
Shifting the Cancer Screening Paradigm: The Rising Potential of Blood-Based Multi-Cancer Early Detection Tests




Abstract
:1. Introduction
2. Multi-Cancer Early Detection (MCED) Tests: State of the Art
2.1. Mutation-Based MCED Tests
2.2. DNA Methylation-Based MCED Tests
2.3. Fragmentation-Based MCED Tests
2.4. Gene Expression/Non-Coding RNA-Based MCED Tests
2.5. Circulating Tumor Cell-Based MCED Tests
2.6. Extracellular Vesicle-Based MCED Tests
2.7. Other Approaches to MCED Tests

{kind=link}
{kind=link}
{kind=link}
| Biomarker | Source | Tumor Types | Sample | Methods | Main Findings | Test/ Company | Ref. |
|---|---|---|---|---|---|---|---|
| DNA methylation | Tissue | lung, breast, colorectal, esophagus, liver, pancreatic, gastric, cervical, head and neck | 120 tumor tissue 123 normal tissue | Bisulfite pyrosequencing | TCGA methylation data mining identified HIST1H4F as hypermethylated in 17 tumor types. Methylation analysis in tissue samples of 9 cancer types showed AUCs above 0.87 for all cancers and above 0.90 for all except pancreatic cancer. | -- | [121] |
| Tissue | lung, breast, colorectal, prostate, pancreas, glioblastoma, and B cell chronic lymphocytic leukemia | 83 tumor tissue 54 normal tissue | Bisulfite pyrosequencing | Methylation levels at 27 CpGs of the GHSR gene showed a higher average methylation degree in all tumor samples compared to normal samples. 27 CpG-signature displayed an AUC of 0.8789 for discriminating cancer from normal tissue. | -- | [122] | |
| Tissue | colorectal, gastric, and esophageal | 229 tumor and normal-adjacent tissue | Bisulfite sequencing PCR | TCGA methylation data mining identified differentially methylated regions (DMRs) in the SST gene. 7 CpG sites were shown to be hypermethylated in all 3 cancers. A combination of 2 CpGs (+18 and +129) displayed the best AUC of 0.698, with 59.3% sensitivity and 72.8% specificity for detecting the 3 gastrointestinal cancers. | -- | [123] | |
| Tissue | lung, breast, colon, gastric, and endometrial | 184 tumor tissue 34 normal tissue | Bisulfite amplicon sequencing | Designed a 302-bp PCR amplicon, covering the ZNF154 tumor-specific hypermethylated region, and methylation patterns were used to develop a multi-cancer classifier. AUC of 0.96 for discriminating cancer from normal tissue. Computational simulation of ctDNA displayed AUCs of up to 0.79. | -- | [124] | |
| Plasma | colon, pancreatic, liver, and ovarian | 71 cancer patients 20 healthy individuals | DREAMing | TCGA methylation data from white blood cells revealed that ZNF154 locus remains unmethylated, even in older individuals, showing the potential for the development of a blood test for cancer detection. AUC values ranged from 0.75 to 0.87 for discriminating cancer patients from healthy individuals, except for liver cancer which displayed an AUC of 0.48. | -- | [42] | |
| Plasma | lung and prostate | 323 cancer patients 136 healthy individuals | qMSP | “PanCancer” panel (FOXA1, RARβ2, and RASSF1A) detected cancer with 64.3% sensitivity, 69.8% specificity and 66.4% accuracy. “CancerType” panel (GSTP1 and SOX17) discriminated between lung and prostate cancer with 93% specificity. | -- | [44] | |
| Plasma | lung, breast, and colorectal | 253 cancer patients 103 healthy individuals | qMSP | “PanCancer” panel (APC, FOXA1, RASSF1A) detected cancer with 72.4% sensitivity, 73.5% specificity and 72.8% accuracy. “CancerType” panel (SCGB3A1, SEPT9, and SOX17) discriminated TOO with 80.0%, 98.9%, and 85.1% specificity for breast, colorectal, and lung cancer, respectively. | -- | [43] | |
| Serum | lung, breast, colorectal, gastric, pancreatic, and hepatocellular | 70 cancer patients 10 healthy individuals | MSP | Methylation levels of a 4 gene-panel (RUNX3, p16, RASSF1A, and CDH1) showed 89% sensitivity and 100% specificity for cancer detection. | -- | [125] | |
| Plasma | colorectal and pancreatic | 60 cancer patients 60 healthy individuals | Methylation array | Found a 7 gene panel (MDR1, SRBC, VHL, MUC2, RB1, SYK, and GPC3) that detects colorectal and pancreatic cancers with 63.16% sensitivity, 84% specificity, and AUC of 0.8177. | -- | [126] | |
| Plasma | lung, breast, and liver | 46 cancer patients 32 healthy individuals | Bisulfite sequencing | Developed CancerLocator, a test based on cfDNA bisulfite sequencing combined with a probabilistic model for cancer detection and TOO discrimination. CancerLocator uses TCGA methylation data as features to estimate the fraction of ctDNA in the plasma and the likelihood of coming from each tumor type. TOO discrimination showed a low error rate of 0.265 (99.7% accuracy). | Cancer Locator | [127] | |
| Plasma | liver but applicable to any cancer | 33 cancer patients 36 healthy individuals | Bisulfite sequencing | Developed CancerDetector, a test based on cfDNA bisulfite sequencing combined with a probabilistic model that joints methylation states of multiple adjacent CpG sites on an individual sequencing read, for cancer detection. 94.8% sensitivity and 100% specificity were obtained. | Cancer Detector | [128] | |
| Plasma | > 50 cancer types | 2482 cancer patients 4207 healthy individuals | Bisulfite sequencing | Developed a targeted methylation assay combined with a machine learning classifier for detecting and discriminating TOO in more than 50 cancer types using cfDNA. 54.9% sensitivity and 99.3% specificity were obtained in the validation set. 93% accuracy for TOO prediction. | Galleri (GRAIL) | [54] | |
| 2823 cancer patients 1254 healthy individuals | Developed a refined assay and classifiers optimized for screening purposes and performed clinical validation. 51.5% sensitivity and 99.5% specificity were obtained. 88.7% accuracy for TOO prediction. PPV of 44.4% and NPV of 99.4% for cancer detection. | [55] | |||||
| Plasma | colorectal, hepatocellular, esophageal, gastric, and pancreatic | 254 cancer patients 46 healthy individuals | Bisulfite sequencing | Developed EpiPanGI Dx, a cfDNA methylation-based test combining bisulfite sequencing and machine learning, for detecting and discriminating TOO of gastrointestinal cancers. AUC of 0.88 for detecting gastrointestinal cancers. Accuracy of 0.85–0.95 for TOO prediction. | EpiPanGI Dx | [45] | |
| Plasma | lung, colorectal, gastric, liver, and esophageal | 191 pre-diagnosis cancer samples 223 post-diagnosis cancer samples 414 healthy samples | Bisulfite sequencing (using semi-targeted PCR libraries) | Developed PanSeer, a blood test combining the analysis of 477 cancer-specific differentially methylated regions with machine learning for cancer detection. 87.6% sensitivity for post-diagnosis samples, 94.9% sensitivity for pre-diagnosis samples and 96.1% specificity were obtained in the testing set. Cancer can be detected by PanSeer up to 4 years before conventional diagnosis with 95.7% sensitivity. | PanSeer (Singlera Genomics) | [49] | |
| Plasma | lung, pancreatic, and acute myeloid leukemia | 137 cancer patients 62 healthy individuals | cfMeDIP-seq | Developed cfMeDIP-seq, an immunoprecipitation-based protocol for methylation profiling in cfDNA and combined it with machine learning algorithms to discriminate TOO. AUC values ranged from 0.92 to 0.98 for discriminating TOO. | Adela, Inc. | [64] | |
| Plasma | lung, breast, colorectal, and melanoma | 78 cancer patients 66 healthy individuals | Bisulfite sequencing | Developed a targeted methylation sequencing assay to analyze the methylation status of 9 223 cancer related CpG sites, combined with a novel algorithm that converts sequencing data into a methylation score, for cancer detection and TOO discrimination. 83.8% sensitivity and 100% specificity were obtained for cancer detection. 78.9% accuracy for TOO discrimination. | -- | [129] | |
| Plasma | Lung, breast, colorectal, and liver | Not available | NGS | Developed IvyGeneCORE Test, a blood test analyzing cfDNA methylation levels at specific genes combined with artificial intelligence for cancer detection. 84% sensitivity and 90% specificity were obtained for discriminating cancer from healthy individuals. | IvyGeneCORE (Laboratory for Advanced Medicine) | [47] | |
| Plasma | lung, colorectal, pancreatic, liver, esophageal, and ovarian | 625 cancer patients 483 healthy individuals | ELSA-seq | Developed ELSA-seq, a targeted methylation sequencing assay combined with machine learning for cancer detection and TOO discrimination. 80.6% sensitivity and 98.3% specificity were obtained in validation set. 81.0% accuracy for TOO discrimination. | OverC (Burning Rock Dx) | [130] | |
| Plasma | 14 cancer types | 549 cancer patients 80 healthy individuals | Targeted sequencing | Developed a cancer detection model based on 37 methylation-correlated blocks (MCB). 72.86% sensitivity, 96.67% specificity, and AUC of 0.86 were obtained in the validation set. | GENECAST | [131] | |
| Plasma | lung, breast, colorectal, pancreatic, gastric, esophageal, liver, and ovarian | 598 cancer patients 302 healthy individuals | Targeted sequencing | Developed a cancer detection and TOO discrimination model based on 135 MCB. 66.3% sensitivity, 95.5% specificity, and AUC of 0.85 were obtained in the validation set. 75.4% accuracy for TOO discrimination. | [132] | ||
| Plasma | lung, breast, colorectal, and pancreatic | 101 cancer patients 71 healthy individuals | MSRE-qPCR | Developed a 10-marker panel for cancer detection and a 16-marker panel for TOO discrimination. 79% sensitivity, 90% specificity, and AUC of 0.89 were obtained for cancer detection. TOO discrimination accuracy was 80% for colorectal, 78% for lung, 75% for pancreatic, and 62% for breast cancer. | Signal-X (Universal Dx) | [133] | |
| Plasma | Lung, colorectal, bladder, and pancreatic | >1500 cancer patients >1800 healthy individuals | 5mC enrichment and targeted sequencing | Developed a blood test based on cfDNA methylation signatures for early cancer detection and TOO discrimination. 90% and 87% sensitivity at 90% specificity for stage I/II colorectal and lung cancer detection. 73% and 52% sensitivities at 95% specificity for stage I/II pancreatic and bladder cancer detection. At 98% specificity, TOO accuracy was 99% for colorectal, 94% for lung, 88% for bladder, and 86% for pancreatic cancer. | LUNAR (Guardant Health) | [134] | |
| Plasma | lung, breast, colorectal, prostate, pancreatic, liver, and ovarian | 111 cancer patients 55 healthy individuals | Targeted sequencing | Developed Omni1, a targeted methylation sequencing panel comprising around 3000 cancer-specific hypermethylation markers for cancer early detection. 65% sensitivity for stage I cancers, 75% sensitivity for stage II cancers, and 89% specificity were obtained. | Omni1 (Avida Biomed) | [135] | |
| Plasma | lung, breast, colorectal, gastric, esophageal, and liver | 269 cancer patients 170 healthy individuals | Bisulfite sequencing | Developed Aurora, a blood test based on cancer specific cfDNA methylation signatures for detecting 6 major cancer types. AUCs of 0.90, 0.98, and 0.92 were obtained for lung, breast and colorectal cancer detection, respectively. | Aurora (AnchorDx) | [136] | |
| 203 cancer patients 206 healthy individuals | Improved to Aurora 2.0, a targeted methylation sequencing assay. AUCs of 0.94 and 0.935 were obtained for gastric and esophageal cancer detection, respectively. AUCs of 0.973, 0.962, and 0.92 were obtained for lung, breast, and colorectal cancer detection, respectively. | [137] | |||||
| 1000 cancer patients 505 healthy individuals | AUCs of 0.973, 0.962 and 0.92, 0.94, and 0.935 were obtained for lung, breast, colorectal, gastric and esophageal cancer detection, respectively. At 99% specificity, 84%, 75%, 82%, 85%, and 78% sensitivity were obtained for lung, breast, colorectal, gastric, and esophageal cancer, respectively. | [138] | |||||
| Tissue Plasma | breast, colorectal, prostate, and lymphoma | 72 tumor and 31 normal tissues 100 cancer and 45 healthy plasmas | Electrochemical assays | Developed electrochemical and colorimetric assays that can detect methylation differences between cancer and healthy genomes based on the level of DNA adsorption on planar and colloidal gold surfaces. DNA adsorption levels could discriminate between cancer patients and healthy individuals with an AUC of 0.887 using an electrochemical assay. DNA adsorption levels could discriminate between cancer patients and healthy individuals with an AUC of 0.785 using a colorimetric assay. | -- | [65] | |
| Stool | colorectal and gastric | 105 cancer patients 113 healthy individuals | Hi-SA | Developed a method combining single-step sodium bisulfite modification and fluorescence PCR to measure RASSF2 and SFRP2 methylation status in fecal DNA. DNA recovery from feces showed an AUC of 0.78 for distinguishing cancer from non-advanced lesions (adenomas, polyps and healthy). Methylation levels showed an AUC of 0.78. A combination score showed the best AUC of 0.81. | -- | [139] | |
| DNA methylation and circulating proteins | Plasma Serum | lung, pancreatic, gastric, esophageal, liver, and ovarian | 180 cancer patients 257 healthy individuals | Multiplex PCR and LQAS | Developed a multi-analyte blood test based on 26 methylation markers and 5 circulating proteins combined machine learning algorithms for cancer detection. 83% sensitivity, 94% specificity, and AUC of 0.96 were obtained in the validation set. | Exact Sciences | [140] |
| 160 cancer patients 315 healthy individuals | 85% sensitivity, 95% specificity, and AUC of 0.96 were obtained in the validation set. | [141] | |||||
| DNA methylation and copy number variations (CNVs) | Plasma | lung, breast, hepatocellular, nasopharyngeal, smooth muscle sarcoma, and neuroendocrine tumor | 46 cancer patients 32 healthy individuals | Bisulfite sequencing | Performed bisulfite sequencing to analyze genome-wide hypomethylation combined with copy number alterations in cfDNA and developed algorithms for cancer detection. If a sample was positive if either hypomethylation or CNAs were observed, 85% sensitivity, and 88% specificity were obtained. If a sample was positive if both hypomethylation and CNAs were observed, 60% sensitivity, and 94% specificity were obtained. | -- | [142] |
| DNA methylation, fragmentation, CNVs and microbial composition | Plasma | lung, colon, gastric, and liver | 275 cancer patients 204 healthy individuals | cfMethyl-Seq | Developed CancerRadar, a test based on genome-wide methylation profiling of cfDNA combined with machine learning for cancer detection and TOO discrimination. 85.6% sensitivity and 99% specificity for cancer detection. 91.5% accuracy for TOO discrimination. | Cancer Radar (Early Diagnostics) | [76] |
| DNA hydroxymethylation | Plasma | lung, breast, colorectal, gastric, esophageal, and liver | 2241 cancer patients 2289 healthy individuals | 5hmC-Seal profiling | Used the 5hmC-Seal technology to profile genome-wide 5hmC in cfDNA and combined it with machine learning for cancer detection and TOO discrimination. 79.3% sensitivity and 95% specificity were obtained in training set. 67.6% sensitivity and 98.2% specificity were obtained in the testing set. 83.2% accuracy for TOO discrimination. | Epican Genetech | [67] |
| Plasma | lung, breast, prostate, and pancreatic | 188 cancer patients 180 healthy individuals | 5hmC sequencing | Developed a novel 5hmC enrichment technology coupled with sequencing and machine learning for cancer detection. AUCs of 0.89, 0.84, 0.95, and 0.83 were obtained for breast, lung, pancreatic and prostate cancer detection, respectively. | BlueStar Genomics | [69] | |
| Genetic variants | Plasma | lung, breast, colorectal, prostate, bladder, pancreatic, and liver | 260 cancer patients 415 healthy individuals | NGS | Developed DEEPGENTM, an assay based on NGS combined with machine learning for cancer detection. 57% sensitivity at 95% specificity, 43% sensitivity at 99% specificity, and AUC of 0.90 were obtained. | DEEPGEN (Quantgene) | [28] |
| Stool | colorectal, pancreatic, gastric, biliary, and oropharyngeal | 69 cancer patients 69 healthy individuals | Digital melt curve method | Identified target mutations in genes commonly mutated in gastrointestinal cancer by sequencing tumor tissues. Target mutation analysis in stool detected cancer with 68% sensitivity and 100% specificity. | -- | [24] | |
| Genetic variants and cfDNA fragmentation | Plasma | lung, breast, colorectal, GIST, ovarian, Hodgkin lymphoma, diffuse large B-cell lymphoma, and multiple myeloma | 558 cancer patients 367 healthy individuals | WGS | Developed GIPXplore, a method combining cfDNA whole-genome sequencing profiles with machine learning for cancer detection and TOO discrimination. 92% sensitivity, 98% specificity, and AUC of 0.99 were obtained for discriminating hematological cancers from healthy samples. 85% accuracy for TOO prediction. 55% sensitivity, 95% specificity, and AUC of 0.83 were obtained for discriminating solid cancers from healthy samples. 69% accuracy for TOO prediction. | -- | [143] |
| Plasma | 17 tumor types | 200 cancer patients 65 healthy individuals | WGS | Analysis of mutations in size-selected cfDNA fragments improved diagnostic capacity. Combined fragmentation and mutation analysis provided an AUC > 0.99 compared to AUC <0.80 without using fragmentation features. | -- | [75] | |
| cfDNA fragmentation | Plasma | Lung, colorectal, and liver | 971 cancer patients 243 healthy individuals | WGS | Used cfDNA fragmentation profiles combined with machine learning for cancer early detection and TOO discrimination. 95.5% sensitivity, 95% specificity, and AUC of 0.983 were obtained. 93.1% accuracy for TOO prediction. | -- | [72] |
| Plasma | lung, breast, colorectal, pancreatic, gastric, bile duct, and ovarian | 236 cancer patients 245 healthy individuals | WGS | Developed DELFI, a test based on cfDNA fragmentation patterns combined with machine learning for cancer detection and TOO discrimination. 73% sensitivity, 98% specificity, and AUC of 0.94 were obtained for discriminating cancer from healthy samples. 61% accuracy for TOO prediction. Combining DELFI with mutant ctDNA, sensitivity for cancer detection increased to 91%, and TOO accuracy increased to 75%. | DELFI (Delfi Diagnostics) | [74] | |
| Circulating proteins and cfDNA mutations | Plasma | lung, breast, colorectal, pancreas, gastric, liver, esophageal, and ovarian | 1005 cancer patients 812 healthy individuals | Targeted sequencing and Bead-based immunoassay | Developed CancerSEEK, a blood test based on cfDNA mutations on 16 genes and 8 circulating proteins combined with machine learning for cancer detection and TOO discrimination. 62% sensitivity, 99% specificity, and AUC of 0.91 were obtained for discriminating cancer from healthy samples. 63% accuracy for TOO prediction. | CancerSEEK (Exact Sciences) | [29] |
| -- | 9911 women not previously known to have cancer | Evaluated the feasibility of CancerSEEK testing combined with PET-CT to detect cancer in a prospective cohort. The blood test was considered positive for 134 participants. 127 were further evaluated by PET. 64 showed imaging concerning for cancer. 26 were proven to have cancer by biopsy or other method. 27.1% sensitivity, 98.9% specificity, and 19.4% PPV were obtained for blood testing alone. 15.6% sensitivity, 99.6% specificity, and 28.3% PPV were obtained for blood testing combined with PET. | [30] | ||||
| Circulating Hsp90α | Plasma | lung, breast, colorectal, stomach, liver, pancreatic, esophageal, and lymphoma | 661 cancer patients 308 non-cancer patients 331 healthy individuals | ELISA | Hsp90α levels in plasma discriminated cancer from non-cancer controls (healthy + at-risk). AUC of 0.893, 81.72% sensitivity, and 81.03% specificity were obtained in the validation set. | -- | [144] |
| Gene expression | Whole blood | lung, breast, colorectal, pancreatic, hepatobiliary, and glioblastoma | 228 cancer patients 55 healthy individuals | RNA sequencing | Identified 2246 differentially expressed mRNAs in tumor-educated-platelets (TEPs). 1072 mRNAs were selected for developing a machine learning classifier for multi-cancer detection and TOO prediction. 97% sensitivity, 94% specificity, and 96% accuracy were obtained in the validation set. 71% accuracy for TOO prediction. | thromboDx BV | [86] |
| Bone marrow | leukemias, myelodysplastic syndrome, myeloproliferative neoplasm, and lymphoma | 136 cancer patients | RNA sequencing | Developed RANKING, a machine learning algorithm applied to RNA-seq data for the identification of hematological cancers. Accuracy of 100% for acute myelocytic leukemia and acute lymphocytic leukemia classification. | -- | [145] | |
| Whole blood | breast, rectum, colon, esophagus, stomach, thyroid, and uterus | 45 cancer patients 30 healthy individuals | RNA sequencing | Developed a machine learning classifier that uses RNA-seq data for cancer detection. Identified 900 differentially expressed genes that were used for constructing the classifier. 0.77 accuracy and 0.72 precision were obtained in the testing set. Another classifier based only on very long intergenic non-coding RNAs (vlincRNAs) outperformed the previous with 0.86 accuracy and precision. vlincRNAs demonstrated superior performance compared with mRNAs for cancer status identification. | -- | [80] | |
| Whole blood | 22 tumor types | 500 cancer patients 500 non-cancer patients | qRT-PCR | Developed the HrC scale, using OCT-4A expression in 120 samples (based on fold increase), for cancer detection and staging. 100% sensitivity, 100% specificity, and AUC of 1 were obtained. | -- | [87] | |
| lncRNA | Serum | 15 tumor types | 900 cancer patients 450 patients with benign conditions 450 healthy individuals | qRT-PCR | AUC values ranged from 0.826 to 0.966 for discriminating cancer patients from healthy individuals. AUC values ranged from 0.723 to 0.896 for discriminating cancer from benign conditions. LOC553103 expression was not able to discriminating cancer from benign conditions in pancreatic, ovarian and thyroid cancer. | -- | [81] |
| Serum | 12 tumor types | 360 cancer patients 360 patients with benign conditions 360 healthy individuals | qRT-PCR | AUC values ranged from 0.833 to 0.967 for discriminating cancer patients from healthy individuals. AUC values ranged from 0.7 to 0.81 for discriminating cancer from benign conditions. BLACAT1 expression was not able to discriminating cancer from benign conditions in breast, ovarian, prostate, and nasopharyngeal cancer. | -- | [82] | |
| microRNA | Serum | 14 tumor types | 112 cancer patients 48 patients with benign conditions 8 healthy individuals | qRT-PCR | Higher miR-93 expression was observed for all cancers compared to healthy controls, except for colorectal, bladder, gastric, renal, cervical, and ovarian cancer. AUC values ranged from 0.86 to 1.00, sensitivities from 63% to 100% and specificities from 81% to 100% for discriminating cancer patients from healthy individuals. | -- | [83] |
| Serum | 13 tumor types | 254 cancer patients 27 healthy individuals | microRNA chip | miR-1307-3p levels showed 98% sensitivity, 85% specificity, and AUC of 0.98 for cancer detection in the validation set. | -- | [84] | |
| Epitope detection in monocytes (EDIM) | Whole blood | 17 tumor types | 240 cancer patients 117 healthy individuals | Flow cytometry | EDIM-TKTL1 test is based on the detection of activated macrophages that present the TKTL1 antigen intracellularly. 94% sensitivity, 81% specificity and AUC of 0.89 were obtained. | PanTumDetect® (Zyagnum AG) | [107] |
| oral squamous cell carcinoma, breast, and prostate | 213 cancer patients 74 healthy individuals | Combination of EDIM-TKTL1 and EDIM-Apo10 tests showed 95.8% sensitivity and 97.3% specificity for cancer detection. | [108] | ||||
| cholangiocellular, pancreatic and colorectal | 62 cancer patients 13 patients with inflammatory conditions 16 healthy individuals | Combination of EDIM-TKTL1 and EDIM-Apo10 tests showed 100% sensitivity, 96.2% specificity and an AUC of 0.9934 for cancer detection. A positive result was seen for 100% of all cancer patients, 0% of healthy individuals, and 7.7% of individuals with inflammation. | [109] | ||||
| Circulating ensembles of tumor-associated cells (C-ETACs) | Whole blood | 18 cancer types | 5509 cancer patients 10,625 healthy individuals | Immuno-staining | C-ETACs were detected in 4944 out of 5509 cancer patients as well as in 255 of the 8493 individuals with no abnormal findings in routine screening procedures. This reflects an 89.8% sensitivity and 97% specificity. C-ETACs were detected in 137 out of 2132 asymptomatic individuals with abnormal findings in routine screening procedures. Assuming that cancer will not clinically manifest in none of the asymptomatic individuals positive for C-ETACs results in a maximum false-positive rate of 3.7%. | -- | [94] |
| Whole blood | 27 cancer types | 9416 cancer patients 6725 individuals with suspected cancer 13,919 healthy individuals | Immunocytochemistry | Additional organ-specific markers were profiled aiming to predict TOO. C-ETACs were detected in 91.8% of the 9416 cancer patients. Of the 6725 symptomatic individuals, 6025 were diagnosed with cancer and C-ETACs were detected in 92.6% of these. This resulted in a sensitivity of 92.1%. C-ETACs were undetectable in 13,408 of the 13,919 healthy individuals, resulting in a specificity of 96.3%. 93.1% accuracy for TOO prediction. | -- | [95] | |
| Circulating tumor cells (CTCs) | Whole blood | lung, colorectal, gastric, liver, and esophageal | 174 cancer patients 32 non-cancer patients 25 healthy individuals | Magnetic enrichment and immunofluorescence | CTCs count in cancer patients was significantly higher compared to non-cancer patients with high-risk conditions and healthy individuals (p < 0.001). The average CTCs count was 7.3 for cancer patients, 2.4 for non-cancer patients, and 0.9 for healthy individuals. CTCs count superior to 5 could be indicative of cancer status. | -- | [92] |
| Extracellular vesicles (EVs) | Plasma | breast, lung, acute myelocytic leukemia, and acute lymphocytic leukemia | 53 cancer patients 15 healthy individuals | Digital Profiling of Proteins on Individual EV (DPPIE) | Developed an ultrasensitive assay of digital profiling of proteins on individual EV (DPPIE), based on DNA aptamer recognition of specific EV proteins and rolling circle amplification reactions, that produce fluorescent signals on each single EV. DPPIE showed an AUC of 1.0, with specificity and sensitivity of 100% for carcinomas. | -- | [104] |
| Serum | lung, breast, prostate, liver, ovarian, and lymphoma | 145 cancer patients 27 healthy individuals | Thermophoretic aptasensor (TAS) | Developed TAS, an assay based on DNA aptamer recognition of 7 EV proteins and thermophoretic enrichment for cancer detection and TOO discrimination. 95% sensitivity, 100% specificity were obtained for cancer detection and 68% accuracy for TOO discrimination in the validation set. | -- | [105] | |
| Plasma | pancreatic, bladder, and ovarian | 139 cancer patients 184 healthy individuals | Verita™ and bead-based immunoassay | Developed an EV-based blood test combining alternating current electrokinetics (Verita™ System) for EVs isolation, immunoassays for protein quantification, and machine learning algorithms for early cancer detection. 71.2% sensitivity, 99.5% specificity, and AUC of 0.95 were obtained for discriminating cancer from healthy samples. | -- | [101] | |
| Plasma | 16 cancer types | 77 cancer patients 43 healthy individuals | Mass spectrometry | Analysis of tumor-specific extracellular vesicles and particles (EVP) proteomes combined with machine learning allowed cancer detection and TOO discrimination. Based on a 47-protein panel, 95% sensitivity and 90% specificity were obtained in the testing set. Based on all 372 tumor-related proteins, 100% sensitivity and 90% specificity were obtained. 30 protein panel discriminated TOO with very high accuracy. | -- | [103] | |
| Serum | 15 cancer types | 133 cancer patients 45 healthy individuals | qRT-PCR | Exossomal hTERT expression levels detected cancer with 62% sensitivity and 100% specificity. | -- | [100] | |
| Glycosaminoglycans | Plasma Urine | 14 cancer types | 753 plasma samples (460 cancers and 293 healthy) 559 urine samples (219 cancers and 340 healthy) | Mass spectrometry | Measured the levels of glycosaminoglycans in plasma and urine samples and combined it with machine learning for cancer detection. AUC of 0.78 was obtained in the validation set for discriminating 5 cancer types from healthy individuals using urine glycosaminoglycans. AUC of 0.84 was obtained in the validation set for discriminating 14 cancer types from healthy individuals using plasma glycosaminoglycans. | GAGome (Elypta) | [114] |
| Metabolites | Serum | lung, colorectal, pancreatic, gastric, liver, and thyroid | 950 cancer patients 233 healthy individuals | Mass spectrometry | Developed a laser desorption/ionization mass spectrometry-based liquid biopsy for multi-cancer detection and classification (MNALCI). MNALCI showed 93% sensitivity and 91% specificity for cancer detection in the internal validation cohort and 84% sensitivity and specificity in the external validation cohort. 92% accuracy for TOO discrimination in the internal validation cohort and 85% in the external cohort. | -- | [112] |
| Serum | breast, endometrial, cervical, and ovarian | 1119 cancer patients 250 healthy individuals | Mass spectrometry | Developed a method combining untargeted serum metabolomics with machine learning to identify metabolite signatures that allow early stages cancer detection. 98% sensitivity, 98.3% specificity, and 98% accuracy were obtained. TOO discrimination with 94.4% accuracy for breast, 91.6% for endometrial, 87.6% for cervical, and 92% for ovarian cancer. | -- | [113] | |
| Plasma denaturation profiles | Plasma | glioma but applicable to any cancer | 84 cancer patients 63 healthy individuals | Differential scanning fluorimetry | Applied nanoDSF, a differential scanning fluorimetry method for analyzing protein denaturation profiles, to plasma samples and combined it with a machine learning algorithm for distinguish the denaturation profiles of cancer patients. All 5 machine learning algorithms showed accuracies above 87%. Neural Networks (NN) algorithm performed the best, showing 92% sensitivity, 93% specificity and 92.5% accuracy. | -- | [146] |
| Metallobalance | Serum | breast, colorectal, prostate, pancreatic, gastric, liver, bile duct, thyroid, ovarian, cervical, and endometrial | 1856 cancer patients 5327 healthy individuals | Mass spectrometry | Applied a mass spectrometry-based technology to evaluate the serum profile of 17 elements as a cancer detection tool. AUC of 0.830 for discriminating cancer patients from healthy individuals. Classical markers (CEA, CA19-9, CA125, PSA) alone could not discriminating cancer patients from healthy individuals. However, for individuals with a normal CEA reading, the levels of Na, K, Cu, Fe Co, and Mo displayed differences in cancer over healthy samples, and the same applied to the other classical markers. | -- | [116] |
| Serum spectral profile | Serum | lung, breast, colorectal, prostate, pancreatic, renal, ovarian, and brain | 1543 cancer patients 460 symptomatic non-cancer patients 91 healthy individuals | Infrared spectroscopy | Developed Dxcover®, an infrared spectroscopy-based blood test for the early detection of cancer and TOO discrimination. 90% sensitivity with 61% specificity (adjusted for higher sensitivity), 56% sensitivity with 91% specificity (adjusted for higher specificity), and AUC of 0.86 were obtained for cancer detection. AUC values ranged from 0.74 to 0.91 for TOO discrimination. | Dxcover® | [117] |
| Tumor- activatable minicircles | Whole blood | Applicable to any cancer | -- | Luminescence measurement in the blood | Developed engineered non-viral vectors (minicircles) by coupling SEAP expression to activation of the Survinin promoter, resulting in luminescence production when tumor cells uptake the vectors. Minicircles were injected into tumor-bearing and control mice and SEAP was measured in the blood. AUC of 0.918 was obtained for discriminating cancer from healthy mice. | -- | [119] |
| Engineered macrophages | Whole blood | Applicable to any cancer | -- | Luminescence measurement in the blood | Developed engineered macrophages by coupling luciferase expression to activation of the Arginase-1 promoter, resulting in luminescence production when macrophages adopt an M2 tumor-associated phenotype. Engineered macrophages were injected into tumor-bearing and control mice and luciferase was measured in the blood. 100% sensitivity and specificity were obtained for discriminating cancer from healthy mice. | -- | [120] |
3. Bioinformatics Meets Cancer Detection: Finding the Right Targets and Improving Biomarker Performance
| Biomarker | Database | Tumor Types | Main Findings | Ref. |
|---|---|---|---|---|
| DNA methylation | TCGA GEO | 26 tumor types | Identified 7 informative CpG sites capable of discriminating tumor from normal samples. AUC of 0.986 was obtained in the training set. Validation using GEO datasets of breast, colorectal cancer, and prostate cancer obtained AUCs of 0.97, 0.95, and 0.93, respectively. Validation set comprising the remaining cancer types obtained an AUC of 0.94. Identified 12 CpG sites capable of discriminating each tumor type with an AUC of 0.98. | [168] |
| TCGA GEO | 27 tumor types | Identified 12 CpG markers and 13 promoter markers and constructed diagnostic models by deep learning. CpG marker model achieved 98.1% sensitivity, 99.5% specificity, and 98.5% accuracy on training set, while achieving 92.8% sensitivity, 90.1% specificity, and 92.4% accuracy on testing set. Promoter marker model achieved 96.9% sensitivity, 99.9% specificity, and 97.8% accuracy on testing set, while achieving 89.8% sensitivity, 81.1% specificity, and 88.3% accuracy on testing set. | [156] | |
| TCGA GEO | 27 tumor types | Developed the CAncer Cell-of-Origin (CACO) methylation panel comprising 2 572 cytosines that are significantly hypermethylated in tumor tissues compared with normal tissues and healthy blood samples. CACO panel identified TOO with AUC ranging from 0.856 to 0.998 in discovery cohort and 0.854 to 0.998 in validation cohort. CACO panel could identify TOO in liquid biopsies and unknown primary carcinoma samples. | [169] | |
| TCGA | 14 tumor types | Combined genome-wide differential methylation profiling with machine learning to detect cancer and discriminate TOO. Set of 4 CpGs detected cancer with an AUC of 0.95 in the discovery set and an AUC of 0.96 in the validation set. Set of 20 CpGs discriminated TOO with AUC values ranging from 0.87 to 0.99; 12 out of 14 cancer types were discriminated with sensitivities and specificities above 90%. | [157] | |
| TCGA GEO | 3 tumor types | Developed a machine learning algorithm to detect and discriminate TOO in 3 urological cancers (prostate, bladder, and kidney) using 128 methylation markers. 99.1% accuracy in training set; 97.6% accuracy in 2 independent validation sets. | [170] | |
| TCGA GEO | 33 tumor types | Identified a 12-market set that can detect all 33 cancers in TCGA database with AUCs > 0.84. Identified sets of 6 markers that can discriminate TOO with AUCs ranging from 0.969 to 1. | [171] | |
| TCGA | 12 tumor types | While performing genome-wide methylation analysis for pancreatic cancer biomarker discovery, identified SST as hypermethylated in pancreatic tumors compared to normal tissue and showed an AUC of 0.89 for pancreatic cancer detection in cfDNA. SST methylation and expression in 11 other cancer types showed significant hypermethylation and downregulation of expression when compared to the respective normal tissue (p < 0.0001). | [154] | |
| TCGA GEO | 14 tumor types | Identified 6 CpGs in the GSDME gene differentially methylated between tumor and normal samples and used them for developing a machine learning algorithm for cancer identification. 98.8% sensitivity, 94.2% specificity, and AUC of 0.86 in the training set. AUC of 0.85 in validation set. 6 CpG model showed TOO discrimination capacity. | [172] | |
| DNA methylation, gene expression and somatic mutations | TCGA | 13 tumor types | Developed EAGLING, a model that expands the Illumina 450K array data to cover about 30% of CpGs in the genome. Used this expanded methylation data combined with gene expression and somatic mutation data to identify genes with differential patterns in various cancer types (triple-evidenced genes). Developed a machine learning algorithm, using the identified triple-evidenced genes, for cancer detection. AUC of 0.85 was obtained; 95.3% accuracy was obtained for TOO discrimination. TNXB, RRM2, CELSR3, SLC16A3, FANCI, MMP9, MMP11, SIK1, and TRIM59 showed great capacity for cancer diagnosis. | [158] |
| Gene mutations | TCGA | 5 tumor types | Based on a tumor’s mutations and their respective GO terms and KEGG pathways, a machine learning algorithm was developed for TOO discrimination; 62% accuracy was obtained for discriminating TOO in 5 cancer types. | [173] |
| Gene expression | GEO | 10 tumor types | Developed a deep learning classifier for multi-cancer diagnosis using transcriptomic data termed DeepDCancer. 90% accuracy was obtained for distinguishing cancer from normal samples, while accuracies ranged from 86 to 98% (94% average) for discriminating individual cancer types. 96% accuracy was obtained for distinguishing cancer from normal samples using an improved classifier, DeepDCancer. | [159] |
| TCGA | 40 tumor types | Developed SCOPE, a machine learning algorithm that uses RNA-seq data for TOO prediction. SCOPE achieved 97% accuracy in training set and 99% in testing set. SCOPE showed the ability to identify TOO in cancers of unknown primary. | [174] | |
| TCGA | 11 tumor types | Developed GeneCT, a deep learning algorithm that uses RNA-seq data for cancer identification and TOO prediction. Known cancer-related genes were used for cancer status identification and transcription factors for TOO prediction. 100% sensitivity and 99.6% specificity for cancer identification in training set. 96.0% sensitivity and 96.1 specificity for cancer identification in validation set. 99.6% accuracy for TOO prediction in training set and 98.6% in validation set. | [160] | |
| TCGA | 33 tumor types | 5 machine learning algorithms were compared on their performance for cancer classification. Linear support vector machine (SVM) showed the best accuracy of 95.8%. | [175] | |
| TCGA | 5 tumor types | Developed a deep learning model for TOO discrimination using RNA-seq data among the 5 most common cancers in women. LASSO feature selection reduced all 14,899 genes to only 173 relevant genes. 99.45% accuracy was obtained for discriminating TOO in 5 cancer types. | [176] | |
| TCGA GTEx | 28 tumor types | Identified differentially expressed genes (DEGs) that were shared in various cancer types and constructed a diagnostic model using 10 upregulated DEGs (CCNA2, CDK1, CCNB1, CDC20, TOP2A, BUB1B, AURKB, NCAPG, CDC45, and TTK). AUC of 0.894 was obtained for discriminating cancer from normal samples. | [177] | |
| TCGA | 15 tumor types | MMP11 and MMP13 expression was significantly higher in most cancer types compared to tissue matched controls. Each cancer type featured at least one MMP with an AUC greater than 0.9, except prostate cancer; 6 cancer types featured 4 or more MMPs with AUC > 0.9. If serum detection is possible, upregulated MMP11 or MMP13 could serve as a multi-cancer biomarker. | [178] | |
| TCGA | 9 tumor types | Hsp90α expression was significantly higher in 8 cancers compared to tissue matched controls, except for prostate cancer which displayed significant lower expression. AUC values ranged from 0.63 to 0.94 for individual cancer types. | [155] | |
| TCGA GTEx | 33 tumor types | Claudin-6 was significantly overexpressed in 20 cancer types. AUC > 0.7 were obtained for detecting 15 cancer types. AUC > 0.9 were obtained for detecting acute myeloid leukemia, testicular, ovarian, and uterine cancer. | [179] | |
| TCGA GTEx | 33 tumor types | YTHDC2 expression was significantly downregulated in most cancers compared with normal tissues. YTHDC2 displayed high diagnostic value (AUC > 0.90) for 7 cancer types and moderate diagnostic value (AUC > 0.723) in 8 cancer types. | [180] | |
| TCGA GTEx | 24 tumor types | PAFAH1B expression was significantly upregulated in most cancers compared with normal tissues. PAFAH1B displayed high diagnostic value (AUC > 0.90) for 15 cancer types and moderate diagnostic value (AUC > 0.75) in 9 cancer types. | [181] | |
| TCGA GTEx | 20 tumor types | SHC1 expression was significantly upregulated in most cancers compared with normal tissues. SHC1 displayed high diagnostic value (AUC > 0.90) for 4 cancer types and moderate diagnostic value (AUC > 0.70) in 16 cancer types. Strong diagnostic capability for KICH (AUC = 0.92), LIHC (AUC = 0.95), and PAAD (AUC = 0.95). | [182] | |
| TCGA GTEx | 29 tumor types | GPC2 expression was significantly upregulated in 12 early-stage cancers compared with normal tissues. GPC2 displayed high diagnostic value (AUC > 0.90) for 6 cancer types, moderate diagnostic value (AUC > 0.70) in 16 cancer types, and low diagnostic value (AUC > 0.50) in 7 cancer types. | [183] | |
| ncRNA | TCGA | 26 tumor types | Developed algorithms to remove all the factor effects (genetic, epidemiological, and environmental variables) from big data and revealed 56 ncRNAs as universal markers for 26 cancer types. Used these 56 ncRNAs as markers and employed machine learning algorithms to discriminating cancer from normal samples and identify TOO. AUC of 0.963 for discriminating cancer from normal samples. AUC values ranged from 0.99 to 1 for detecting individual cancer types. 82.15% accuracy for discriminating TOO. | [161] |
| lncRNA | TCGA GEO | 9 tumor types | CRNDE expression was significantly higher in 9 cancers compared to tissue matched controls. AUC values ranged from 0.855 to 0.984, sensitivities from 70 to 97% and specificities from 75 to 100%. Meta-analysis from 6 studies showed a pooled sensitivity of 77%, specificity of 90%, and AUC of 0.87. | [184] |
| TCGA GEO | 12 tumor types | Identified 6 differently expressed long intergenic noncoding RNAs (lincRNAs) (PCAN-1 to PCAN-6) and applied machine learning algorithms for cancer detection using 5 of them. AUC of 0.947 was obtained in the training set. AUC of 0.947, 81.7% sensitivity, and 97% specificity were obtained in the testing set. | [185] | |
| TCGA GEO | 8 tumor types | Using RNA-seq and methylation data from TCGA, identified 9 epigenetically regulated lncRNAs (lncRNAs regulated by methylation) that can predict cancer. Developed a score based on expression and methylation data of these 9 genes (PVT1, PSMD5-AS1, FAM83H-AS1, MIR4458HG, HCP5, GAS5, CTD2201E18.3, HCG11, and AC016747.3) that was applied to all cancer and normal samples. AUC values ranged from 0.741 to 0.992 for detecting 8 cancer types. AUC values ranged from 0.712 to 1 in an independent validation set. | [186] | |
| TCGA | 33 tumor types | SNHG3 expression was significantly upregulated in 16 (out of 33) cancers compared with normal tissues. 72% sensitivity, 87% specificity, and an AUC of 0.89 was observed for cancer detection. | [187] | |
| microRNA | TCGA | 21 tumor types | Used machine learning algorithms to develop a multi-cancer diagnostic method based on microRNA expression. Support vector machine (SVM) classifier was chosen, since it provided the highest accuracy of 97.2%, sensitivities over 90%, and specificities of 100% for most cancers. | [188] |
| GEO | 11 tumor types | Developed a computational pipeline for extracellular microRNA-based cancer detection and classification. All classifiers showed accuracies over 95%. SVM classifier performed the best, with 99% accuracy. Identified a 10 microRNA-signature capable of TOO discrimination. | [162] | |
| TCGA | 4 tumor types | Identified 3 differentially expressed miRNAs (miR-552, miR-490, and miR-133a-2) with diagnostic potential for digestive tract cancers. 3 miRNAs showed high diagnostic value in rectal cancer (AUC > 0.961) and moderate diagnostic value in esophageal (AUC > 0.826), gastric (AUC > 0.798), and colon cancer (AUC > 0.797). | [189] | |
| GEO | 12 tumor types | Developed a serum-based 4-microRNA diagnostic model (has-miR-5100, has-miR-1343-3hashsa-miR-1290hasnd hsa-miR-4787-3p) for cancer early detection. Sensitivities ranging from 83.2 to 100% for biliary tract, bladder, colorectal, esophageal, gastric, glioma, liver, pancreatic, and prostate cancers were obtained, while reasonable sensitivities of 68.2 and 72.0% for ovarian cancer and sarcoma, respectively, with 99.3% specificity. | [190] | |
| GEO | 12 tumor types | Developed a m6A target miRNAs serum signature, based on 18 microRNAs combined with machine learning, for cancer detection. 93.9% sensitivity, 93.3% specificity, and AUC of 0.979 in training set. 94.2% sensitivity, 91.6% specificity, and AUC of 0.976 in internal validation set. 90.8% sensitivity, 84.7% specificity, and AUC of 0.936 in external validation set. | [191] | |
| Progenitorness score | TCGA GEO | 17 tumor types | Selected 77 progenitor genes and formulated a score to quantify the progenitorness of a sample using its expression profile data. Tumor samples showed significantly higher progenitorness scores than normal tissues for all cancer types, with AUC ranging from 0.746 to 1.000. For the majority of cancers, AUC was above 0.90. | [192] |
4. What Is Stopping MCED Tests from Moving into Clinical Application?
| Trial ID | Trial Name | MCED Test | Sponsor | Status (as of July 2022) |
|---|---|---|---|---|
| NCT02889978 | CCGA | Galleri | GRAIL, LLC | Active, not recruiting |
| NCT03085888 | STRIVE | Galleri | GRAIL, LLC | Active, not recruiting |
| NCT03934866 | SUMMIT | Galleri | University College London and GRAIL | Active, not recruiting |
| NCT04241796 | PATHFINDER | Galleri | GRAIL, LLC | Active, not recruiting |
| NCT05155605 | PATHFINDER 2 | Galleri | GRAIL, LLC | Recruiting |
| NCT05205967 | REFLECTION | Galleri | GRAIL, LLC | Recruiting |
| NCT05235009 | LEV87A | GAGome | Elypta | Recruiting |
| NCT05295017 | LEV93A | GAGome | Elypta | Recruiting |
| NCT05227534 | PREVENT | OverC | Guangzhou Burning Rock Dx | Recruiting |
| NCT04825834 | DELFI-L101 | DELFI | Delfi Diagnostics Inc. | Recruiting |
| NCT04213326 | ASCEND | CancerSEEK | Exact Sciences | Completed |
| NCT03756597 | PAN | ReCIVA | Owlstone Ltd. | Unknown |
| NCT03517332 | -- | DEEPGEN | Quantgene Inc. | Unknown |
| NCT03967652 | -- | Na-nose | Anhui Medical University | Not yet recruiting |
| NCT05366881 | CAMPERR | -- | Adela, Inc. | Recruiting |
| NCT05254834 | Vallania | -- | Freenome Holdings Inc. | Recruiting |
| NCT04972201 | PROMISE | -- | Chinese Academy of Medical Sciences (and Burning Rock Dx) | Recruiting |
| NCT04822792 | PRESCIENT | -- | Chinese Academy of Medical Sciences (and Burning Rock Dx) | Recruiting |
| NCT04820868 | THUNDER | -- | Shanghai Zhongshan Hospital (and Burning Rock Dx) | Recruiting |
| NCT04817306 | PREDICT | -- | Shanghai Zhongshan Hospital (and Burning Rock Dx) | Recruiting |
| NCT05227261 | K-DETEK | -- | Gene Solutions | Recruiting |
| NCT05159544 | FuSion | -- | Singlera Genomics Inc. | Recruiting |
| NCT04405557 | PREDICT | -- | Geneplus-Beijing Co. | Active, not recruiting |
| NCT02662621 | EXODIAG | -- | Centre Georges Francois Leclerc | Completed |
| NCT04197414 | -- | -- | Yonsei University | Recruiting |
| NCT03951428 | -- | -- | LifeStory Health Inc. | Unknown |
| NCT03869814 | -- | -- | Bluestar Genomics Inc. | Active, not recruiting |
| NCT02612350 | -- | -- | Pathway Genomics | Completed |
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Clarke, C.A.; Hubbell, E.; Kurian, A.W.; Colditz, G.A.; Hartman, A.R.; Gomez, S.L. Projected Reductions in Absolute Cancer-Related Deaths from Diagnosing Cancers Before Metastasis, 2006-2015. Cancer Epidemiol. Biomark. Prev 2020, 29, 895–902. [Google Scholar] [CrossRef] [Green Version]
- Smith, R.A.; Oeffinger, K.C. The Importance of Cancer Screening. Med. Clin. N. Am. 2020, 104, 919–938. [Google Scholar] [CrossRef] [PubMed]
- WHO. Guide to Cancer Early Aiagnosis; World Health Organization: Geneva, Switzerland, 2017. [Google Scholar]
- Barsouk, A.; Saginala, K.; Aluru, J.S.; Rawla, P.; Barsouk, A. US Cancer Screening Recommendations: Developments and the Impact of COVID-19. Med. Sci. 2022, 10, 16. [Google Scholar] [CrossRef] [PubMed]
- Armaroli, P.; Villain, P.; Suonio, E.; Almonte, M.; Anttila, A.; Atkin, W.S.; Dean, P.B.; de Koning, H.J.; Dillner, L.; Herrero, R.; et al. European Code against Cancer, 4th Edition: Cancer screening. Cancer Epidemiol. 2015, 39, S139–S152. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grossman, D.C.; Curry, S.J.; Owens, D.K.; Bibbins-Domingo, K.; Caughey, A.B.; Davidson, K.W.; Doubeni, C.A.; Ebell, M.; Epling, J.W., Jr.; Kemper, A.R.; et al. Screening for Prostate Cancer: US Preventive Services Task Force Recommendation Statement. JAMA 2018, 319, 1901–1913. [Google Scholar] [CrossRef]
- Wu, G.X.; Raz, D.J. Lung Cancer Screening. Cancer Treat Res 2016, 170, 1–23. [Google Scholar] [CrossRef]
- Marmot, M.G.; Altman, D.G.; Cameron, D.A.; Dewar, J.A.; Thompson, S.G.; Wilcox, M. The benefits and harms of breast cancer screening: An independent review. Lancet 2012, 380, 1778–1786. [Google Scholar] [CrossRef] [Green Version]
- Force, U.P.S.T. Screening for Cervical Cancer: US Preventive Services Task Force Recommendation Statement. JAMA 2018, 320, 674–686. [Google Scholar] [CrossRef] [Green Version]
- Barry, M.J.; Simmons, L.H. Prevention of Prostate Cancer Morbidity and Mortality: Primary Prevention and Early Detection. Med. Clin. N. Am. 2017, 101, 787–806. [Google Scholar] [CrossRef]
- Geneve, N.; Kairys, D.; Bean, B.; Provost, T.; Mathew, R.; Taheri, N. Colorectal Cancer Screening. Prim. Care 2019, 46, 135–148. [Google Scholar] [CrossRef]
- Mannelli, C. Tissue vs Liquid Biopsies for Cancer Detection: Ethical Issues. J. Bioeth. Inq. 2019, 16, 551–557. [Google Scholar] [CrossRef] [PubMed]
- Poulet, G.; Massias, J.; Taly, V. Liquid Biopsy: General Concepts. Acta Cytol. 2019, 63, 449–455. [Google Scholar] [CrossRef] [PubMed]
- Marrugo-Ramírez, J.; Mir, M.; Samitier, J. Blood-Based Cancer Biomarkers in Liquid Biopsy: A Promising Non-Invasive Alternative to Tissue Biopsy. Int. J. Mol. Sci. 2018, 19, 2877. [Google Scholar] [CrossRef] [Green Version]
- Ignatiadis, M.; Sledge, G.W.; Jeffrey, S.S. Liquid biopsy enters the clinic—Implementation issues and future challenges. Nat. Rev. Clin. Oncol. 2021, 18, 297–312. [Google Scholar] [CrossRef]
- Lone, S.N.; Nisar, S.; Masoodi, T.; Singh, M.; Rizwan, A.; Hashem, S.; El-Rifai, W.; Bedognetti, D.; Batra, S.K.; Haris, M.; et al. Liquid biopsy: A step closer to transform diagnosis, prognosis and future of cancer treatments. Mol. Cancer 2022, 21, 79. [Google Scholar] [CrossRef]
- Bettegowda, C.; Sausen, M.; Leary, R.J.; Kinde, I.; Wang, Y.; Agrawal, N.; Bartlett, B.R.; Wang, H.; Luber, B.; Alani, R.M.; et al. Detection of circulating tumor DNA in early- and late-stage human malignancies. Sci. Transl. Med. 2014, 6, 224ra224. [Google Scholar] [CrossRef] [Green Version]
- Alix-Panabières, C.; Pantel, K. Liquid Biopsy: From Discovery to Clinical Application. Cancer Discov. 2021, 11, 858–873. [Google Scholar] [CrossRef] [PubMed]
- Ahlquist, D.A. Universal cancer screening: Revolutionary, rational, and realizable. NPJ Precis. Oncol. 2018, 2, 23. [Google Scholar] [CrossRef] [PubMed] [Green Version]
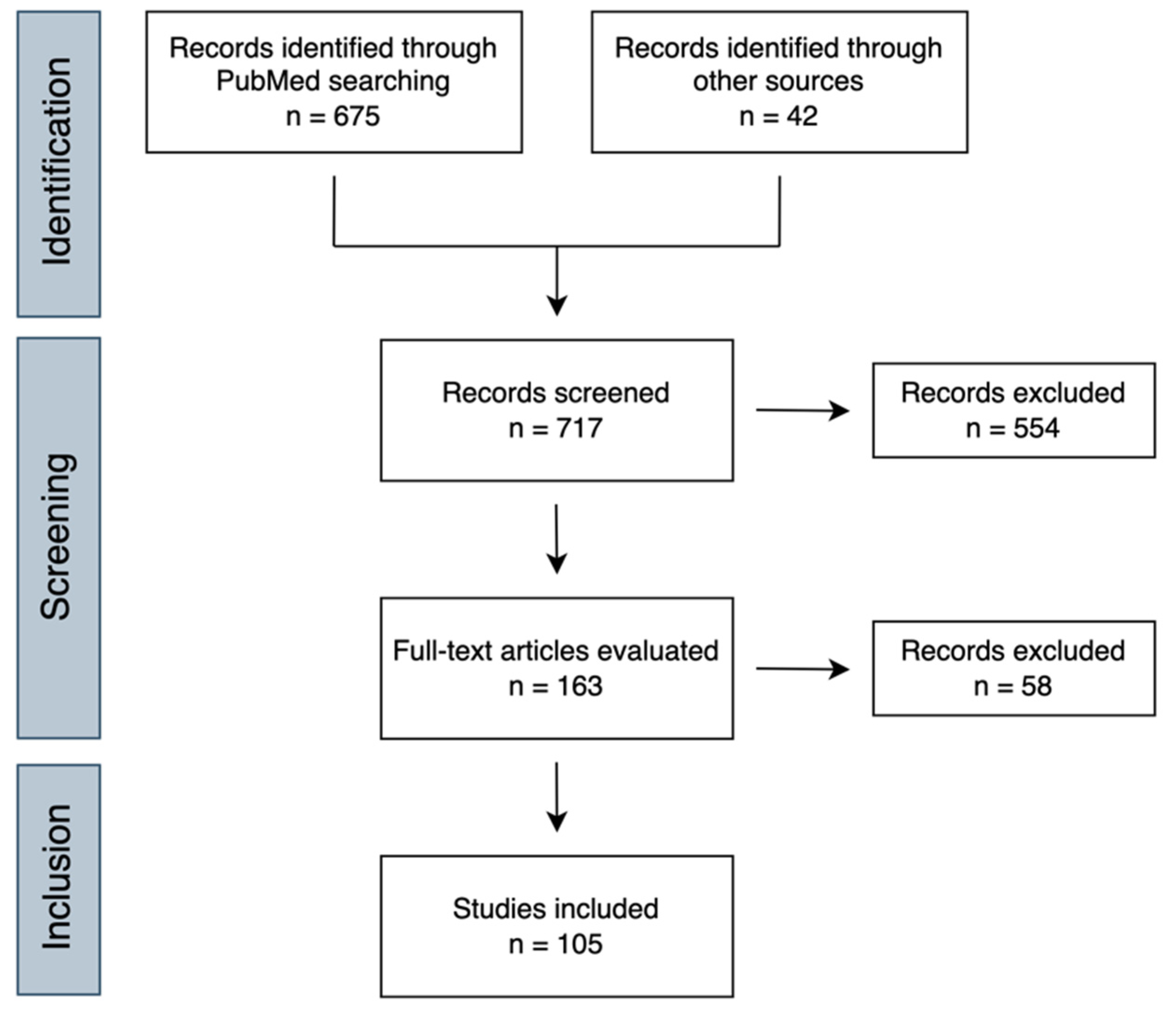
- Ouzzani, M.; Hammady, H.; Fedorowicz, Z.; Elmagarmid, A. Rayyan—A web and mobile app for systematic reviews. Syst. Rev. 2016, 5, 210. [Google Scholar] [CrossRef] [Green Version]
- Keller, L.; Belloum, Y.; Wikman, H.; Pantel, K. Clinical relevance of blood-based ctDNA analysis: Mutation detection and beyond. Br. J. Cancer 2021, 124, 345–358. [Google Scholar] [CrossRef]
- Siravegna, G.; Marsoni, S.; Siena, S.; Bardelli, A. Integrating liquid biopsies into the management of cancer. Nat. Rev. Clin. Oncol. 2017, 14, 531–548. [Google Scholar] [CrossRef] [PubMed]
- Zou, H.; Harrington, J.J.; Taylor, W.R.; Devens, M.E.; Cao, X.; Heigh, R.I.; Romero, Y.; Chari, S.T.; Petersen, G.M.; Roberts, L.R.; et al. T2036 Pan-Detection of Gastrointestinal Neoplasms By Stool DNA Testing: Establishment of Feasibility. Gastroenterology 2009, 136, A-625. [Google Scholar] [CrossRef]
- Yang, D.; Hillman, S.L.; Harris, A.M.; Sinicrope, P.S.; Devens, M.E.; Ahlquist, D.A. Patient perceptions of stool DNA testing for pan-digestive cancer screening: A survey questionnaire. World J. Gastroenterol. 2014, 20, 4972–4979. [Google Scholar] [CrossRef] [PubMed]
- Hermann, B.T.; Pfeil, S.; Groenke, N.; Schaible, S.; Kunze, R.; Ris, F.; Hagen, M.E.; Bhakdi, J. DEEPGEN(TM)-A Novel Variant Calling Assay for Low Frequency Variants. Genes 2021, 12, 507. [Google Scholar] [CrossRef] [PubMed]
- Quantgene Inc. DEEPGEN™ R&D Solution. Available online: https://www.quantgene.com/deepgen-research-solutions (accessed on 20 August 2022).
- Ris, F.; Hellan, M.; Douissard, J.; Nieva, J.J.; Triponez, F.; Woo, Y.; Geller, D.; Buchs, N.C.; Buehler, L.; Moenig, S.; et al. Blood-Based Multi-Cancer Detection Using a Novel Variant Calling Assay (DEEPGENTM): Early Clinical Results. Cancers 2021, 13, 4104. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J.D.; Li, L.; Wang, Y.; Thoburn, C.; Afsari, B.; Danilova, L.; Douville, C.; Javed, A.A.; Wong, F.; Mattox, A.; et al. Detection and localization of surgically resectable cancers with a multi-analyte blood test. Science 2018, 359, 926–930. [Google Scholar] [CrossRef] [Green Version]
- Lennon, A.M.; Buchanan, A.H.; Kinde, I.; Warren, A.; Honushefsky, A.; Cohain, A.T.; Ledbetter, D.H.; Sanfilippo, F.; Sheridan, K.; Rosica, D.; et al. Feasibility of blood testing combined with PET-CT to screen for cancer and guide intervention. Science 2020, 369, 6499. [Google Scholar] [CrossRef]
- van der Pol, Y.; Mouliere, F. Toward the Early Detection of Cancer by Decoding the Epigenetic and Environmental Fingerprints of Cell-Free DNA. Cancer Cell 2019, 36, 350–368. [Google Scholar] [CrossRef]
- Tempero, M. Pan-Cancer Screening: A Dream or a Nightmare. J. Natl. Compr. Canc. Netw. 2021, 19, 773. [Google Scholar] [CrossRef]
- Srivastava, S.; Hanash, S. Pan-Cancer Early Detection: Hype or Hope? Cancer Cell 2020, 38, 23–24. [Google Scholar] [CrossRef]
- Inbar-Feigenberg, M.; Choufani, S.; Butcher, D.T.; Roifman, M.; Weksberg, R. Basic concepts of epigenetics. Fertil. Steril. 2013, 99, 607–615. [Google Scholar] [CrossRef] [PubMed]
- Lokk, K.; Modhukur, V.; Rajashekar, B.; Märtens, K.; Mägi, R.; Kolde, R.; Koltšina, M.; Nilsson, T.K.; Vilo, J.; Salumets, A.; et al. DNA methylome profiling of human tissues identifies global and tissue-specific methylation patterns. Genome Biol. 2014, 15, 3248. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sun, K.; Jiang, P.; Chan, K.C.A.; Wong, J.; Cheng, Y.K.Y.; Liang, R.H.S.; Chan, W.-K.; Ma, E.S.K.; Chan, S.L.; Cheng, S.H.; et al. Plasma DNA tissue mapping by genome-wide methylation sequencing for noninvasive prenatal, cancer, and transplantation assessments. Proc. Natl. Acad. Sci. USA 2015, 112, E5503–E5512. [Google Scholar] [CrossRef] [Green Version]
- Guo, S.; Diep, D.; Plongthongkum, N.; Fung, H.-L.; Zhang, K.; Zhang, K. Identification of methylation haplotype blocks aids in deconvolution of heterogeneous tissue samples and tumor tissue-of-origin mapping from plasma DNA. Nat. Genet. 2017, 49, 635–642. [Google Scholar] [CrossRef] [PubMed]
- Jones, P.A.; Baylin, S.B. The fundamental role of epigenetic events in cancer. Nat. Rev. Genet. 2002, 3, 415–428. [Google Scholar] [CrossRef] [PubMed]
- Kulis, M.; Esteller, M. DNA methylation and cancer. Adv. Genet. 2010, 70, 27–56. [Google Scholar] [CrossRef]
- Baylin, S.B.; Jones, P.A. Epigenetic Determinants of Cancer. Cold Spring Harb. Perspect Biol. 2016, 8. [Google Scholar] [CrossRef] [Green Version]
- Constâncio, V.; Nunes, S.P.; Henrique, R.; Jerónimo, C. DNA Methylation-Based Testing in Liquid Biopsies as Detection and Prognostic Biomarkers for the Four Major Cancer Types. Cells 2020, 9, 624. [Google Scholar] [CrossRef] [Green Version]
- Miller, B.F.; Petrykowska, H.M.; Elnitski, L. Assessing ZNF154 methylation in patient plasma as a multicancer marker in liquid biopsies from colon, liver, ovarian and pancreatic cancer patients. Sci. Rep. 2021, 11, 221. [Google Scholar] [CrossRef]
- Nunes, S.P.; Moreira-Barbosa, C.; Salta, S.; Palma de Sousa, S.; Pousa, I.; Oliveira, J.; Soares, M.; Rego, L.; Dias, T.; Rodrigues, J.; et al. Cell-Free DNA Methylation of Selected Genes Allows for Early Detection of the Major Cancers in Women. Cancers 2018, 10, 357. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Constâncio, V.; Nunes, S.P.; Moreira-Barbosa, C.; Freitas, R.; Oliveira, J.; Pousa, I.; Oliveira, J.; Soares, M.; Dias, C.G.; Dias, T.; et al. Early detection of the major male cancer types in blood-based liquid biopsies using a DNA methylation panel. Clin. Epigenet. 2019, 11, 175. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kandimalla, R.; Xu, J.; Link, A.; Matsuyama, T.; Yamamura, K.; Parker, M.I.; Uetake, H.; Balaguer, F.; Borazanci, E.; Tsai, S.; et al. EpiPanGI Dx: A Cell-free DNA Methylation Fingerprint for the Early Detection of Gastrointestinal Cancers. Clin. Cancer Res. 2021, 27, 6135–6144. [Google Scholar] [CrossRef] [PubMed]
- Hao, X.; Luo, H.; Krawczyk, M.; Wei, W.; Wang, W.; Wang, J.; Flagg, K.; Hou, J.; Zhang, H.; Yi, S.; et al. DNA methylation markers for diagnosis and prognosis of common cancers. Proc. Natl. Acad. Sci. USA 2017, 114, 7414–7419. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- IvyGene Labs. The IvyGeneCORE Test. Available online: https://www.ivygenelabs.co.za/the-ivygenecore-test/ (accessed on 20 August 2022).
- Singlera Genomics. Singlera Genomics’ PanSeer Assay Technology. Available online: https://singleraoncology.com/technology/ (accessed on 20 August 2022).
- Chen, X.; Gole, J.; Gore, A.; He, Q.; Lu, M.; Min, J.; Yuan, Z.; Yang, X.; Jiang, Y.; Zhang, T.; et al. Non-invasive early detection of cancer four years before conventional diagnosis using a blood test. Nat. Commun. 2020, 11, 3475. [Google Scholar] [CrossRef]
- Sheridan, C. Grail to pour $1 billion into blood test to detect early cancer. Nat. Biotechnol. 2017, 35, 101–102. [Google Scholar] [CrossRef]
- Fiala, C.; Diamandis, E.P. Can Grail find the trail to early cancer detection? Clin. Chem. Lab. Med. 2019, 57, 403–406. [Google Scholar] [CrossRef]
- Klein, E.A.; Hubbell, E.; Maddala, T.; Aravanis, A.; Beausang, J.F.; Filippova, D.; Gross, S.; Jamshidi, A.; Kurtzman, K.; Shen, L.; et al. Development of a comprehensive cell-free DNA (cfDNA) assay for early detection of multiple tumor types: The Circulating Cell-free Genome Atlas (CCGA) study. J. Clin. Oncol. 2018, 36, 12021. [Google Scholar] [CrossRef] [Green Version]
- Liu, M.C.; Klein, E.; Hubbell, E.; Maddala, T.; Aravanis, A.M.; Beausang, J.F.; Filippova, D.; Gross, S.; Jamshidi, A.; Kurtzman, K.; et al. Plasma cell-free DNA (cfDNA) assays for early multi-cancer detection: The circulating cell-free genome atlas (CCGA) study. Ann. Oncol. 2018, 29, viii14. [Google Scholar] [CrossRef]
- Liu, M.C.; Oxnard, G.R.; Klein, E.A.; Swanton, C.; Seiden, M.V.; Liu, M.C.; Oxnard, G.R.; Klein, E.A.; Smith, D.; Richards, D.; et al. Sensitive and specific multi-cancer detection and localization using methylation signatures in cell-free DNA. Ann. Oncol. 2020, 31, 745–759. [Google Scholar] [CrossRef]
- Klein, E.A.; Richards, D.; Cohn, A.; Tummala, M.; Lapham, R.; Cosgrove, D.; Chung, G.; Clement, J.; Gao, J.; Hunkapiller, N.; et al. Clinical validation of a targeted methylation-based multi-cancer early detection test using an independent validation set. Ann. Oncol. 2021, 32, 1167–1177. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.; Dong, Z.; Hubbell, E.; Kurtzman, K.N.; Oxnard, G.R.; Venn, O.; Melton, C.; Clarke, C.A.; Shaknovich, R.; Ma, T.; et al. Prognostic Significance of Blood-Based Multi-cancer Detection in Plasma Cell-Free DNA. Clin. Cancer Res 2021, 27, 4221–4229. [Google Scholar] [CrossRef] [PubMed]
- GRAIL. The Galleri® Test. Available online: https://www.galleri.com/the-galleri-test/request-the-test (accessed on 2 September 2022).
- Nadauld, L.D.; McDonnell, C.H.; Beer, T.M.; Liu, M.C.; Klein, E.A.; Hudnut, A.; Whittington, R.A.; Taylor, B.; Oxnard, G.R.; Lipson, J.; et al. The PATHFINDER Study: Assessment of the Implementation of an Investigational Multi-Cancer Early Detection Test into Clinical Practice. Cancers 2021, 13, 3501. [Google Scholar] [CrossRef]
- Beer, T.M.; McDonnell, C.H.; Nadauld, L.; Liu, M.C.; Klein, E.A.; Reid, R.L.; Marinac, C.; Chung, K.; Lopatin, M.; Fung, E.T.; et al. Interim results of PATHFINDER, a clinical use study using a methylation-based multi-cancer early detection test. J. Clin. Oncol. 2021, 39, 3010. [Google Scholar] [CrossRef]
- Kint, S.; De Spiegelaere, W.; De Kesel, J.; Vandekerckhove, L.; Van Criekinge, W. Evaluation of bisulfite kits for DNA methylation profiling in terms of DNA fragmentation and DNA recovery using digital PCR. PLoS ONE 2018, 13, e0199091. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sørensen, A.L.; Collas, P. Immunoprecipitation of methylated DNA. Methods Mol. Biol. 2009, 567, 249–262. [Google Scholar] [CrossRef] [PubMed]
- Adela Inc. A breakthrough approach to early detection. Available online: https://www.adelabio.com/ (accessed on 21 August 2022).
- Shen, S.Y.; Burgener, J.M.; Bratman, S.V.; De Carvalho, D.D. Preparation of cfMeDIP-seq libraries for methylome profiling of plasma cell-free DNA. Nat. Protoc. 2019, 14, 2749–2780. [Google Scholar] [CrossRef] [PubMed]
- Shen, S.Y.; Singhania, R.; Fehringer, G.; Chakravarthy, A.; Roehrl, M.H.A.; Chadwick, D.; Zuzarte, P.C.; Borgida, A.; Wang, T.T.; Li, T.; et al. Sensitive tumour detection and classification using plasma cell-free DNA methylomes. Nature 2018, 563, 579–583. [Google Scholar] [CrossRef]
- Sina, A.A.I.; Carrascosa, L.G.; Liang, Z.; Grewal, Y.S.; Wardiana, A.; Shiddiky, M.J.A.; Gardiner, R.A.; Samaratunga, H.; Gandhi, M.K.; Scott, R.J.; et al. Epigenetically reprogrammed methylation landscape drives the DNA self-assembly and serves as a universal cancer biomarker. Nat. Commun. 2018, 9, 4915. [Google Scholar] [CrossRef] [Green Version]
- Szyf, M. The elusive role of 5′-hydroxymethylcytosine. Epigenomics 2016, 8, 1539–1551. [Google Scholar] [CrossRef]
- Li, W.; Zhang, X.; Lu, X.; You, L.; Song, Y.; Luo, Z.; Zhang, J.; Nie, J.; Zheng, W.; Xu, D.; et al. 5-Hydroxymethylcytosine signatures in circulating cell-free DNA as diagnostic biomarkers for human cancers. Cell Res. 2017, 27, 1243–1257. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bluestar Genomics. Multi-Cancer Panels. Available online: https://www.bluestargenomics.com/multi-cancer-panels/ (accessed on 21 August 2022).
- Bergamaschi, A.; Ning, Y.; Ku, C.-J.; Ellison, C.; Collin, F.; Guler, G.; Phillips, T.; McCarthy, E.; Wang, W.; Antoine, M.; et al. Pilot study demonstrating changes in DNA hydroxymethylation enable detection of multiple cancers in plasma cell-free DNA. medRxiv 2020. [Google Scholar] [CrossRef]
- Peng, X.; Li, H.D.; Wu, F.X.; Wang, J. Identifying the tissues-of-origin of circulating cell-free DNAs is a promising way in noninvasive diagnostics. Brief Bioinform. 2021, 22, bbaa060. [Google Scholar] [CrossRef]
- Snyder, M.W.; Kircher, M.; Hill, A.J.; Daza, R.M.; Shendure, J. Cell-free DNA Comprises an In Vivo Nucleosome Footprint that Informs Its Tissues-Of-Origin. Cell 2016, 164, 57–68. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bao, H.; Wang, Z.; Ma, X.; Guo, W.; Zhang, X.; Tang, W.; Chen, X.; Wang, X.; Chen, Y.; Mo, S.; et al. Letter to the Editor: An ultra-sensitive assay using cell-free DNA fragmentomics for multi-cancer early detection. Mol. Cancer 2022, 21, 129. [Google Scholar] [CrossRef] [PubMed]
- DELFI Diagnostics. Our Science. Available online: https://delfidiagnostics.com/our-science/ (accessed on 21 August 2022).
- Cristiano, S.; Leal, A.; Phallen, J.; Fiksel, J.; Adleff, V.; Bruhm, D.C.; Jensen, S.; Medina, J.E.; Hruban, C.; White, J.R.; et al. Genome-wide cell-free DNA fragmentation in patients with cancer. Nature 2019, 570, 385–389. [Google Scholar] [CrossRef]
- Mouliere, F.; Chandrananda, D.; Piskorz, A.M.; Moore, E.K.; Morris, J.; Ahlborn, L.B.; Mair, R.; Goranova, T.; Marass, F.; Heider, K.; et al. Enhanced detection of circulating tumor DNA by fragment size analysis. Sci. Transl. Med. 2018, 10, 466. [Google Scholar] [CrossRef] [Green Version]
- Stackpole, M.; Zeng, W.; Li, S.; Liu, C.-C.; Zhou, Y.; He, S.; Yeh, A.; Wang, Z.; Sun, F.; Li, Q.; et al. Abstract 24: Multi-feature ensemble learning on cell-free dna for accurately detecting and locating cancer. Cancer Res. 2021, 81, 24. [Google Scholar] [CrossRef]
- Giraldez, M.D.; Spengler, R.M.; Etheridge, A.; Goicochea, A.J.; Tuck, M.; Choi, S.W.; Galas, D.J.; Tewari, M. Phospho-RNA-seq: A modified small RNA-seq method that reveals circulating mRNA and lncRNA fragments as potential biomarkers in human plasma. Embo J. 2019, 38, e101695. [Google Scholar] [CrossRef]
- Larson, M.H.; Pan, W.; Kim, H.J.; Mauntz, R.E.; Stuart, S.M.; Pimentel, M.; Zhou, Y.; Knudsgaard, P.; Demas, V.; Aravanis, A.M.; et al. A comprehensive characterization of the cell-free transcriptome reveals tissue- and subtype-specific biomarkers for cancer detection. Nat. Commun. 2021, 12, 2357. [Google Scholar] [CrossRef]
- Ludwig, N.; Leidinger, P.; Becker, K.; Backes, C.; Fehlmann, T.; Pallasch, C.; Rheinheimer, S.; Meder, B.; Stähler, C.; Meese, E.; et al. Distribution of miRNA expression across human tissues. Nucleic Acids Res. 2016, 44, 3865–3877. [Google Scholar] [CrossRef] [PubMed]
- Qi, F.; Gao, F.; Cai, Y.; Han, X.; Qi, Y.; Ni, J.; Sun, J.; Huang, S.; Chen, S.; Wu, C.; et al. Complex Age- and Cancer-Related Changes in Human Blood Transcriptome-Implications for Pan-Cancer Diagnostics. Front. Genet. 2021, 12, 746879. [Google Scholar] [CrossRef] [PubMed]
- Pan, H.; Sun, L.; Wang, W.; Qin, Z.; Tang, L.; Gu, X.; Zhang, J.; He, B. Serum long non-coding RNA LOC553103 as non-specific diagnostic and prognostic biomarker for common types of human cancer. Clin. Chim. Acta 2020, 508, 69–76. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.; Dai, M.; Zhu, H.; Li, J.; Huang, Z.; Liu, X.; Huang, Y.; Chen, J.; Dai, S. Evaluation on the diagnostic and prognostic values of long non-coding RNA BLACAT1 in common types of human cancer. Mol. Cancer 2017, 16, 160. [Google Scholar] [CrossRef] [Green Version]
- Gao, Y.; Deng, K.; Liu, X.; Dai, M.; Chen, X.; Chen, J.; Chen, J.; Huang, Y.; Dai, S.; Chen, J. Molecular mechanism and role of microRNA-93 in human cancers: A study based on bioinformatics analysis, meta-analysis, and quantitative polymerase chain reaction validation. J. Cell Biochem. 2019, 120, 6370–6383. [Google Scholar] [CrossRef]
- Hashimoto, K.; Inada, M.; Yamamoto, Y.; Ochiya, T. Preliminary evaluation of miR-1307-3p in human serum for detection of 13 types of solid cancer using microRNA chip. Heliyon 2021, 7, e07919. [Google Scholar] [CrossRef] [PubMed]
- Varkey, J.; Nicolaides, T. Tumor-Educated Platelets: A Review of Current and Potential Applications in Solid Tumors. Cureus 2021, 13, e19189. [Google Scholar] [CrossRef]
- Best, M.G.; Sol, N.; Kooi, I.; Tannous, J.; Westerman, B.A.; Rustenburg, F.; Schellen, P.; Verschueren, H.; Post, E.; Koster, J.; et al. RNA-Seq of Tumor-Educated Platelets Enables Blood-Based Pan-Cancer, Multiclass, and Molecular Pathway Cancer Diagnostics. Cancer Cell 2015, 28, 666–676. [Google Scholar] [CrossRef] [Green Version]
- Tripathi, V.; Bhartiya, D.; Vaid, A.; Chhabria, S.; Sharma, N.; Chand, B.; Takle, V.; Palahe, P.; Tripathi, A. Quest for Pan-Cancer Diagnosis/Prognosis Ends with HrC Test Measuring Oct4A in Peripheral Blood. Stem Cell Rev. Rep. 2021, 17, 1827–1839. [Google Scholar] [CrossRef]
- Vasseur, A.; Kiavue, N.; Bidard, F.C.; Pierga, J.Y.; Cabel, L. Clinical utility of circulating tumor cells: An update. Mol. Oncol. 2021, 15, 1647–1666. [Google Scholar] [CrossRef]
- Flores, B.C.T.; Correia, M.P.; Rodríguez, J.G.; Henrique, R.; Jerónimo, C. Bridging the Gaps between Circulating Tumor Cells and DNA Methylation in Prostate Cancer. Cancers 2021, 13, 4209. [Google Scholar] [CrossRef] [PubMed]
- Crook, T.; Leonard, R.; Mokbel, K.; Thompson, A.; Michell, M.; Page, R.; Vaid, A.; Mehrotra, R.; Ranade, A.; Limaye, S.; et al. Accurate Screening for Early-Stage Breast Cancer by Detection and Profiling of Circulating Tumor Cells. Cancers 2022, 14, 3341. [Google Scholar] [CrossRef] [PubMed]
- Ilie, M.; Hofman, V.; Long-Mira, E.; Selva, E.; Vignaud, J.-M.; Padovani, B.; Mouroux, J.; Marquette, C.-H.; Hofman, P. “Sentinel” Circulating Tumor Cells Allow Early Diagnosis of Lung Cancer in Patients with Chronic Obstructive Pulmonary Disease. PLoS ONE 2014, 9, e111597. [Google Scholar] [CrossRef] [Green Version]
- Huang, C.; Ding, S.; Huang, C.; Pan, F.; Liu, X.; Zhang, H.; Zhou, J.; Liang, X.; Wang, X.; Song, P. Distribution and Clinical Analysis of EpCAM+/Vimentin+ Circulating Tumor Cells in High-Risk Population and Cancer Patients. Front Oncol. 2021, 11, 642971. [Google Scholar] [CrossRef]
- Hillig, T.; Horn, P.; Nygaard, A.B.; Haugaard, A.S.; Nejlund, S.; Brandslund, I.; Sölétormos, G. In vitro detection of circulating tumor cells compared by the CytoTrack and CellSearch methods. Tumour Biol. 2015, 36, 4597–4601. [Google Scholar] [CrossRef] [Green Version]
- Akolkar, D.; Patil, D.; Crook, T.; Limaye, S.; Page, R.; Datta, V.; Patil, R.; Sims, C.; Ranade, A.; Fulmali, P.; et al. Circulating ensembles of tumor-associated cells: A redoubtable new systemic hallmark of cancer. Int. J. Cancer 2020, 146, 3485–3494. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gaya, A.; Crook, T.; Plowman, N.; Ranade, A.; Limaye, S.; Bhatt, A.; Page, R.; Patil, R.; Fulmali, P.; Datta, V.; et al. Evaluation of circulating tumor cell clusters for pan-cancer noninvasive diagnostic triaging. Cancer Cytopathol. 2021, 129, 226–238. [Google Scholar] [CrossRef]
- Doyle, L.M.; Wang, M.Z. Overview of Extracellular Vesicles, Their Origin, Composition, Purpose, and Methods for Exosome Isolation and Analysis. Cells 2019, 8, 727. [Google Scholar] [CrossRef] [Green Version]
- Urabe, F.; Kosaka, N.; Ito, K.; Kimura, T.; Egawa, S.; Ochiya, T. Extracellular vesicles as biomarkers and therapeutic targets for cancer. Am. J. Physiol. Cell Physiol. 2020, 318, C29–C39. [Google Scholar] [CrossRef]
- Yu, W.; Hurley, J.; Roberts, D.; Chakrabortty, S.K.; Enderle, D.; Noerholm, M.; Breakefield, X.O.; Skog, J.K. Exosome-based liquid biopsies in cancer: Opportunities and challenges. Ann. Oncol. 2021, 32, 466–477. [Google Scholar] [CrossRef]
- Hanahan, D.; Weinberg, R.A. Hallmarks of Cancer: The Next Generation. Cell 2011, 144, 646–674. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goldvaser, H.; Gutkin, A.; Beery, E.; Edel, Y.; Nordenberg, J.; Wolach, O.; Rabizadeh, E.; Uziel, O.; Lahav, M. Characterisation of blood-derived exosomal hTERT mRNA secretion in cancer patients: A potential pan-cancer marker. Br. J. Cancer 2017, 117, 353–357. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hinestrosa, J.P.; Kurzrock, R.; Lewis, J.M.; Schork, N.J.; Schroeder, G.; Kamat, A.M.; Lowy, A.M.; Eskander, R.N.; Perrera, O.; Searson, D.; et al. Early-stage multi-cancer detection using an extracellular vesicle protein-based blood test. Commun. Med. 2022, 2, 29. [Google Scholar] [CrossRef]
- Biological Dynamics. Early Cancer Detection Program. Available online: https://biologicaldynamics.com/early-cancer-detection (accessed on 21 August 2022).
- Hoshino, A.; Kim, H.S.; Bojmar, L.; Gyan, K.E.; Cioffi, M.; Hernandez, J.; Zambirinis, C.P.; Rodrigues, G.; Molina, H.; Heissel, S.; et al. Extracellular Vesicle and Particle Biomarkers Define Multiple Human Cancers. Cell 2020, 182, 1044–1061.e1018. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Shi, J.; Zhang, H.; Zhu, Y.; Liu, W.; Zhang, K.; Zhang, Z. Localized fluorescent imaging of multiple proteins on individual extracellular vesicles using rolling circle amplification for cancer diagnosis. J. Extracell Vesicles 2020, 10, e12025. [Google Scholar] [CrossRef] [PubMed]
- Liu, C.; Zhao, J.; Tian, F.; Cai, L.; Zhang, W.; Feng, Q.; Chang, J.; Wan, F.; Yang, Y.; Dai, B.; et al. Low-cost thermophoretic profiling of extracellular-vesicle surface proteins for the early detection and classification of cancers. Nat. Biomed. Eng. 2019, 3, 183–193. [Google Scholar] [CrossRef]
- Coy, J.F. EDIM-TKTL1/Apo10 Blood Test: An Innate Immune System Based Liquid Biopsy for the Early Detection, Characterization and Targeted Treatment of Cancer. Int. J. Mol. Sci. 2017, 18, 878. [Google Scholar] [CrossRef] [Green Version]
- Feyen, O.; Coy, J.F.; Prasad, V.; Schierl, R.; Saenger, J.; Baum, R.P. EDIM-TKTL1 blood test: A noninvasive method to detect upregulated glucose metabolism in patients with malignancies. Future Oncol. 2012, 8, 1349–1359. [Google Scholar] [CrossRef] [Green Version]
- Grimm, M.; Schmitt, S.; Teriete, P.; Biegner, T.; Stenzl, A.; Hennenlotter, J.; Muhs, H.J.; Munz, A.; Nadtotschi, T.; König, K.; et al. A biomarker based detection and characterization of carcinomas exploiting two fundamental biophysical mechanisms in mammalian cells. BMC Cancer 2013, 13, 569. [Google Scholar] [CrossRef]
- Saman, S.; Stagno, M.J.; Warmann, S.W.; Malek, N.P.; Plentz, R.R.; Schmid, E. Biomarkers Apo10 and TKTL1: Epitope-detection in monocytes (EDIM) as a new diagnostic approach for cholangiocellular, pancreatic and colorectal carcinoma. Cancer Biomark. 2020, 27, 129–137. [Google Scholar] [CrossRef] [Green Version]
- Burg, S.; Audrey, L.; Grust; Feyen, O.; Failing, K.; Banat, G.-A.; Coy, J.; Grimm, M.; Gosau, M.; Smeets, R. Clinical Study Blood-Test Based Targeted Visualization Enables Early Detection of Premalignant and Malignant Tumors in Asymptomatic Individuals. J. Clin. Med. Images 2022, 6, 1–12. [Google Scholar]
- Zyagnum AG. EDIM® TECHNOLOGY. Available online: https://www.zyagnum.com/en/edim-technology/ (accessed on 21 August 2022).
- Zhang, H.; Zhao, L.; Jiang, J.; Zheng, J.; Yang, L.; Li, Y.; Zhou, J.; Liu, T.; Xu, J.; Lou, W.; et al. Multiplexed nanomaterial-assisted laser desorption/ionization for pan-cancer diagnosis and classification. Nat. Commun. 2022, 13, 617. [Google Scholar] [CrossRef]
- Gupta, A.; Sagar, G.; Siddiqui, Z.; Rao, K.V.S.; Nayak, S.; Saquib, N.; Anand, R. A non-invasive method for concurrent detection of early-stage women-specific cancers. Sci. Rep. 2022, 12, 2301. [Google Scholar] [CrossRef] [PubMed]
- Gatto, F.; Bratulic, S.; Cavarretta, I.T.R.; Alfano, M.; Maccari, F.; Galeotti, F.; Volpi, N.; Edqvist, P.-H.; Levin, M.; Nyman, J.; et al. Detection of any-stage cancer using plasma and urine glycosaminoglycans. J. Clin. Oncol. 2021, 39, 3034. [Google Scholar] [CrossRef]
- Elypta. Systems Biology to Identify Biomarkers of Cancer Metabolism—The GAGome. Available online: https://www.elypta.com/science (accessed on 21 August 2022).
- Kusakabe, M.; Sato, M.; Nakamura, Y.; Mikami, H.; Lin, J.; Nagase, H. Elemental analysis by Metallobalance provides a complementary support layer over existing blood biochemistry panel-based cancer risk assessment. PeerJ 2021, 9, e12247. [Google Scholar] [CrossRef]
- Cameron, J.M.; Sala, A.; Antoniou, G.; Brennan, P.M.; Conn, J.J.A.; Connal, S.; Palmer, D.S.; Smith, B.R.; Baker, M.J. Abstract 5920: Multi-cancer early detection with a spectroscopic liquid biopsy platform. Cancer Res. 2022, 82, 5920. [Google Scholar] [CrossRef]
- Dxcover Limited. The Dxcover Platform for Detection of Cancer. Available online: https://www.dxcover.com/technology (accessed on 21 August 2022).
- Ronald, J.A.; Chuang, H.Y.; Dragulescu-Andrasi, A.; Hori, S.S.; Gambhir, S.S. Detecting cancers through tumor-activatable minicircles that lead to a detectable blood biomarker. Proc. Natl. Acad. Sci. USA 2015, 112, 3068–3073. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aalipour, A.; Chuang, H.Y.; Murty, S.; D’Souza, A.L.; Park, S.M.; Gulati, G.S.; Patel, C.B.; Beinat, C.; Simonetta, F.; Martinić, I.; et al. Engineered immune cells as highly sensitive cancer diagnostics. Nat. Biotechnol. 2019, 37, 531–539. [Google Scholar] [CrossRef] [PubMed]
- Dong, S.; Li, W.; Wang, L.; Hu, J.; Song, Y.; Zhang, B.; Ren, X.; Ji, S.; Li, J.; Xu, P.; et al. Histone-Related Genes Are Hypermethylated in Lung Cancer and Hypermethylated HIST1H4F Could Serve as a Pan-Cancer Biomarker. Cancer Res. 2019, 79, 6101–6112. [Google Scholar] [CrossRef] [Green Version]
- Moskalev, E.A.; Jandaghi, P.; Fallah, M.; Manoochehri, M.; Botla, S.K.; Kolychev, O.V.; Nikitin, E.A.; Bubnov, V.V.; von Knebel Doeberitz, M.; Strobel, O.; et al. GHSR DNA hypermethylation is a common epigenetic alteration of high diagnostic value in a broad spectrum of cancers. Oncotarget 2014, 6, 4418. [Google Scholar] [CrossRef] [Green Version]
- Dai, X.; Sun, X.; Wu, Y.; Lv, Z.; Yu, Z.; Yuan, Y.; Sun, L. Site-Specific Hypermethylation of SST 1stExon as a Biomarker for Predicting the Risk of Gastrointestinal Tract Cancers. Dis. Mrk. 2022, 2022, 4570290. [Google Scholar] [CrossRef] [PubMed]
- Margolin, G.; Petrykowska, H.M.; Jameel, N.; Bell, D.W.; Young, A.C.; Elnitski, L. Robust Detection of DNA Hypermethylation of ZNF154 as a Pan-Cancer Locus with in Silico Modeling for Blood-Based Diagnostic Development. J. Mol. Diagn. 2016, 18, 283–298. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tan, S.H.; Ida, H.; Lau, Q.C.; Goh, B.C.; Chieng, W.S.; Loh, M.; Ito, Y. Detection of promoter hypermethylation in serum samples of cancer patients by methylation-specific polymerase chain reaction for tumour suppressor genes including RUNX3. Oncol. Rep. 2007, 18, 1225–1230. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Melson, J.; Li, Y.; Cassinotti, E.; Melnikov, A.; Boni, L.; Ai, J.; Greenspan, M.; Mobarhan, S.; Levenson, V.; Deng, Y. Commonality and differences of methylation signatures in the plasma of patients with pancreatic cancer and colorectal cancer. Int. J. Cancer 2014, 134, 2656–2662. [Google Scholar] [CrossRef] [PubMed]
- Kang, S.; Li, Q.; Chen, Q.; Zhou, Y.; Park, S.; Lee, G.; Grimes, B.; Krysan, K.; Yu, M.; Wang, W.; et al. CancerLocator: Non-invasive cancer diagnosis and tissue-of-origin prediction using methylation profiles of cell-free DNA. Genome Biol. 2017, 18, 53. [Google Scholar] [CrossRef] [Green Version]
- Li, W.; Li, Q.; Kang, S.; Same, M.; Zhou, Y.; Sun, C.; Liu, C.C.; Matsuoka, L.; Sher, L.; Wong, W.H.; et al. CancerDetector: Ultrasensitive and non-invasive cancer detection at the resolution of individual reads using cell-free DNA methylation sequencing data. Nucleic Acids Res. 2018, 46, e89. [Google Scholar] [CrossRef] [Green Version]
- Liu, L.; Toung, J.M.; Jassowicz, A.F.; Vijayaraghavan, R.; Kang, H.; Zhang, R.; Kruglyak, K.M.; Huang, H.J.; Hinoue, T.; Shen, H.; et al. Targeted methylation sequencing of plasma cell-free DNA for cancer detection and classification. Ann. Oncol. 2018, 29, 1445–1453. [Google Scholar] [CrossRef]
- Gao, Q.; Li, B.; Cai, S.; Xu, J.; Wang, C.; Fang, S.; Qiu, F.; Su, J.; Xu, F.; Wen, X.; et al. LBA3 Early detection and localization of multiple cancers using a blood-based methylation assay (ELSA-seq). Ann. Oncol. 2020, 31, S1358. [Google Scholar] [CrossRef]
- Han, T.; Hong, Y.; Zhihua, P.; Xiaofeng, S.; Yu, J.; Chen, G.; Chen, W.; He, J. An ultrasensitive method for noninvasive pan-cancer early detection based on targeted methylation sequencing of cell-free DNA. J. Clin. Oncol. 2021, 39, 10544. [Google Scholar] [CrossRef]
- Han, T.; Liu, T.; Suxing, L.; Li, X.; Zhang, Q.; Yu, J.; Hong, Y.; Li, Y.; Huang, Y.S.; He, J.; et al. An ultrasensitive approach for cancer screening and tissue of origin prediction based on targeted methylation sequencing of cell-free DNA. J. Clin. Oncol. 2022, 40, 10553. [Google Scholar] [CrossRef]
- Kinross, J.; Kruusmaa, K.; Bitenc, M.; Chersicola, M.; Pulverer, W.; Weinhaeusel, A. 97P A panel of methylation markers for multi-cancer detection from plasma. Ann. Oncol. 2020, 31, S280. [Google Scholar] [CrossRef]
- Valouev, A.; Zotenko, E.; Snyder, M.; Eid, C.; Nguyen, N.; Min, J.; He, Y.; Jaimovich, A.; Axelrod, H.; Natarajan, P.; et al. Abstract 2141: Development of a highly-sensitive targeted cell-free DNA epigenomic assay for early-stage multi-cancer screening. Cancer Res. 2022, 82, 2141. [Google Scholar] [CrossRef]
- Zhao, G.Q.; Bao, Y.; Wang, H.; Vu, P.; Patel, S.P.; Lin, S. A novel NGS kit solution for multi-cancer early detection using circulating cell free DNA based methylation analysis. J. Clin. Oncol. 2022, 40, 10542. [Google Scholar] [CrossRef]
- Xu, L.; Wang, J.; Yang, T.; Tao, J.; Liu, X.; Ye, Z.; Zhao, D.; Jiang, Z.; Chen, Z.; Fan, J.-B. Abstract 4601: Toward the development of a $100 screening test for 6 major cancer types. Cancer Res. 2020, 80, 4601. [Google Scholar] [CrossRef]
- Xu, L.; Wang, J.; Ma, W.; Liu, X.; Yang, T.; Li, S.; Hu, Q.; Tao, J.; Ye, Z.; Chen, Z.; et al. Abstract 2610: A high performance blood test for multiple cancer early screening. Cancer Res. 2021, 81, 2610. [Google Scholar] [CrossRef]
- Xu, L.; Wang, J.; Ma, W.; Liu, X.; Li, S.; Chen, S.; Hu, Q.; Yang, T.; Ye, Z.; Chen, Z.; et al. Validation of a high performing blood test for multiple major cancer screenings. J. Clin. Oncol. 2021, 39, 10561. [Google Scholar] [CrossRef]
- Nagasaka, T.; Tanaka, N.; Cullings, H.M.; Sun, D.-S.; Sasamoto, H.; Uchida, T.; Koi, M.; Nishida, N.; Naomoto, Y.; Boland, C.R.; et al. Analysis of Fecal DNA Methylation to Detect Gastrointestinal Neoplasia. JNCI J. Natl. Cancer Inst. 2009, 101, 1244–1258. [Google Scholar] [CrossRef]
- Katerov, S.; Vaccaro, A.; Hennek, J.; Carlson, J.; Taylor, W.R.; Mahoney, D.; Kisiel, J.B.; Allawi, H.T. Abstract 111: Accurate multi-cancer detection using methylated DNA markers and proteins in plasma. Cancer Res. 2021, 81, 111. [Google Scholar] [CrossRef]
- Allawi, H.T.; Katerov, S.; Vaccaro, A.; Fleming, H.L.; Rugowski, D.E.; Otto, B.; Heilberger, J.; Cassel, J.; Hennek, J.; Taylor, W.; et al. Abstract 631: Validation of a panel of methylated DNA and protein markers for multi-cancer detection in plasma. Cancer Res. 2022, 82, 631. [Google Scholar] [CrossRef]
- Chan, K.C.A.; Jiang, P.; Chan, C.W.M.; Sun, K.; Wong, J.; Hui, E.P.; Chan, S.L.; Chan, W.C.; Hui, D.S.C.; Ng, S.S.M.; et al. Noninvasive detection of cancer-associated genome-wide hypomethylation and copy number aberrations by plasma DNA bisulfite sequencing. Proc. Natl. Acad. Sci. USA 2013, 110, 18761–18768. [Google Scholar] [CrossRef] [Green Version]
- Che, H.; Jatsenko, T.; Lenaerts, L.; Dehaspe, L.; Vancoillie, L.; Brison, N.; Parijs, I.; Van Den Bogaert, K.; Fischerova, D.; Heremans, R.; et al. Pan-Cancer Detection and Typing by Mining Patterns in Large Genome-Wide Cell-Free DNA Sequencing Datasets. Clin. Chem. 2022, 68, 1164–1176. [Google Scholar] [CrossRef] [PubMed]
- Liu, W.; Li, J.; Zhang, P.; Hou, Q.; Feng, S.; Liu, L.; Cui, D.; Shi, H.; Fu, Y.; Luo, Y. A novel pan-cancer biomarker plasma heat shock protein 90alpha and its diagnosis determinants in clinic. Cancer Sci. 2019, 110, 2941–2959. [Google Scholar] [CrossRef] [PubMed]
- de Lange, K.; de Boer, E.N.; Bosga, A.; Alimohamed, M.Z.; Johansson, L.F.; Mulder, A.B.; Vellenga, E.; van Diemen, C.C.; Deelen, P.; van den Berg, E.; et al. Targeted RNA-Sequencing Enables Detection of Relevant Translocations and Single Nucleotide Variants and Provides a Method for Classification of Hematological Malignancies-RANKING. Clin. Chem. 2020, 66, 1521–1530. [Google Scholar] [CrossRef]
- Tsvetkov, P.O.; Eyraud, R.; Ayache, S.; Bougaev, A.A.; Malesinski, S.; Benazha, H.; Gorokhova, S.; Buffat, C.; Dehais, C.; Sanson, M.; et al. An AI-Powered Blood Test to Detect Cancer Using NanoDSF. Cancers 2021, 13, 1294. [Google Scholar] [CrossRef]
- Tomczak, K.; Czerwińska, P.; Wiznerowicz, M. The Cancer Genome Atlas (TCGA): An immeasurable source of knowledge. Contemp. Oncol. 2015, 19, A68–A77. [Google Scholar] [CrossRef]
- Goldman, M.; Craft, B.; Swatloski, T.; Ellrott, K.; Cline, M.; Diekhans, M.; Ma, S.; Wilks, C.; Stuart, J.; Haussler, D.; et al. The UCSC Cancer Genomics Browser: Update 2013. Nucleic Acids Res. 2013, 41, D949–D954. [Google Scholar] [CrossRef]
- Cerami, E.; Gao, J.; Dogrusoz, U.; Gross, B.E.; Sumer, S.O.; Aksoy, B.A.; Jacobsen, A.; Byrne, C.J.; Heuer, M.L.; Larsson, E.; et al. The cBio cancer genomics portal: An open platform for exploring multidimensional cancer genomics data. Cancer Discov. 2012, 2, 401–404. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chandrashekar, D.S.; Bashel, B.; Balasubramanya, S.A.H.; Creighton, C.J.; Ponce-Rodriguez, I.; Chakravarthi, B.; Varambally, S. UALCAN: A Portal for Facilitating Tumor Subgroup Gene Expression and Survival Analyses. Neoplasia 2017, 19, 649–658. [Google Scholar] [CrossRef]
- Weinstein, J.N.; Collisson, E.A.; Mills, G.B.; Shaw, K.R.; Ozenberger, B.A.; Ellrott, K.; Shmulevich, I.; Sander, C.; Stuart, J.M. The Cancer Genome Atlas Pan-Cancer analysis project. Nat. Genet. 2013, 45, 1113–1120. [Google Scholar] [CrossRef]
- Human Genomics. The Genotype-Tissue Expression (GTEx) pilot analysis: Multitissue gene regulation in humans. Science 2015, 348, 648–660. [Google Scholar] [CrossRef] [Green Version]
- Barrett, T.; Troup, D.B.; Wilhite, S.E.; Ledoux, P.; Rudnev, D.; Evangelista, C.; Kim, I.F.; Soboleva, A.; Tomashevsky, M.; Edgar, R. NCBI GEO: Mining tens of millions of expression profiles--database and tools update. Nucleic Acids Res. 2007, 35, D760–D765. [Google Scholar] [CrossRef] [Green Version]
- Manoochehri, M.; Wu, Y.; Giese, N.A.; Strobel, O.; Kutschmann, S.; Haller, F.; Hoheisel, J.D.; Moskalev, E.A.; Hackert, T.; Bauer, A.S. SST gene hypermethylation acts as a pan-cancer marker for pancreatic ductal adenocarcinoma and multiple other tumors: Toward its use for blood-based diagnosis. Mol. Oncol. 2020, 14, 1252–1267. [Google Scholar] [CrossRef] [Green Version]
- Chen, W.; Li, G.; Peng, J.; Dai, W.; Su, Q.; He, Y. Transcriptomic analysis reveals that heat shock protein 90α is a potential diagnostic and prognostic biomarker for cancer. Eur. J Cancer Prev. 2020, 29, 357–364. [Google Scholar] [CrossRef] [PubMed]
- Liu, B.; Liu, Y.; Pan, X.; Li, M.; Yang, S.; Li, S.C. DNA Methylation Markers for Pan-Cancer Prediction by Deep Learning. Genes 2019, 10, 778. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ibrahim, J.; Op de Beeck, K.; Fransen, E.; Peeters, M.; Van Camp, G. Genome-wide DNA methylation profiling and identification of potential pan-cancer and tumor-specific biomarkers. Mol. Oncol. 2022, 16, 2432–2447. [Google Scholar] [CrossRef] [PubMed]
- Fan, S.; Tang, J.; Li, N.; Zhao, Y.; Ai, R.; Zhang, K.; Wang, M.; Du, W.; Wang, W. Integrative analysis with expanded DNA methylation data reveals common key regulators and pathways in cancers. NPJ Genom. Med. 2019, 4, 2. [Google Scholar] [CrossRef] [Green Version]
- Yuan, B.; Yang, D.; Rothberg, B.E.G.; Chang, H.; Xu, T. Unsupervised and supervised learning with neural network for human transcriptome analysis and cancer diagnosis. Sci. Rep. 2020, 10, 19106. [Google Scholar] [CrossRef]
- Sun, K.; Wang, J.; Wang, H.; Sun, H. GeneCT: A generalizable cancerous status and tissue origin classifier for pan-cancer biopsies. Bioinformatics 2018, 34, 4129–4130. [Google Scholar] [CrossRef]
- Wang, A.; Hai, R.; Rider, P.J.; He, Q. Noncoding RNAs and Deep Learning Neural Network Discriminate Multi-Cancer Types. Cancers 2022, 14, 352. [Google Scholar] [CrossRef]
- Yuan, F.; Li, Z.; Chen, L.; Zeng, T.; Zhang, Y.H.; Ding, S.; Huang, T.; Cai, Y.D. Identifying the Signatures and Rules of Circulating Extracellular MicroRNA for Distinguishing Cancer Subtypes. Front. Genet. 2021, 12, 651610. [Google Scholar] [CrossRef]
- Huang, S.; Yang, J.; Fong, S.; Zhao, Q. Artificial intelligence in cancer diagnosis and prognosis: Opportunities and challenges. Cancer Lett. 2020, 471, 61–71. [Google Scholar] [CrossRef] [PubMed]
- Shimizu, H.; Nakayama, K.I. Artificial intelligence in oncology. Cancer Sci. 2020, 111, 1452–1460. [Google Scholar] [CrossRef] [Green Version]
- Xu, C.; Jackson, S.A. Machine learning and complex biological data. Genome Biol. 2019, 20, 76. [Google Scholar] [CrossRef] [PubMed]
- Ledesma, D.; Symes, S.; Richards, S. Advancements within Modern Machine Learning Methodology: Impacts and Prospects in Biomarker Discovery. Curr. Med. Chem. 2021, 28, 6512–6531. [Google Scholar] [CrossRef] [PubMed]
- Boehm, K.M.; Khosravi, P.; Vanguri, R.; Gao, J.; Shah, S.P. Harnessing multimodal data integration to advance precision oncology. Nat. Rev. Cancer 2022, 22, 114–126. [Google Scholar] [CrossRef]
- Ding, W.; Chen, G.; Shi, T. Integrative analysis identifies potential DNA methylation biomarkers for pan-cancer diagnosis and prognosis. Epigenetics 2019, 14, 67–80. [Google Scholar] [CrossRef] [Green Version]
- Shimizu, D.; Taniue, K.; Matsui, Y.; Haeno, H.; Araki, H.; Miura, F.; Fukunaga, M.; Shiraishi, K.; Miyamoto, Y.; Tsukamoto, S.; et al. Pan-cancer methylome analysis for cancer diagnosis and classification of cancer cell of origin. Cancer Gene Ther. 2022, 29, 428–436. [Google Scholar] [CrossRef]
- Peng, D.; Ge, G.; Xu, Z.; Ma, Q.; Shi, Y.; Zhou, Y.; Gong, Y.; Xiong, G.; Zhang, C.; He, S.; et al. Diagnostic and prognostic biomarkers of common urological cancers based on aberrant DNA methylation. Epigenomics 2018, 10, 1189–1199. [Google Scholar] [CrossRef]
- Vrba, L.; Futscher, B.W. A suite of DNA methylation markers that can detect most common human cancers. Epigenetics 2018, 13, 61–72. [Google Scholar] [CrossRef] [Green Version]
- Ibrahim, J.; Op de Beeck, K.; Fransen, E.; Peeters, M.; Van Camp, G. The Gasdermin E Gene Has Potential as a Pan-Cancer Biomarker, While Discriminating between Different Tumor Types. Cancers 2019, 11, 1810. [Google Scholar] [CrossRef] [Green Version]
- Wang, S.; Cai, Y. Identification of the functional alteration signatures across different cancer types with support vector machine and feature analysis. Biochim. Biophys. Acta Mol. Basis Dis. 2018, 1864, 2218–2227. [Google Scholar] [CrossRef] [PubMed]
- Grewal, J.K.; Tessier-Cloutier, B.; Jones, M.; Gakkhar, S.; Ma, Y.; Moore, R.; Mungall, A.J.; Zhao, Y.; Taylor, M.D.; Gelmon, K.; et al. Application of a Neural Network Whole Transcriptome-Based Pan-Cancer Method for Diagnosis of Primary and Metastatic Cancers. JAMA Netw. Open 2019, 2, e192597. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hsu, Y.H.; Si, D. Cancer Type Prediction and Classification Based on RNA-sequencing Data. In Proceedings of the 2018 40th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Honolulu, HI, USA, 18–21 July 2018; pp. 5374–5377. [Google Scholar]
- Mohammed, M.; Mwambi, H.; Mboya, I.B.; Elbashir, M.K.; Omolo, B. A stacking ensemble deep learning approach to cancer type classification based on TCGA data. Sci. Rep. 2021, 11, 15626. [Google Scholar] [CrossRef]
- Zhu, L.; Miao, Y.; Xi, F.; Jiang, P.; Xiao, L.; Jin, X.; Fang, M. Identification of Potential Biomarkers for Pan-Cancer Diagnosis and Prognosis Through the Integration of Large-Scale Transcriptomic Data. Front Pharm. 2022, 13, 870660. [Google Scholar] [CrossRef] [PubMed]
- Gobin, E.; Bagwell, K.; Wagner, J.; Mysona, D.; Sandirasegarane, S.; Smith, N.; Bai, S.; Sharma, A.; Schleifer, R.; She, J.-X. A pan-cancer perspective of matrix metalloproteases (MMP) gene expression profile and their diagnostic/prognostic potential. BMC Cancer 2019, 19, 581. [Google Scholar] [CrossRef] [Green Version]
- Zhang, C.; Guo, C.; Li, Y.; Liu, K.; Zhao, Q.; Ouyang, L. Identification of Claudin-6 as a Molecular Biomarker in Pan-Cancer Through Multiple Omics Integrative Analysis. Front. Cell Dev. Biol. 2021, 9, 726656. [Google Scholar] [CrossRef]
- Zhang, C.; Guo, C.; Li, Y.; Ouyang, L.; Zhao, Q.; Liu, K. The role of YTH domain containing 2 in epigenetic modification and immune infiltration of pan-cancer. J. Cell Mol. Med. 2021, 25, 8615–8627. [Google Scholar] [CrossRef] [PubMed]
- Yuan, Y.; Jiang, X.; Tang, L.; Wang, J.; Duan, L. Comprehensive Analysis of the Prognostic and Immunological Role of PAFAH1B in Pan-Cancer. Front. Mol. Biosci. 2021, 8, 799497. [Google Scholar] [CrossRef]
- Chen, J.; Gao, G.; Li, L.; Ding, J.; Chen, X.; Lei, J.; Long, H.; Wu, L.; Long, X.; He, L.; et al. Pan-Cancer Study of SHC-Adaptor Protein 1 (SHC1) as a Diagnostic, Prognostic and Immunological Biomarker in Human Cancer. Front. Genet. 2022, 13, 817118. [Google Scholar] [CrossRef]
- Chen, G.; Luo, D.; Zhong, N.; Li, D.; Zheng, J.; Liao, H.; Li, Z.; Lin, X.; Chen, Q.; Zhang, C.; et al. GPC2 Is a Potential Diagnostic, Immunological, and Prognostic Biomarker in Pan-Cancer. Front. Immunol. 2022, 13, 857308. [Google Scholar] [CrossRef]
- Hongzhen, Z.; Yanyu, L.; Xuexiang, L.; Meiyu, D.; Xiaoli, C.; Yun, G.; Jingfan, C.; Shengming, D. The diagnostic and prognostic significance of long non-coding RNA CRNDE in pan-cancer based on TCGA, GEO and comprehensive meta–analysis. Pathol. Res. Pract. 2019, 215, 256–264. [Google Scholar] [CrossRef] [PubMed]
- Ching, T.; Peplowska, K.; Huang, S.; Zhu, X.; Shen, Y.; Molnar, J.; Yu, H.; Tiirikainen, M.; Fogelgren, B.; Fan, R.; et al. Pan-Cancer Analyses Reveal Long Intergenic Non-Coding RNAs Relevant to Tumor Diagnosis, Subtyping and Prognosis. EBioMedicine 2016, 7, 62–72. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xu, D.; Wang, L.; Pang, S.; Cao, M.; Wang, W.; Yu, X.; Xu, Z.; Xu, J.; Wang, H.; Lu, J.; et al. The Functional Characterization of Epigenetically Related lncRNAs Involved in Dysregulated CeRNA-CeRNA Networks Across Eight Cancer Types. Front. Cell Dev. Biol. 2021, 9, 649755. [Google Scholar] [CrossRef] [PubMed]
- Wang, D.; Zou, L.; Luo, J.; Zhang, C.; Feng, H.; Qin, G. Potential diagnostic and prognostic value of the long non-coding RNA SNHG3 in human cancers: A systematic review and meta-analysis. Int. J. Biol. Mrk. 2022, 37, 3–12. [Google Scholar] [CrossRef] [PubMed]
- Cheerla, N.; Gevaert, O. MicroRNA based Pan-Cancer Diagnosis and Treatment Recommendation. BMC Bioinform. 2017, 18, 32. [Google Scholar] [CrossRef] [Green Version]
- Lai, C.H.; Liang, X.Z.; Liang, X.Y.; Ma, S.J.; Li, J.G.; Shi, M.F.; Zhu, X.; Lan, H.H.; Zeng, J.H. Study on miRNAs in Pan-Cancer of the Digestive Tract Based on the Illumina HiSeq System Data Sequencing. Biomed. Res. Int. 2019, 2019, 8016120. [Google Scholar] [CrossRef]
- Zhang, A.; Hu, H. A Novel Blood-Based microRNA Diagnostic Model with High Accuracy for Multi-Cancer Early Detection. Cancers 2022, 14, 1450. [Google Scholar] [CrossRef]
- Zhang, B.; Chen, Z.; Tao, B.; Yi, C.; Lin, Z.; Li, Y.; Shao, W.; Lin, J.; Chen, J. m(6)A target microRNAs in serum for cancer detection. Mol. Cancer 2021, 20, 170. [Google Scholar] [CrossRef]
- Ji, X.; Cui, Q. Ancient genes can be served as pan-cancer diagnostic and prognostic biomarkers. J. Cell Mol. Med. 2020, 24, 6908–6915. [Google Scholar] [CrossRef]
- Braunstein, G.D.; Ofman, J.J. Criteria for Evaluating Multi-cancer Early Detection Tests. Touchrev. Oncol. Haematol. 2021, 17, 3–6. [Google Scholar] [CrossRef]
- Etzioni, R.; Gulati, R.; Weiss, N.S. Multicancer Early Detection: Learning From the Past to Meet the Future. J. Natl. Cancer Inst. 2022, 114, 349–352. [Google Scholar] [CrossRef] [PubMed]
- Loomans-Kropp, H.A.; Umar, A.; Minasian, L.M.; Pinsky, P.F. Multi-Cancer Early Detection Tests: Current Progress and Future Perspectives. Cancer Epidemiol. Biomark. Prev. 2022, 31, 512–514. [Google Scholar] [CrossRef] [PubMed]
- Putcha, G.; Gutierrez, A.; Skates, S. Multicancer Screening: One Size Does Not Fit All. JCO Precis. Oncol. 2021, 5, 574–576. [Google Scholar] [CrossRef] [PubMed]
- Hackshaw, A.; Berg, C.D. An efficient randomised trial design for multi-cancer screening blood tests: Nested enhanced mortality outcomes of screening trial. Lancet Oncol. 2021, 22, 1360–1362. [Google Scholar] [CrossRef]
- Hubbell, E.; Clarke, C.A.; Aravanis, A.M.; Berg, C.D. Modeled Reductions in Late-stage Cancer with a Multi-Cancer Early Detection Test. Cancer Epidemiol. Biomark. Prev. 2021, 30, 460–468. [Google Scholar] [CrossRef] [PubMed]
- Hathaway, C.; Paetsch, P.; Li, Y.; Wu, J.; Asgarian, S.; Parker, A.; Welsh, A.; Deverka, P.; Cohain, A. Association of Breast Cancer Screening Behaviors with Stage at Breast Cancer Diagnosis and Potential for Additive Multi-Cancer Detection via Liquid Biopsy Screening: A Claims-Based Study. Front. Oncol. 2021, 11, 688455. [Google Scholar] [CrossRef]
- Hackshaw, A.; Cohen, S.S.; Reichert, H.; Kansal, A.R.; Chung, K.C.; Ofman, J.J. Estimating the population health impact of a multi-cancer early detection genomic blood test to complement existing screening in the US and UK. Br. J. Cancer 2021, 125, 1432–1442. [Google Scholar] [CrossRef]
- Tafazzoli, A.; Ramsey, S.D.; Shaul, A.; Chavan, A.; Ye, W.; Kansal, A.R.; Ofman, J.; Fendrick, A.M. The Potential Value-Based Price of a Multi-Cancer Early Detection Genomic Blood Test to Complement Current Single Cancer Screening in the USA. Pharmacoeconomics 2022, 40, 1107–1117. [Google Scholar] [CrossRef]
- Jiao, B.; Gulati, R.; Katki, H.A.; Castle, P.E.; Etzioni, R. A Quantitative Framework to Study Potential Benefits and Harms of Multi-Cancer Early Detection Testing. Cancer Epidemiol. Biomark. Prev. 2022, 31, 38–44. [Google Scholar] [CrossRef]
- Marlow, L.A.V.; Schmeising-Barnes, N.; Brain, K.; Duncombe, S.; Robb, K.A.; Round, T.; Sanderson, S.C.; Waller, J. Multi-cancer early detection tests for cancer screening: A behavioural science perspective. Lancet Oncol. 2022, 23, 837–839. [Google Scholar] [CrossRef]
- Ewalt, M.D.; West, H.; Aisner, D.L. Next Generation Sequencing—Testing Multiple Genetic Markers at Once. JAMA Oncol. 2019, 5, 1076. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Soto, J.; Rodriguez-Antolin, C.; Vallespín, E.; de Castro Carpeño, J.; Ibanez de Caceres, I. The impact of next-generation sequencing on the DNA methylation-based translational cancer research. Transl. Res. 2016, 169, 1–18. [Google Scholar] [CrossRef] [Green Version]
- Rossi, G.; Ignatiadis, M. Promises and Pitfalls of Using Liquid Biopsy for Precision Medicine. Cancer Res. 2019, 79, 2798–2804. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Connors, D.; Allen, J.; Alvarez, J.D.; Boyle, J.; Cristofanilli, M.; Hiller, C.; Keating, S.; Kelloff, G.; Leiman, L.; McCormack, R.; et al. International liquid biopsy standardization alliance white paper. Crit. Rev. Oncol./Hematol. 2020, 156, 103112. [Google Scholar] [CrossRef] [PubMed]



Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Brito-Rocha, T.; Constâncio, V.; Henrique, R.; Jerónimo, C. Shifting the Cancer Screening Paradigm: The Rising Potential of Blood-Based Multi-Cancer Early Detection Tests. Cells 2023, 12, 935. https://doi.org/10.3390/cells12060935
Brito-Rocha T, Constâncio V, Henrique R, Jerónimo C. Shifting the Cancer Screening Paradigm: The Rising Potential of Blood-Based Multi-Cancer Early Detection Tests. Cells. 2023; 12(6):935. https://doi.org/10.3390/cells12060935
Chicago/Turabian StyleBrito-Rocha, Tiago, Vera Constâncio, Rui Henrique, and Carmen Jerónimo. 2023. "Shifting the Cancer Screening Paradigm: The Rising Potential of Blood-Based Multi-Cancer Early Detection Tests" Cells 12, no. 6: 935. https://doi.org/10.3390/cells12060935
APA StyleBrito-Rocha, T., Constâncio, V., Henrique, R., & Jerónimo, C. (2023). Shifting the Cancer Screening Paradigm: The Rising Potential of Blood-Based Multi-Cancer Early Detection Tests. Cells, 12(6), 935. https://doi.org/10.3390/cells12060935