations. Dent. Mater. 2012, 28, 72–86. [Google Scholar] [CrossRef] [Green Version]
- Yoo, J.; Yoon, H.; Park, J.; Park, E. Porcelain repair-Influence of different systems and surface treatments on resin bond strength. J. Adv. Prosthodont. 2015, 7, 343–348. [Google Scholar] [CrossRef] [Green Version]
- Silva, N.R.; Thompson, V.P.; Valverde, G.B.; Coelho, P.G.; Powers, J.M.; Farah, J.W.; Esquivel-Upshaw, J. Comparative reliability analyses of zirconium oxide and lithium disilicate restorations in vitro and in vivo. J. Am. Dent. Assoc. 2011, 142, 4S–9S. [Google Scholar] [CrossRef] [PubMed]
- Sailer, I.; Feher, A.; Filser, F.; Luthy, H.; Gauckler, L.J.; Scharer, P.; Hammerle, C.F. Prospective clinical study of zirconia posterior fixed partial dentures: 3-year follow-up. Quintessence Int. -Engl. Ed. 2006, 37, 685–693. [Google Scholar]
- Sailer, I.; Feher, A.; Filser, F.; Gauckler, L.J.; Luthy, H.; Hammerle, C.H.F. Five-year clinical results of zirconia frameworks for posterior fixed partial dentures. Int. J. Prosthodont. 2007, 20, 151–156. [Google Scholar]
- Miura, S.; Kasahara, S.; Kudo, M.; Okuyama, Y.; Izumida, A.; Yoda, M.; Egusa, H.; Sasaki, K. Clinical Chipping of Zirconia All-ceramic Restorations; Interface Oral Health Science 2014; Springer: Tokyo, Japan, 2015; pp. 317–323. [Google Scholar]
- Chaiyabutr, Y.; McGowan, S.; Phillips, K.M.; Kois, J.C.; Giordano, R.A. The effect of hydrofluoric acid surface treatment and bond strength of a zirconia veneering ceramic. J. Prosthet. Dent. 2008, 100, 194–202. [Google Scholar] [CrossRef]
- Fischer, J.; Baltzer, N.; Fleetwood, P. Thermal creep analysis of noble metal alloys for the ceramic-fused-to-metal technique. J. Biomed. Mater. Res. Off. J. Soc. Biomater. Jpn. Soc. Biomater. Aust. Soc. Biomater. 1999, 48, 258–264. [Google Scholar] [CrossRef]
- Anusavice, K.; Carroll, J. Effect of incompatibility stress on the fit of metal-ceramic crowns. J. Dent. Res. 1987, 66, 1341–1345. [Google Scholar] [CrossRef] [PubMed]
- Sirisha, K.; Rambabu, T.; Ravishankar, Y.; Ravikumar, P. Validity of bond strength tests: A critical review-Part II. J. Conserv. Dent. 2014, 17, 420–426. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cristoforides, P.; Amaral, R.; May, L.; Bottino, M.; Valandro, L. Composite resin to yttria stabilized tetragonal zirconia polycrystal bonding: Comparison of repair methods. Oper. Dent. 2012, 37, 263–271. [Google Scholar] [CrossRef] [Green Version]
- Kirmali, O.; Barutcigil, Ç.; Ozarslan, M.M.; Barutcigil, K.; Harorlı, O.T. Repair bond strength of composite resin to sandblasted and laser irradiated Y-TZP ceramic surfaces. Scanning 2015, 37, 186–192. [Google Scholar] [CrossRef]
- Blum, I.R.; Nikolinakos, N.; Lynch, C.D.; Wilson, N.H.; Millar, B.J.; Jagger, D.C. An in vitro comparison of four intra-oral ceramic repair systems. J. Dent. 2012, 40, 906–912. [Google Scholar] [CrossRef]
- Kim, B.; Bae, H.E.; Shim, J.; Lee, K. The influence of ceramic surface treatments on the tensile bond strength of composite resin to all-ceramic coping materials. J. Prosthet. Dent. 2005, 94, 357–362. [Google Scholar] [CrossRef] [PubMed]
- Afrasiabi, A.; Mostajir, E.; Golbari, N. The effect of Z-primer on the shear bond strength of zirconia ceramic to dentin: In vitro. J. Clin. Exp. Dent. 2018, 10, e661–e664. [Google Scholar] [CrossRef] [PubMed]
- Kitayama, S.; Nikaido, T.; Takahashi, R.; Zhu, L.; Ikeda, M.; Foxton, R.M.; Sadr, A.; Tagami, J. Effect of primer treatment on bonding of resin cements to zirconia ceramic. Dent. Mater. 2010, 26, 426–432. [Google Scholar] [CrossRef] [PubMed]
- Barragan, G.; Chasqueira, F.; Arantes-Oliveira, S.; Portugal, J. Ceramic repair: Influence of chemical and mechanical surface conditioning on adhesion to zirconia. Oral Health Dent. Manag. 2014, 13, 155–158. [Google Scholar]
- Kocaağaoğlu, H.H.; Gürbulak, A. An assessment of shear bond strength between ceramic repair systems and different ceramic infrastructures. Scanning 2015, 37, 300–305. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| S. No. | Groups | Material | Trade Name | Manufacturer | Lot Number |
|---|---|---|---|---|---|
| 1. | Zr | Zirconia | ZirCAD | Ivoclar Vivadent AG, Schaan/Liechhtenstein | X24851 |
| 2. | Cr | Ceramic | Ceram IPS e.max | Ivoclar Vivadent AG, Schaan/Liechhtenstein | X32767 |
| 3. | Group-A | Z-PRIMETM Plus, Porcelain primer, Porcelain bonding resin | Intra Oral repair Kit | Bisco, INC. 1100W. Irving Park Rd. Schauburg, U.S.A. | 81026A |
| 4. | Group-B | Tetric Evoceram Light curing nano-hybrid composite, Monobond Plus, Heliobond | Ceramic repair N | Ivoclar Vivadent AG, Schaan/Liechhtenstein | 90429A |
| 5. | Group-C | Ceramic bond I, Ceramic bond II | Signum | Kulzer GmbH, Hanau, Germany | X51289 |
| 6. | Group-D | Scotch bondTM | Scotch bondTM | 3M, St. Paul, MN | K654 |
| 7. | Group-E | Single bondTM | Single bondTM | 3M, St. Paul, MN | 1900004131 |
| Groups | Application Procedure |
|---|---|
| Group-A | Isolation of area to be repaired. Removal of glaze and bevel (45°) porcelain around the area to be repaired. Application of PORCELAIN ETCHANT (9.5% HF) for 90 s. Application of 1 coat of PORCELAIN PRIMER to the etched porcelain surface and allowing to dwell for 30 s. Air drying. Application 1 coat of Z-PRIME Plus to the exposed metal/zirconia/alumina and drying with an air syringe for 3–5 s. Application of a thin layer of PORCELAIN BONDING RESIN to the repair site. Spreading of composite evenly over the surface and light-curing. Completion of repair using composite and finishing/polishing. |
| Group-B | Isolation. Preparation of the defective ceramic surface. Application of Monobond N. and allowing to react for 60 s. Application of Heliobond, and light-curing for 10 s. Completion of the repair using composite and finishing/polishing. |
| Group-C | Preparation of the ceramic surface. Drying the surface thoroughly using oil-free air. Application of a thin layer of Signum ceramic bond I to the dust-free ceramic surface with a new brush or microbrush and allowing it to dry for about 10 s. Application of thin layer of Signum ceramic bond II and rub in for approx. 20–30 s—no light curing required! Composite build-up: Layer thickness <2 mm, light curing. |
| Group-D | Deglazing of the surface to be repaired. Application of the adhesive to the prepared tooth and rubbing it in for 20 s. Gently air-drying the adhesive for approximately 5 s to evaporate the solvent. Light curing for 10 s. Completion of repair using composite and finishing/polishing. |
| Group-E | Deglazing of the surface to be repaired. Application of the adhesive to the prepared tooth and rubbing it in for 20 s. Air drying the adhesive for about 5 s to evaporate the solvent. Light curing for 10 s. Completion of repair using composite and finishing/polishing. |
| Material Groups | N | * Mean | Std. Deviation | 95% Confidence Interval for Mean | Minimum | Maximum | ANOVA p-Value | ||
|---|---|---|---|---|---|---|---|---|---|
| Lower Bound | Upper Bound | ||||||||
| Pre Repair Strength | Group-A | 15 | 30.06 | 1.27 | 29.36 | 30.77 | 26.89 | 30.88 | 0.062 |
| Group-B | 15 | 28.05 | 2.54 | 26.65 | 29.46 | 23.28 | 30.87 | ||
| Group-C | 15 | 27.66 | 2.35 | 26.35 | 28.96 | 22.86 | 30.86 | ||
| Group-D | 15 | 28.75 | 2.75 | 27.23 | 30.28 | 22.91 | 30.87 | ||
| Group-E | 15 | 27.87 | 3.02 | 26.20 | 29.55 | 22.82 | 30.88 | ||
| Total | 75 | 28.48 | 2.55 | 27.89 | 29.07 | 22.82 | 30.88 | ||
| Post Repair Strength | Group-A | 15 | 13.44 | 3.04 | 11.75 | 15.12 | 8.29 | 20.70 | 0.002 |
| Group-B | 15 | 12.37 | 2.49 | 10.99 | 13.75 | 7.22 | 16.34 | ||
| Group-C | 15 | 13.79 | 1.32 | 13.06 | 14.53 | 12.34 | 16.93 | ||
| Group-D | 15 | 9.77 | 4.77 | 7.13 | 12.41 | 4.30 | 23.90 | ||
| Group-E | 15 | 11.16 | 1.90 | 10.11 | 12.22 | 9.03 | 15.50 | ||
| Total | 75 | 12.11 | 3.24 | 11.36 | 12.85 | 4.30 | 23.90 | ||
| Materials Tested | Shear Bond Strength | Mean | Std. Deviation | Std. Error Mean | Mean Difference | * p Value |
|---|---|---|---|---|---|---|
| Pair 1 Group-A | Pre-repair (n = 15) | 30.06 | 1.27 | 0.32 | 16.62 | 0.000 |
| Post-repair (n = 15) | 13.44 | 3.04 | 0.78 | |||
| Pair 2 Group-B | Pre-repair (n = 15) | 28.05 | 2.54 | 0.65 | 15.68 | 0.000 |
| Post-repair (n = 15) | 12.37 | 2.49 | 0.64 | |||
| Pair 3 Group-C | Pre-repair (n = 15) | 27.66 | 2.35 | 0.60 | 13.86 | 0.000 |
| Post-repair (n = 15) | 13.79 | 1.32 | 0.34 | |||
| Pair 4 Group-D | Pre-repair (n = 15) | 28.75 | 2.75 | 0.71 | 18.98 | 0.000 |
| Post-repair (n = 15) | 9.77 | 4.77 | 1.23 | |||
| Pair 5 Group-E | Pre-repair (n = 15) | 27.87 | 3.02 | 0.78 | 16.71 | 0.000 |
| Post-repair (n = 15) | 11.16 | 1.90 | 0.49 |
| Dependent Variable | Groups | Comparison | Mean Difference | * Sig. |
|---|---|---|---|---|
| Post-Repair Shear Bond Strength0 | A | B | 1.066 | 0.860 |
| C | −0.357 | 0.997 | ||
| D | 3.666 * | 0.010 | ||
| E | 2.273 | 0.229 | ||
| B | A | −1.066 | 0.860 | |
| C | −1.423 | 0.680 | ||
| D | 2.599 | 0.125 | ||
| E | 1.2063 | 0.797 | ||
| C | A | 0.357 | 0.997 | |
| B | 1.423 | 0.680 | ||
| D | 4.023 * | 0.003 | ||
| E | 2.63 | 0.118 | ||
| D | A | −3.666 * | 0.010 | |
| B | −2.599 | 0.125 | ||
| C | −4.023 * | 0.003 | ||
| E | −1.393 | 0.698 | ||
| E | A | −2.273 | 0.229 | |
| B | −1.206 | 0.797 | ||
| C | −2.63 | 0.118 | ||
| D | 1.393 | 0.698 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Habib, S.R.; Bajunaid, S.; Almansour, A.; AbuHaimed, A.; Almuqrin, M.N.; Alhadlaq, A.; Zafar, M.S. Shear Bond Strength of Veneered Zirconia Repaired Using Various Methods and Adhesive Systems: A Comparative Study. Polymers 2021, 13, 910. https://doi.org/10.3390/polym13060910
Habib SR, Bajunaid S, Almansour A, AbuHaimed A, Almuqrin MN, Alhadlaq A, Zafar MS. Shear Bond Strength of Veneered Zirconia Repaired Using Various Methods and Adhesive Systems: A Comparative Study. Polymers. 2021; 13(6):910. https://doi.org/10.3390/polym13060910
Chicago/Turabian StyleHabib, Syed Rashid, Salwa Bajunaid, Abdulrahman Almansour, Abdulkarim AbuHaimed, Muqrin Nasser Almuqrin, Abdullah Alhadlaq, and Muhammad Sohail Zafar. 2021. "Shear Bond Strength of Veneered Zirconia Repaired Using Various Methods and Adhesive Systems: A Comparative Study" Polymers 13, no. 6: 910. https://doi.org/10.3390/polym13060910
APA StyleHabib, S. R., Bajunaid, S., Almansour, A., AbuHaimed, A., Almuqrin, M. N., Alhadlaq, A., & Zafar, M. S. (2021). Shear Bond Strength of Veneered Zirconia Repaired Using Various Methods and Adhesive Systems: A Comparative Study. Polymers, 13(6), 910. https://doi.org/10.3390/polym13060910