
Vascular Calcification Progression Modulates the Risk Associated with Vascular Calcification Burden in Incident to Dialysis Patients

 , , ,
, , ,  and
and
Abstract
:Study Highlights
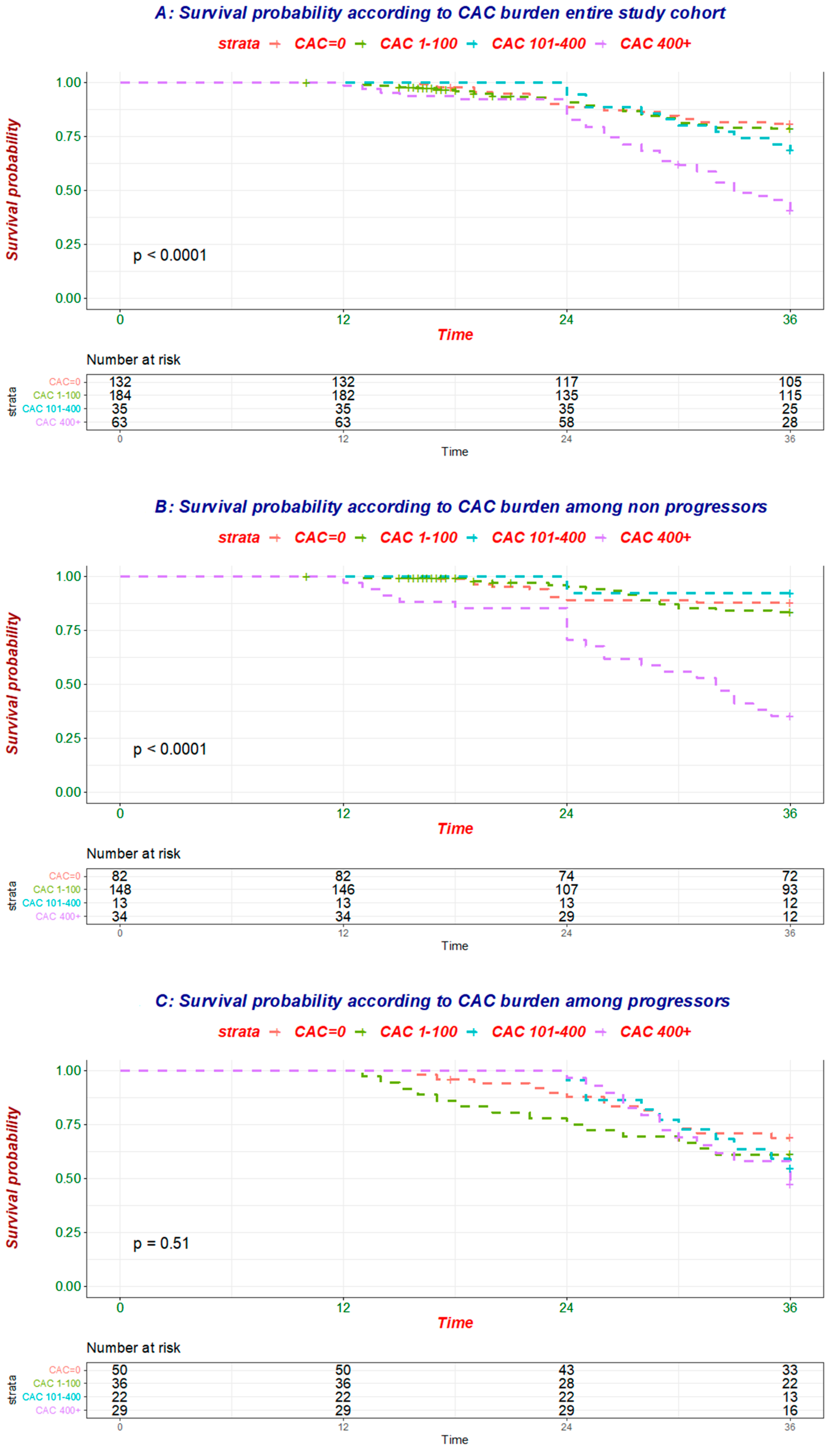
- Coronary artery calcification (CAC) burden portends poor prognosis (hazard ratio (HR) for all-cause mortality: 1.29; 95% confidence interval (95% CI): 1.17–1.44) in incident to dialysis patients.
- CAC progression (CACP) portends poor prognosis (HR for all-cause mortality: 5.16; 2.61–10.21) in incident to dialysis patients.
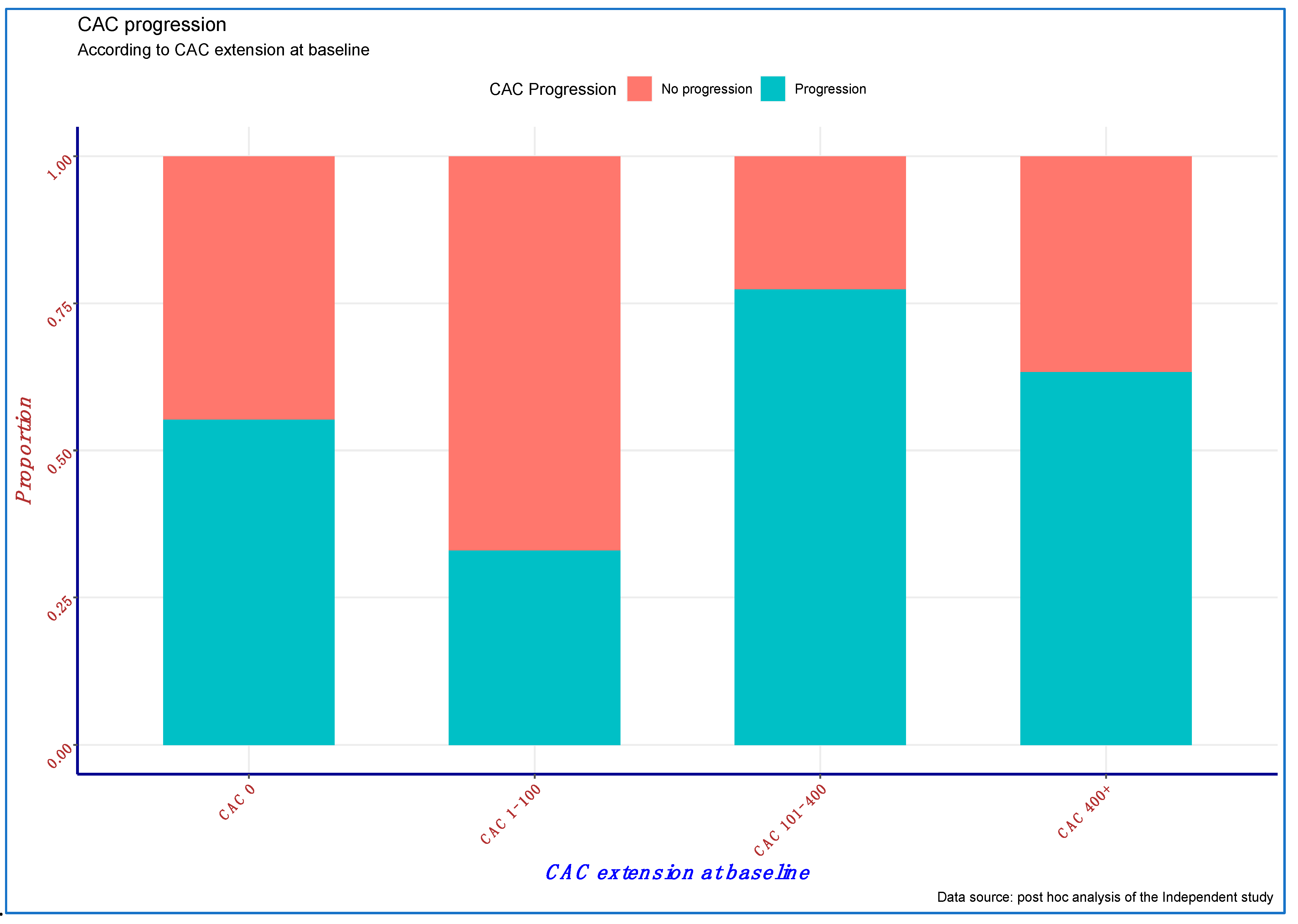
- CACP mitigated the risk associated with CAC burden (p = 0.002).
- Calcium-free phosphate binder is associated with survival benefit.
- Adjustment for calcium-free phosphate binder attenuated the strength of the link between CACP and mortality, suggesting that CACP modulation may improve survival in incident to dialysis patients.
1. Introduction
2. Material and Methods
2.1. Study Cohort and Endpoint of Interest
2.2. Demographic, Clinical and Laboratory Characteristics, and Vascular Calcification Assessment
2.3. Statistical Analysis
3. Results
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Luyckx, V.A.; Tonelli, M.; Stanifer, J.W. The global burden of kidney disease and the sustainable development goals. Bull. World Health Organ. 2018, 96, 414–422D. [Google Scholar] [CrossRef]
- Mills, K.T.; Xu, Y.; Zhang, W.; Bundy, J.D.; Chen, C.S.; Kelly, T.N.; Chen, J.; He, J. A systematic analysis of worldwide population-based data on the global burden of chronic kidney disease in 2010. Kidney Int. 2015, 88, 950–957. [Google Scholar] [CrossRef] [Green Version]
- Turin, T.C.; Tonelli, M.; Manns, B.J.; Ravani, P.; Ahmed, S.B.; Hemmelgarn, B.R. Chronic kidney disease and life expectancy. Nephrol. Dial. Transpl. 2012, 27, 3182–3186. [Google Scholar] [CrossRef] [Green Version]
- Thompson, S.; James, M.; Wiebe, N.; Hemmelgarn, B.; Manns, B.; Klarenbach, S.; Tonelli, M.; Alberta Kidney Disease, N. Cause of Death in Patients with Reduced Kidney Function. J. Am. Soc. Nephrol. 2015, 26, 2504–2511. [Google Scholar] [CrossRef]
- Go, A.S.; Chertow, G.M.; Fan, D.; McCulloch, C.E.; Hsu, C.Y. Chronic kidney disease and the risks of death, cardiovascular events, and hospitalization. N. Engl. J. Med. 2004, 351, 1296–1305. [Google Scholar] [CrossRef] [PubMed]
- Raggi, P.; Giachelli, C.; Bellasi, A. Interaction of vascular and bone disease in patients with normal renal function and patients undergoing dialysis. Nat. Clin. Pr. Cardiovasc. Med. 2007, 4, 26–33. [Google Scholar] [CrossRef]
- Bellasi, A.; Raggi, P. Vascular calcification in chronic kidney disease: Usefulness of a marker of vascular damage. J. Nephrol. 2011, 24, S11–S15. [Google Scholar] [CrossRef]
- Nelson, A.J.; Raggi, P.; Wolf, M.; Gold, A.M.; Chertow, G.M.; Roe, M.T. Targeting Vascular Calcification in Chronic Kidney Disease. JACC Basic Transl. Sci. 2020, 5, 398–412. [Google Scholar] [CrossRef]
- Dilsizian, V.; Gewirtz, H.; Marwick, T.H.; Kwong, R.Y.; Raggi, P.; Al-Mallah, M.H.; Herzog, C.A. Cardiac Imaging for Coronary Heart Disease Risk Stratification in Chronic Kidney Disease. JACC Cardiovasc. Imaging 2021, 14, 669–682. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.; Budoff, M.J.; Reilly, M.P.; Yang, W.; Rosas, S.E.; Rahman, M.; Zhang, X.; Roy, J.A.; Lustigova, E.; Nessel, L.; et al. Coronary Artery Calcification and Risk of Cardiovascular Disease and Death Among Patients With Chronic Kidney Disease. JAMA Cardiol. 2017, 2, 635–643. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liabeuf, S.; Desjardins, L.; Diouf, M.; Temmar, M.; Renard, C.; Choukroun, G.; Massy, Z.A. The Addition of Vascular Calcification Scores to Traditional Risk Factors Improves Cardiovascular Risk Assessment in Patients with Chronic Kidney Disease. PLoS ONE 2015, 10, e0131707. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Block, G.A.; Raggi, P.; Bellasi, A.; Kooienga, L.; Spiegel, D.M. Mortality effect of coronary calcification and phosphate binder choice in incident hemodialysis patients. Kidney Int. 2007, 71, 438–441. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Budoff, M.J.; Hokanson, J.E.; Nasir, K.; Shaw, L.J.; Kinney, G.L.; Chow, D.; Demoss, D.; Nuguri, V.; Nabavi, V.; Ratakonda, R.; et al. Progression of coronary artery calcium predicts all-cause mortality. JACC Cardiovasc. Imaging 2010, 3, 1229–1236. [Google Scholar] [CrossRef] [Green Version]
- Di Iorio, B.R.; Cucciniello, E.; Bellizzi, V. Vascular calcification and QT interval in incident hemodialysis patients. J. Nephrol 2009, 22, 694–698. [Google Scholar] [PubMed]
- Di Iorio, B.; Molony, D.; Bell, C.; Cucciniello, E.; Bellizzi, V.; Russo, D.; Bellasi, A. Sevelamer versus calcium carbonate in incident hemodialysis patients: Results of an open-label 24-month randomized clinical trial. Am. J. Kidney Dis. 2013, 62, 771–778. [Google Scholar] [CrossRef]
- Agatston, A.S.; Janowitz, W.R.; Hildner, F.J.; Zusmer, N.R.; Viamonte, M., Jr.; Detrano, R. Quantification of coronary artery calcium using ultrafast computed tomography. J. Am. Coll. Cardiol. 1990, 15, 827–832. [Google Scholar] [CrossRef] [Green Version]
- Hokanson, J.E.; MacKenzie, T.; Kinney, G.; Snell-Bergeon, J.K.; Dabelea, D.; Ehrlich, J.; Eckel, R.H.; Rewers, M. Evaluating changes in coronary artery calcium: An analytic method that accounts for interscan variability. AJR Am. J. Roentgenol. 2004, 182, 1327–1332. [Google Scholar] [CrossRef]
- Raggi, P.; Bellasi, A.; Ferramosca, E.; Block, G.A.; Muntner, P. Pulse Wave Velocity Is Inversely Related to Vertebral Bone Density in Hemodialysis Patients. Hypertension 2007, 49, 1278–1284. [Google Scholar] [CrossRef] [Green Version]
- Shantouf, R.S.; Budoff, M.J.; Ahmadi, N.; Ghaffari, A.; Flores, F.; Gopal, A.; Noori, N.; Jing, J.; Kovesdy, C.P.; Kalantar-Zadeh, K. Total and individual coronary artery calcium scores as independent predictors of mortality in hemodialysis patients. Am. J. Nephrol. 2010, 31, 419–425. [Google Scholar] [CrossRef] [Green Version]
- Moe, S.; Drueke, T.; Cunningham, J.; Goodman, W.; Martin, K.; Olgaard, K.; Ott, S.; Sprague, S.; Lameire, N.; Eknoyan, G. Definition, evaluation, and classification of renal osteodystrophy: A position statement from Kidney Disease: Improving Global Outcomes (KDIGO). Kidney Int. 2006, 69, 1945–1953. [Google Scholar] [CrossRef] [Green Version]
- Bellasi, A.; Lacey, C.; Taylor, A.J.; Raggi, P.; Wilson, P.W.; Budoff, M.J.; Vaccarino, V.; Shaw, L.J. Comparison of prognostic usefulness of coronary artery calcium in men versus women (results from a meta- and pooled analysis estimating all-cause mortality and coronary heart disease death or myocardial infarction). Am. J. Cardiol. 2007, 100, 409–414. [Google Scholar] [CrossRef]
- Matsushita, K.; Sang, Y.; Ballew, S.H.; Shlipak, M.; Katz, R.; Rosas, S.E.; Peralta, C.A.; Woodward, M.; Kramer, H.J.; Jacobs, D.R.; et al. Subclinical atherosclerosis measures for cardiovascular prediction in CKD. J. Am. Soc. Nephrol. 2015, 26, 439–447. [Google Scholar] [CrossRef] [Green Version]
- Russo, D.; Corrao, S.; Battaglia, Y.; Andreucci, M.; Caiazza, A.; Carlomagno, A.; Lamberti, M.; Pezone, N.; Pota, A.; Russo, L.; et al. Progression of coronary artery calcification and cardiac events in patients with chronic renal disease not receiving dialysis. Kidney Int. 2011. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Criqui, M.H.; Denenberg, J.O.; Ix, J.H.; McClelland, R.L.; Wassel, C.L.; Rifkin, D.E.; Carr, J.J.; Budoff, M.J.; Allison, M.A. Calcium density of coronary artery plaque and risk of incident cardiovascular events. JAMA 2014, 311, 271–278. [Google Scholar] [CrossRef] [PubMed]
- Bellasi, A.; Ferramosca, E.; Ratti, C.; Block, G.; Raggi, P. The density of calcified plaques and the volume of calcium predict mortality in hemodialysis patients. Atherosclerosis 2016, 250, 166–171. [Google Scholar] [CrossRef] [PubMed]
- Kooman, J.P.; Kotanko, P.; Schols, A.M.; Shiels, P.G.; Stenvinkel, P. Chronic kidney disease and premature ageing. Nat. Rev. Nephrol. 2014, 10, 732–742. [Google Scholar] [CrossRef]
- Jamal, S.A.; Vandermeer, B.; Raggi, P.; Mendelssohn, D.C.; Chatterley, T.; Dorgan, M.; Lok, C.E.; Fitchett, D.; Tsuyuki, R.T. Effect of calcium-based versus non-calcium-based phosphate binders on mortality in patients with chronic kidney disease: An updated systematic review and meta-analysis. Lancet 2013, 382, 1268–1277. [Google Scholar] [CrossRef]
- Evenepoel, P.; Wolf, M. A balanced view of calcium and phosphate homeostasis in chronic kidney disease. Kidney Int. 2013, 83, 789–791. [Google Scholar] [CrossRef] [Green Version]
- Evenepoel, P. Control of hyperphosphatemia beyond phosphate. Kidney Int. 2007, 71, 376–379. [Google Scholar] [CrossRef] [Green Version]
- Anderson, J.J.; Kruszka, B.; Delaney, J.A.; He, K.; Burke, G.L.; Alonso, A.; Bild, D.E.; Budoff, M.; Michos, E.D. Calcium Intake From Diet and Supplements and the Risk of Coronary Artery Calcification and its Progression Among Older Adults: 10-Year Follow-up of the Multi-Ethnic Study of Atherosclerosis (MESA). J. Am. Heart Assoc. 2016, 5. [Google Scholar] [CrossRef]
- Raggi, P.; Chertow, G.M.; Torres, P.U.; Csiky, B.; Naso, A.; Nossuli, K.; Moustafa, M.; Goodman, W.G.; Lopez, N.; Downey, G.; et al. The ADVANCE study: A randomized study to evaluate the effects of cinacalcet plus low-dose vitamin D on vascular calcification in patients on hemodialysis. Nephrol. Dial. Transpl. 2011, 26, 1327–1339. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Di Lullo, L.; Tripepi, G.; Ronco, C.; D’Arrigo, G.; Barbera, V.; Russo, D.; Di Iorio, B.R.; Uguccioni, M.; Paoletti, E.; Ravera, M.; et al. Cardiac valve calcification and use of anticoagulants: Preliminary observation of a potentially modifiable risk factor. Int. J. Cardiol. 2019, 278, 243–249. [Google Scholar] [CrossRef]
- Sakaguchi, Y.; Hamano, T.; Obi, Y.; Monden, C.; Oka, T.; Yamaguchi, S.; Matsui, I.; Hashimoto, N.; Matsumoto, A.; Shimada, K.; et al. A Randomized Trial of Magnesium Oxide and Oral Carbon Adsorbent for Coronary Artery Calcification in Predialysis CKD. J. Am. Soc. Nephrol. 2019, 30, 1073–1085. [Google Scholar] [CrossRef]
- Raggi, P.; Bellasi, A.; Sinha, S.; Bover, J.; Rodriguez, M.; Ketteler, M.; Bushinsky, D.A.; Garg, R.; Perello, J.; Gold, A.; et al. Effects of SNF472, a Novel Inhibitor of Hydroxyapatite Crystallization in Patients Receiving Hemodialysis—Subgroup Analyses of the CALIPSO Trial. Kidney Int. Rep. 2020, 5, 2178–2182. [Google Scholar] [CrossRef] [PubMed]
- Raggi, P.; Bellasi, A.; Bushinsky, D.; Bover, J.; Rodriguez, M.; Ketteler, M.; Sinha, S.; Salcedo, C.; Gillotti, K.; Padgett, C.; et al. Slowing Progression of Cardiovascular Calcification With SNF472 in Patients on Hemodialysis: Results of a Randomized Phase 2b Study. Circulation 2020, 141, 728–739. [Google Scholar] [CrossRef] [PubMed]
- D’Marco, L.; Bellasi, A.; Mazzaferro, S.; Raggi, P. Vascular calcification, bone and mineral metabolism after kidney transplantation. World J. Transpl. 2015, 5, 222–230. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variable | Total (n = 414) | Alive (n = 308) | Expired (n = 106) | |
|---|---|---|---|---|
| Mean (SD)(n) | Mean (SD)(n) | Mean (SD)(n) | p-Value | |
| Age (years) | 65.3 (14.8)(414) | 63.1 (14.8)(308) | 71.5 (12.9)(106) | <0.0001 |
| Male (%) | 48.8% (202) | 46.4% (143) | 55.7% (59) | 0.127 |
| Body Weight (kg) | 70.7(13.7)(414) | 72.8 (13.3)(308) | 64.7 (13.0)(106) | <0.0001 |
| ASCVD (%) | 32.6% (135) | 27.3% (84) | 48.1% (51) | <0.0001 |
| Diabetes (%) | 28.3% (117) | 18.8% (58) | 55.7% (59) | <0.0001 |
| Systolic Blood Pressure (mmHg) | 137 (18)(414) | 136 (17)(308) | 140 (19)(106) | 0.056 |
| Diastolic Blood Pressure (mmHg) | 76 (9)(414) | 76 (8)(308) | 76 (10)(106) | 0.741 |
| LVMI (g/cm2) | 149 (45)(414) | 146 (48)(308) | 158 (34)(106) | 0.007 |
| QTc (ms) | 407 (32)(414) | 406 (34)(308) | 410 (26)(106) | 0.314 |
| QTd (ms) | 26 (11)(414) | 27 (11)(308) | 25 (11)(106) | 0.193 |
| CAC Agatston score (unit) | 273 (728)(414) | 181 (633)(308) | 542 (903)(106) | 0.0002 |
| CAC strata | <0.0001 | |||
| CAC = 0 | 31.8 (132) | 34.7 (107) | 23.5 (25) | |
| CAC 1–99 | 44.4 (184) | 49.0 (151) | 31.1 (33) | |
| CAC 100–399 | 8.4 (35) | 7.7 (24) | 10.3 (11) | |
| CAC 400+ | 15.3 (63) | 8.4 (26) | 34.9 (37) | |
| CAC Agatston score progression | 33.1% (137) | 26.9% (83) | 50.9% (54) | <0.0001 |
| Pulse Wave Velocity (m/s) | 8.7 (2.4)(414) | 8.5 (1.8)(308) | 9.4 (3.7)(106) | 0.012 |
| Hemoglobin (g/dL) | 11.0 (1.4)(414) | 11.1(1.4) (308) | 10.9(1.5)(106) | 0.269 |
| Albumin (g/dL) | 3.8 (0.4)(414) | 3.9 (0.4)(308) | 3.6 (0.4)(106) | <0.0001 |
| Total Cholesterol (mg/dL) | 161(48)(414) | 158(44)(308) | 165(53)(106) | 0.192 |
| LDL Cholesterol (mg/dL) | 100(29)(414) | 98(28)(308) | 102(31)(106) | 0.168 |
| Triglycerides (mg/dL) | 175(111)(414) | 179(126)(308) | 170(89)(106) | 0.402 |
| Serum Creatinine (g/dL) | 7.9 (2.6)(414) | 8.0 (2.5)(308) | 7.4 (2.5)(106) | 0.019 |
| Hemoglobin (g/dL) | 11 (1.4)(414) | 10.9 (1.4)(308) | 11.2 (1.4)(106) | 0.045 |
| Sodium (mE/L) | 139 (3.2)(413) | 138 (3.4)(307) | 139 (2.7)(106) | 0.0005 |
| Potassium (mEq/L) | 5.2 (0.8)(414) | 5.2 (0.8)(308) | 5.1 (0.7)(106) | 0.117 |
| Calcium (mg/dL) | 8.9 (0.7)(413) | 8.9 (0.8)(307) | 8.6 (0.6)(106) | <0.0001 |
| Phosphate (mg/dL) | 5.2 (1.5)(413) | 5.3 (1.6)(307) | 4.9 (1.4)(106) | 0.015 |
| Parathyroid Hormone (pg/mL) | 271 (207)(414) | 277 (204)(308) | 255 (215)(106) | 0.363 |
| C-reactive protein (mg/L) | 7.7 (11.2)(414) | 8.4 (12.4)(308) | 5.5 (6.5)(106) | 0.003 |
| Use of ACE Inhibitors (%) | 79.5% (329) | 79.9% (246) | 78.3% (83) | 0.837 |
| Use of ARBs (%) | 88.2% (365) | 86% (265) | 94.3% (100) | 0.035 |
| Use of Beta Blockers (%) | 50.2% (208) | 54.2% (167) | 38.7% (41) | 0.008 |
| Use of Calcium Channel Blockers (%) | 32.4% (134) | 29.2% (90) | 41.5% (44) | 0.027 |
| Use of Cinacalcet (%) | 52.4% (217) | 52.9% (163) | 50.9% (54) | 0.811 |
| Use of Vitamin D (%) | 43.2% (179) | 43.2% (133) | 43.4% (46) | 1 |
| Use of Sevelamer (%) | 50.7% (210) | 42.2% (130) | 75.5% (80) | <0.0001 |
| Use of Calcium-Based Binders (%) | 49.3% (204) | 57.8% (178) | 24.5% (26) | <0.0001 |
| 95% Confidence Interval | ||||
|---|---|---|---|---|
| Odds Ratio | Lower Boundary | Upper Boundary | ||
| Baseline coronary artery calcification [log(CACstart + 1)] | 0.913 | 0.817 | 1.021 | 0.110 |
| Use of calcium-free phosphate binder (yes vs. no) | 0.128 | 0.059 | 0.279 | <0.001 |
| Pulse wave velocity at baseline (m/s) | 0.988 | 0.9 | 1.085 | 0.796 |
| Age (years) | 1.022 | 1.006 | 1.039 | 0.008 |
| History of diabetes (yes vs. no) | 0.691 | 0.411 | 1.162 | 0.163 |
| History of ASCVD (yes vs. no) | 1.096 | 0.679 | 1.767 | 0.708 |
| Interaction term (baseline CAC × calcium-free phosphate binder) | 1.381 | 1.125 | 1.70E + 00 | 0.002 |
| 95% Confidence Interval | ||||
| Odds Ratio | Lower Boundary | Upper Boundary | ||
| Baseline coronary artery calcification [log(CACstart + 1)] | 0.921 | 0.827 | 1.025 | 0.131 |
| Use of calcium-free phosphate binder (yes vs. no) | 0.132 | 0.063 | 0.279 | <0.001 |
| Age (years) | 1.019 | 1.004 | 1.036 | 0.015 |
| Interaction term (baseline CAC × calcium-free phosphate binder) | 1.36 | 1.115 | 1.659 | <0.001 |
| Predictors of All-Cause Mortality (Cox Model)—All Subjects n = 414 (106 Fatalities) | ||||
|---|---|---|---|---|
| 95% Confidence Interval | ||||
| Model | HR | Lower Boundary | Upper Boundary | Pr(>|z|) |
| Unadjusted | ||||
| Baseline CAC score (log CAC +1) per log increase | 1.32252 | 1.1855 | 1.4754 | <0.001 |
| CAC progression (yes vs. no) | 4.2082 | 2.1258 | 8.3307 | <0.001 |
| Interaction term | 0.7978 | 0.6913 | 0.9207 | 0.002 |
| Model 1: adjusted for age | ||||
| Baseline CAC score (log CAC +1) per log increase | 1.3024 | 1.1671 | 1.4533 | 2.34 × 10−6 |
| CAC progression (yes vs. no) | 4.1393 | 2.093 | 8.1863 | 4.45 × 10−5 |
| Interaction term | 0.7939 | 0.6881 | 0.9159 | 0.00156 |
| Model 2: adjusted for Model 1 + diabetes + ASCVD + systolic blood pressure | ||||
| Baseline CAC score (log CAC +1) per log increase | 1.2876 | 1.1565 | 1.4335 | 3.96 × 10−6 |
| CAC progression (yes vs. no) | 4.2444 | 2.1608 | 8.3371 | 2.71 × 10−5 |
| Interaction term | 0.8268 | 0.7172 | 0.9531 | 0.00876 |
| Model 3: adjusted for Model 2 + PWV + LVMI | ||||
| Baseline CAC score (log CAC +1) per log increase | 1.2987 | 1.171 | 1.4402 | 7.34 × 10−7 |
| CAC progression (yes vs. no) | 5.165 | 2.6128 | 10.2101 | 2.33 × 10−6 |
| Interaction term | 0.8019 | 0.6965 | 0.9232 | 0.00213 |
| Model 4 adjusted for Model 3 + use of calcium-free phosphate binder | ||||
| Baseline CAC score (log CAC +1) per log increase | 1.1287 | 1.0114 | 1.2596 | 0.03055 |
| CAC progression (yes vs. no) | 1.9591 | 0.9214 | 4.1652 | 0.08058 |
| Interaction term | 0.96 | 0.8255 | 1.1164 | 0.59595 |
| Entire Study Cohort | Confidence Interval | ||||
|---|---|---|---|---|---|
| Survival (%) | St Err | Lower 95% | Upper 95% | ||
| CAC = 0 | 0.86 | 0.03 | 0.85 | 0.92 | |
| CAC 1–100 | 0.84 | 0.02 | 0.8 | 0.913 | |
| CAC 101–400 | 0.87 | 0.05 | 0.77 | 0.99 | |
| CAC 400+ | 0.56 | 0.06 | 0.44 | 0.712 | |
| No Evidence of CAC Progression | |||||
| CAC = 0 | 0.94 | 0.02 | 0.9 | 0.99 | |
| CAC 1–100 | 0.89 | 0.02 | 0.83 | 0.95 | |
| CAC 101–400 | 0.92 | 0.07 | 0.78 | 1 | |
| CAC 400+ | 0.44 | 0.09 | 0.29 | 0.67 | |
| Evidence of CAC Progression | |||||
| CAC = 0 | 0.72 | 0.06 | 0.6 | 0.86 | |
| CAC 1–100 | 0.71 | 0.07 | 0.57 | 0.88 | |
| CAC 101–400 | 0.83 | 0.08 | 0.67 | 1 | |
| CAC 400+ | 0.69 | 0.09 | 0.53 | 0.89 | |
| Predictors of All-Cause Mortality (Cox Model)—Non-Progressor Subjects n = 277 (52 Fatalities) | ||||
|---|---|---|---|---|
| Model | HR | 95% Confidence Interval | Pr(>|z|) | |
| Lower Boundary | Upper Boundary | |||
| Unadjusted | ||||
| Baseline CAC score (log CAC +1) per log increase | 1.313 | 1.178 | 1.465 | <0.001 |
| Model 1: adjusted for age | ||||
| Baseline CAC score (log CAC +1) per log increase | 1.29 | 1.156 | 1.44 | <0.001 |
| Model 2: adjusted for Model 1 + diabetes + ASCVD + systolic blood pressure | ||||
| Baseline CAC score (log CAC +1) per log increase | 1.3343 | 1.1881 | 1.499 | <0.001 |
| Model 3: adjusted for Model 2 + PWV + LVMI | ||||
| Baseline CAC score (log CAC +1) per log increase | 1.3577 | 1.2165 | 1.515 | <0.001 |
| Model 4 adjusted for Model 3 + use of calcium-free phosphate binder | ||||
| Baseline CAC score (log CAC +1) per log increase | 1.1512 | 1.0157 | 1.3047 | 0.027 |
| Predictors of All-Cause Mortality (Cox Model)—Non-Progressor Subjects n = 137 (54 Fatalities) | ||||
|---|---|---|---|---|
| Model | HR | 95% Confidence Interval | Pr( > |z|) | |
| Lower Boundary | Upper Boundary | |||
| Unadjusted | ||||
| Baseline CAC score (log CAC +1) per log increase | 1.058 | 0.9638 | 1.16 | 0.237 |
| Model 1: adjusted for age | ||||
| Baseline CAC score (log CAC +1) per log increase | 1.036 | 0.9438 | 1.137 | 0.456 |
| Model 2: adjusted for Model 1 + diabetes + ASCVD + systolic blood pressure | ||||
| Baseline CAC score (log CAC +1) per log increase | 1.073 | 0.9738 | 1.182 | 0.154 |
| Model 3: adjusted for Model 2 + PWV + LVMI | ||||
| Baseline CAC score (log CAC +1) per log increase | 1.069 | 0.9663 | 1.182 | 0.197 |
| Model 4 adjusted for Model 3 + use of calcium-free phosphate binder | ||||
| Baseline CAC score (log CAC +1) per log increase | 1.116 | 0.9993 | 1.246 | 0.051 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bellasi, A.; Di Lullo, L.; Russo, D.; Ciarcia, R.; Magnocavallo, M.; Lavalle, C.; Ratti, C.; Cozzolino, M.; Di Iorio, B.R. Vascular Calcification Progression Modulates the Risk Associated with Vascular Calcification Burden in Incident to Dialysis Patients. Cells 2021, 10, 1091. https://doi.org/10.3390/cells10051091
Bellasi A, Di Lullo L, Russo D, Ciarcia R, Magnocavallo M, Lavalle C, Ratti C, Cozzolino M, Di Iorio BR. Vascular Calcification Progression Modulates the Risk Associated with Vascular Calcification Burden in Incident to Dialysis Patients. Cells. 2021; 10(5):1091. https://doi.org/10.3390/cells10051091
Chicago/Turabian StyleBellasi, Antonio, Luca Di Lullo, Domenico Russo, Roberto Ciarcia, Michele Magnocavallo, Carlo Lavalle, Carlo Ratti, Mario Cozzolino, and Biagio Raffaele Di Iorio. 2021. "Vascular Calcification Progression Modulates the Risk Associated with Vascular Calcification Burden in Incident to Dialysis Patients" Cells 10, no. 5: 1091. https://doi.org/10.3390/cells10051091
APA StyleBellasi, A., Di Lullo, L., Russo, D., Ciarcia, R., Magnocavallo, M., Lavalle, C., Ratti, C., Cozzolino, M., & Di Iorio, B. R. (2021). Vascular Calcification Progression Modulates the Risk Associated with Vascular Calcification Burden in Incident to Dialysis Patients. Cells, 10(5), 1091. https://doi.org/10.3390/cells10051091