


Conventional Dental Impressions vs. Impressions Reinforced with Rigid Mouthguards
 , ,
, ,  ,
,  ,
,  ,
,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Groups
- Group 1 (CA)—for conventional impressions made from alginate;
- Group 2 (CCS)—for conventional impressions made from condensation silicone;
- Group 3 (CAS)—for conventional impressions made from addition silicone;
- Group 4 (RA)—for reinforced impressions made from alginate;
- Group 5 (RCS)—for reinforced impressions made from condensation silicone;
- Group 6 (RAS)—for reinforced impressions made from addition silicone.
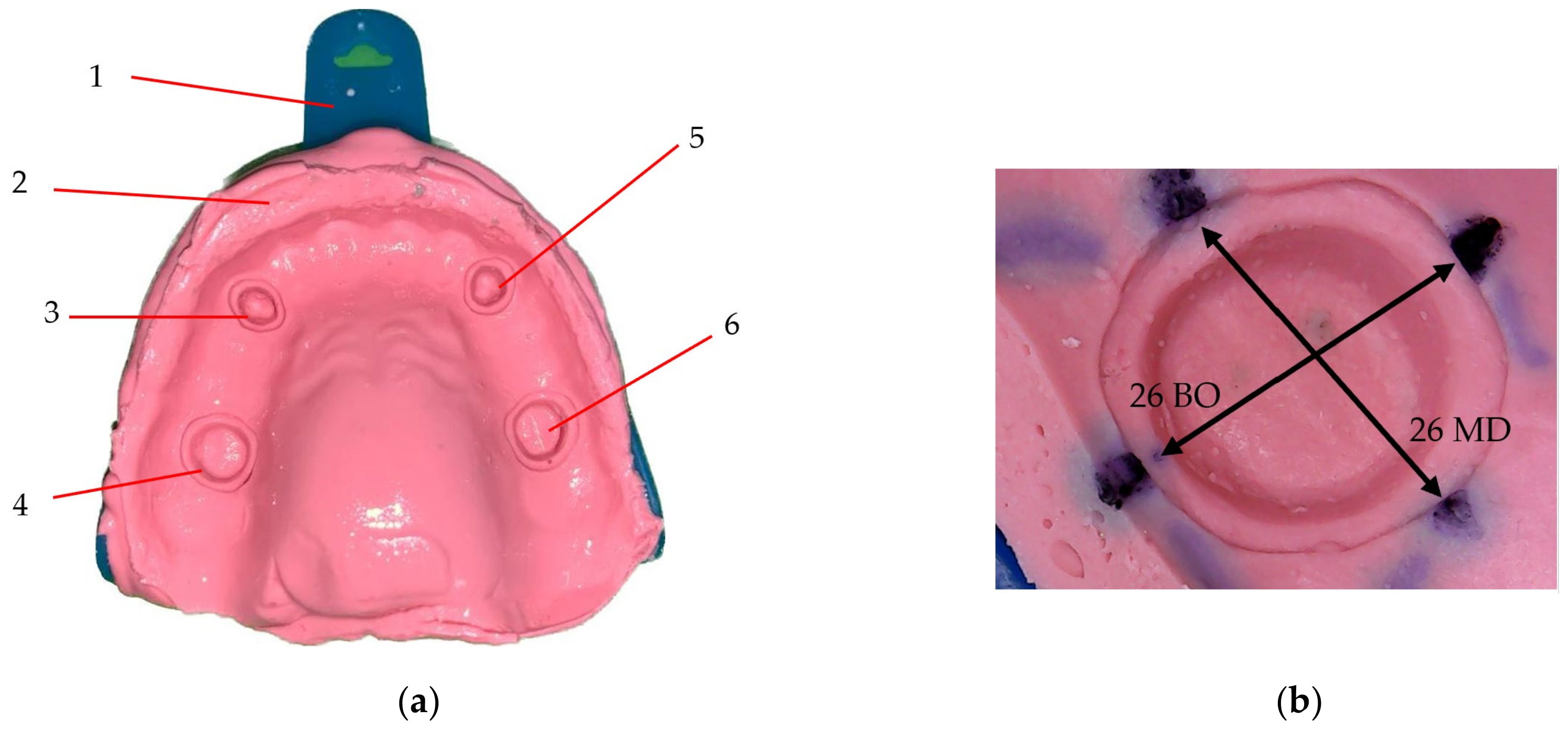
2.2. Sample Preparation
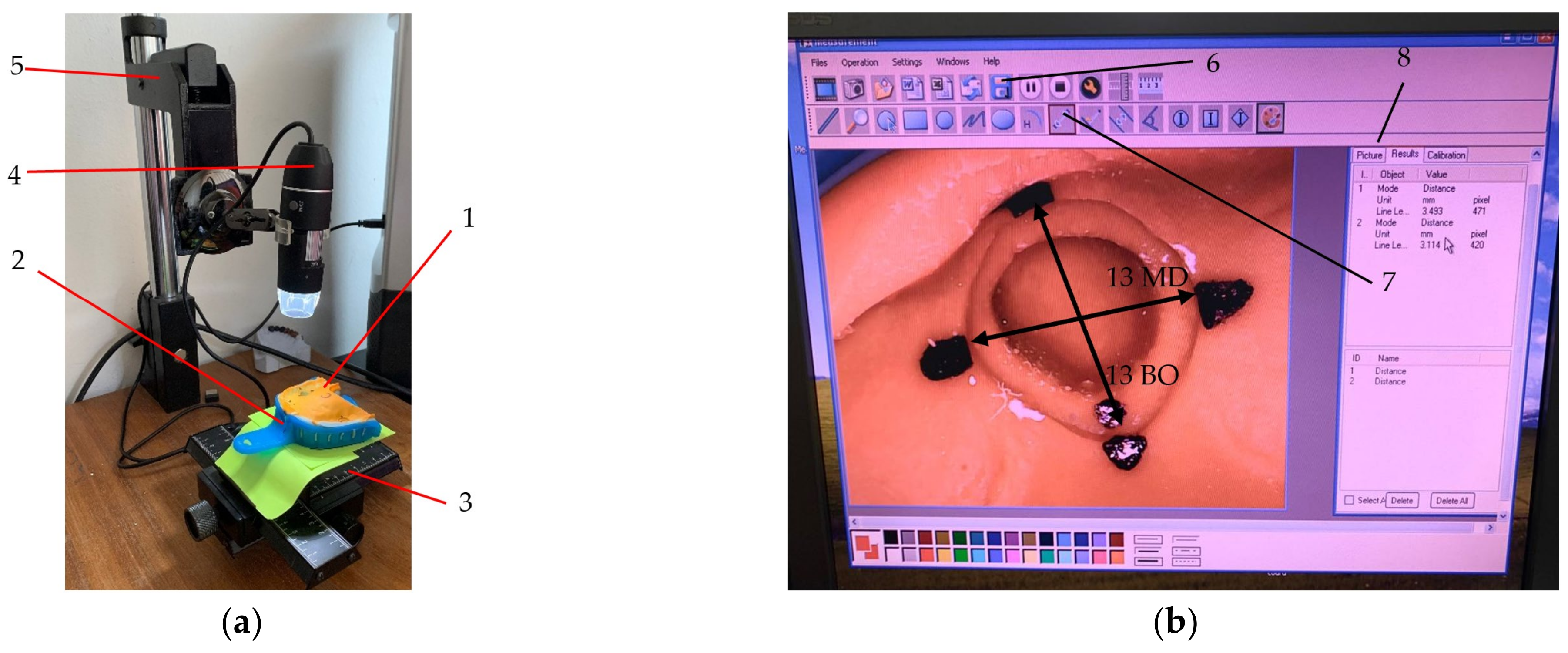
2.3. Measurement Protocols
2.4. Statistical Analysis
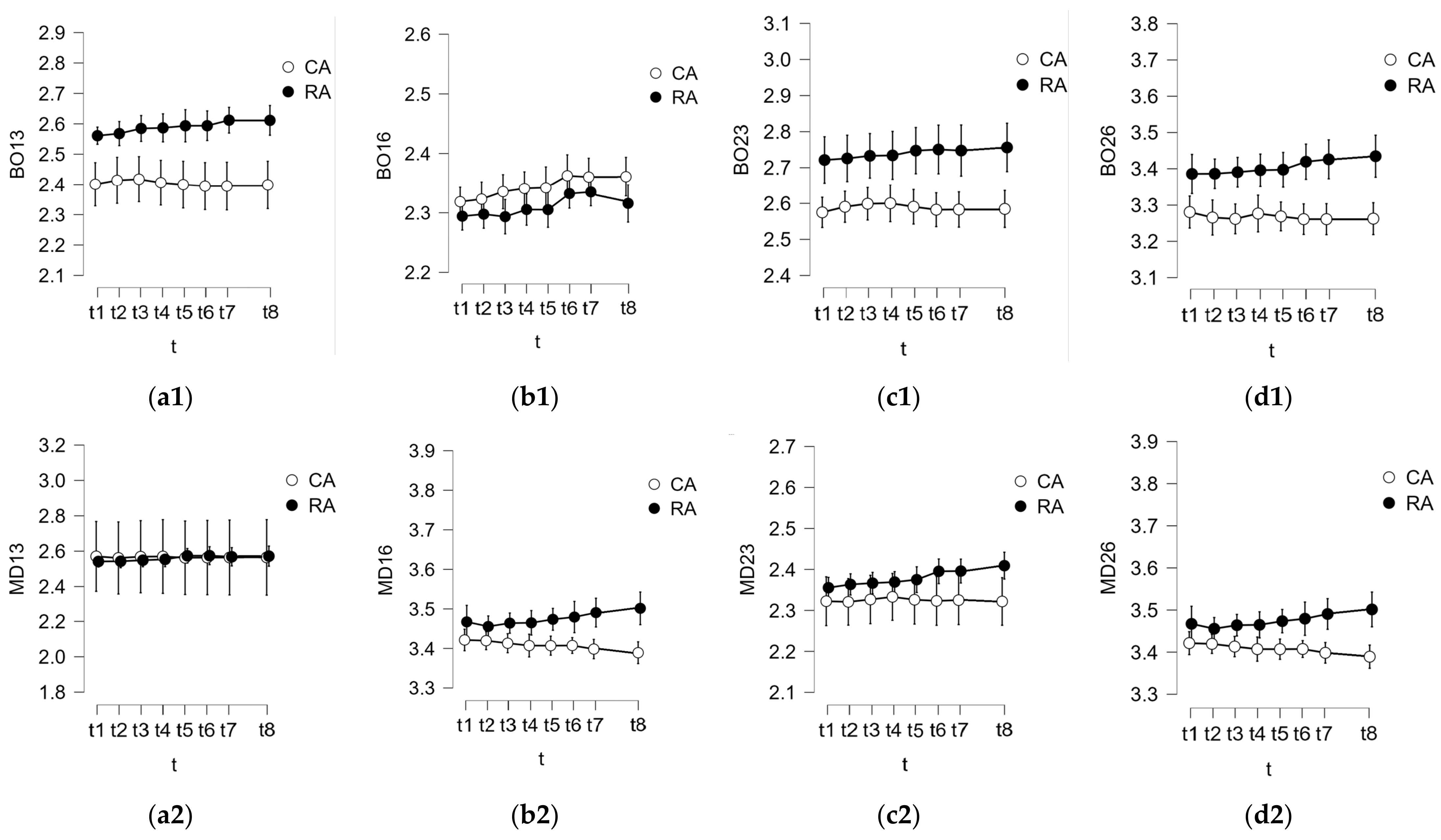
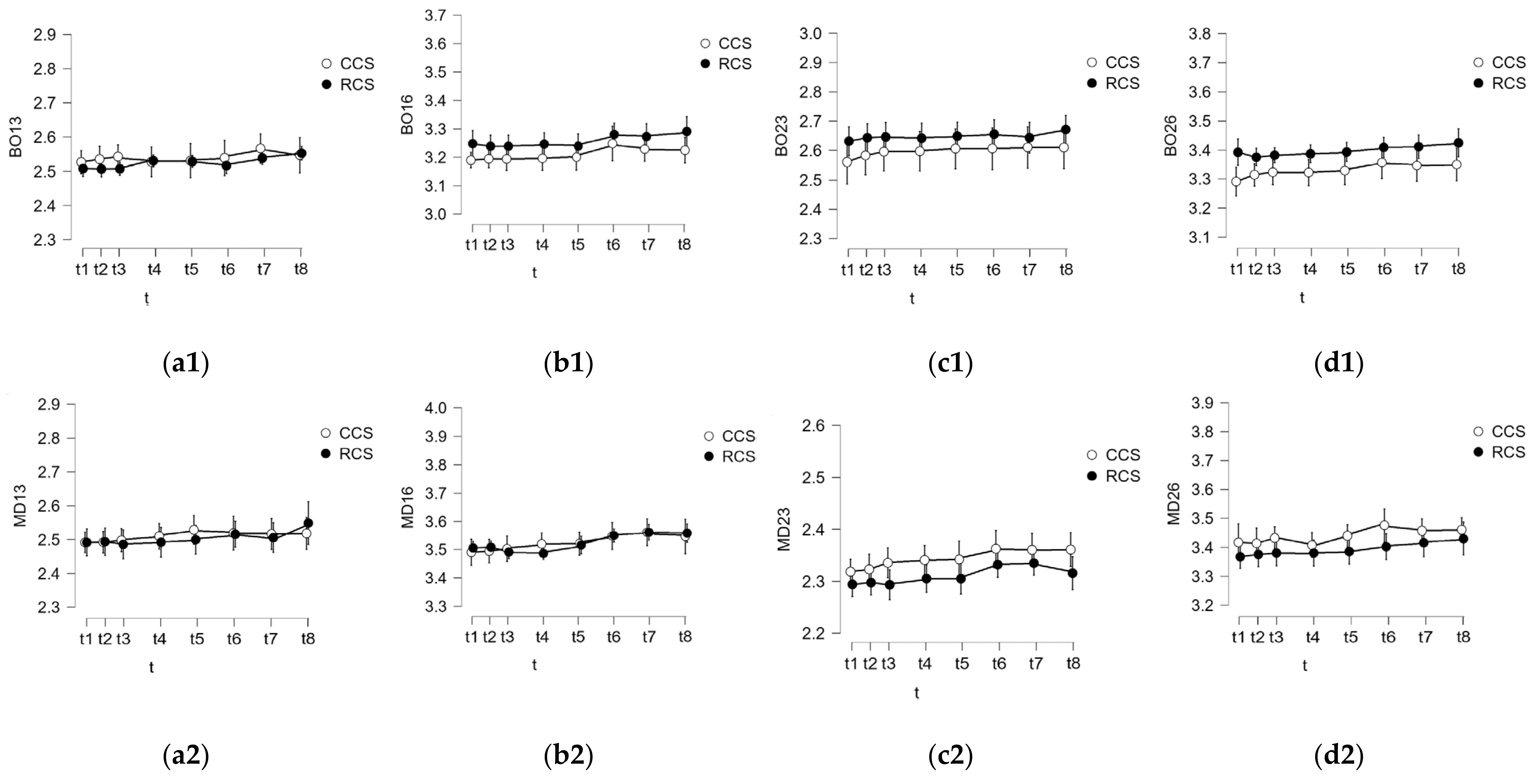
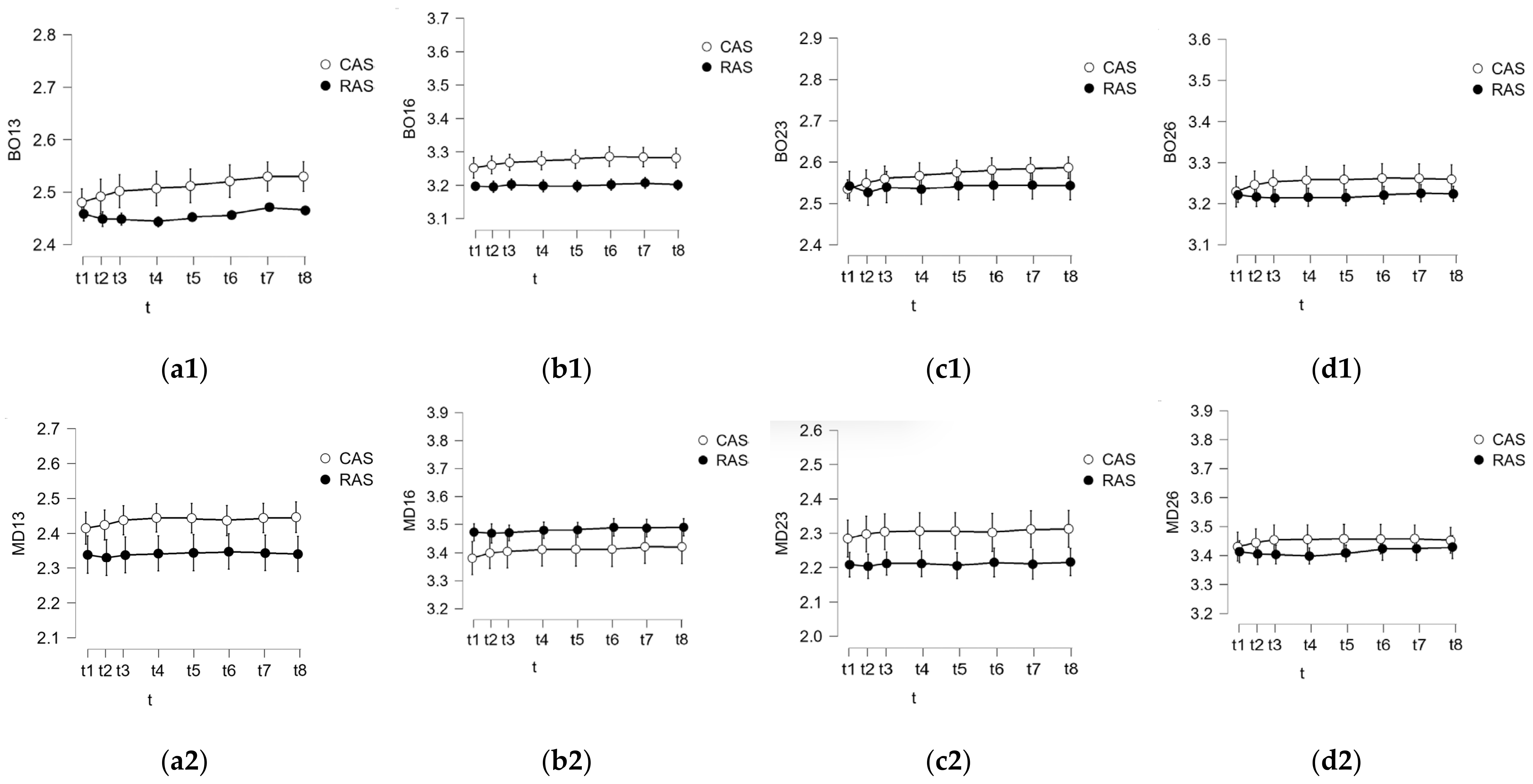
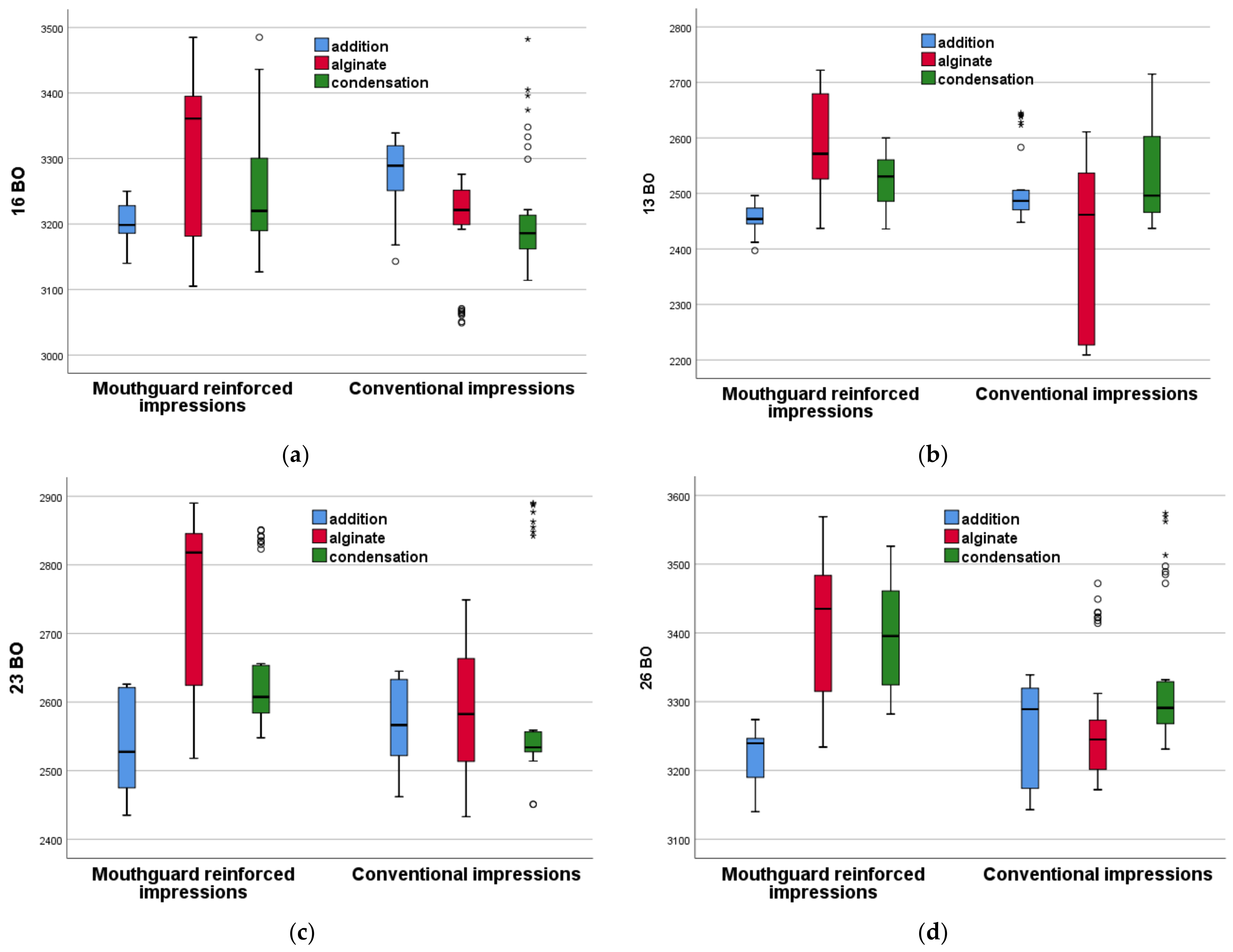
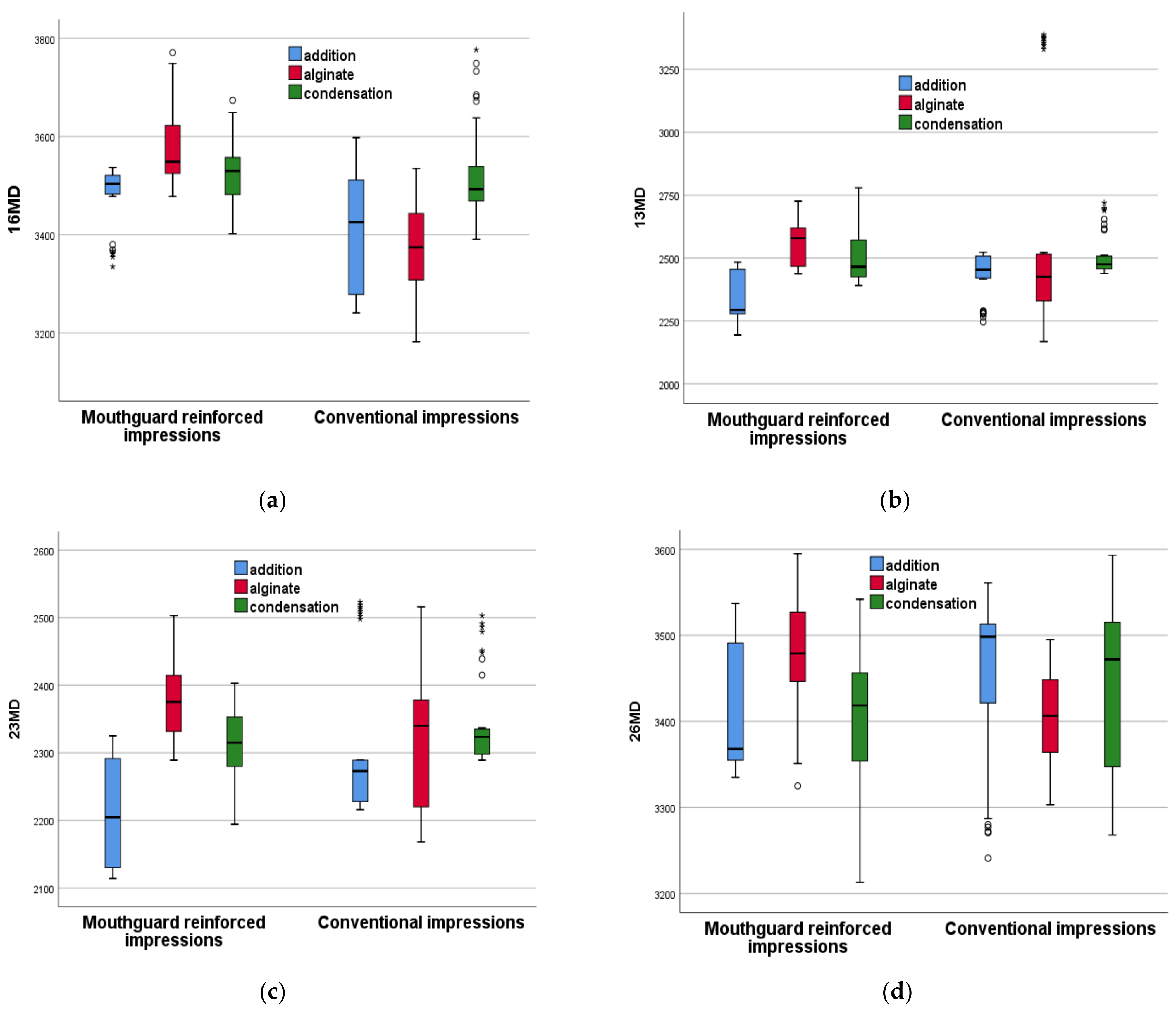
3. Results
4. Discussion
4.1. Comparison between the Different Groups
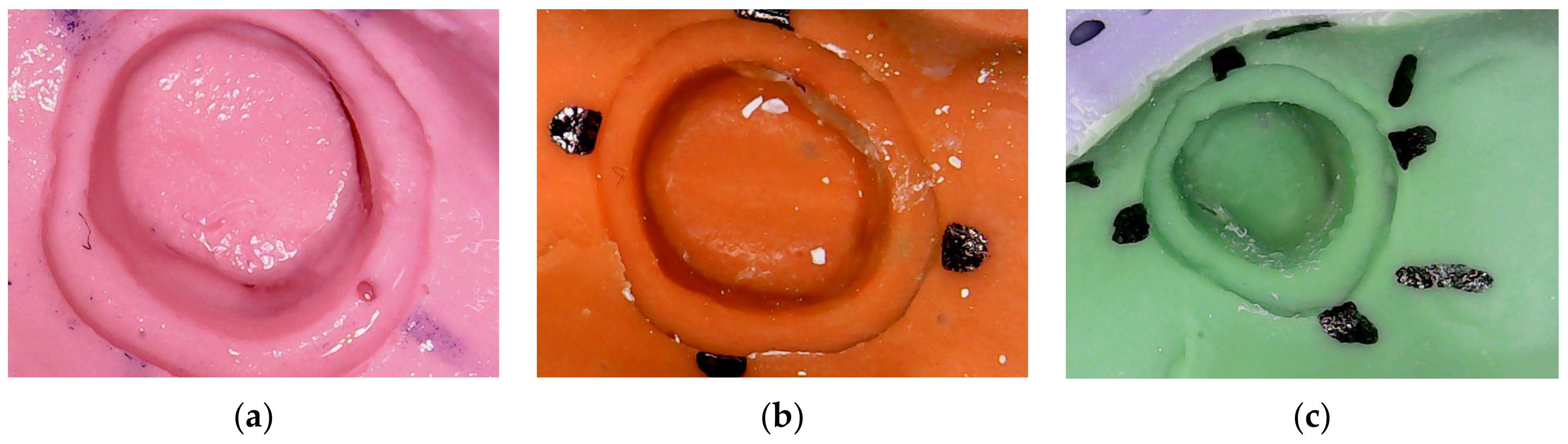
4.2. Defects in the Obtained Impressions
4.3. Discussion Regarding Different Impressions Materials
4.4. Discussion Regarding the Impression Technique
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Polymeric Material | Consistency | Residual Deformation (%) | Flexibility (%) | Dimensional Variation (%) | Hardness Shore A | Tear Resistance (g/cm) |
|---|---|---|---|---|---|---|
| Polysulfides | low | 3–4 | 14–17 | 0.5–2 | 20 | 2500–7000 |
| medium | 3–5 | 11–15 | 0.5–1 | 30 | 3000–7000 | |
| heavy | 3–6 | 9–12 | 0.5–1 | 35 | - | |
| Polyether | low | 1.5 | 3 | 0.03 | 35–40 | 1800 |
| medium | 1–2 | 2–3 | 0.02 | 35–60 | 2800–4800 | |
| Medium + viscosity-lowering agent | 2 | 6 | 0.04 | 30–50 | 2500 | |
| Heavy | 2 | 3 | 0.02 | 40–50 | 3000 | |
| Condensation silicones | low | 1–2 | 4–9 | 0.05–0.1 | 15–30 | 2300–2600 |
| putty | 2–3 | 2–5 | 0.02–0.05 | 50–65 | - | |
| Addition silicones | low | 0.05–0.4 | 3–6 | 0.01–0.03 | 35 | 1500–3000 |
| medium | 0.05–0.3 | 2–5 | 0.01–0.03 | 50 | 2200–3500 | |
| heavy | 0.1–0.3 | 2–3 | 0.01–0.03 | 60 | 2500–4300 | |
| putty | 0.2–0.5 | 1–2 | 0.01–0.1 | 50–75 | - |
References
- Yaqoob, A.; Al Shehrani, I.; Alfarsi, M.; Baba, S.; Kanji, M.A.; Hussain, M.W. Panorama of impression techniques in fixed partial dentures: A systematic review. Int. J. Med. Dent. 2018, 22, 70–84. [Google Scholar]
- Brown, J.; Smith, M. The Role of Impression Material Selection in Minimizing Dimensional Changes in Dental Restorations. J. Dent. Res. 2014, 93, 212–216. [Google Scholar]
- Abduo, J.; Elseyoufi, M. Accuracy of Intraoral Scanners: A Systematic Review of Influencing Factors. Eur. J. Prosthodont. Restor. Dent. 2018, 26, 101–121. [Google Scholar] [CrossRef] [PubMed]
- Patel, S.; Johnson, L. The Influence of Impression Technique and Thickness on the Dimensional Stability of Condensation and Addition Silicone Impression Materials. J. Dent. Res. 2016, 95, 342–346. [Google Scholar]
- Kim, H.; Lee, J. The Influence of Impression Tray Type on the Dimensional Stability of Dental Impression Materials. J. Prosthet. Dent. 2016, 115, 259–264. [Google Scholar]
- Rubel, B.S. Impression Materials: A Comparative Review of Impression Materials Most Commonly Used in Restorative Dentistry. Dent. Clin. N. Am. 2007, 51, 629–642. [Google Scholar] [CrossRef] [PubMed]
- Punj, A.; Bompolaki, D.; Garaicoa, J. Dental Impression Materials and Techniques. Dent. Clin. N. Am. 2017, 61, 779–796. [Google Scholar] [CrossRef] [PubMed]
- Pisulkar, S.; Nimonkar, S.; Borle, A.; Dhage, Y. Recent advances in elastomeric impression materials. EAS J. Dent. Oral Med. 2019, 1, 83–86. [Google Scholar]
- Payam, Z.; Sahba, R. Impression materials for dental prosthesis. In Advanced Dental Biomaterials; Elsevier: New York, NY, USA, 2019; p. 207. [Google Scholar]
- Vitti, R.P.; da Silva, M.A.B.; Consani, R.L.X.; Sinhoreti, M.A.C. Dimensional Accuracy of Stone Casts Made from Silicone-Based Impression Materials and Three Impression Techniques. Braz. Dent. J. 2013, 24, 498–502. [Google Scholar] [CrossRef] [PubMed]
- Martins, F.; Reis, J.; Barbero Navarro, I.; Maurício, P. Dimensional Stability of a Preliminary Vinyl Polysiloxane Impression Material. Dent. J. 2019, 7, 81. [Google Scholar] [CrossRef] [PubMed]
- Soganci, G.; Cinar, D.; Caglar, A.; Yagiz, A. 3D evaluation of the effect of disinfectants on dimensional accuracy and stability of two elastomeric impression materials. Dent. Mater. J. 2018, 37, 675–684. [Google Scholar] [CrossRef] [PubMed]
- Troiano, G.; Amoroso, G.; Crimi, S.; Matarese, M.; D’Amico, C.; NastroSiniscalchi, E.; Cicciù, M. Alginate materials and dental impression technique: A current state of the art and application to dental practice. Mar. Drugs 2018, 17, 18. [Google Scholar] [CrossRef]
- Babiker, G.H.; Khalifa, N.; Alhajj, M.N. Dimensional Accuracy of Alginate Impressions Using Different Methods of Disinfection with Varying Concentrations. Compend. Contin. Educ. Dent. 2018, 39, e17–e20. [Google Scholar] [PubMed]
- Kumar, D.; Madihalli, A.U.; Reddy, K.R.; Rastogi, N.; Pradeep, N.T. Elastomeric impression materials: A comparison of accuracy of multiple pours. J. Contemp. Dent. Pract. 2011, 12, 272–288. [Google Scholar] [CrossRef] [PubMed]
- Karaaslan, G.; Malkoc, M.A.; Yildirim, G.; Malkoc, S. Comparison of time-dependent two-dimensional and three-dimensional stability with micro-computerized tomography and wettability of three impression materials. Niger. J. Clin. Pract. 2018, 21, 912–920. [Google Scholar] [CrossRef] [PubMed]
- Williams, J.; Johnson, L. The Effect of Dimensional Changes in Dental Impression on the Fit of Crown Restorations. J. Prosthet. Dent. 2012, 107, 220–225. [Google Scholar]
- Patel, S.; Johnson, L. The Impact of Dimensional Changes in Dental Impressions on the Accuracy of Veneers and Bridges. J. Dent. Res. 2018, 97, 53–58. [Google Scholar]
- Neethu, L.; Vasunni, G.K. Comparative evaluation of dimensional stability of three different elastomeric impression materials: An in vitro study. IOSR J. Dent. Med. Sci. 2015, 14, 89–93. [Google Scholar]
- Abd-Al Hamed, A.; El-Gharabawy, S.H.; Al-Abbassy, F.; Elsalam, A.E.A. Laboratory evaluation of dimensional changes of different elastomeric impression materials using 3D laser scanner. IJSR 2016, 5, 2064–2070. [Google Scholar]
- German, M.J.; Carrick, T.E.; McCabe, J.F. Surface detail reproduction of elastomeric impression materials related to rheological properties. Dent. Mater. 2008, 24, 951–956. [Google Scholar] [CrossRef] [PubMed]
- Shen, C.; Rawls, H.; Esquivel-Upshaw, J. Phillips’ Science of Dental Material, 13th ed.; Elsevier: St Louis, MI, USA, 2021. [Google Scholar]
- Lu, H.; Nguyen, B.; Powers, J. Mechanical properties of 3 hydrophilic addition silicone and polyether elastomeric impression materials. J. Prosthet. Dent. 2004, 92, 151–154. [Google Scholar] [CrossRef] [PubMed]
- Gonçalves, F.S.; Popoff, D.A.; Castro, C.D.; Silva, G.C.; Magalhães, C.S.; Moreira, A.N. Dimensional stability of elastomeric impression materials: A critical review of the literature. Eur. J. Prosthodont. Restor. Dent. 2011, 19, 163–166. [Google Scholar] [PubMed]
- CoolingTech Microscope—Download. Available online: https://coolingtech-microscope.updatestar.com/en (accessed on 30 March 2014).
- Kulkarni, M.M.; Thombare, R.U. Dimensional Changes of Alginate Dental Impression Materials-An Invitro Study. J. Clin. Diagn. Res. 2015, 9, ZC98–ZC102. [Google Scholar] [CrossRef] [PubMed]
- Hamrun, N.; Talib, B.; Ruslin, M.; Pangeran, H.; Hatta, M.; Marlina, E.; Yusuf, A.S.H.; Saito, T.; Ou, K.-L. A Promising Potential of Brown Algae Sargassum polycystum as Irreversible Hydrocolloid Impression Material. Mar. Drugs 2022, 20, 55. [Google Scholar] [CrossRef] [PubMed]
- Abdelraouf, R.M.; Bayoumi, R.E.; Hamdy, T.M. Effect of Powder/Water Ratio Variation on Viscosity, Tear Strength and Detail Reproduction of Dental Alginate Impression Material (In Vitro and Clinical Study). Polymers 2021, 13, 2923. [Google Scholar] [CrossRef] [PubMed]
- Jayachandran, D.; Alarmelu; Dorairaj, J.; Priya, S. Evaluation of the Efficacy of Novel Self Disinfectant Solution in Irreversible Hydrocolloid Impression Material—An Experimental Study. Indian J. Dent. Res. 2024, 34, 252–256. [Google Scholar] [CrossRef]
- Phudphong, P.; Amornvit, P.; Sirintawat, N. Comparison of Accuracy of Alginate Impression and Intraoral Scanner in Model with and without Orthodontic Brackets. Appl. Sci. 2021, 11, 6037. [Google Scholar] [CrossRef]
- Al-Odinee, N.M.; Al-Hamzi, M.; Al-shami, I.Z.; Madfa, A.; Al-Kholani, A.I. Evaluation of the quality of fixed prosthesis impressions in private laboratories in a sample from Yemen. BMC Oral Health 2020, 20, 304. [Google Scholar] [CrossRef] [PubMed]
- Rau, C.T.; Olafsson, V.G.; Delgado, A.J.; Ritter, A.V.; Donovan, T.E. The quality of fxed prosthodontic impressions: An assessment of crown and bridge impressions received at commercial laboratories. J. Am. Dent. Assoc. 2017, 148, 654–660. [Google Scholar] [CrossRef] [PubMed]
- Winstanley, R.; Carrotte, P.; Johnson, A. The quality of impressions for crowns and bridges received at commercial dental laboratories. Br. Dent. J. 1997, 183, 209. [Google Scholar] [CrossRef] [PubMed]
- Albashaireh, Z.S.; Alnegrish, A.S. Assessing the quality of clinical procedures and technical standards of dental laboratories in fxed partial denture therapy. Int. J. Prosthodont. 1999, 12, 236. [Google Scholar] [PubMed]
- Zu Saifudin, A.S.A.; Kamaruddin, F.; AbGhani, S.M. The quality of working impressions for the fabrication of fxed prosthodontics prostheses (crown and bridgework). Eur. J. Gen. Dent. 2014, 3, 100. [Google Scholar]
- Khan, S.A.; Tushar, N.S.; Singh, P.; Kumari, N.; Singh, S.S. Comparison and Evaluation of Linear Dimensional Accuracy of Three Elastomeric Impression Materials at Different Time Intervals Using Vision Inspection System: An In Vitro Study. J. Int. Soc. Prev. Community Dent. 2020, 10, 736–742. [Google Scholar] [PubMed]
- Bin Hassan, S.; Alshadidi, A.; Aldosari, L.; Heboyan, A.; Singh, R. Effect of Chemical Disinfection on the Dimensional Stability of Polyvinyl Ether Siloxane Impression Material: A Systemic Review and Meta-Analysis. BMC Oral Health 2023, 23, 471. [Google Scholar] [CrossRef] [PubMed]
- Wezgowiec, J.; Paradowska-Stolarz, A.; Malysa, A.; Orzeszek, S.; Seweryn, P.; Wieckiewicz, M. Effects of Various Disinfection Methods on the Material Properties of Silicone Dental Impressions of Different Types and Viscosities. Int. J. Mol. Sci. 2022, 23, 10859. [Google Scholar] [CrossRef] [PubMed]
- Bud, E.S.; Bocanet, V.I.; Muntean, M.H.; Vlasa, A.; Păcurar, M.; Zetu, I.N.; Soporan, B.I.; Bud, A. Extra-Oral Three-Dimensional (3D) Scanning Evaluation of Three Different Impression Materials—An In Vitro Study. Polymers 2022, 14, 3678. [Google Scholar] [CrossRef] [PubMed]
- Jones, J. Dimensional Stability of Condensation and Addition Silicones in Dental Impressions. J. Dent. Res. 2014, 93, 150–155. [Google Scholar]
- Smith, M.; Johnson, L. Comparison of the Dimensional Stability of Condensation and Addition Silicone Impression Materials. J. Prosthet. Dent. 2015, 113, 177–182. [Google Scholar]
- Torassian, G.; Kau, C.H.; English, J.D.; Powers, J.; Bussa, H.I.; Marie Salas-Lopez, A.; Corbett, J.A. Digital models vs plaster models using alginate and alginate substitute materials. Angle Orthod. 2010, 80, 662–669. [Google Scholar] [CrossRef] [PubMed]
- Singh, I.; Singh, K.; Sethi, N. Digital Impression in Dentistry-A Comprehensive Review. Asian Pac. J. Health Sci. 2022, 9, 133–138. [Google Scholar] [CrossRef]
- Zahid, S.; Qadir, S.; Bano, N.; Qureshi, S.; Kaleem, M. Evaluation of the dimensional stability of alginate impression materials immersed in various disinfectant solutions. Pak. Oral Dent. J. 2017, 37, 371–376. [Google Scholar]
- Indahyani, D.; Barid, I.; Anggraeni, P. The Value of Imbibition and Syneresis for Dental Impression on Red Seaweed: A Laboratory Experiment. Padjadjaran J. Dent. 2024, 35, 274. [Google Scholar] [CrossRef]
- Peutzfeldt, A.; Asmussen, E. Accuracy of alginate and elastomeric impression materials. Eur. J. Oral Sci. 1989, 97, 375–379. [Google Scholar] [CrossRef] [PubMed]
- Sharma, S.; Kumar, G.; Narula, S.; Sharma, K. Comparative Analysis of Dimensional Accuracy of Vinylsiloxane Ether, Polyvinylsiloxane and Extended Pour Alginate Impression Materials—An in Vitro Study. Sch. J. Appl. Med. Sci. 2020. [Google Scholar] [CrossRef]
- Rehab, A.; Al-Naqash, W.A. The effect of Silver-Zinc zeolite incorporation on some properties of condensation silicone impression materials. J. Baghdad Coll. Dent. 2016, 28, 22–27. [Google Scholar]
- Giri, T.; Banerjee, S.; Banerjee, T.; Mandal, B.; Dongre, P.; Khanna, P.; Giri, D. A Comparative Study to Evaluate the Linear Dimensional Change and Compression Resistance of Four Elastomeric Interocclusal Recording Materials: An in vitro Study. J. Pharm. Bioallied Sci. 2024, 16, S834–S837. [Google Scholar] [CrossRef]
- Novac, A.C.; Filip, V.; Negruț, D.; Moldovan, I.; Pop, D.M.; Tănase, A.; Zaharia, C.; Crăciunescu, E.L.; Negruțiu, M.L.; Romînu, M.; et al. Time Assessment in Classical vs Digital Impressions. Rom. J. Oral Rehabil. 2023, 15. [Google Scholar]
- Donovan, T.E. Dental biomaterials. In Sturdevant’s Art and Science of Operative Dentistry; Elsevier: New York, NY, USA, 2019; pp. 453–510. [Google Scholar]
- Nouri, N.; Amini, P.; Amini, R.; Mousavi, M.; Estabragh, S.R.; Ebrahimi, A. Dimensional Accuracy of Polyvinyl Siloxane Impression Materials Considering Impression Techniques—A Literature Review. J. Dent. Sch. 2019, 37, 32–39. [Google Scholar]
- Lee, J.D.; Gallucci, G.O.; Lee, S.J. An In-Vitro Evaluation of Articulation Accuracy for Digitally Milled Models vs. Conventional Gypsum Casts. Dent. J. 2022, 10, 11. [Google Scholar] [CrossRef] [PubMed]
- Sayed, M.E.; Alshehri, A.H.; Al-Makramani, B.M.A.; Al-Sanabani, F.; Shaabi, F.I.; Alsurayyie, F.H.; Ahmed, W.M.; Al-Mansour, H.; Jain, S. Accuracy of Master Casts Generated Using Conventional and Digital Impression Modalities: Part 1—The Half-Arch Dimension. Appl. Sci. 2021, 11, 12034. [Google Scholar] [CrossRef]
- Sayed, M.E.; Al-Mansour, H.; Alshehri, A.H.; Al-Sanabani, F.; Al-Makramani, B.M.A.; Mugri, M.H.; Ahmed, W.M.; Alqahtani, N.M.; Bukhary, D.M.; Alsurayyie, F.H.; et al. Accuracy of Master Casts Generated Using Conventional and Digital Impression Modalities: Part 2—The Full Arch Dimension. Appl. Sci. 2022, 12, 2148. [Google Scholar] [CrossRef]
- Perlea, P.; Stefanescu, C.; Dalaban, M.-G.; Petre, A.-E. Experimental Study on Dimensional Variations of 3D Printed Dental Models Based on Printing Orientation. Clin. Case Rep. 2024, 12, e8630. [Google Scholar] [CrossRef] [PubMed]
- Sampaio-Fernandes, M.A.; Pinto, R.; Almeida, P.R.; Sampaio-Fernandes, M.M.; Marques, D.; Figueiral, M.H. Accuracy of Extraoral Digital Impressions with Multi-Unit Implants. Appl. Sci. 2023, 13, 8769. [Google Scholar] [CrossRef]
- Pera, F.; Pesce, P.; Bagnasco, F.; Pancini, N.; Carossa, M.; Baldelli, L.; Annunziata, M.; Migliorati, M.; Baldi, D.; Menini, M. Comparison of Milled Full-Arch Implant-Supported Frameworks Realised with a Full Digital Workflow or from Conventional Impression: A Clinical Study. Materials 2023, 16, 833. [Google Scholar] [CrossRef] [PubMed]
- D’Ambrosio, F.; Giordano, F.; Sangiovanni, G.; Di Palo, M.P.; Amato, M. Conventional versus Digital Dental Impression Techniques: What Is the Future? An Umbrella Review. Prosthesis 2023, 5, 851–875. [Google Scholar] [CrossRef]
- Albanchez-González, M.I.; Brinkmann, J.C.; Peláez-Rico, J.; López-Suárez, C.; Rodríguez-Alonso, V.; Suárez-García, M.J. Accuracy of Digital Dental Implants Impression Taking with Intraoral Scanners Compared with Conventional Impression Techniques: A Systematic Review of In Vitro Studies. Int. J. Environ. Res. Public Health 2022, 19, 2026. [Google Scholar] [CrossRef] [PubMed]
- Tabesh, M.; Nejatidanesh, F.; Savabi, G.; Davoudi, A.; Savabi, O. Marginal Accuracy of Lithium Disilicate Full-Coverage Single Crowns Made by Direct and Indirect Digital or Conventional Workflows: A Systematic Review and Meta-Analysis. J. Prosthodont. 2022, 31, 744–753. [Google Scholar] [CrossRef] [PubMed]
- Valenti, C.; Isabella Federici, M.; Masciotti, F.; Marinucci, L.; Xhimitiku, I.; Cianetti, S.; Pagano, S. Mechanical properties of 3D-printed prosthetic materials compared with milled and conventional processing: A systematic review and meta-analysis of in vitro studies. J. Prosthet. Dent. 2022, in press. [CrossRef]
- Parize, H.; Dias Corpa Tardelli, J.; Bohner, L.; Sesma, N.; Muglia, V.A.; Cândido Dos Reis, A. Digital versus conventional workflow for the fabrication of physical casts for fixed prosthodontics: A systematic review of accuracy. J. Prosthet. Dent. 2022, 128, 25–32. [Google Scholar] [CrossRef] [PubMed]
- Manicone, P.F.; De Angelis, P.; Rella, E.; Damis, G.; D’Addona, A. Patient preference and clinical working time between digital scanning and conventional impression making for implant-supported prostheses: A systematic review and meta-analysis. J. Prosthet. Dent. 2022, 128, 589–596. [Google Scholar] [CrossRef] [PubMed]
- Kong, L.; Li, Y.; Liu, Z. Digital versus conventional full-arch impressions in linear and 3D accuracy: A systematic review and meta-analysis of in vivo studies. Clin. Oral Investig. 2022, 26, 5625–5642. [Google Scholar] [CrossRef] [PubMed]
- Naumovski, B.; Kapushevska, B. Dimensional Stability and Accuracy of Silicone—Based Impression Materials Using Different Impression Techniques—A Literature Review. Prilozi 2017, 38, 131–138. [Google Scholar] [CrossRef] [PubMed]









| Materials | Rigid and Semi-Rigid | Elastics |
|---|---|---|
| Irreversible | Gypsum Acrylic Resin Zinc Oxide Eugenol paste | Alginates Polysulfides Polyethers Silicones (condensation or addition) |
| Reversible | Waxes Thermoplastic materials Bucco-plastic materials Gutta-percha | Agar-agar hydrocolloids |
| Tooth | Conventional Impressions: Group 1 (CA) | Mouthguard-Reinforced Impressions: Group 4 (RA) | p M–W | |||
|---|---|---|---|---|---|---|
| Mean ± SD (μm) | Median (Interquartile Range) (μm) | Mean ± SD (μm) | Median (Interquartile Range) (μ) | |||
| 16 | BO | 3199.9 ± 73.38 | 3221.5 (53) | 3299.1 ± 120.46 | 3361 (216) | 0.005 |
| MD | 3363.5 ± 98.09 | 3374.5 (137) | 3575.3 ± 75.96 | 3549 (106) | <0.001 | |
| 13 | BO | 2403.1 ± 154.34 | 2461.5 (313) | 2588.9 ± 91.1 | 2571.5 (155) | <0.001 |
| MD | 2565.9 ± 419.36 | 2426 (189) | 2569.6 ± 90.14 | 2579.5 (153) | 0.001 | |
| 23 | BO | 2588.2 ± 95.83 | 2582.5 (156) | 2739.5 ± 133.99 | 2818 (223) | <0.001 |
| MD | 2324.9 ± 118.77 | 2340 (160) | 2378.8 ± 60.18 | 2375.5 (90) | 0.026 | |
| 26 | BO | 3267.4 ± 89.82 | 3245 (74) | 3404.5 ± 00.48 | 3435 (175) | <0.001 |
| MD | 3407.9 ± 51.55 | 3406.5 (87) | 3474.6 ± 70.9 | 3479 (85) | <0.001 | |
| Tooth | Conventional Impressions: Group 2 (CCS) | Mouthguard-Reinforced Impressions: Group 5 (RCS) | p M–W | |||
|---|---|---|---|---|---|---|
| Mean ± SD (μm) | Median (Interquartile Range) (μm) | Mean ± SD (μm) | Median (Interquartile Range) (μm) | |||
| 16 | BO | 3209.8 ± 89.14 | 3186 (56) | 3257 ± 89.86 | 3220 (114) | 0.003 |
| MD | 3523.2 ± 98.33 | 3493 (71) | 3522.3 ± 59.87 | 3530 (80) | 0.227 | |
| 13 | BO | 2539.2 ± 88.79 | 2496 (140) | 2523.4 ± 43.14 | 2530.5 (76) | 0.988 |
| MD | 2509.3 ± 82.9 | 2475.5 (53) | 2504.1 ± 92.88 | 2466 (151) | 0.290 | |
| 23 | BO | 2596.3 ± 139.86 | 2534 (31) | 2647.6 ± 100.98 | 2607.5 (73) | <0.001 |
| MD | 2343.1 ± 64.48 | 2323.5 (39) | 2309.9 ± 55.85 | 2315 (74) | 0.218 | |
| 26 | BO | 3329.2 ± 102 | 3291 (64) | 3397.5 ± 75.98 | 3395.5 (140) | <0.001 |
| MD | 3438.4 ± 98.21 | 3472 (168) | 3392.8 ± 94.93 | 3418.5 (104) | 0.065 | |
| Tooth | Conventional Impressions: Group 3 (CAS) | Mouthguard-Reinforced Impressions: Group 6 (RAS) | p M–W | |||
|---|---|---|---|---|---|---|
| Mean ± SD (μm) | Median (Interquartile Range) (μm) | Mean ± SD (μm) | Median (Interquartile Range) (μm) | |||
| 16 | BO | 3273.3 ± 57.95 | 3289 (71) | 3200.3 ± 32.8 | 3198.5 (43) | <0.001 |
| MD | 3408.4 ± 120.81 | 3426 (234) | 3479.7 ± 61.87 | 3504 (38) | 0.055 | |
| 13 | BO | 2509.2 ± 63.77 | 2486.5 (36) | 2455.6 ± 21.51 | 2454 (30) | <0.001 |
| MD | 2436.6 ± 87.35 | 2453.5 (90) | 2340.8 ± 105.22 | 2293.5 (181) | 0.001 | |
| 23 | BO | 2567.5 ± 60.32 | 2566.5 (114) | 2539.9 ± 71.05 | 2527.5 (149) | 0.022 |
| MD | 2303.5 ± 107.95 | 2273 (62) | 2210.4 ± 77.83 | 2204.5 (162) | 0.003 | |
| 26 | BO | 3253.2 ± 71.51 | 3289 (146) | 3218.8 ± 42.12 | 3239.5 (58) | 0.019 |
| MD | 3451.5 ± 98.82 | 3498.5 (92) | 3413.3 ± 72.94 | 3368 (137) | 0.017 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Novac, A.C.; Tudor, A.; Pop, D.M.; Neagu, C.S.; Crăciunescu, E.L.; Romînu, M.; Negruțiu, M.L.; Duma, V.-F.; Sinescu, C. Conventional Dental Impressions vs. Impressions Reinforced with Rigid Mouthguards. Polymers 2024, 16, 994. https://doi.org/10.3390/polym16070994
Novac AC, Tudor A, Pop DM, Neagu CS, Crăciunescu EL, Romînu M, Negruțiu ML, Duma V-F, Sinescu C. Conventional Dental Impressions vs. Impressions Reinforced with Rigid Mouthguards. Polymers. 2024; 16(7):994. https://doi.org/10.3390/polym16070994
Chicago/Turabian StyleNovac, Andreea Codruta, Anca Tudor, Daniela Maria Pop, Carina Sonia Neagu, Emanuela Lidia Crăciunescu, Mihai Romînu, Meda Lavinia Negruțiu, Virgil-Florin Duma, and Cosmin Sinescu. 2024. "Conventional Dental Impressions vs. Impressions Reinforced with Rigid Mouthguards" Polymers 16, no. 7: 994. https://doi.org/10.3390/polym16070994
APA StyleNovac, A. C., Tudor, A., Pop, D. M., Neagu, C. S., Crăciunescu, E. L., Romînu, M., Negruțiu, M. L., Duma, V. -F., & Sinescu, C. (2024). Conventional Dental Impressions vs. Impressions Reinforced with Rigid Mouthguards. Polymers, 16(7), 994. https://doi.org/10.3390/polym16070994