

Pre-Clinical Evaluation of Efficacy and Safety of Human Limbus-Derived Stromal/Mesenchymal Stem Cells with and without Alginate Encapsulation for Future Clinical Applications



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Ethical Approvals
2.1.1. Approvals
2.1.2. Donor Corneas
2.1.3. Characterization of hLMSCs Expanded in GMP-Compliant Clean Room
2.1.4. Assessment of the Efficacy of hLMSCs in a Murine Model of Corneal Scar
2.1.5. Determination of Safety and Toxicity of hLMSCs in Rabbits with Corneal Wounds
2.2. Isolation and Expansion of hLMSCs
2.3. Analyzing the Distinctive Phenotype of hLMSCs
2.3.1. Immunostaining
2.3.2. FACS
2.4. Assessment of hLMSC Stability
2.4.1. Evaluation of the Viability of Pelletized hLMSCs
2.4.2. Karyotyping
2.4.3. Growth Kinetics
2.5. Assessment of the Sterility of hLMSCs
2.5.1. Mycoplasma Assessment
2.5.2. Endotoxin Levels
2.6. Generation of the Murine Model of Corneal Scar
2.7. Assessment of Safety and Toxicity of hLMSCs
2.7.1. Rabbit Body Weights and Death Rates
2.7.2. Ophthalmic Investigations
2.7.3. Inflammatory Marker Quantification
Schirmer Strip Tear Fluid Extraction
BCA Protein Quantitation
Quantification of Markers through Immunoassay
2.7.4. Blood Investigations
2.7.5. Tissue Evaluations
External Examinations and Necropsies
Organs Weights and Histopathology
2.8. Statistical Analysis
3. Results
3.1. Characteristic Analysis of hLMSCs
3.1.1. Phenotypic Assessment of hLMSCs
3.1.2. Evaluation of the Viability and Stability of hLMSCs
3.2. Comparison of the Effectiveness of the hLMSCs with and without the Incorporation of Alginate
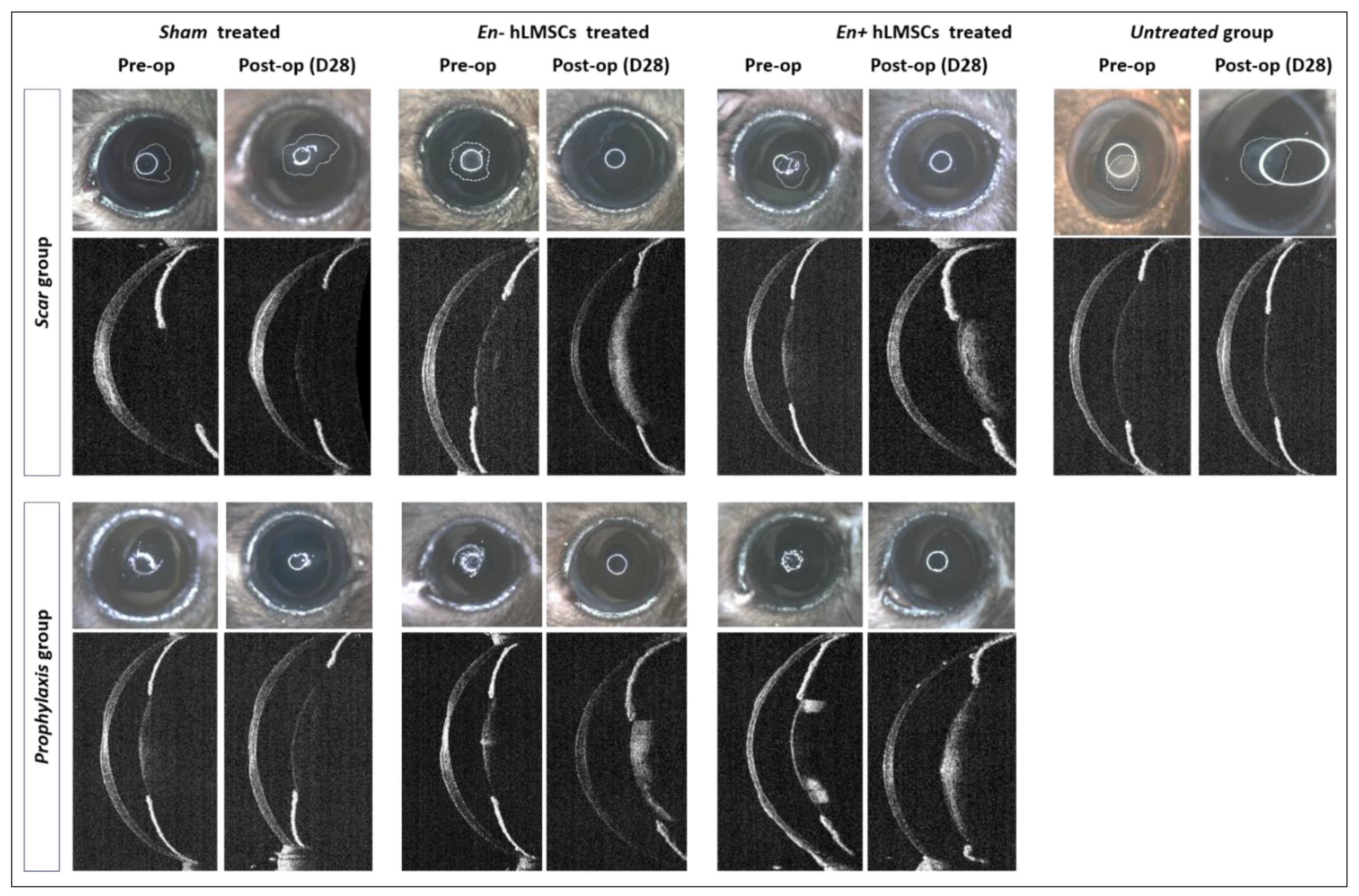
3.2.1. Change in Corneal Haze
3.2.2. Reduction in the Scar Area
3.2.3. Epithelium to Stroma Reflectivity
3.3. Determination of the Safety and Toxicity of hLMSCs
3.3.1. Clinical Symptoms, Body Weights, and Death Rate
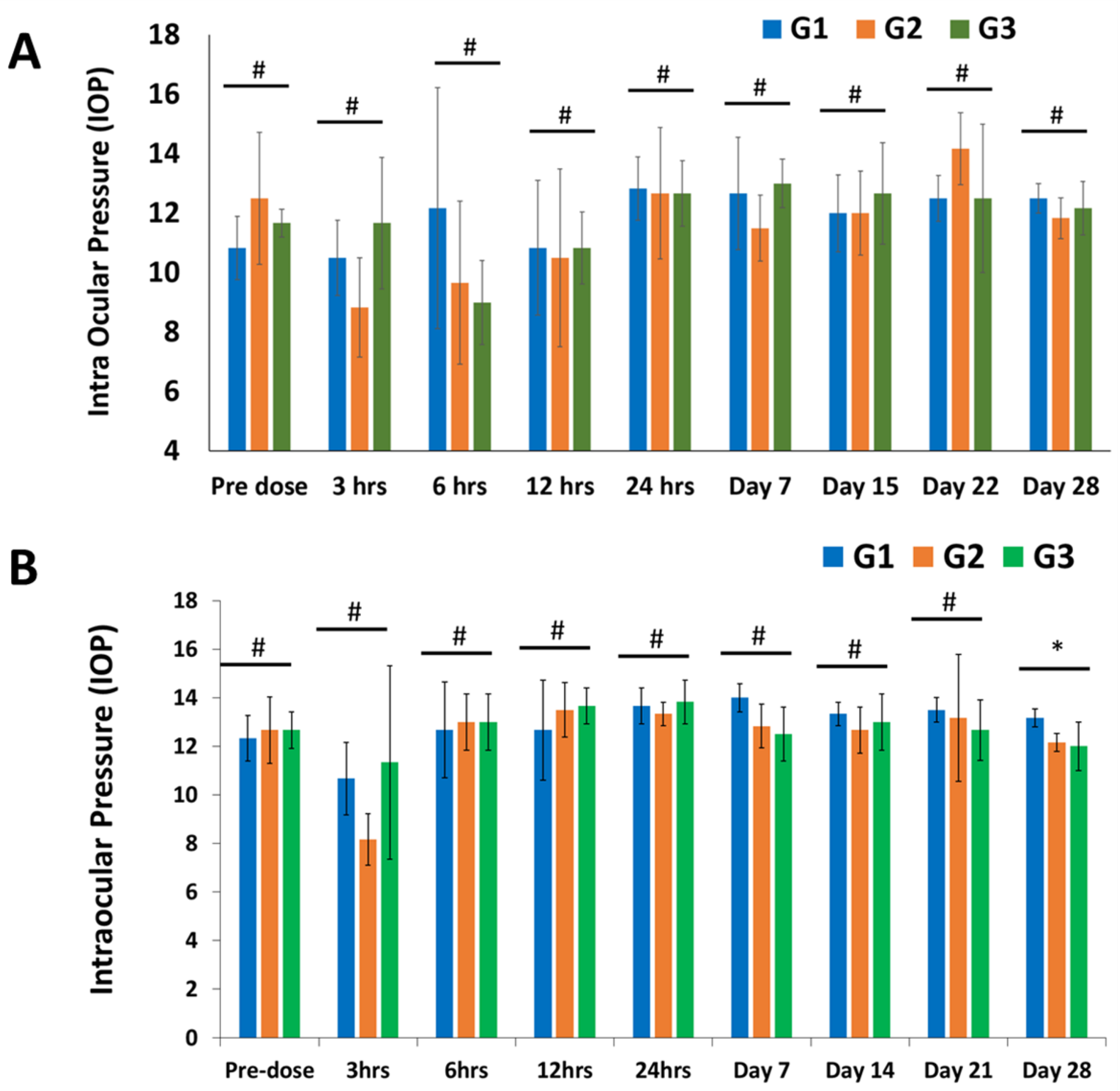
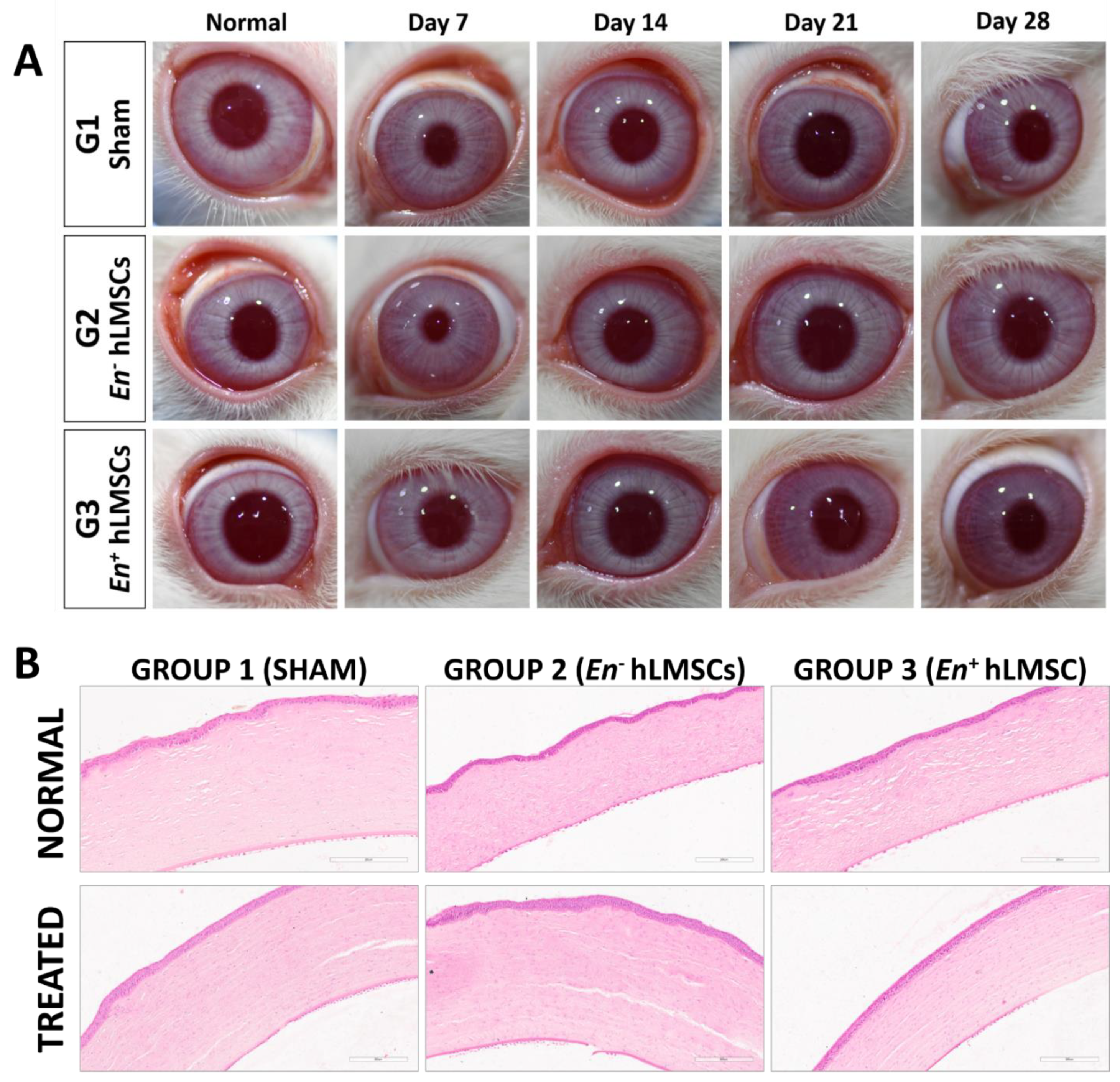
3.3.2. Ophthalmic Observations and IOP
3.3.3. Evaluation of Immunogenicity and Inflammatory Markers
3.3.4. Hematology
3.3.5. Clinical Chemistry
3.3.6. Organ Weights, Gross Observations, and Necropsy
3.3.7. Histopathology
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Maurice, D.M. The Structure and Transparency of the Cornea. J. Physiol. 1957, 136, 263–286. [Google Scholar] [CrossRef] [PubMed]
- Meek, K.M.; Boote, C. The Organization of Collagen in the Corneal Stroma. Exp. Eye Res. 2004, 78, 503–512. [Google Scholar] [CrossRef] [PubMed]
- Funderburgh, J.L.; Mann, M.M.; Funderburgh, M.L. Keratocyte Phenotype Mediates Proteoglycan Structure: A Role for Fibroblasts in Corneal Fibrosis. J. Biol. Chem. 2003, 278, 45629–45637. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Basu, S.; Hertsenberg, A.J.; Funderburgh, M.L.; Burrow, M.K.; Mann, M.M.; Du, Y.; Lathrop, K.L.; Syed-Picard, F.N.; Adams, S.M.; Birk, D.E.; et al. Human Limbal Biopsy-Derived Stromal Stem Cells Prevent Corneal Scarring. Sci. Transl. Med. 2014, 6, 266ra172. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jester, J.V.; Rodrigues, M.M.; Herman, I.M. Characterization of Avascular Corneal Wound Healing Fibroblasts. New Insights into the Myofibroblast. Am. J. Pathol. 1987, 127, 140–148. [Google Scholar]
- Torricelli, A.A.M.; Santhanam, A.; Wu, J.; Singh, V.; Wilson, S.E. The Corneal Fibrosis Response to Epithelial-Stromal Injury. Exp. Eye Res. 2016, 142, 110–118. [Google Scholar] [CrossRef] [Green Version]
- Singh, V.; Santhiago, M.R.; Barbosa, F.L.; Agrawal, V.; Singh, N.; Ambati, B.K.; Wilson, S.E. Effect of TGFβ and PDGF-B Blockade on Corneal Myofibroblast Development in Mice. Exp. Eye Res. 2011, 93, 810–817. [Google Scholar] [CrossRef] [Green Version]
- Wilson, S.E. TGF Beta -1, -2 and -3 in the Modulation of Fibrosis in the Cornea and Other Organs. Exp. Eye Res. 2021, 207, 108594. [Google Scholar] [CrossRef]
- Thompson, R.W.; Price, M.O.; Bowers, P.J.; Price, F.W. Long-Term Graft Survival after Penetrating Keratoplasty. Ophthalmology 2003, 110, 1396–1402. [Google Scholar] [CrossRef]
- Coster, D.J.; Williams, K.A. The Impact of Corneal Allograft Rejection on the Long-Term Outcome of Corneal Transplantation. Am. J. Ophthalmol. 2005, 140, 1112–1122. [Google Scholar] [CrossRef] [Green Version]
- Williams, K.A.; Lowe, M.; Bartlett, C.; Kelly, T.-L.; Coster, D.J. All Contributors Risk Factors for Human Corneal Graft Failure within the Australian Corneal Graft Registry. Transplantation 2008, 86, 1720–1724. [Google Scholar] [CrossRef]
- Mittal, S.K.; Omoto, M.; Amouzegar, A.; Sahu, A.; Rezazadeh, A.; Katikireddy, K.R.; Shah, D.I.; Sahu, S.K.; Chauhan, S.K. Restoration of Corneal Transparency by Mesenchymal Stem Cells. Stem Cell Rep. 2016, 7, 583–590. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Du, Y.; Funderburgh, M.L.; Mann, M.M.; SundarRaj, N.; Funderburgh, J.L. Multipotent Stem Cells in Human Corneal Stroma. Stem Cells 2005, 23, 1266–1275. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kureshi, A.K.; Dziasko, M.; Funderburgh, J.L.; Daniels, J.T. Human Corneal Stromal Stem Cells Support Limbal Epithelial Cells Cultured on RAFT Tissue Equivalents. Sci. Rep. 2015, 5, 16186. [Google Scholar] [CrossRef] [Green Version]
- Funderburgh, J.L.; Funderburgh, M.L.; Du, Y. Stem Cells in the Limbal Stroma. Ocul. Surf. 2016, 14, 113–120. [Google Scholar] [CrossRef] [Green Version]
- Dos Santos, A.; Balayan, A.; Funderburgh, M.L.; Ngo, J.; Funderburgh, J.L.; Deng, S.X. Differentiation Capacity of Human Mesenchymal Stem Cells into Keratocyte Lineage. Investig. Ophthalmol. Vis. Sci. 2019, 60, 3013–3023. [Google Scholar] [CrossRef] [Green Version]
- Du, Y.; Carlson, E.C.; Funderburgh, M.L.; Birk, D.E.; Pearlman, E.; Guo, N.; Kao, W.W.-Y.; Funderburgh, J.L. Stem Cell Therapy Restores Transparency to Defective Murine Corneas. Stem Cells 2009, 27, 1635–1642. [Google Scholar] [CrossRef] [Green Version]
- Coppola, A.; Tomasello, L.; Pitrone, M.; Cillino, S.; Richiusa, P.; Pizzolanti, G.; Giordano, C. Human Limbal Fibroblast-like Stem Cells Induce Immune-Tolerance in Autoreactive T Lymphocytes from Female Patients with Hashimoto’s Thyroiditis. Stem Cell Res. Ther. 2017, 8, 154. [Google Scholar] [CrossRef] [Green Version]
- Mitragotri, N.; Damala, M.; Singh, V.; Basu, S. Limbal Stromal Stem Cells in Corneal Wound Healing: Current Perspectives and Future Applications. In Corneal Regeneration: Therapy and Surgery; Alió, J.L., Alió del Barrio, J.L., Arnalich-Montiel, F., Eds.; Essentials in Ophthalmology; Springer International Publishing: Cham, Switzerland, 2019; pp. 387–402. ISBN 978-3-030-01304-2. [Google Scholar]
- Del Barrio, J.L.A.; El Zarif, M.; de Miguel, M.P.; Azaar, A.; Makdissy, N.; Harb, W.; El Achkar, I.; Arnalich-Montiel, F.; Alió, J.L. Cellular Therapy With Human Autologous Adipose-Derived Adult Stem Cells for Advanced Keratoconus. Cornea 2017, 36, 952–960. [Google Scholar] [CrossRef]
- Basu, S.; Damala, M.; Singh, V. Limbal Stromal Stem Cell Therapy for Acute and Chronic Superficial Corneal Pathologies: Early Clinical Outcomes of The Funderburgh Technique. Investig. Ophthalmol. Vis. Sci. 2017, 58, 3371. [Google Scholar]
- Funderburgh, J.; Basu, S.; Damala, M.; Tavakkoli, F.; Sangwan, V.; Singh, V. Limbal Stromal Stem Cell Therapy for Acute and Chronic Superficial Corneal Pathologies: One-Year Outcomes. Investig. Ophthalmol. Vis. Sci. 2018, 59, 3455. [Google Scholar]
- Singh, V.; Agarwal, H.; Kethiri, A.R.; Damala, M.; Basu, S.; Sangwan, V.S. Immunological Characterization of Chemical Burn-Induced Ocular Surface Pannus in Humans, Rabbits and Mice after Limbal Stem Cell Deficiency. Investig. Ophthalmol. Vis. Sci. 2017, 58, 1423. [Google Scholar]
- Nurković, J.S.; Vojinović, R.; Dolićanin, Z. Corneal Stem Cells as a Source of Regenerative Cell-Based Therapy. Stem Cells Int. 2020, 2020, 8813447. [Google Scholar] [CrossRef]
- Damala, M.; Swioklo, S.; Koduri, M.A.; Mitragotri, N.S.; Basu, S.; Connon, C.J.; Singh, V. Encapsulation of Human Limbus-Derived Stromal/Mesenchymal Stem Cells for Biological Preservation and Transportation in Extreme Indian Conditions for Clinical Use. Sci. Rep. 2019, 9, 16950. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- The Association for Research in Vision and Ophthalmology-Statement for the Use of Animals in Ophthalmic and Vision Research. Available online: https://www.arvo.org/About/policies/statement-for-the-use-of-animals-in-ophthalmic-and-vision-research/#three (accessed on 3 September 2022).
- Ich-m-3-R2-Non-Clinical-Safety-Studies-Conduct-Human-Clinical-Trials-Marketing-Authorization_en.Pdf. Available online: https://www.ema.europa.eu/en/documents/scientific-guideline/ich-m-3-r2-non-clinical-safety-studies-conduct-human-clinical-trials-marketing-authorization_en.pdf (accessed on 7 November 2022).
- OECD. Test No. 405: Acute Eye Irritation/Corrosion; Organisation for Economic Co-Operation and Development: Paris, France, 2021. [Google Scholar]
- Dominici, M.; Le Blanc, K.; Mueller, I.; Slaper-Cortenbach, I.; Marini, F.; Krause, D.; Deans, R.; Keating, A.; Prockop, D.; Horwitz, E. Minimal Criteria for Defining Multipotent Mesenchymal Stromal Cells. The International Society for Cellular Therapy Position Statement. Cytotherapy 2006, 8, 315–317. [Google Scholar] [CrossRef] [PubMed]
- Endotoxin Testing Recommendations for Single-Use Intraocular Ophthalmic Devices—Guidance for Industry and Food and Drug Administration Staff. 9. Available online: https://www.fda.gov/media/88615/download (accessed on 7 November 2022).
- Schedule Y(Ammended Version)—CDSCO. 48. Available online: https://rgcb.res.in/documents/Schedule-Y.pdf (accessed on 7 November 2022).
- Posa, A.; Bräuer, L.; Schicht, M.; Garreis, F.; Beileke, S.; Paulsen, F. Schirmer Strip vs. Capillary Tube Method: Non-Invasive Methods of Obtaining Proteins from Tear Fluid. Ann. Anat.-Anat. Anz. Ann. 2013, 195, 137–142. [Google Scholar] [CrossRef]
- McTiernan, C.D.; Simpson, F.C.; Haagdorens, M.; Samarawickrama, C.; Hunter, D.; Buznyk, O.; Fagerholm, P.; Ljunggren, M.K.; Lewis, P.; Pintelon, I.; et al. LiQD Cornea: Pro-Regeneration Collagen Mimetics as Patches and Alternatives to Corneal Transplantation. Sci. Adv. 2020, 6, eaba2187. [Google Scholar] [CrossRef]
- Fernández-Pérez, J.; Madden, P.W.; Ahearne, M. Engineering a Corneal Stromal Equivalent Using a Novel Multilayered Fabrication Assembly Technique. Tissue Eng. Part A 2020, 26, 1030–1041. [Google Scholar] [CrossRef]
- Wang, F.; Shi, W.; Li, H.; Wang, H.; Sun, D.; Zhao, L.; Yang, L.; Liu, T.; Zhou, Q.; Xie, L. Decellularized Porcine Cornea-Derived Hydrogels for the Regeneration of Epithelium and Stroma in Focal Corneal Defects. Ocul. Surf. 2020, 18, 748–760. [Google Scholar] [CrossRef]
- Chameettachal, S.; Prasad, D.; Parekh, Y.; Basu, S.; Singh, V.; Bokara, K.K.; Pati, F. Prevention of Corneal Myofibroblastic Differentiation In Vitro Using a Biomimetic ECM Hydrogel for Corneal Tissue Regeneration. ACS Appl. Bio Mater. 2021, 4, 533–544. [Google Scholar] [CrossRef]
- WO2019169380A1-Stem Cell-Derived Exosomes for the Treatment of Corneal Scarring—Google Patents. Available online: https://patents.google.com/patent/WO2019169380A1/en (accessed on 11 July 2022).
- Saika, S.; Yamanaka, O.; Okada, Y.; Tanaka, S.-I.; Miyamoto, T.; Sumioka, T.; Kitano, A.; Shirai, K.; Ikeda, K. TGF Beta in Fibroproliferative Diseases in the Eye. Front. Biosci.-Sch. 2009, 1, 376–390. [Google Scholar] [CrossRef] [PubMed]
- Kamiyama, K.; Iguchi, I.; Wang, X.; Imanishi, J. Effects of PDGF on the Migration of Rabbit Corneal Fibroblasts and Epithelial Cells. Cornea 1998, 17, 315–325. [Google Scholar] [CrossRef]
- Kim, W.J.; Mohan, R.R.; Mohan, R.R.; Wilson, S.E. Effect of PDGF, IL-1alpha, and BMP2/4 on Corneal Fibroblast Chemotaxis: Expression of the Platelet-Derived Growth Factor System in the Cornea. Investig. Ophthalmol. Vis. Sci. 1999, 40, 1364–1372. [Google Scholar]
- Miyagi, H.; Thomasy, S.M.; Russell, P.; Murphy, C.J. The Role of Hepatocyte Growth Factor in Corneal Wound Healing. Exp. Eye Res. 2018, 166, 49–55. [Google Scholar] [CrossRef]
- de Oliveira, R.C.; Murillo, S.; Saikia, P.; Wilson, S.E. The Efficacy of Topical HGF on Corneal Fibrosis and Epithelial Healing after Scar-Producing PRK Injury in Rabbits. Transl. Vis. Sci. Technol. 2020, 9, 29. [Google Scholar] [CrossRef] [Green Version]
- Maltseva, O.; Folger, P.; Zekaria, D.; Petridou, S.; Masur, S.K. Fibroblast Growth Factor Reversal of the Corneal Myofibroblast Phenotype. Investig. Ophthalmol. Vis. Sci. 2001, 42, 2490–2495. [Google Scholar]
- Ljubimov, A.V.; Saghizadeh, M. Progress in Corneal Wound Healing. Prog. Retin. Eye Res. 2015, 49, 17–45. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Medeiros, C.S.; Marino, G.K.; Santhiago, M.R.; Wilson, S.E. The Corneal Basement Membranes and Stromal Fibrosis. Investig. Ophthalmol. Vis. Sci. 2018, 59, 4044–4053. [Google Scholar] [CrossRef] [Green Version]
- Wilson, S.E. Corneal Wound Healing. Exp. Eye Res. 2020, 197, 108089. [Google Scholar] [CrossRef]
- Mathew, B.; Ravindran, S.; Liu, X.; Torres, L.; Chennakesavalu, M.; Huang, C.-C.; Feng, L.; Zelka, R.; Lopez, J.; Sharma, M.; et al. Mesenchymal Stem Cell-Derived Extracellular Vesicles and Retinal Ischemia-Reperfusion. Biomaterials 2019, 197, 146–160. [Google Scholar] [CrossRef]
- Bagno, L.; Hatzistergos, K.E.; Balkan, W.; Hare, J.M. Mesenchymal Stem Cell-Based Therapy for Cardiovascular Disease: Progress and Challenges. Mol. Ther. 2018, 26, 1610–1623. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Putra, I.; Shen, X.; Anwar, K.N.; Rabiee, B.; Samaeekia, R.; Almazyad, E.; Giri, P.; Jabbehdari, S.; Hayat, M.R.; Elhusseiny, A.M.; et al. Preclinical Evaluation of the Safety and Efficacy of Cryopreserved Bone Marrow Mesenchymal Stromal Cells for Corneal Repair. Transl. Vis. Sci. Technol. 2021, 10, 3. [Google Scholar] [CrossRef] [PubMed]
- NewDrugs_CTRules_2019.Pdf. Available online: https://cdsco.gov.in/opencms/export/sites/CDSCO_WEB/Pdf-documents/NewDrugs_CTRules_2019.pdf (accessed on 7 November 2022).
- Wright, B.; Cave, R.A.; Cook, J.P.; Khutoryanskiy, V.V.; Mi, S.; Chen, B.; Leyland, M.; Connon, C.J. Enhanced Viability of Corneal Epithelial Cells for Efficient Transport/Storage Using a Structurally Modified Calcium Alginate Hydrogel. Regen. Med. 2012, 7, 295–307. [Google Scholar] [CrossRef] [PubMed] [Green Version]








Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Damala, M.; Sahoo, A.; Pakalapati, N.; Singh, V.; Basu, S. Pre-Clinical Evaluation of Efficacy and Safety of Human Limbus-Derived Stromal/Mesenchymal Stem Cells with and without Alginate Encapsulation for Future Clinical Applications. Cells 2023, 12, 876. https://doi.org/10.3390/cells12060876
Damala M, Sahoo A, Pakalapati N, Singh V, Basu S. Pre-Clinical Evaluation of Efficacy and Safety of Human Limbus-Derived Stromal/Mesenchymal Stem Cells with and without Alginate Encapsulation for Future Clinical Applications. Cells. 2023; 12(6):876. https://doi.org/10.3390/cells12060876
Chicago/Turabian StyleDamala, Mukesh, Abhishek Sahoo, Naveen Pakalapati, Vivek Singh, and Sayan Basu. 2023. "Pre-Clinical Evaluation of Efficacy and Safety of Human Limbus-Derived Stromal/Mesenchymal Stem Cells with and without Alginate Encapsulation for Future Clinical Applications" Cells 12, no. 6: 876. https://doi.org/10.3390/cells12060876
APA StyleDamala, M., Sahoo, A., Pakalapati, N., Singh, V., & Basu, S. (2023). Pre-Clinical Evaluation of Efficacy and Safety of Human Limbus-Derived Stromal/Mesenchymal Stem Cells with and without Alginate Encapsulation for Future Clinical Applications. Cells, 12(6), 876. https://doi.org/10.3390/cells12060876