
The rs508487, rs236911, and rs236918 Genetic Variants of the Proprotein Convertase Subtilisin–Kexin Type 7 (PCSK7) Gene Are Associated with Acute Coronary Syndrome and with Plasma Concentrations of HDL-Cholesterol and Triglycerides

 , , ,
, , ,  , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Characteristics of the Study Population
2.2. Laboratory Analyses
2.3. Genetic Analysis
2.4. Inheritance Model Analysis
2.5. Analysis of the Haplotypes
2.6. Statistical Analysis
3. Results
3.1. Characteristics of the ACS Patients and Controls
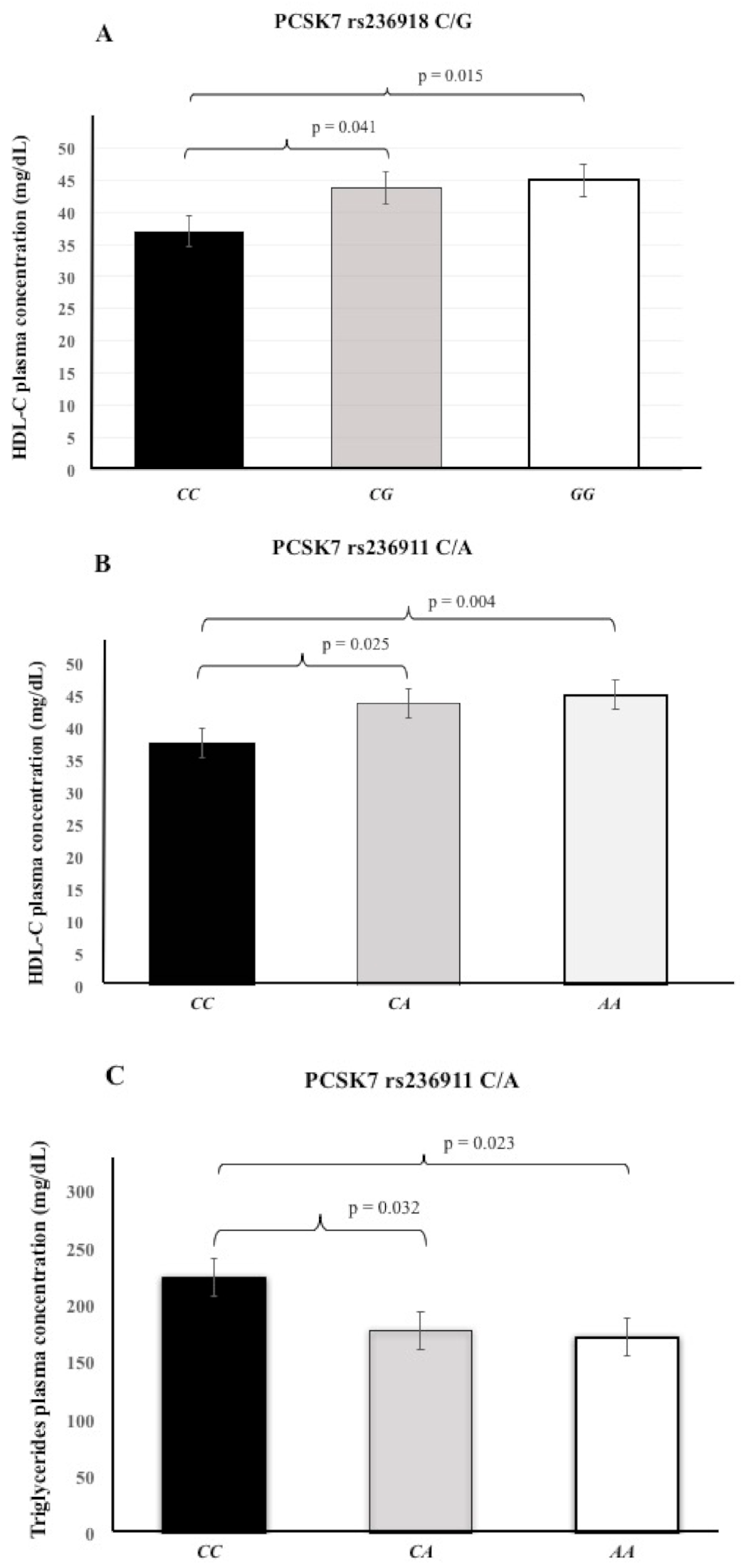
3.2. Association of PCSK7 SNPs with Plasma Lipids Levels
3.3. Allele and Genotype Frequencies
3.4. Association of PCSK7 SNPs with ACS
3.5. Linkage Disequilibrium Analysis
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| LDLR | Low-density lipoprotein receptor |
| HDL-C | High-density lipoprotein-cholesterol |
| LDL-C | Low-density lipoprotein-cholesterol |
| T2DM | Type 2 diabetes mellitus |
| SNP | Single nucleotide polymorphism |
| ACS | Acute coronary syndrome |
| PCSK7 | Proprotein convertase subtilisin–kexin type 7 |
References
- Virmani, R.; Kolodgie, F.D.; Burke, A.P.; Finn, A.V.; Gold, H.K.; Tulenko, T.N.; Wrenn, S.P.; Narula, J. Atherosclerotic Plaque Progression and Vulnerability to Rupture: Angiogenesis as a Source of Intraplaque Hemorrhage. Thromb. Vasc. Biol. 2005, 25, 2054–2061. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Achar, S.A.; Kundu, S.; Norcross, W.A. Diagnosis of acute coronary syndrome. Am. Fam. Physician. 2004, 72, 119–126. [Google Scholar]
- Cabezas, M.C.; Burggraaf, B.; Klop, B. Dyslipidemias in clinical practice. Clin. Chim. Acta 2018, 487, 117–125. [Google Scholar] [CrossRef]
- Hoogeveen, R.C.; Gaubatz, J.W.; Sun, W.; Dodge, R.C.; Crosby, J.R.; Jiang, J. Small dense low-density lipoprotein-cholesterol concentrations predict risk for coronary heart disease: The atherosclerosis risk in communities (ARIC) study. Arterioscler Thromb. Vasc. Biol. 2014, 34, 1069–1077. [Google Scholar] [CrossRef] [Green Version]
- Seidah, N.G.; Sadr, M.S.; Chrétien, M.; Mbikay, M. The Multifaceted Proprotein Convertases: Their Unique, Redundant, Complementary, and Opposite Functions*. J. Biol. Chem. 2013, 288, 21473–21481. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ashraf, Y.; Duval, S.; Sachan, V.; Essalmani, R.; Susan-Resiga, D.; Roubtsova, A.; Hamelin, J.; Gerhardy, S.; Kirchhofer, D.; Tagliabracci, V.S.; et al. Proprotein convertase 7 (PCSK7) reduces apoA-V levels. FEBS J. 2020, 287, 3565–3578. [Google Scholar] [CrossRef]
- Forte, T.M.; Ryan, R.O. Apolipoprotein A5: Extracellular and Intracellular Roles in Triglyceride Metabolism. Curr. Drug Targets 2015, 16, 1274–1280. [Google Scholar] [CrossRef]
- Dai, W.; Zhang, Z.; Yao, C.; Zhao, S. Emerging evidences for the opposite role of apolipoprotein C3 and apolipoprotein A5 in lipid metabolism and coronary artery disease. Lipids Health Dis. 2019, 18, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Guardiola, M.; Cofán, M.; Orós, I.D.C.; Cenarro, A.; Plana, N.; Talmud, P.J.; Masana, L.; Ros, E.; Civeira, F.; Ribalta, J. APOA5 variants predispose hyperlipidemic patients to atherogenic dyslipidemia and subclinical atherosclerosis. Atherosclerosis 2015, 240, 98–104. [Google Scholar] [CrossRef] [PubMed]
- Dongiovanni, P.; Meroni, M.; Baselli, G.; Mancina, R.M.; Ruscica, M.; Longo, M.; Rametta, R.; Cespiati, A.; Pelusi, S.; Ferri, N.; et al. PCSK7 gene variation bridges atherogenic dyslipidemia with hepatic inflammation in NAFLD patients. J. Lipid Res. 2019, 60, 1144–1153. [Google Scholar] [CrossRef]
- Gombojav, B.; Lee, S.J.; Kho, M.; Song, Y.-M.; Lee, K.; Sung, J. Multiple susceptibility loci at chromosome 11q23.3 are associated with plasma triglyceride in east Asia). J. Lipid Res. 2017, 57, 318–324. [Google Scholar]
- Peloso, G.M.; Auer, P.L.; Bis, J.C.; Voorman, A.; Morrison, A.; Stitziel, N.; Brody, J.A.; Khetarpal, S.A.; Crosby, J.R.; Fornage, M.; et al. Association of Low-Frequency and Rare Coding-Sequence Variants with Blood Lipids and Coronary Heart Disease in 56,000 Whites and Blacks. Am. J. Hum. Genet. 2014, 94, 223–232. [Google Scholar] [CrossRef] [Green Version]
- Kurano, M.; Tsukamoto, K.; Kamitsuji, S.; Kamatani, N.; Hara, M.; Ishikawa, T.; Kim, B.-J.; Moon, S.; Kim, Y.J.; Teramoto, T. Genome-wide association study of serum lipids confirms previously reported associations as well as new associations of common SNPs within PCSK7 gene with triglyceride. J. Hum. Genet. 2016, 61, 427–433. [Google Scholar] [CrossRef] [PubMed]
- Cannon, C.P.; Battler, A.; Brindis, R.G.; Cox, J.L.; Ellis, S.G.; Every, N.R.; Flaherty, J.T.; A Harrington, R.; Krumholz, H.M.; Simoons, M.L.; et al. American College of Cardiology key data elements and definitions for measuring the clinical management and outcomes of patients with acute coronary syndromes: A report of the American College of Cardiology Task Force on Clinical Data Standards (Acute Coronary Syndromes Writing Committee) Endorsed by the American Association of Cardiovascular and Pulmonary Rehabilitation, American College of Emergency Physicians, American Heart Association, Cardiac Society of Australia & New Zealand, National Heart Foundation of Australia, Society for Cardiac Angiography and Interventions, and the Taiwan Society of Cardiology. J. Am. Coll. Cardiol. 2001, 38, 2114–2130. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hamm, C.W.; Bassand, J.-P.; Agewall, S.; Bax, J.; Boersma, E.; Bueno, H.; Caso, P.; Dudek, D.; Gielen, S.; Huber, K.; et al. ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation: The Task Force for the management of acute coronary syndromes (ACS) in patients presenting without persistent ST-segment elevation of the European Society of Cardiology (ESC). Eur. Hear. J. 2011, 32, 2999–3054. [Google Scholar] [CrossRef] [Green Version]
- Posadas-Sanchez, R.; Perez-Hernandez, N.; Angeles-Martinez, J.; Lopez-Bautista, F.; Villarreal-Molina, T.; Rodríguez-Perez, J.M. Interleukin 35 Polymorphisms Are Associated with Decreased Risk of Premature Coronary Artery Disease, Metabolic Parameters, and IL-35 Levels: The Genetics of Atherosclerotic Disease (GEA) Study. Mediat. Inflamm. 2017, 6012795. [Google Scholar] [CrossRef]
- Delong, D.M.; Delong, E.R.; Wood, P.D.; Lippel, K.; Rifkind, B.M. A Comparison of Methods for the Estimation of Plasma Low- and Very Low-Density Lipoprotein Cholesterol. JAMA 1986, 256, 2372–2377. [Google Scholar] [CrossRef]
- Lahiri, D.K.; Nurnberger, J.I. A rapid non-enzymatic method for the preparation HMW DNA from blood for RFLP studies. Nucleic Acids Res. 1991, 19, 5444. [Google Scholar] [CrossRef]
- Perez-Calahorra, S.; Laclaustra, M.; Marco-Benedi, V.; Pinto, X.; Sanchez-Hernandez, R.M.; Plana, N.; Ortega, E.; Fuentes, F.; Civeira, F. Comparative efficacy between atorvastatin and rosuvastatin in the prevention of cardiovascular disease recurrence. Lipids Health Dis. 2019, 18, 1–6. [Google Scholar] [CrossRef] [Green Version]
- Kim, K.-J.; Yoon, J.; Won, K.H.; Lim, S.-W.; Chae, I.-H.; Lee, S.Y.; Kim, H.-S.; Kim, S.-W. Assessment of the Efficacy of Lowering LDL Cholesterol with Rosuvastatin 10 mg in Four Korean Statin Benefit Groups as per ACC/AHA Guidelines (NewStaR4G). J. Clin. Med. 2020, 9, 916. [Google Scholar] [CrossRef] [Green Version]
- Ettehad, D.; A Emdin, C.; Kiran, A.; Anderson, S.G.; Callender, T.; Emberson, J.; Chalmers, J.; Rodgers, A.; Rahimi, K. Blood pressure lowering for prevention of cardiovascular disease and death: A systematic review and meta-analysis. Lancet 2016, 387, 957–967. [Google Scholar] [CrossRef] [Green Version]
- Stickel, F.; Buch, S.; Zoller, H.; Hultcrantz, R.; Gallati, S.; Österreicher, C.; Finkenstedt, A.; Stadlmayr, A.; Aigner, E.; Sahinbegovic, E.; et al. Evaluation of genome-wide loci of iron metabolism in hereditary hemochromatosis identifies PCSK7 as a host risk factor of liver cirrhosis. Hum. Mol. Genet. 2014, 23, 3883–3890. [Google Scholar] [CrossRef]
- Pelucchi, S.; Galimberti, S.; Greni, F.; Rametta, R.; Mariani, R.; Pelloni, I. Proprotein convertase/rs236918 associated with liver fibrosis in Italian patients with HFE-related hemochromatosis. J. Gastroenterol. Hepatol. 2016, 31, 1342–1348. [Google Scholar] [CrossRef]
- Pennacchio, L.A.; Olivier, M.; Hubacek, J.A.; Cohen, J.C.; Cox, D.R.; Fruchart, J.-C.; Krauss, R.M.; Rubin, E.M. An Apolipoprotein Influencing Triglycerides in Humans and Mice Revealed by Comparative Sequencing. Science 2001, 294, 169–173. [Google Scholar] [CrossRef] [Green Version]
- Zhu, Y.; He, B.; Xiao, Y.; Chen, Y. Iron metabolism and its association with dyslipidemia risk in children and adolescents: A cross-sectional study. Lipids Health Dis. 2019, 18, 1–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oexle, K.; Ried, J.S.; Hicks, A.A.; Tanaka, T.; Hayward, C.; Bruegel, M. Novel association to the proprotein convertase PCSK7 gene locus revealed by analyzing soluble transferrin receptor (sTfR) levels. Hum. Mol. Genet. 2011, 20, 1042–1047. [Google Scholar] [CrossRef] [PubMed]
- Guillemot, J.; Canuel, M.; Essalmani, R.; Prat, A.; Seidah, N.G. Implication of the proprotein convertases in iron homeostasis: Proprotein convertase 7 sheds human transferrin receptor 1 and furin activates hepcidin. Hepatology 2013, 57, 2514–2524. [Google Scholar] [CrossRef]
- Sullivan, J.L. Iron in arterial plaque: A modifiable risk factor for atherosclerosis. Biochim. et Biophys. Acta Gen. Subj. 2009, 1790, 718–723. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Characteristics | ACS Patients (n = 603) | Healthy Controls (n = 622) | p-Value | |
|---|---|---|---|---|
| Median (percentile 25–75) | Median (percentile 25–75) | |||
| Age (years) | 58 (51–65) | 54 (49–59) | 0.001 | |
| Sex n (%) | Male | 491 (82) | 430 (69) | <0.001 |
| Female | 112 (18) | 192 (31) | ||
| BMI (kg/m2) | 27 (25–29) | 28 (26–31) | 0.593 | |
| Blood pressure (mmHg) | Systolic | 130 (115–144) | 115 (106–126) | <0.001 |
| Diastolic | 80 (70–90) | 72 (67–78) | <0.001 | |
| Glucose (mg/dL) | 158 (102–188) | 97 (84–99) | <0.001 | |
| Total cholesterol (mg/dL) | 163 (127–200) | 188 (164–210) | <0.001 | |
| HDL-C (mg/dL) | 37 (32–45) | 42 (35–53) | <0.001 | |
| LDL-C (mg/dL) | 103 (75–133) | 115 (94–134) | <0.001 | |
| Triglycerides (mg/dL) | 149 (109–201) | 154 (113–209) | 0.144 | |
| Ratio LDL/HDL | 2.72 (1.99–3.45) | 2.73 (2.08–3.42) | 0.891 | |
| n (%) | n (%) | |||
| Hypertension | Yes | 345 (57) | 182 (29) | <0.001 |
| Type II diabetes mellitus | Yes | 209 (35) | 58 (9) | <0.001 |
| Dyslipidemia | Yes | 515 (85) | 451 (72) | <0.001 |
| Smoking | Yes | 214 (35) | 135 (22) | <0.001 |
| Polymorphic Site | ACS n = 603 (n [%]) | Controls n = 622 (n [%]) | * p | |
|---|---|---|---|---|
| PCSK7 rs236918 C/G | ||||
| Allele | ||||
| G | 926 (77) | 1009 (81) | 0.010 | |
| C | 280 (23) | 235 (19) | ||
| Genotype | ||||
| GG | 354 (58.7) | 403 (64.8) | ||
| GC | 218 (36.1) | 203 (32.6) | 0.008 | |
| CC | 31 (5.1) | 16 (2.6) | ||
| PCSK7 rs236911 C/A | ||||
| Allele | ||||
| A | 886 (73) | 967 (78) | 0.015 | |
| C | 320 (27) | 277 (22) | ||
| Genotype | ||||
| AA | 323 (53.6) | 370 (59.5) | ||
| AC | 240 (39.8) | 227 (36.5) | 0.014 | |
| CC | 40 (6.6) | 25 (4) | ||
| PCSK7 UTR’3 rs508487 T/C | ||||
| Allele | ||||
| C | 1127 (93) | 1191 (96) | 0.015 | |
| T | 79 (7) | 53 (4) | ||
| Genotype | ||||
| CC | 524 (86.9) | 569 (91.5) | ||
| CT | 79 (13.1) | 53 (8.5) | 0.012 | |
| TT | 0 | 0 |
| n (Genotype Frequency) | MAF | Model | OR (95%CI) | pC | |||
|---|---|---|---|---|---|---|---|
| PCSK7 | rs236918 C/G | ||||||
| Control | GG | GC | CC | C | |||
| (n = 622) | 403 (0.648) | 203 (0.326) | 16 (0.026) | 0.188 | Co-dominant | 2.19 (1.05–4.58) | 0.093 |
| Dominant | 1.20 (0.91–1.58) | 0.209 | |||||
| ACS | 354 (0.587) | 218 (0.361) | 31 (0.051) | 0.232 | Recessive | 2.11 (1.02–4.37) | 0.039 |
| (n = 603) | Over-dominant | 1.07 (0.81–1.42) | 0.639 | ||||
| Additive | 1.24 (0.98–1.58) | 0.076 | |||||
| PCSK7 | rs236911 C/A | ||||||
| Control | AA | AC | CC | C | |||
| (n = 622) | 370 (0.595) | 227 (0.365) | 25 (0.040) | 0.222 | Co-dominant | 2.08 (1.09–3.95) | 0.065 |
| Dominant | 1.25 (0.95–1.64) | 0.121 | |||||
| ACS | 323 (0.536) | 240 (0.398) | 40 (0.066) | 0.265 | Recessive | 1.95 (1.03–3.67) | 0.037 |
| (n = 603) | Over-dominant | 1.10 (0.83–1.46) | 0.509 | ||||
| Additive | 1.28 (1.01–1.61) | 0.037 | |||||
| PCSK7 UTR’3 | rs508487 T/C | ||||||
| Control | CC | CT | TT | T | |||
| (n = 622) | 569 (0.915) | 53 (0.085) | 0 (0.0) | 0.042 | |||
| Co-dominant | 1.78 (1.15–2.76) | 0.010 | |||||
| ACS | 524 (0.869) | 79 (0.131) | 0 (0.0) | 0.065 | |||
| (n = 603) |
| rs508487 | rs236911 | rs236918 | ACS (n = 603) | Controls (n = 622) | OR | 95%CI | pC |
|---|---|---|---|---|---|---|---|
| Haplotype | Hf | Hf | |||||
| C | A | G | 0.730 | 0.765 | 0.83 | 0.69–0.99 | 0.021 |
| C | C | C | 0.167 | 0.142 | 1.21 | 1.00–1.51 | 0.045 |
| T | C | C | 0.062 | 0.036 | 1.80 | 1.23–2.64 | 0.001 |
| C | C | G | 0.035 | 0.040 | 0.88 | 0.57–1.33 | 0.312 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vargas-Alarcón, G.; Pérez-Méndez, O.; González-Pacheco, H.; Ramírez-Bello, J.; Posadas-Sánchez, R.; Escobedo, G.; Fragoso, J.M. The rs508487, rs236911, and rs236918 Genetic Variants of the Proprotein Convertase Subtilisin–Kexin Type 7 (PCSK7) Gene Are Associated with Acute Coronary Syndrome and with Plasma Concentrations of HDL-Cholesterol and Triglycerides. Cells 2021, 10, 1444. https://doi.org/10.3390/cells10061444
Vargas-Alarcón G, Pérez-Méndez O, González-Pacheco H, Ramírez-Bello J, Posadas-Sánchez R, Escobedo G, Fragoso JM. The rs508487, rs236911, and rs236918 Genetic Variants of the Proprotein Convertase Subtilisin–Kexin Type 7 (PCSK7) Gene Are Associated with Acute Coronary Syndrome and with Plasma Concentrations of HDL-Cholesterol and Triglycerides. Cells. 2021; 10(6):1444. https://doi.org/10.3390/cells10061444
Chicago/Turabian StyleVargas-Alarcón, Gilberto, Oscar Pérez-Méndez, Héctor González-Pacheco, Julián Ramírez-Bello, Rosalinda Posadas-Sánchez, Galileo Escobedo, and José Manuel Fragoso. 2021. "The rs508487, rs236911, and rs236918 Genetic Variants of the Proprotein Convertase Subtilisin–Kexin Type 7 (PCSK7) Gene Are Associated with Acute Coronary Syndrome and with Plasma Concentrations of HDL-Cholesterol and Triglycerides" Cells 10, no. 6: 1444. https://doi.org/10.3390/cells10061444
APA StyleVargas-Alarcón, G., Pérez-Méndez, O., González-Pacheco, H., Ramírez-Bello, J., Posadas-Sánchez, R., Escobedo, G., & Fragoso, J. M. (2021). The rs508487, rs236911, and rs236918 Genetic Variants of the Proprotein Convertase Subtilisin–Kexin Type 7 (PCSK7) Gene Are Associated with Acute Coronary Syndrome and with Plasma Concentrations of HDL-Cholesterol and Triglycerides. Cells, 10(6), 1444. https://doi.org/10.3390/cells10061444