
An Updated Review of Salivary pH Effects on Polymethyl Methacrylate (PMMA)-Based Removable Dental Prostheses

 , , and
, , and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Eligibility Criteria
2.2. Search Strategy
2.3. Data Management, Screening, and Selection
2.4. Risk of Bias Assessment
2.5. Data Analysis
3. Results
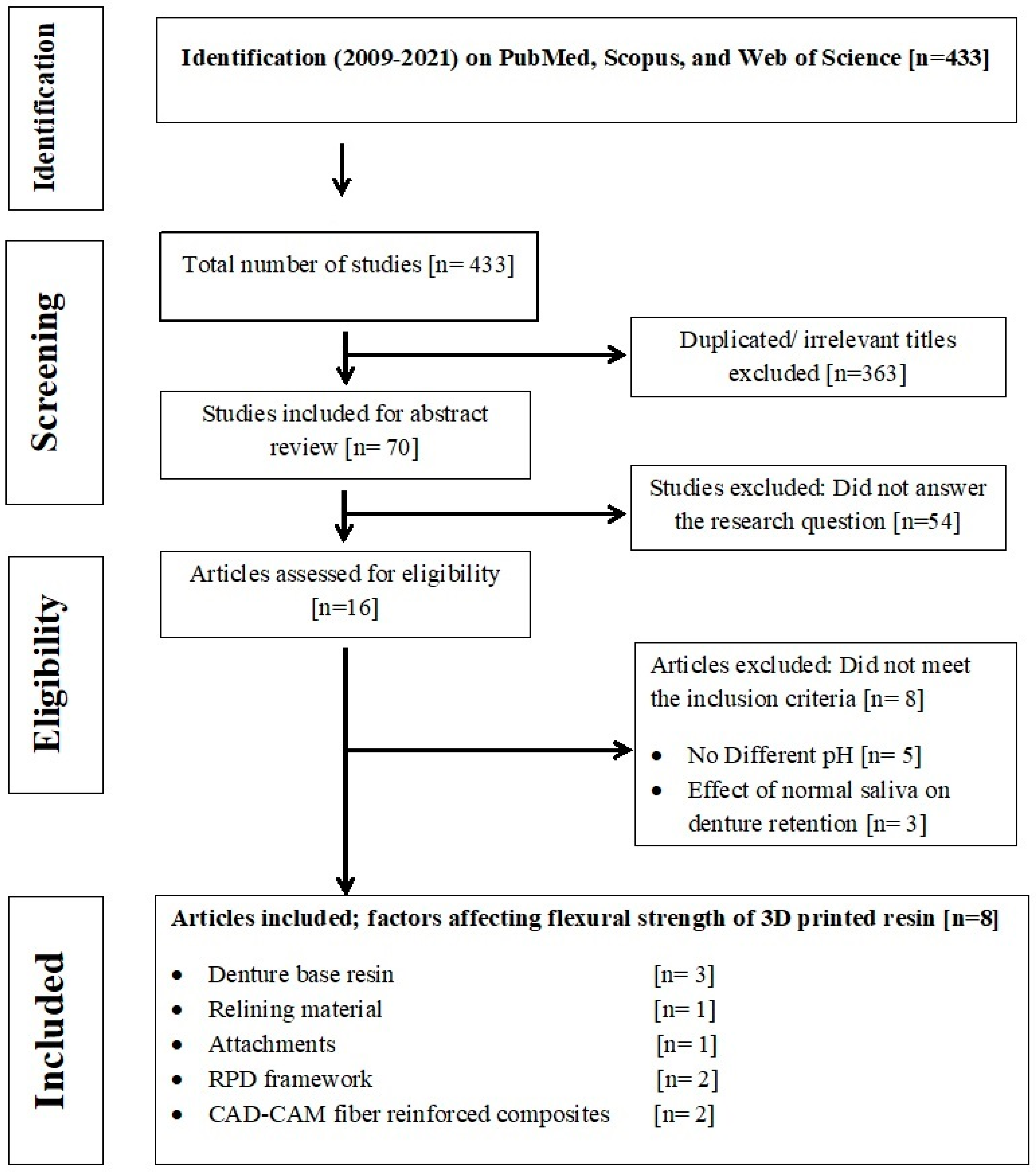
3.1. Data Selection
3.2. Risk of Bias
3.3. Data Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Gupta, A.; Felton, D.A.; Jemt, T.; Koka, S. Rehabilitation of Edentulism and Mortality: A Systematic Review. J. Prosthodont. 2019, 28, 526–535. [Google Scholar] [CrossRef]
- Muller, F.; Schimmel, M. Tooth loss and dental prostheses in the oldest old. Eur. Geriatr. Med. 2010, 1, 239–243. [Google Scholar] [CrossRef]
- Friel, T.; Waia, S. Removable Partial Dentures for Older Adults. Prim. Dent. J. 2020, 9, 34–39. [Google Scholar] [CrossRef]
- Zafar, M.S. Prosthodontic Applications of Polymethyl Methacrylate (PMMA): An Update. Polymers 2020, 12, 2299. [Google Scholar] [CrossRef]
- Khan, A.A.; Fareed, M.A.; Alshehri, A.H.; Aldegheishem, A.; Alharthi, R.; Saadaldin, S.A.; Zafar, M.S. Mechanical Properties of the Modified Denture Base Materials and Polymerization Methods: A Systematic Review. Int. J. Mol. Sci. 2022, 23, 5737. [Google Scholar] [CrossRef]
- Gad, M.M.; Fouda, S.M.; Al-Harbi, F.A.; Näpänkangas, R.; Raustia, A. PMMA denture base material enhancement: A review of fiber, filler, and nanofiller addition. Int. J. Nanomed. 2017, 12, 3801–3812. [Google Scholar] [CrossRef]
- Abualsaud, R.; Gad, M.M. Flexural Strength of CAD/CAM Denture Base Materials: Systematic Review and Meta-analysis of In-vitro Studies. J. Int. Soc. Prev. Community Dent. 2022, 12, 160–170. [Google Scholar] [CrossRef]
- Steinmassl, O.; Dumfahrt, H.; Grunert, I.; Steinmassl, P.A. CAD/CAM produces dentures with improved fit. Clin. Oral Investig. 2018, 22, 2829–2835. [Google Scholar] [CrossRef]
- Baba, N.Z.; Goodacre, B.J.; Goodacre, C.J.; Müller, F.; Wagner, S. CAD/CAM Complete Denture Systems and Physical Properties: A Review of the Literature. J. Prosthodont. 2021, 30, 113–124. [Google Scholar] [CrossRef]
- Prpić, V.; Schauperl, Z.; Ćatić, A.; Dulčić, N.; Čimić, S. Comparison of Mechanical Properties of 3D-Printed, CAD/CAM, and Conventional Denture Base Materials. J. Prosthodont. 2020, 29, 524–528. [Google Scholar] [CrossRef]
- Stawarczyk, B.; Beuer, F.; Wimmer, T.; Jahn, D.; Sener, B.; Roos, M.; Schmidlin, P.R. Polyetheretherketone-a suitable material for fixed dental prostheses? J. Biomed. Mater. Res. B Appl. Biomater. 2013, 101, 1209–1216. [Google Scholar] [CrossRef]
- Schwitalla, A.D.; Spintig, T.; Kallage, I.; Müller, W.D. Flexural behavior of PEEK materials for dental application. Dent. Mater. 2015, 31, 1377–1384. [Google Scholar] [CrossRef]
- Chen, X.; Mao, B.; Zhu, Z.; Yu, J.; Lu, Y.; Zhang, Q.; Yue, L.; Yu, H. A three-dimensional finite element analysis of mechanical function for 4 removable partial denture designs with 3 framework materials: CoCr, Ti-6Al-4V alloy and PEEK. Sci. Rep. 2019, 9, 13975. [Google Scholar] [CrossRef]
- Lekha, K.; Savitha, N.; Roseline, M.; Nadiger, R.K. Acetal resin as an esthetic claspmaterial. J. Interdiscip. Dent. 2012, 2, 11. [Google Scholar] [CrossRef]
- Alghazzawi, T.F. Advancements in CAD/CAM technology: Options for practical implementation. J. Prosthodont. Res. 2016, 60, 72–84. [Google Scholar] [CrossRef]
- Anadioti, E.; Musharbash, L.; Blatz, M.B.; Papavasiliou, G.; Kamposiora, P. 3D printed complete removable dental prostheses: A narrative review. BMC Oral Health 2020, 20, 343. [Google Scholar] [CrossRef]
- Gad, M.M.; Fouda, S.M.; Abualsaud, R.; Alshahrani, F.A.; Al-Thobity, A.M.; Khan, S.Q.; Akhtar, S.; Ateeq, I.S.; Helal, M.A.; Al-Harbi, F.A. Strength and Surface Properties of a 3D-Printed Denture Base Polymer. J. Prosthodont. 2021, 31, 412–418. [Google Scholar] [CrossRef]
- Gad, M.M.; Alshehri, S.Z.; Alhamid, S.A.; Albarrak, A.; Khan, S.Q.; Alshahrani, F.A.; Alqarawi, F.K. Water Sorption, Solubility, and Translucency of 3D-Printed Denture Base Resins. Dent. J. 2022, 10, 42. [Google Scholar] [CrossRef]
- Nowakowska-Toporowska, A.; Malecka, K.; Raszewski, Z.; Wieckiewicz, W. Changes in hardness of addition-polymerizing silicone-resilient denture liners after storage in artificial saliva. J. Prosthet. Dent. 2019, 121, 317–321. [Google Scholar] [CrossRef]
- Hashem, M.I. Advances in soft denture liners: An update. J. Contemp. Dent. Pract. 2015, 16, 314–318. [Google Scholar]
- Usta Kutlu, I.; Yanikoğlu, N.D.; Kul, E.; Duymuş, Z.Y.; Sağsöz, N.P. Effect of sealer coating and storage methods on the surface roughness of soft liners. J. Prosthet. Dent. 2016, 115, 371–376. [Google Scholar] [CrossRef]
- Landayan, J.I.A.; Manaloto, A.C.F.; Lee, J.Y.; Shin, S.W. Effect of aging on tear strength and cytotoxicity of soft denture lining materials; in vitro. J. Adv. Prosthodont. 2014, 6, 115–120. [Google Scholar] [CrossRef]
- Yanikoglu, N.D.; Duymuş, Z.Y. Comparative study of water sorption and solubility of soft lining materials in the different solutions. Dent. Mater. J. 2004, 23, 233–239. [Google Scholar] [CrossRef]
- Takahashi, Y.; Hamanaka, I.; Shimizu, H. Flexural properties of denture base resins subjected to long-term water immersion. Acta Odontol. Scand. 2013, 71, 716–720. [Google Scholar] [CrossRef]
- Gale, M.S.; Darvell, B.W. Thermal cycling procedures for laboratory testing of dental restorations. J. Dent. 1999, 27, 89–99. [Google Scholar] [CrossRef]
- Muddugangadhar, B.C.; Sangur, R.; Rudraprasad, I.V.; Nandeeshwar, D.B.; Kumar, B.H. A clinical study to compare between resting and stimulated whole salivary flow rate and pH before and after complete denture placement in different age groups. Indian Prosthodont. Soc. 2015, 15, 356–366. [Google Scholar] [CrossRef]
- Bettencourt, A.F.; Neves, C.B.; de Almeida, M.S.; Pinheiro, L.M.; Oliveira, S.A.; Lopes, L.P.; Castro, M.F. Biodegradation of acrylic based resins: A review. Dent. Mater. 2010, 26, e171–e180. [Google Scholar] [CrossRef]
- Polychronakis, N.; Polyzois, G.; Lagouvardos, P.; Andreopoulos, A.; Ngo, H.C. Long-term microwaving of denture base materials: Effects on dimensional, color and translucency stability. J. Appl. Oral Sci. 2018, 26, e20170536. [Google Scholar] [CrossRef]
- Humphrey, S.P.; Williamson, R.T. A review of saliva: Normal composition, flow, and function. J. Prosthet. Dent. 2001, 85, 162–169. [Google Scholar] [CrossRef]
- Hussein, Y.A.; Al-Ameer, S.S. The influence of different pH of saliva and thermal cycling on the adaptation of different denture base materials. J. Bagh. Coll. Dent. 2012, 24, 47–53. [Google Scholar]
- Antunes, C.; Aleem, A.; Curtis, S.A. Gastroesophageal Reflux Disease (GERD). Mo. Med. 2018, 115, 214–218. [Google Scholar]
- Shamseer, L.; Moher, D.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A.; the PRISMA-P Group. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P)2015: Elaboration and explanation. BMJ 2015, 350, 7647. [Google Scholar] [CrossRef] [PubMed]
- Koda, T.; Tsuchiya, H.; Yamauchi, M.; Ohtani, S.; Takagi, N.; Kawano, J. Leachability of denture-base acrylic resins in artificial saliva. Dent. Mater. 1990, 6, 13–16. [Google Scholar] [CrossRef]
- Akay, C.; Tanış, M.Ç.; Sevim, H. Effect of artificial saliva with different pH levels on the cytotoxicity of soft denture lining materials. Int. J. Artif. Organs. 2017, 40, 581–588. [Google Scholar] [CrossRef] [PubMed]
- Silva, A.S.; Aroso, C.; Ustrell, R.; Braga, A.C.; Mendes, J.M.; Escuin, T. The influence of saliva pH value on the retention and durability of bar-clip attachments. J. Adv. Prosthodont. 2015, 7, 32–38. [Google Scholar] [CrossRef]
- Gao, S.; Gao, S.; Xu, B.; Yu, H. Effects of Different pH-Values on the Nanomechanical Surface Properties of PEEK and CFR-PEEK Compared to Dental Resin-Based Materials. Materials 2015, 8, 4751–4767. [Google Scholar] [CrossRef]
- de Sá, J.; Vieira, F.; Aroso, C.M.; Cardoso, M.; Mendes, J.M.; Silva, A.S. The Influence of Saliva pH on the Fracture Resistance of Three Complete Denture Base Acrylic Resins. Int. J. Dent. 2020, 2020, 8941876. [Google Scholar]
- Bechir, F.; Bataga, S.M.; Ungureanu, E.; Vranceanu, D.M.; Pacurar, M.; Bechir, E.S.; Cotrut, C.M. Experimental Study Regarding the Behavior at Different pH of Two Types of Co-Cr Alloys Used for Prosthetic Restorations. Materials 2021, 14, 4635. [Google Scholar] [CrossRef]
- Fathy, S.M.; Emera, R.M.K.; Abdallah, R.M. Surface Microhardness, Flexural Strength, and Clasp Retention and Deformation of Acetal vs Poly-ether-ether Ketone after Combined Thermal Cycling and pH Aging. J. Contemp. Dent. Pract. 2021, 22, 140–145. [Google Scholar] [CrossRef]
- Bechir, F.; Bataga, S.M.; Tohati, A.; Ungureanu, E.; Cotrut, C.M.; Bechir, E.S.; Suciu, M.; Vranceanu, D.M. Evaluation of the Behavior of Two CAD/CAM Fiber-Reinforced Composite Dental Materials by Immersion Tests. Materials 2021, 14, 7185. [Google Scholar] [CrossRef]
- Bangera, M.K.; Kotian, R.N.R. Effect of titanium dioxide nanoparticle reinforcement on flexural strength of denture base resin: A systematic review and meta-analysis. Jpn. Dent. Sci. Rev. 2020, 56, 68–76. [Google Scholar] [CrossRef] [PubMed]
- Faggion, C.M., Jr. Guidelines for reporting pre-clinical in vitro studies on dental materials. J. Evid. Based Dent. Pract. 2012, 12, 182–189. [Google Scholar] [CrossRef] [PubMed]
- de Oliveira Limírio, J.P.J.; Gomes, J.M.L.; Alves Rezende, M.C.R.; Lemos, C.A.A.; Rosa, C.D.D.R.D.; Pellizzer, E.P. Mechanical properties of polymethyl methacrylate as a denture base: Conventional versus CAD-CAM resin—A systematic review and meta-analysis of in vitro studies. J. Prosthet. Dent. 2021, in press. [CrossRef]
- Sofya, P.A.; Rahmayani, L.; Purnama, R.R. Effect of soft drink towards heat cured acrylic resin denture base surface roughness. Padjadjaran J. Dent. 2017, 29. [Google Scholar] [CrossRef]
- Lussi, A.; Jaeggi, T.; Zero, D. The role of diet in the aetiology of dental erosion. Caries Res. 2004, 38 (Suppl. S1), 34–44. [Google Scholar] [CrossRef]
- Minich, D.M.; Bland, J.S. Acid-alkaline balance: Role in chronic disease and detoxification. Altern. Ther. Health Med. 2007, 13, 62–65. [Google Scholar] [PubMed]
- Figueiral, M.H.; Azul, A.M.; Fonseca, P.; Pinto, E.; Branco, F.M. Influence of saliva on prosthetic stomatitis. Rev. Port. Estomatol. Med. Dent. E’Cir. Maxilofac. 2006, 47, 197–202. [Google Scholar]
- Garcia, L.F.; Roselino, L.M.; Mundim, F.M.; Consani, S. The influence of artificial accelerated aging on dimensional stability of acrylic resin submitted to different storage protocols. J. Prosthodont. 2010, 19, 432–437. [Google Scholar] [CrossRef]
- Wei, X.; Pan, Y.; Wang, M.; Wang, Y.; Lin, H.; Jiang, L.; Lin, D.; Cheng, H. Comparative analysis of leaching residual monomer and biological effects of four types of conventional and CAD/CAM dental polymers: An in vitro study. Clin. Oral Investig. 2022, 26, 2887–2898. [Google Scholar] [CrossRef]
- El-Hadary, A.; Drummond, J.L. Comparative study of water, Solubility, and tensile bond strength of two soft lining materials. Prosthet. Dent. 2000, 83, 356–361. [Google Scholar] [CrossRef]
- Song, Y.H.; Song, H.J.; Han, M.K.; Yang, H.S.; Park, Y.J. Cytotoxicity of soft denture lining materials depending on their component types. Int. J. Prosthodont. 2014, 27, 229–235. [Google Scholar] [CrossRef] [PubMed]
- Khan, A.A.; De Vera, M.A.; Mohamed, B.A.; Javed, R.; Al-Kheraif, A.A. Enhancing the physical properties of acrylic resilient denture liner using graphene oxide nanosheets. J. Vinyl Addit. Technol. 2022, 28, 487–493. [Google Scholar] [CrossRef]
- Achim, G. Mechanisms of Polymer Degradation and Erosion. Biomaterials 1996, 17, 103–114. [Google Scholar]
- Armencia, A.O.; Hurju, I.; Tărniceriu, C.C.; Lese, A.; Feier, R.; Scutariu, M.M.; Balcos, C. The study of roughness and resistance to corrosion of dental alloys in the oral environment. Rom. J. Oral Rehabil. 2020, 12, 190–197. [Google Scholar]
- Kassapidou, M.; Stenport, V.F.; Hjalmarsson, L.; Johansson, C.B. Cobalt-chromium alloys in fixed prosthodontics in Sweden. Acta Biomater. Odontol. Scand. 2017, 3, 53–62. [Google Scholar] [CrossRef] [PubMed]
- Soares, F.M.D.S.; Santana, A.I.D.C.; dos Santos, L.B.F.; Gomes, P.A.M.C.; Monteiro, E.D.S.; Coimbra, M.E.R.; Elias, C.N. Influence of oral pH Environment in the Corrosion Resistance of Cr-Co-Mo alloy Used for Dentistry Prosthetic Components. Mater. Res. 2019, 22. [Google Scholar] [CrossRef]
- Najeeb, S.; Zafar, M.S.; Khurshid, Z.; Siddiqui, F. Applications of polyetheretherketone (PEEK) in oral implantology and prosthodontics. J. Prosthodont. Res. 2016, 60, 12–19. [Google Scholar] [CrossRef]


{kind=link}
| Author/Year/ Type of Study | Restorations/Specimen Dimensions | Saliva/Type | Sample Size | Aging Effect | Tested Properties | Results and Outcome | |
|---|---|---|---|---|---|---|---|
| pH | Composition | ||||||
| Koda T et al., 1990 [33] | Auto-polymerized Heat-polymerized microwave-polymerized/ Resin disks (thickness of 2.0 × 8.5 mm | pH 4 pH 5.0 pH 6.0 pH 6.8 | 0.3 mM CaS04; 1.0 mM NaCl; 0.7 mM KC1; 0.4 mM KH2P04 0.4 mM Na2HP04 | (n = 10) | 10 days immersion | Leachability of MMA, methacrylic acid (M), benzoic acid (BA), and methyl acrylate (MA), | The leachability of MMA, M, BA, and MA increased in more acidic and less acidic pH and this mainly due hydrolysis of MMA which resulted in more chemotoxic actions of denture base material |
| Akay C et al., 2017 [34] | denture lining materials/ disk 5-mm x 2-mm thickness | pH 4 pH 7 pH 14 | 4.1 mM KH2PO4, 4.0 mM Na2 HPO4, 24.8 mM KHCO3, 16.5 mM NaCl, 0.25 mM CaCl2. | (n = 96) (n = 12) | 21 days immersion | Cytotoxicity | The cytotoxicity of soft liners increases with storage in different salivary pH. |
| Silva et al., 2015 [35] | 4 types of attachments | pH 4 pH 7 | KC1;18.5% 6.5 mL NaCl 20% 8.6mL CaCl2•2H2O 10% 8 mL Sorbitol 50% 48 mL Carboxymethylcellulose 20 g Citric acid 10 g Nipagin 1.6 g Nipasol 0.4 g Water 1950 mL | (n = 4) | 5400 insertion/removal cycles were simulated (5 years) | durability and retention | Different salivary pH adversely affects the retention and the most negative effect on the attachment retention was recorded with more acidic pH. |
| Gao et al., 2015 [36] | polyetheretherketone (PEEK) and a carbon fiber-reinforced PEEK (CFR-PEEK) with 30% short carbon fibers, a dental composite based on Bis-GMA and polymethylmethacrylate (PMMA)/ milled disks of 8 × 10 mm | pH 3 pH 7 pH 10 | NaCl 125.6 KCl 963.9 KSCN 189.2 KH2PO4 654.5 Urea 200.0 NaSO4·10H2O 763.2 NH4Cl 178.0 CaCl2·2H2O 227.8 NaHCO3 630.8 | (n = 40/material) (n = 10/pH) | 30 days immersion | elastic moduli, nanohardness, viscoelasticity, and friction performance | no significant changes in PEEK after immersion in different salivary pH |
| Sa et al., 2019 [37] | prosthesis bases | pH 4 pH 7 | 0.4 g/L NaCl, 0.4 g/L KCl, 0.795 g/L CaCl2.2H2O, 0.005 g/L Na2S.9H2O, 0.69 g/L NaH2PO4.2HSO, 1 g/L urea | (n = 5) | 30 days immersion | fatigue resistance | the fracture resistance of denture base resins was decreases with results at low pH environment |
| Bechir et al., 2021 [38] | Co-Cr alloy, casted or milled/ discs with a diameter of 15 mm and a thickness of 5 mm. | pH 3 pH 5.7 pH 7.6 | Na2HPO4 0.19 NaCl 0.7 KSCN 0.33 KH2PO4 0.26 NaHCO3 1.5 Ureea 1.3 | NS | NS | corrosion behavior of two commercial Co-Cr dental alloys manufactured by casting and by milling | Co-Cr alloys (cast and milled) have poor corrosion resistance when immersed in artificial saliva with acidic salivary pH. However, the corrosion behavior of milled one was better, making this alloy a better option for GERD patients |
| Fathy et al., 2021 [39] | denture base and clasp construction/ Two Aker clasps materials (acetal and PEEK) 65× 10 ×2.5 mm 92 disk-shaped (10 × 1 mm) | pH 5.8 pH 7.2 pH 8.3 | NaCl 0.70, Na2PO4 0.26, KSCN 0.33, KH2PO4 0.20 | (n = 10) | NS | flexural strength, hardness, clasp retention and deformation | At acidic and alkaline pH and combining thermal aging, the flexural strength and surface microhardness of acetal, as well as its clasp retention and deformation, Meanwhile, PEEK clasps were not significantly affected. |
| Bechir et al., 2021 [40] | restorative materials for prosthetic oral rehabilitation Two CAD/CAM Fiber-Reinforced Composite Dental/ 15 mm × 5 mm | pH 3 pH 5.7 pH 7.6 | Na2HPO4 0.19 g NaCl 0.70 g KSCN 0.33 g KH2PO4 0.26 g NaHCO3 1.50 g Urea 1.30 g | NS | 21 days | changes in mass or surface morphology | Novel composite biomaterials showed a stable surface when in contact with different salivary pH and can be used to fabricate prosthetic frameworks in GERD patients |
| Questions—JBI Critical Appraisal Checklist | Revisor 1 | Revisor 1 | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Yes | No | Unclear | NA | Yes | No | Unclear | NA | ||
| 1 | Is it clear in the study what is the ‘cause’ and what is the ‘effect’ (there is no confusion about which variable comes first)? | 8 | 8 | ||||||
| 2 | Were the participants included in any comparisons similar? | 8 | 8 | ||||||
| 3 | Were the participants included in any comparisons receiving similar treatment/care, other than the exposure or intervention of interest? | 5 | 3 | 8 | |||||
| 4 | Was there a control group? | 8 | 8 | ||||||
| 5 | Were there multiple measurements of the outcome both pre and post the intervention/exposure? | 6 | 2 | 8 | |||||
| 6 | Was follow up complete and if not, were differences between groups in terms of their follow up adequately described and analyzed? | 8 | 8 | ||||||
| 7 | Were the outcomes of participants included in any comparisons measured in the same way? | 8 | 7 | 1 | |||||
| 8 | Were outcomes measured in a reliable way? | 6 | 2 | 8 | |||||
| 9 | Was appropriate statistical analysis used? | 8 | 8 | ||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alshahrani, F.A.; AlToraibily, F.; Alzaid, M.; Mahrous, A.A.; Al Ghamdi, M.A.; Gad, M.M. An Updated Review of Salivary pH Effects on Polymethyl Methacrylate (PMMA)-Based Removable Dental Prostheses. Polymers 2022, 14, 3387. https://doi.org/10.3390/polym14163387
Alshahrani FA, AlToraibily F, Alzaid M, Mahrous AA, Al Ghamdi MA, Gad MM. An Updated Review of Salivary pH Effects on Polymethyl Methacrylate (PMMA)-Based Removable Dental Prostheses. Polymers. 2022; 14(16):3387. https://doi.org/10.3390/polym14163387
Chicago/Turabian StyleAlshahrani, Faris A., Fatemah AlToraibily, Maryam Alzaid, Amr A. Mahrous, Maram A. Al Ghamdi, and Mohammed M. Gad. 2022. "An Updated Review of Salivary pH Effects on Polymethyl Methacrylate (PMMA)-Based Removable Dental Prostheses" Polymers 14, no. 16: 3387. https://doi.org/10.3390/polym14163387
APA StyleAlshahrani, F. A., AlToraibily, F., Alzaid, M., Mahrous, A. A., Al Ghamdi, M. A., & Gad, M. M. (2022). An Updated Review of Salivary pH Effects on Polymethyl Methacrylate (PMMA)-Based Removable Dental Prostheses. Polymers, 14(16), 3387. https://doi.org/10.3390/polym14163387