
Cryopreservation of Human Adipose Tissues and Adipose-Derived Stem Cells with DMSO and/or Trehalose: A Systematic Review

 , ,
, , 
Abstract
:1. Introduction
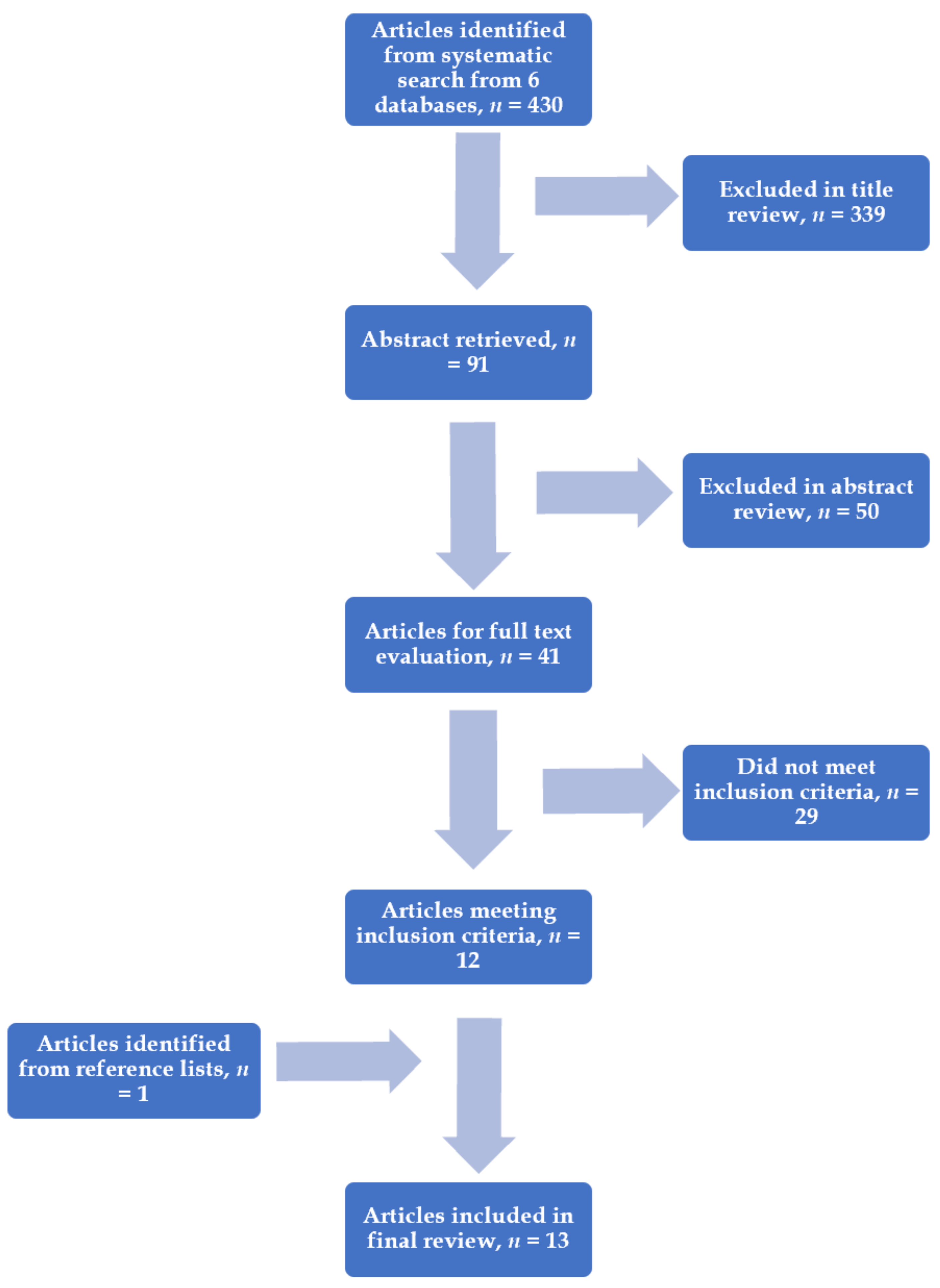
2. Materials and Methods
3. Results
3.1. Combined Use of Trehalose and DMSO for Cryopreservation
3.2. Comparing Trehalose vs. DMSO for Cryopreservation
3.3. Comparing Trehalose with Fresh Fat Control or Simple Cryopreservation
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Choudhery, M.S.; Badowski, M.; Muise, A.; Pierce, J.; Harris, D.T. Cryopreservation of whole adipose tissue for future use in regenerative medicine. J. Surg. Res. 2014, 187, 24–35. [Google Scholar] [CrossRef] [PubMed]
- Mizuno, H.; Tobita, M.; Uysal, A.C. Concise review: Adipose-derived stem cells as a novel tool for future regenerative medicine. Stem Cells 2012, 30, 804–810. [Google Scholar] [CrossRef] [PubMed]
- Dominici, M.; Le Blanc, K.; Mueller, I.; Slaper-Cortenbach, I.; Marini, F.; Krause, D.; Deans, R.; Keating, A.; Prockop, D.; Horwitz, E. Minimal criteria for defining multipotent mesenchymal stromal cells. The International Society for Cellular Therapy position statement. Cytotherapy 2006, 8, 315–317. [Google Scholar] [CrossRef]
- Thirumala, S.; Gimble, J.M.; Devireddy, R.V. Cryopreservation of stromal vascular fraction of adipose tissue in a serum-free freezing medium. J. Tissue Eng. Regen. Med. 2010, 4, 224–232. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huang, H.; Rey-Bedon, C.; Yarmush, M.L.; Usta, O.B. Deep-supercooling for extended preservation of adipose-derived stem cells. Cryobiology 2020, 92, 67–75. [Google Scholar] [CrossRef] [PubMed]
- Cui, X.; Pu, L.L. The search for a useful method for the optimal cryopreservation of adipose aspirates: Part I. In vitro study. Aesthet. Surg. J. 2009, 29, 248–252. [Google Scholar] [CrossRef] [Green Version]
- Dovgan, B.; Barlic, A.; Knezevic, M.; Miklavcic, D. Cryopreservation of Human Adipose-Derived Stem Cells in Combination with Trehalose and Reversible Electroporation. J. Membr. Biol. 2017, 250, 1–9. [Google Scholar] [CrossRef]
- Hoareau, L.; Bencharif, K.; Girard, A.C.; Gence, L.; Delarue, P.; Hulard, O.; Festy, F.; Roche, R. Effect of centrifugation and washing on adipose graft viability: A new method to improve graft efficiency. J. Plast. Reconstr. Aesthet. Surg. 2013, 66, 712–719. [Google Scholar] [CrossRef]
- Wang, X.; Hua, T.C.; Sun, D.W.; Liu, B.; Yang, G.; Cao, Y. Cryopreservation of tissue-engineered dermal replacement in Me2SO: Toxicity study and effects of concentration and cooling rates on cell viability. Cryobiology 2007, 55, 60–65. [Google Scholar] [CrossRef]
- Elbein, A.D.; Pan, Y.T.; Pastuszak, I.; Carroll, D. New insights on trehalose: A multifunctional molecule. Glycobiology 2003, 13, 17R–27R. [Google Scholar] [CrossRef] [PubMed]
- Colaco, C.; Kampinga, J.; Roser, B. Amorphous stability and trehalose. Science 1995, 268, 788. [Google Scholar] [CrossRef]
- Allison, S.D.; Chang, B.; Randolph, T.W.; Carpenter, J.F. Hydrogen bonding between sugar and protein is responsible for inhibition of dehydration-induced protein unfolding. Arch. Biochem. Biophys. 1999, 365, 289–298. [Google Scholar] [CrossRef] [PubMed]
- Albertorio, F.; Chapa, V.A.; Chen, X.; Diaz, A.J.; Cremer, P.S. The alpha,alpha-(1-->1) linkage of trehalose is key to anhydrobiotic preservation. J. Am. Chem. Soc. 2007, 129, 10567–10574. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Erdag, G.; Eroglu, A.; Morgan, J.; Toner, M. Cryopreservation of fetal skin is improved by extracellular trehalose. Cryobiology 2002, 44, 218–228. [Google Scholar] [CrossRef]
- Rao, W.; Huang, H.; Wang, H.; Zhao, S.; Dumbleton, J.; Zhao, G.; He, X. Nanoparticle-mediated intracellular delivery enables cryopreservation of human adipose-derived stem cells using trehalose as the sole cryoprotectant. ACS Appl. Mater. Interfaces 2015, 7, 5017–5028. [Google Scholar] [CrossRef]
- Pegg, D.E. The history and principles of cryopreservation. Semin. Reprod. Med. 2002, 20, 5–13. [Google Scholar] [CrossRef]
- Wusteman, M.C.; Simmonds, J.; Vaughan, D.; Pegg, D.E. Vitrification of rabbit tissues with propylene glycol and trehalose. Cryobiology 2008, 56, 62–71. [Google Scholar] [CrossRef]
- Pietramaggiori, G.; Kaipainen, A.; Ho, D.; Orser, C.; Pebley, W.; Rudolph, A.; Orgill, D.P. Trehalose lyophilized platelets for wound healing. Wound Repair Regen. 2007, 15, 213–220. [Google Scholar] [CrossRef]
- Rodrigues, J.P.; Paraguassu-Braga, F.H.; Carvalho, L.; Abdelhay, E.; Bouzas, L.F.; Porto, L.C. Evaluation of trehalose and sucrose as cryoprotectants for hematopoietic stem cells of umbilical cord blood. Cryobiology 2008, 56, 144–151. [Google Scholar] [CrossRef]
- Crowe, J.H. Trehalose as a “chemical chaperone”: Fact and fantasy. Adv. Exp. Med. Biol. 2007, 594, 143–158. [Google Scholar] [CrossRef]
- Pu, L.L.; Cui, X.; Fink, B.F.; Cibull, M.L.; Gao, D. Long-term preservation of adipose aspirates after conventional lipoplasty. Aesthet. Surg. J. 2004, 24, 536–541. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pu, L.L.; Cui, X.; Fink, B.F.; Gao, D.; Vasconez, H.C. Adipose aspirates as a source for human processed lipoaspirate cells after optimal cryopreservation. Plast. Reconstr. Surg. 2006, 117, 1845–1850. [Google Scholar] [CrossRef] [PubMed]
- Cui, X.D.; Gao, D.Y.; Fink, B.F.; Vasconez, H.C.; Pu, L.L. Cryopreservation of human adipose tissues. Cryobiology 2007, 55, 269–278. [Google Scholar] [CrossRef] [PubMed]
- Shu, Z.; Gao, D.; Pu, L.L. Update on cryopreservation of adipose tissue and adipose-derived stem cells. Clin. Plast. Surg. 2015, 42, 209–218. [Google Scholar] [CrossRef] [PubMed]
- Pu, L.L.; Cui, X.; Li, J.; Fink, B.F.; Cibull, M.L.; Gao, D. The fate of cryopreserved adipose aspirates after in vivo transplantation. Aesthet. Surg. J. 2006, 26, 653–661. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Rosa, A.; De Francesco, F.; Tirino, V.; Ferraro, G.A.; Desiderio, V.; Paino, F.; Pirozzi, G.; D’Andrea, F.; Papaccio, G. A new method for cryopreserving adipose-derived stem cells: An attractive and suitable large-scale and long-term cell banking technology. Tissue Eng. Part C Methods 2009, 15, 659–667. [Google Scholar] [CrossRef] [PubMed]
- Cui, X.; Pu, L.L. The search for a useful method for the optimal cryopreservation of adipose aspirates: Part II. In vivo study. Aesthet. Surg. J. 2010, 30, 451–456. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pu, L.L.; Coleman, S.R.; Cui, X.; Ferguson, R.E., Jr.; Vasconez, H.C. Cryopreservation of autologous fat grafts harvested with the Coleman technique. Ann. Plast. Surg. 2010, 64, 333–337. [Google Scholar] [CrossRef] [Green Version]
- Roato, I.; Alotto, D.; Belisario, D.C.; Casarin, S.; Fumagalli, M.; Cambieri, I.; Piana, R.; Stella, M.; Ferracini, R.; Castagnoli, C. Adipose Derived-Mesenchymal Stem Cells Viability and Differentiating Features for Orthopaedic Reparative Applications: Banking of Adipose Tissue. Stem Cells Int. 2016, 2016, 4968724. [Google Scholar] [CrossRef] [Green Version]
- Yong, K.W.; Pingguan-Murphy, B.; Xu, F.; Abas, W.A.; Choi, J.R.; Omar, S.Z.; Azmi, M.A.; Chua, K.H.; Wan Safwani, W.K. Phenotypic and functional characterization of long-term cryopreserved human adipose-derived stem cells. Sci. Rep. 2015, 5, 9596. [Google Scholar] [CrossRef] [Green Version]
- Pu, L.L.; Cui, X.; Fink, B.F.; Cibull, M.L.; Gao, D. Cryopreservation of adipose tissues: The role of trehalose. Aesthet. Surg. J. 2005, 25, 126–131. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Juni, P.; Holenstein, F.; Sterne, J.; Bartlett, C.; Egger, M. Direction and impact of language bias in meta-analyses of controlled trials: Empirical study. Int. J. Epidemiol. 2002, 31, 115–123. [Google Scholar] [CrossRef]
- Mazur, P. Kinetics of Water Loss from Cells at Subzero Temperatures and the Likelihood of Intracellular Freezing. J. Gen. Physiol. 1963, 47, 347–369. [Google Scholar] [CrossRef] [PubMed]
- Mazur, P. Cryobiology: The freezing of biological systems. Science 1970, 168, 939–949. [Google Scholar] [CrossRef] [PubMed]
- Mazur, P. The role of intracellular freezing in the death of cells cooled at supraoptimal rates. Cryobiology 1977, 14, 251–272. [Google Scholar] [CrossRef]
- Mazur, P.; Leibo, S.P.; Chu, E.H. A two-factor hypothesis of freezing injury. Evidence from Chinese hamster tissue-culture cells. Exp. Cell Res. 1972, 71, 345–355. [Google Scholar] [CrossRef]
- Erdim, M.; Tezel, E.; Numanoglu, A.; Sav, A. The effects of the size of liposuction cannula on adipocyte survival and the optimum temperature for fat graft storage: An experimental study. J. Plast. Reconstr. Aesthet. Surg. 2009, 62, 1210–1214. [Google Scholar] [CrossRef] [PubMed]
- Wolter, T.P.; von Heimburg, D.; Stoffels, I.; Groeger, A.; Pallua, N. Cryopreservation of mature human adipocytes: In vitro measurement of viability. Ann. Plast. Surg. 2005, 55, 408–413. [Google Scholar] [CrossRef] [PubMed]
- Son, D.; Oh, J.; Choi, T.; Kim, J.; Han, K.; Ha, S.; Lee, K. Viability of fat cells over time after syringe suction lipectomy: The effects of cryopreservation. Ann. Plast. Surg. 2010, 65, 354–360. [Google Scholar] [CrossRef] [PubMed]
- Hwang, S.M.; Lee, J.S.; Kim, H.D.; Jung, Y.H.; Kim, H.I. Comparison of the viability of cryopreserved fat tissue in accordance with the thawing temperature. Arch. Plast. Surg. 2015, 42, 143–149. [Google Scholar] [CrossRef] [Green Version]
- MacRae, J.W.; Tholpady, S.S.; Ogle, R.C.; Morgan, R.F. Ex vivo fat graft preservation: Effects and implications of cryopreservation. Ann. Plast. Surg. 2004, 52, 281–282. [Google Scholar] [CrossRef] [PubMed]
- Yong, K.W.; Safwani, W.; Xu, F.; Zhang, X.; Choi, J.R.; Abas, W.; Omar, S.Z.; Azmi, M.A.N.; Chua, K.H.; Pingguan-Murphy, B. Assessment of tumourigenic potential in long-term cryopreserved human adipose-derived stem cells. J. Tissue Eng. Regen. Med. 2017, 11, 2217–2226. [Google Scholar] [CrossRef] [PubMed]
- Lopez, M.; Bollag, R.J.; Yu, J.C.; Isales, C.M.; Eroglu, A. Chemically Defined and Xeno-Free Cryopreservation of Human Adipose-Derived Stem Cells. PLoS ONE 2016, 11, e0152161. [Google Scholar] [CrossRef]


{kind=link}
| Ref. | Level of Evidence OCEBM | Methods, Slow Cooling and Rapid Rewarming | CPA Concentration mol/L, Groups | Temperature, °C | Time | Results |
|---|---|---|---|---|---|---|
| Pu et al. [21] 2004 | Level 3 | Adipose aspirates from lipoplasty were randomised to each group and were evaluated by viable adipocyte counts, G3PDH assay and routine histology. | (1) Simple cryopreservation with liquid nitrogen only; (2) 0.5 mol/L DMSO + 0.2 mol/L trehalose; and (3) Control group with fresh adipose | −196 | 20 min | Group 2 showed significantly higher adipocyte viability and superior cellular function of adipocytes compared to group 1. (2.15 ± 0.68 vs. 1.04 ± 0.35 × 106/mL, P < 0.0001) |
| Pu et al. [25] 2006 | Level 3 | Cryopreserved adipocytes from cosmetic lipoplasty were administered into the posterior scalp of a nude mouse. Gross appearance of fat grafts was observed for up to 16 weeks. At the end of the study, final graft weight and volume and corresponding histology were determined. | (1) 0.5 mol/L DMSO + 0.2 mol/L trehalose solution; (2) Simple cryopreservation with liquid nitrogen only; and (3) Control group with fresh adipose aspirates | −196 | 20 min | Group 1 showed greater graft weight, volume and retained tissue architecture when compared to group 2 (P < 0.0001); the fresh control group showed a greater retained volume (47.7% ± 18.6%), and this was statistically significant relative to both groups 1 (35.3% ± 7.8%, P < 0.05) and 2 (6.5% ± 3.7%, P < 0.0001). |
| De Rosa et al. [26] 2009 | Level 3 | Different concentrations of CPA were evaluated to preserve ADSCs for future clinical applications. | (1) 1% DMSO (0.1 mol/L), 9% trehalose (0.26 mol/L), 90% FBS; (2) 4% DMSO (0.6 mol/L), 6% trehalose (0.18 mol/L), 90% FBS; (3) 8% DMSO (1.1 mol/L), 2% trehalose (0.06 mol/L), 90% FBS; and (4) 10% DMSO (1.4 mol/L), 90% FBS | −196 | 1, 6 and 12 months | The best freezing solution consisted of 90% FBS, 4% DMSO (0.6 mol/L) and 6% trehalose. The thawed cells in this group showed superior differentiation efficiency and higher levels of antigen expression, similar levels found in fresh isolates. |
| Cui et al. [27] 2010 | Level 3 | 0.5 mL of cryopreserved adipocyte grafts was thawed and injected into the posterior scalps of mice for 8 weeks. Graft volume, weight and histology were evaluated at the end of the study. | (1) 0.5 mol/L DMSO + 0.2 mol/L trehalose; (2) 0.35 mol/L trehalose; and (3) Control (fresh fat graft) | −196 | 20 min | Groups 1 and 2 showed no statistically significant difference in maintained volume (vs. 46.1% ± 14.4% vs. 38.2% ± 10.1%, NS) and weight (38.9% ± 14.7% vs. 34.1% ± 12.1%, NS). Both cryopreservation groups were found to be inferior to control (both P < 0.05). |
| Pu et al. [22] 2006 | Level 3 | In vitro study measuring the rate of growth and viable cell count (after 2 weeks) of fresh vs. cryopreserved (with fast rewarming) adipocyte aspirates. | (1) 0.5 mol/L DMSO + 0.2 mol/L trehalose and (2) Control fresh adipose aspirates | −196 | 20 min | The cryopreserved aspirates produced 90% of the cell count from fresh aspirates (3.7 ± 1.4 × 105 processed lipoaspirate cells per millilitre aspirates vs. 4.1 ± 1.4 × 105 cells/mL). |
| Cui et al. [23] 2007 | Level 3 | Different CPAs and their concentrations were tested in vitro. | (1) Fresh adipose aspirates; (2) Cryopreserved adipose aspirates without cryoprotectants; and (3) Cryopreserved adipose aspirates with cryoprotectants—0.2 mol/L DMSO + 0.1 mol/L trehalose, 0.5 mol/L DMSO + 0.2 mol/L trehalose, 0.25 mol/L trehalose, 0.5 mol/L trehalose, 1.0 mol/L DMSO, 1.5 mol/L DMSO | −196 | 20 min | The combination of 0.5 mol/L DMSO and 0.2 mol/L trehalose produced the greatest adipocyte count; group 3 produced a significantly higher adipocyte count than group 2 (2.06 ± 0.54 × 106/mL vs. 1.07 ± 0.41 × 106/mL, P < 0.0011); group 1 displayed only a marginally higher adipocyte count relative to group 3 (vs. 2.57 ± 0.56 × 106/mL vs. 2.06 ± 0.54 × 106/mL, P = 0.083); group 3 displayed less tissue shrinkage relative to group 2. |
| Cui et al. [23] 2007 | Level 3 | 1 mL fat graft was injected into nude mice and subsequently harvested 4 months later and analysed for volume, weight and histology. Maintenance of tissue architecture was rated as per the following scale: “5-pristine cellular architecture in all sections examined; 4-mild disruption of cellular architecture in <50% of sections; 3-mild disruption of cellular architecture in >50% of sections; 2-severe disruption of cellular architecture in <50% of sections; 1-severe disruption of cellular architecture in >50% of sections”. | (1) Fresh adipose aspirates; (2) Cryopreserved adipose aspirates without CPAs; and (3) Cryopreserved adipose aspirates with CPAs—0.5 mol/L DMSO + 0.2 mol/L trehalose | −196 | 1 week | Retained graft volume and weight were significantly higher in group 3 compared to group 2 (both P < 0.0001); histology showed extensive tissue fibrosis in group 2, in contrast to relatively preserved tissue architecture with very little fibrosis in group 3; the mean histological rating score in group 1 was significantly higher than that of group 2 (4.60 ± 0.22 vs. 1.50 ± 0.26, P < 0.0001). |
| Pu et al. [28] 2010 | Level 3 | The fat graft samples from both groups were evaluated with trypan blue vital staining, G3PDH assay and routine histology. | (1) 0.5 mol/L DMSO and 0.2 mol/L trehalose and (2) Fresh fat graft control | −196 | 20 min | Groups 1 and 2 showed similar adipocyte counts (3.46 ± 0.91 vs. 4.12 ± 1.11 × 106/mL, P = 0.22); activity of G3PDH was significantly higher in group 2 compared with group 1 (0.66 ± 0.09 vs. 0.47 ± 0.09 U/mL, P < 0.001); histological analysis showed mainly normal structure of fragmented fatty tissues in both groups. |
| Ref. | Level of Evidence OCEBM | Methods, Slow Cooling and Rapid Rewarming | CPA Concentration mol/L, Groups | Temperature, °C | Time | Results |
|---|---|---|---|---|---|---|
| Rao et al. [15] 2015 | Level 3 | To determine the cryopreservation of primary hADSCs using nanoparticle-mediated intracellular delivery of trehalose as the sole cryoprotectant. | (1) 0.2 mol/L trehalose; (2) 100 mL/L DMSO; and (3) Fresh control | −196 | 1 day | Trehalose acted as a successful CPA; cryopreservation with trehalose resulted in similar cell survival as compared to DMSO. |
| Dovgan et al. [7] 2016 | Level 3 | The efficiency of combining reversible electroporation and trehalose for cryopreservation of hADSCs. | (1) DMSO; (2) 0.25 mol/L trehalose with electroporation; and (3) 0.4 mol/L trehalose without electroporation | −196 | 1 week | No statistically significant difference between DMSO (91.5% ± 1.6%) and 250 mmol/L trehalose (83.8% ± 1.8%) treated with electroporation was observed, with a slight difference between DMSO and 0.4 trehalose without electroporation (78.4% ± 1.5%). |
| Roato et al. [29] 2016 | Level 3 | To evaluate ADSC viability and differentiation capability after cryopreservation. | (1) FBS + 10% DMSO and (2) FBS + 0.35 mol/L trehalose | −196 | 3 days | DMSO is superior to trehalose for cryopreservation of adipose tissue. Cell cultures demonstrated that ADSCs isolated from lipoaspirates cryopreserved in DMSO showed a higher growth rate and arrived at confluence in a few days with a better tissue architecture, compared to the cells preserved with trehalose. |
| Yong et al. [30] 2015 | Level 3 | To compare the effects of various combinations of CPA on hADSCs in terms of cell phenotype, proliferation potential, differentiation potential, stemness and viability. | (1) 0.25 mol/L trehalose; (2) 5% DMSO (0.7 mol/L); (3) 10% DMSO (1.4 mol/L); (4) 5% DMSO (0.7 mol/L) + 20% FBS; (5) 10% DMSO (1.4 mol/L) + 20% FBS; and (6) 10% DMSO (1.4 mol/L) + 90% FBS | −196 | 3 months | 5% DMSO without FBS may be an ideal CPA for efficient long-term cryopreservation of hADSCs. ADSCs preserved in 0.25 mol/L trehalose showed the lowest cell viability (P < 0.05). |
| Ref. | Level of Evidence OCEBM | Methods, Slow Cooling and Rapid Rewarming | CPA Concentration mol/L, Groups | Temperature, °C | Time | Results |
|---|---|---|---|---|---|---|
| Cui et al. [6] 2009 | Level 3 | Adipose aspirates were cryopreserved using trehalose as a CPA in seven different concentrations and compared to a fresh fat control group for viability in vitro. A G3PDH assay was also performed to assess intracellular function. | Trehalose: (1) 0.20 mol/L; (2) 0.25 mol/L; (3) 0.30 mol/L; (4) 0.35 mol/L; (5) 0.40 mol/L; (6) 0.50 mol/L; (7) 0.75 mol/L; and (8) Control | −196 | 20 min | Cryopreservation with 0.35 mol/L trehalose was found to preserve the most adipocytes. This concentration of trehalose showed no statistical difference relative to control (2.4 ± 0.52 vs. 1.88 ± 0.61 × 106/mL; P > 0.05). No concentration of trehalose showed a significant difference in intracellular function relative to control (all P > 0.05). |
| Cui et al. [27] 2010 | Level 3 | 0.5 mL of cryopreserved fat grafts was thawed and injected into the posterior scalps of mice for 8 weeks. Weight, volume and histology of grafts were analysed at the end of the study. | (1) 0.5 mol/L DMSO + 0.2 mol/L trehalose; (2) 0.35 mol/L trehalose; and (3) Control (fresh fat graft) | −196 | 20 min | Group 2 and group 1 were inferior to the control group (both P < 0.05). There was a significantly higher percentage of maintained volume of injected fat in the control group (55.5% ± 11.7%) compared to group 1 (46.1% ± 14.4%, P < 0.05) or group 2 (38.2% ± 10.5%, P < 0.01). The control group showed a significantly higher maintained weight relative to both groups 1 (38.9% ± 14.7%, P < 0.01) and 2 (34.1% ± 12.1%, P < 0.01). |
| Rao et al. [15] 2015 | Level 3 | To determine the cryopreservation of primary hADSCs using nanoparticle-mediated intracellular delivery of trehalose as the sole CPA. | (1) 0.2 mol/L trehalose; (2) 100 mL/L DMSO; and (3) Fresh control | −196 | 1 day | hADSCs’ tissue architecture post cryopreservation with trehalose is similar to that of fresh isolates. Trehalose maintained comparable differentiation capabilities of the cryopreserved vs. fresh hADSCs. Trehalose acted as a successful cryoprotectant. |
| Pu et al. [31] 2005 | Level 3 | The efficacy of trehalose as the sole CPA for cryopreservation of adipocytes, with the aim to develop a protocol which enables optimal preservation of adipose tissues. | (1) Control fresh adipose aspirates; (2) Simple cryopreservation group: cryopreserved adipose aspirates without CPAs; and (3) Optimal cryopreservation group: 0.25 mol/L trehalose | −196 | 20 min | Adipocyte count was significantly higher in group 3 than group 2 (1.78 ± 0.33 vs. 0.99 ± 0.35 × 106/mL, P < 0.0001). Adipocyte count in group 3 was significantly lower than fresh isolates (1.78 ± 0.33 vs. 2.64 ± 0.54 × 106/mL, P < 0.001). The G3PDH activity in group 3 was also significantly lower than control (0.24 ± 0.07 vs. 0.32 ± 0.09 U/mL, P < 0.05). There was a statistically significant increase in G3PDH activity, which was significantly higher in group 3 relative to group 2 (0.24 ± 0.07 vs. 0.15 ± 0.06 U/mL, P < 0.01). |
| Cui et al. [23] 2007 | Level 3 | In vitro study where different cryoprotectant agents and their concentrations were tested. | (1) Fresh adipose aspirates; (2) Cryopreserved adipose aspirates without CPAs; and (3) Cryopreserved adipose aspirates with CPAs. (1) 0.2 mol/L DMSO + 0.1 mol/L trehalose; (2) 0.5 mol/L DMSO + 0.2 mol/L trehalose; (3) 0.25 mol/L trehalose; (4) 0.5 mol/L trehalose; (5) 1.0 mol/L DMSO; and (6) 1.5 mol/L DMSO | −196 | 20 min | The viable adipocyte count in the fresh fat control group was still significantly higher than the count in any of the six different CPA groups (all P < 0.0001). Significantly higher integrated viable adipocyte count of adipose aspirates was found in group 3 compared with group 2 (2.06 ± 0.54 × 106/mL vs. 1.07 ± 0.41 × 106/mL, P < 0.001). |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Crowley, C.A.; Smith, W.P.W.; Seah, K.T.M.; Lim, S.-K.; Khan, W.S. Cryopreservation of Human Adipose Tissues and Adipose-Derived Stem Cells with DMSO and/or Trehalose: A Systematic Review. Cells 2021, 10, 1837. https://doi.org/10.3390/cells10071837
Crowley CA, Smith WPW, Seah KTM, Lim S-K, Khan WS. Cryopreservation of Human Adipose Tissues and Adipose-Derived Stem Cells with DMSO and/or Trehalose: A Systematic Review. Cells. 2021; 10(7):1837. https://doi.org/10.3390/cells10071837
Chicago/Turabian StyleCrowley, Conor A., William P. W. Smith, K. T. Matthew Seah, Soo-Keat Lim, and Wasim S. Khan. 2021. "Cryopreservation of Human Adipose Tissues and Adipose-Derived Stem Cells with DMSO and/or Trehalose: A Systematic Review" Cells 10, no. 7: 1837. https://doi.org/10.3390/cells10071837
APA StyleCrowley, C. A., Smith, W. P. W., Seah, K. T. M., Lim, S. -K., & Khan, W. S. (2021). Cryopreservation of Human Adipose Tissues and Adipose-Derived Stem Cells with DMSO and/or Trehalose: A Systematic Review. Cells, 10(7), 1837. https://doi.org/10.3390/cells10071837