
Fertility in Cystinosis


{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Fertility in Female Cystinosis Patients
3. Fertility in Male Cystinosis Patients
3.1. Sexual Hormone Levels
3.2. Testicular Volume and Histology
3.3. Semen Analysis
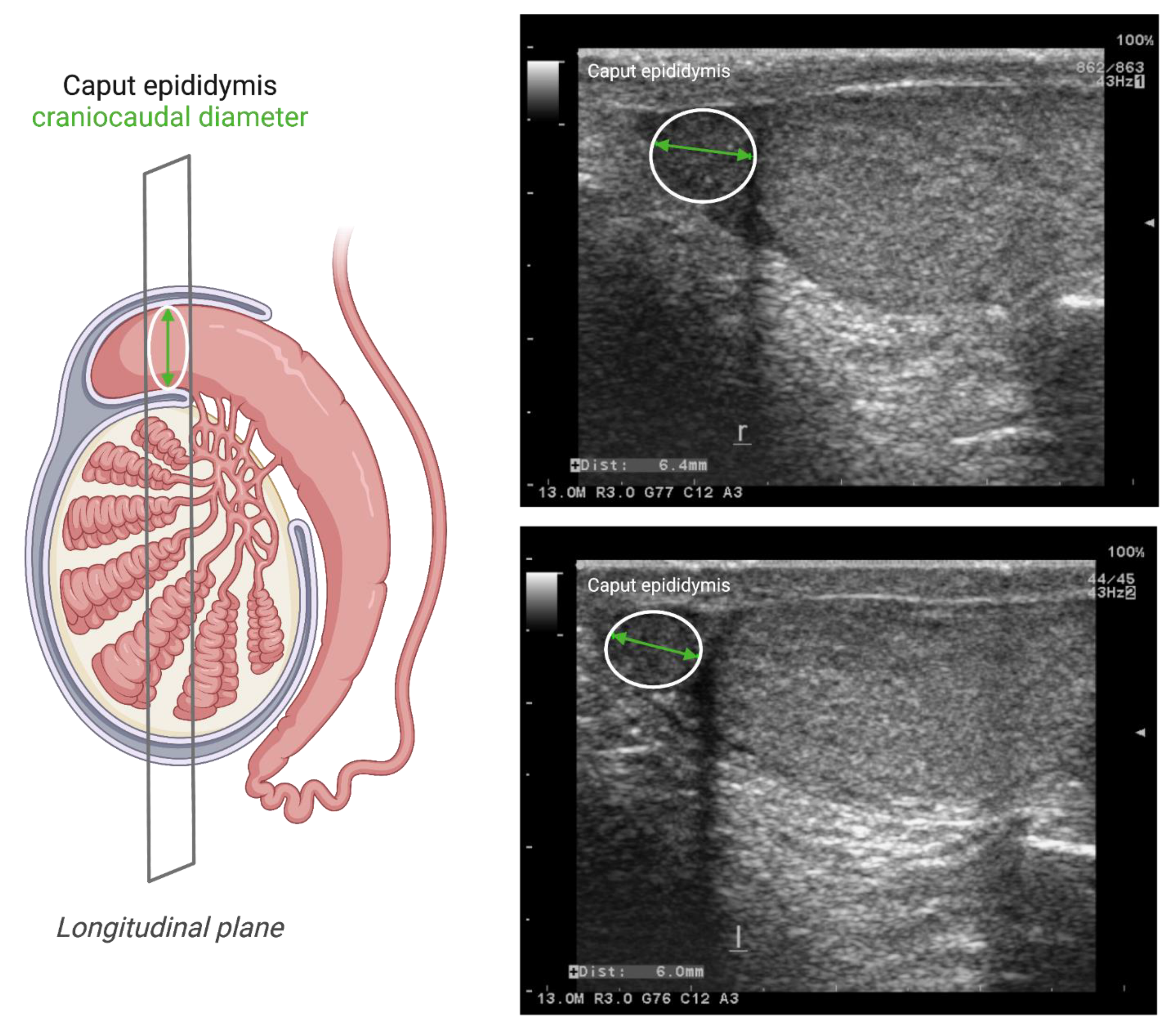
3.4. Scrotal Ultrasound Imaging
3.5. Seminal Plasma Markers
4. Fertility in Cystinosis Animal Models
In Vitro Studies in Cystinosis
5. Effect of Cysteamine on Fertility
6. Future Perspectives
7. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Town, M.; Jean, G.; Cherqui, S.; Attard, M.; Forestier, L.; Whitmore, S.A.; Callen, D.F.; Gribouval, O.; Broyer, M.; Bates, G.P.; et al. A novel gene encoding an integral membrane protein is mutated in nephropathic cystinosis. Nat. Genet. 1998, 18, 319–324. [Google Scholar] [CrossRef]
- Gahl, W.A.; Thoene, J.G.; Schneider, J.A. Cystinosis. N. Engl. J. Med. 2002, 347, 111–121. [Google Scholar] [CrossRef]
- Emma, F.; Nesterova, G.; Langman, C.; Labbe, A.; Cherqui, S.; Goodyer, P.; Janssen, M.C.; Greco, M.; Topaloglu, R.; Elenberg, E.; et al. Nephropathic cystinosis: An international consensus document. Nephrol. Dial. Transplant. 2014, 29 (Suppl. 4), iv87–iv94. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blakey, H.; Proudfoot-Jones, J.; Knox, E.; Lipkin, G. Pregnancy in women with cystinosis. Clin. Kidney J. 2019, 12, 855–858. [Google Scholar] [CrossRef]
- Wosnitzer, M.; Goldstein, M.; Hardy, M.P. Review of Azoospermia. Spermatogenesis 2014, 4, e28218. [Google Scholar] [CrossRef] [Green Version]
- Wosnitzer, M.S.; Goldstein, M. Obstructive azoospermia. Urol. Clin. N. Am. 2014, 41, 83–95. [Google Scholar] [CrossRef]
- Elmonem, M.A.; Veys, K.R.; Soliman, N.A.; van Dyck, M.; van den Heuvel, L.P.; Levtchenko, E. Cystinosis: A review. Orphanet J. Rare Dis. 2016, 11, 47. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Winkler, L.; Offner, G.; Krull, F.; Brodehl, J. Growth and pubertal development in nephropathic cystinosis. Eur. J. Pediatr. 1993, 152, 244–249. [Google Scholar] [CrossRef]
- Reiss, R.E.; Kuwabara, T.; Smith, M.L.; Gahl, W.A. Successful pregnancy despite placental cystine crystals in a woman with nephropathic cystinosis. N. Engl. J. Med. 1988, 319, 223–226. [Google Scholar] [CrossRef] [PubMed]
- Andrews, P.A.; Sacks, S.H.; van’t Hoff, W. Successful pregnancy in cystinosis. JAMA 1994, 272, 1327–1328. [Google Scholar] [CrossRef]
- Haase, M.; Morgera, S.; Bamberg, C.; Halle, H.; Martini, S.; Dragun, D.; Neumayer, H.H.; Budde, K. Successful pregnancies in dialysis patients including those suffering from cystinosis and familial Mediterranean fever. J. Nephrol. 2006, 19, 677–681. [Google Scholar] [PubMed]
- Ramappa, A.J.; Pyatt, J.R. Pregnancy-associated cardiomyopathy occurring in a young patient with nephropathic cystinosis. Cardiol. Young 2010, 20, 220–222. [Google Scholar] [CrossRef] [PubMed]
- Chuang, Y.W.; Wen, M.C.; Wu, M.J.; Shu, K.H.; Cheng, C.H.; Yu, T.M.; Huang, S.T.; Chen, C.H. Follow-up and treatment of renal transplantation with nephropathic cystinosis in central Taiwan. Transplant. Proc. 2012, 44, 80–82. [Google Scholar] [CrossRef]
- Deshpande, N.A.; James, N.T.; Kucirka, L.M.; Boyarsky, B.J.; Garonzik-Wang, J.M.; Montgomery, R.A.; Segev, D.L. Pregnancy outcomes in kidney transplant recipients: A systematic review and meta-analysis. Am. J. Transplant. 2011, 11, 2388–2404. [Google Scholar] [CrossRef]
- Kuczborska, K.; Gozdowska, J.; Lewandowska, D.; Grenda, R.; Galazka, Z.; Nazarewski, S.; Durlik, M. Therapeutic Problems and Pregnancy in a Patient With Infantile Nephropathic Cystinosis: A Case Report. Transplant. Proc. 2019, 51, 545–547. [Google Scholar] [CrossRef]
- Ariceta, G.; Camacho, J.A.; Fernandez-Obispo, M.; Fernandez-Polo, A.; Gamez, J.; Garcia-Villoria, J.; Lara Monteczuma, E.; Leyes, P.; Martin-Begue, N.; Oppenheimer, F.; et al. Cystinosis in adult and adolescent patients: Recommendations for the comprehensive care of cystinosis. Nefrologia 2015, 35, 304–321. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boman, H.; Schneider, J.A. Prenatal diagnosis of nephropathic cystinosis. Pregnancy at risk ascertained through heterozygote diagnosis of parents. Acta Paediatr. Scand. 1981, 70, 389–393. [Google Scholar] [CrossRef] [PubMed]
- Chik, C.L.; Friedman, A.; Merriam, G.R.; Gahl, W.A. Pituitary-testicular function in nephropathic cystinosis. Ann. Intern. Med. 1993, 119, 568–575. [Google Scholar] [CrossRef] [PubMed]
- Besouw, M.T.; Kremer, J.A.; Janssen, M.C.; Levtchenko, E.N. Fertility status in male cystinosis patients treated with cysteamine. Fertil. Steril. 2010, 93, 1880–1883. [Google Scholar] [CrossRef] [Green Version]
- Reda, A.; Veys, K.; Kadam, P.; Taranta, A.; Rega, L.R.; Goffredo, B.M.; Camps, C.; Besouw, M.; Cyr, D.; Albersen, M.; et al. Human and animal fertility studies in cystinosis reveal signs of obstructive azoospermia, an altered blood-testis barrier and a subtherapeutic effect of cysteamine in testis. J. Inherit. Metab. Dis. 2021, 44, 1393–1408. [Google Scholar] [CrossRef]
- Rohayem, J.; Haffner, D.; Cremers, J.F.; Huss, S.; Wistuba, J.; Weitzel, D.; Kliesch, S.; Hohenfellner, K. Testicular function in males with infantile nephropathic cystinosis. Hum. Reprod. 2021, 36, 1191–1204. [Google Scholar] [CrossRef]
- O’Connor, A.E.; De Kretser, D.M. Inhibins in normal male physiology. Semin. Reprod. Med. 2004, 22, 177–185. [Google Scholar] [CrossRef]
- Pierik, F.H.; Vreeburg, J.T.; Stijnen, T.; De Jong, F.H.; Weber, R.F. Serum inhibin B as a marker of spermatogenesis. J. Clin. Endocrinol. Metab. 1998, 83, 3110–3114. [Google Scholar] [CrossRef] [PubMed]
- Bordallo, M.A.; Guimaraes, M.M.; Pessoa, C.H.; Carrico, M.K.; Dimetz, T.; Gazolla, H.M.; Dobbin, J.; Castilho, I.A. Decreased serum inhibin B/FSH ratio as a marker of Sertoli cell function in male survivors after chemotherapy in childhood and adolescence. J. Pediatr. Endocrinol. Metab. 2004, 17, 879–887. [Google Scholar] [CrossRef]
- Gurung, P.; Yetiskul, E.; Jialal, I. Physiology, Male Reproductive System. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2021. [Google Scholar]
- Johnsen, S.G. Testicular biopsy score count—A method for registration of spermatogenesis in human testes: Normal values and results in 335 hypogonadal males. Hormones 1970, 1, 2–25. [Google Scholar] [CrossRef] [PubMed]
- Veys, K.R.; D’Hauwers, K.W.; van Dongen, A.; Janssen, M.C.; Besouw, M.T.P.; Goossens, E.; van den Heuvel, L.P.; Wetzels, A.; Levtchenko, E.N. First Successful Conception Induced by a Male Cystinosis Patient. JIMD Rep. 2018, 38, 1–6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pezzella, A.; Barbonetti, A.; Micillo, A.; D’Andrea, S.; Necozione, S.; Gandini, L.; Lenzi, A.; Francavilla, F.; Francavilla, S. Ultrasonographic determination of caput epididymis diameter is strongly predictive of obstruction in the genital tract in azoospermic men with normal serum FSH. Andrology 2013, 1, 133–138. [Google Scholar] [CrossRef] [PubMed]
- Drabovich, A.P.; Dimitromanolakis, A.; Saraon, P.; Soosaipillai, A.; Batruch, I.; Mullen, B.; Jarvi, K.; Diamandis, E.P. Differential diagnosis of azoospermia with proteomic biomarkers ECM1 and TEX101 quantified in seminal plasma. Sci. Transl. Med. 2013, 5, 212ra160. [Google Scholar] [CrossRef]
- Lei, B.; Xing, R.; Zhou, X.; Lv, D.; Wan, B.; Shu, F.; Zhong, L.; Wu, H.; Mao, X. Neutral alpha-1,4-glucosidase and fructose levels contribute to discriminating obstructive and nonobstructive azoospermia in Chinese men with azoospermia. Andrologia 2016, 48, 670–675. [Google Scholar] [CrossRef]
- Eertmans, F.; Bogaert, V.; Van Poecke, T.; Puype, B. An Improved Neutral a-Glucosidase Assay for Assessment of Epididymal Function-Validation and Comparison to the WHO Method. Diagnostics 2014, 4, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Besouw, M.T.; van Pelt, A.M.; Gaide Chevronnay, H.P.; Courtoy, P.J.; Pastore, A.; Goossens, E.; Devuyst, O.; Antignac, C.; Levtchenko, E.N. Studying nonobstructive azoospermia in cystinosis: Histologic examination of testes and epididymis and sperm analysis in a Ctns(-)/(-) mouse model. Fertil. Steril. 2012, 98, 162–165. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nevo, N.; Chol, M.; Bailleux, A.; Kalatzis, V.; Morisset, L.; Devuyst, O.; Gubler, M.C.; Antignac, C. Renal phenotype of the cystinosis mouse model is dependent upon genetic background. Nephrol. Dial. Transplant. 2010, 25, 1059–1066. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Janne, P.A.; Suchy, S.F.; Bernard, D.; MacDonald, M.; Crawley, J.; Grinberg, A.; Wynshaw-Boris, A.; Westphal, H.; Nussbaum, R.L. Functional overlap between murine Inpp5b and Ocrl1 may explain why deficiency of the murine ortholog for OCRL1 does not cause Lowe syndrome in mice. J. Clin. Investig. 1998, 101, 2042–2053. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bijvoet, A.G.; van de Kamp, E.H.; Kroos, M.A.; Ding, J.H.; Yang, B.Z.; Visser, P.; Bakker, C.E.; Verbeet, M.P.; Oostra, B.A.; Reuser, A.J.; et al. Generalized glycogen storage and cardiomegaly in a knockout mouse model of Pompe disease. Hum. Mol. Genet. 1998, 7, 53–62. [Google Scholar] [CrossRef] [PubMed]
- Schultheis, P.J.; Lorenz, J.N.; Meneton, P.; Nieman, M.L.; Riddle, T.M.; Flagella, M.; Duffy, J.J.; Doetschman, T.; Miller, M.L.; Shull, G.E. Phenotype resembling Gitelman’s syndrome in mice lacking the apical Na+-Cl- cotransporter of the distal convoluted tubule. J. Biol. Chem. 1998, 273, 29150–29155. [Google Scholar] [CrossRef] [Green Version]
- Elmonem, M.A.; Khalil, R.; Khodaparast, L.; Khodaparast, L.; Arcolino, F.O.; Morgan, J.; Pastore, A.; Tylzanowski, P.; Ny, A.; Lowe, M.; et al. Cystinosis (ctns) zebrafish mutant shows pronephric glomerular and tubular dysfunction. Sci. Rep. 2017, 7, 42583. [Google Scholar] [CrossRef] [Green Version]
- Berlingerio, S.P.; He, J.; De Groef, L.; Taeter, H.; Norton, T.; Baatsen, P.; Cairoli, S.; Goffredo, B.; de Witte, P.; van den Heuvel, L.; et al. Renal and Extra Renal Manifestations in Adult Zebrafish Model of Cystinosis. Int. J. Mol. Sci. 2021, 22, 9398. [Google Scholar] [CrossRef]
- Dube, E.; Dufresne, J.; Chan, P.T.; Hermo, L.; Cyr, D.G. Assessing the role of claudins in maintaining the integrity of epididymal tight junctions using novel human epididymal cell lines. Biol. Reprod. 2010, 82, 1119–1128. [Google Scholar] [CrossRef]
- Mandl, A.M. The Effect of Cysteamine on the Survival of Spermatogonia after X-irradiation. Int. J. Radiat. Biol. Relat. Stud. Phys. Chem. Med. 1959, 1, 131–142. [Google Scholar] [CrossRef]
- Starkie, C.M. The effect of cysteamine on the survival of foetal germ cells after irradiation. Int. J. Radiat. Biol. Relat. Stud. Phys. Chem. Med. 1961, 3, 609–617. [Google Scholar] [CrossRef]
- Sariozkan, S.; Tuncer, P.B.; Buyukleblebici, S.; Bucak, M.N.; Canturk, F.; Eken, A. Antioxidative effects of cysteamine, hyaluronan and fetuin on post-thaw semen quality, DNA integrity and oxidative stress parameters in the Brown Swiss bull. Andrologia 2015, 47, 138–147. [Google Scholar] [CrossRef]
- Bucak, M.N.; Atessahin, A.; Varisli, O.; Yuce, A.; Tekin, N.; Akcay, A. The influence of trehalose, taurine, cysteamine and hyaluronan on ram semen Microscopic and oxidative stress parameters after freeze-thawing process. Theriogenology 2007, 67, 1060–1067. [Google Scholar] [CrossRef] [PubMed]
- Bucak, M.N.; Tuncer, P.B.; Sariozkan, S.; Ulutas, P.A.; Coyan, K.; Baspinar, N.; Ozkalp, B. Effects of hypotaurine, cysteamine and aminoacids solution on post-thaw microscopic and oxidative stress parameters of Angora goat semen. Res. Vet. Sci. 2009, 87, 468–472. [Google Scholar] [CrossRef] [PubMed]
- Tuncer, P.B.; Buyukleblebici, S.; Eken, A.; Tasdemir, U.; Durmaz, E.; Buyukleblebici, O.; Coskun, E. Comparison of cryoprotective effects of lycopene and cysteamine in different cryoprotectants on bull semen and fertility results. Reprod. Domest. Anim. 2014, 49, 746–752. [Google Scholar] [CrossRef] [PubMed]
- Swami, D.S.; Kumar, P.; Malik, R.K.; Saini, M.; Kumar, D.; Jan, M.H. Cysteamine supplementation revealed detrimental effect on cryosurvival of buffalo sperm based on computer-assisted semen analysis and oxidative parameters. Anim. Reprod. Sci. 2017, 177, 56–64. [Google Scholar] [CrossRef] [PubMed]
- Anderson, R.A.; Feathergill, K.; Kirkpatrick, R.; Zaneveld, L.J.D.; Coleman, K.T.; Spear, P.G.; Cooper, M.D.; Waller, D.P.; Thoene, J.G. Characterization of cysteamine as a potential contraceptive anti-HIV agent. J. Androl. 1998, 19, 37–49. [Google Scholar] [PubMed]
- Wang, Y.; Zhao, Y.; Yu, S.; Feng, Y.; Zhang, H.; Kou, X.; Chu, M.; Cui, L.; Li, L.; Zhang, P.; et al. Regulation of steroid hormones and energy status with cysteamine and its effect on spermatogenesis. Toxicol. Appl. Pharmacol. 2016, 313, 149–158. [Google Scholar] [CrossRef] [PubMed]
- Assadi, F.K.; Mullin, J.J.; Beckman, D.A. Evaluation of the reproductive and developmental safety of cysteamine in the rat: Effects on female reproduction and early embryonic development. Teratology 1998, 58, 88–95. [Google Scholar] [CrossRef]


Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Reda, A.; Veys, K.; Besouw, M. Fertility in Cystinosis. Cells 2021, 10, 3539. https://doi.org/10.3390/cells10123539
Reda A, Veys K, Besouw M. Fertility in Cystinosis. Cells. 2021; 10(12):3539. https://doi.org/10.3390/cells10123539
Chicago/Turabian StyleReda, Ahmed, Koenraad Veys, and Martine Besouw. 2021. "Fertility in Cystinosis" Cells 10, no. 12: 3539. https://doi.org/10.3390/cells10123539
APA StyleReda, A., Veys, K., & Besouw, M. (2021). Fertility in Cystinosis. Cells, 10(12), 3539. https://doi.org/10.3390/cells10123539