
Association between Plasma HLA-DR+ Placental Vesicles and Preeclampsia: A Pilot Longitudinal Cohort Study

 ,
, 
 and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Sample Collection
2.3. Isolation of STEVs from Plasma
2.4. Western Blot
2.5. Nanoparticle Tracking Analysis (NTA)
2.6. Flow Cytometry
2.7. Placental Growth Factor (PlGF) Analysis
2.8. Statistical Analysis
3. Results
3.1. Clinical Results
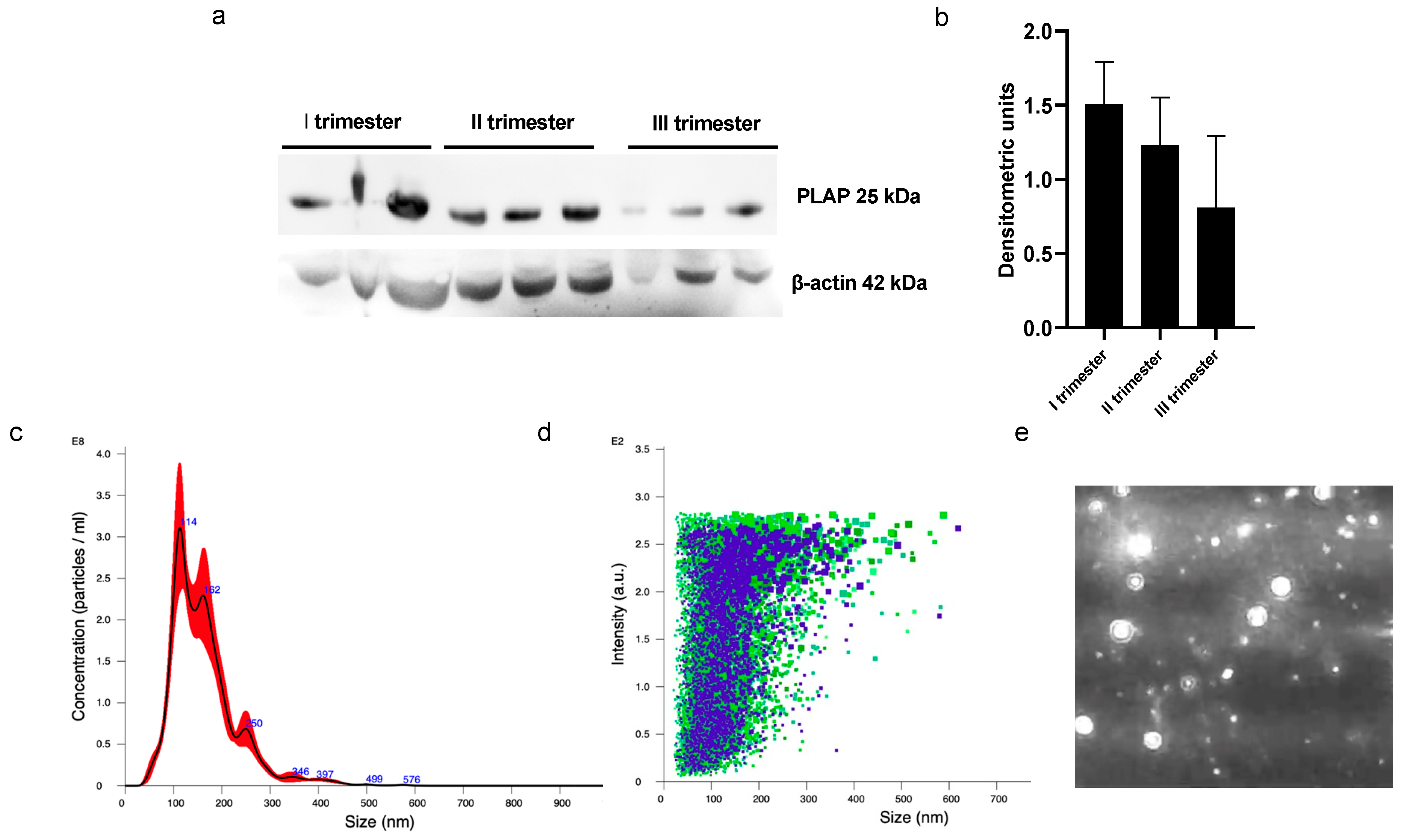
3.2. STEVs Can Be Detected in Peripheral Blood of Pregnant Women from Early First Trimester of Pregnancy
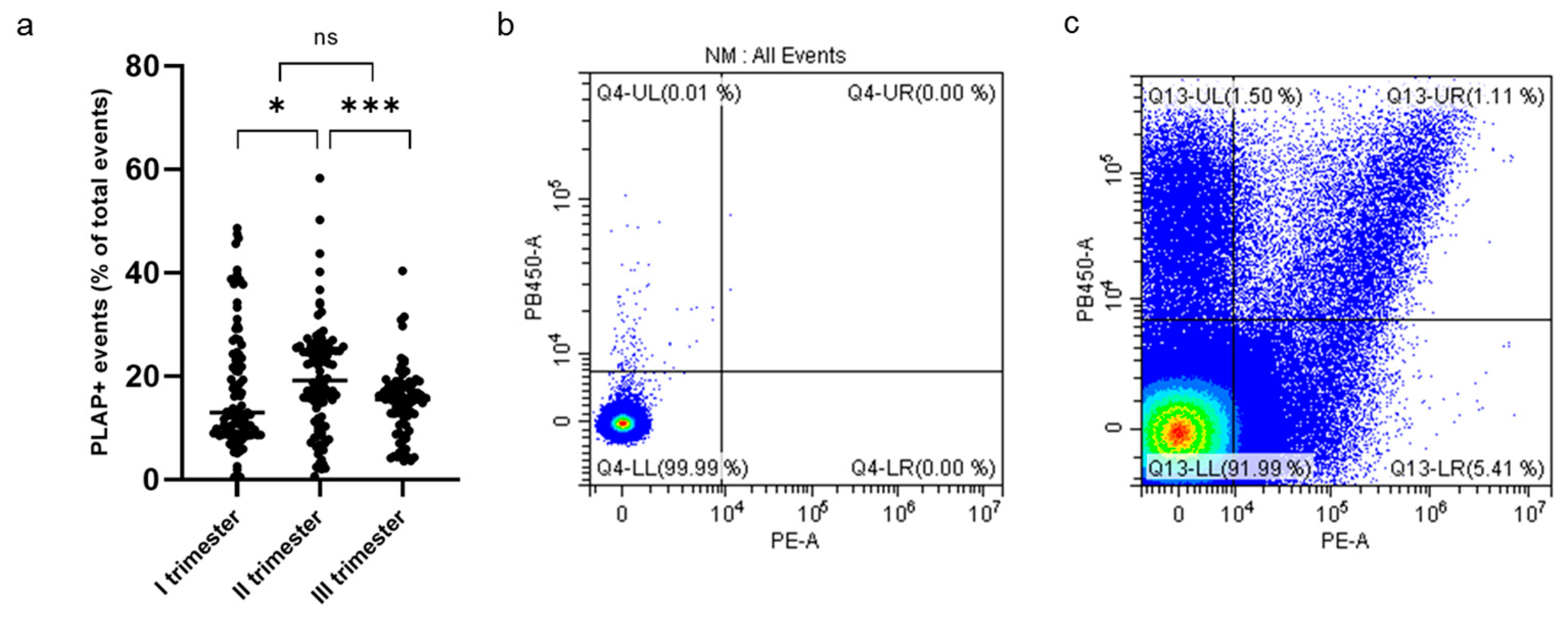
3.3. Circulating HLA-DR+ STEVs Can Be Detected in Pregnant Women during the Three Trimesters of Pregnancy
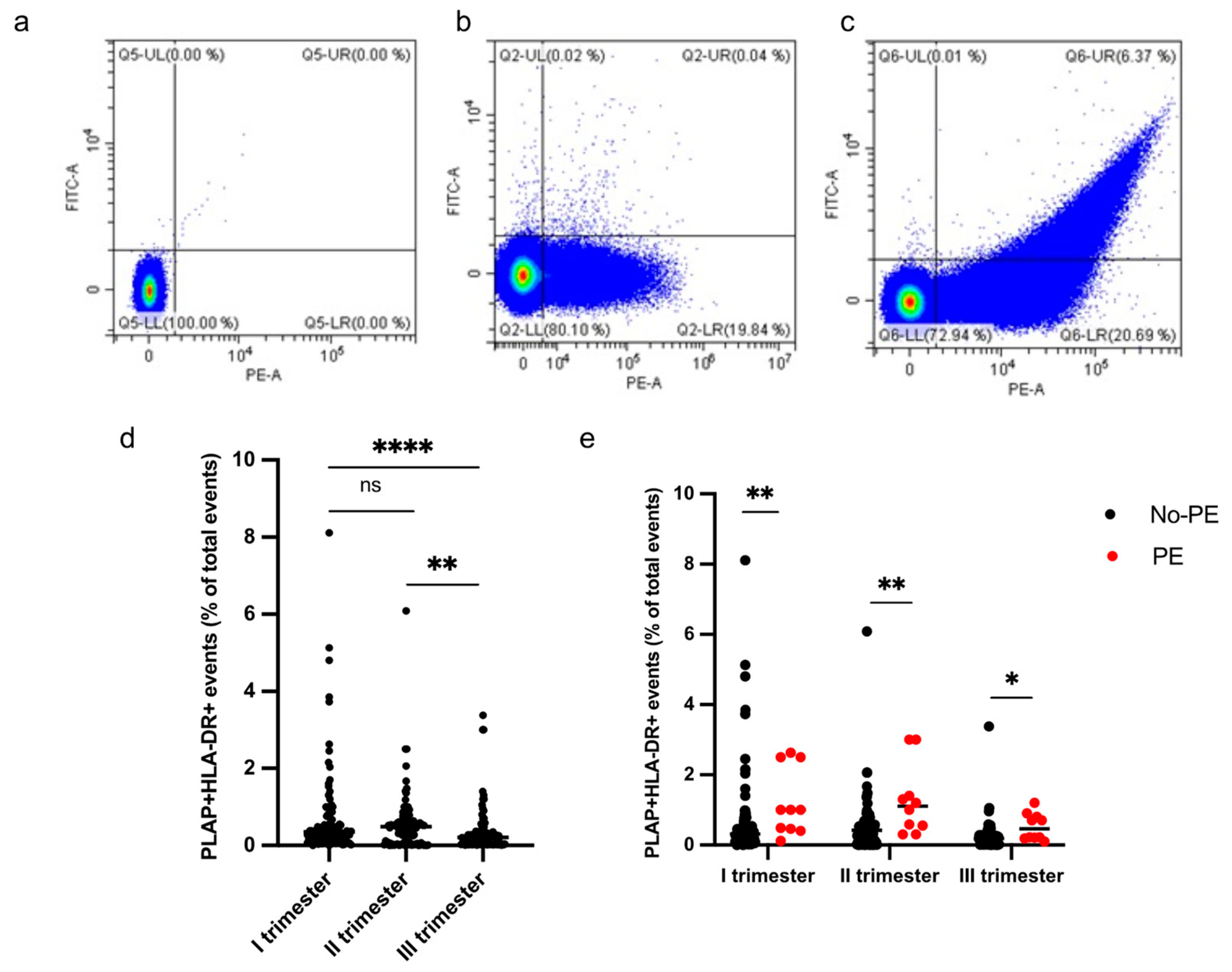
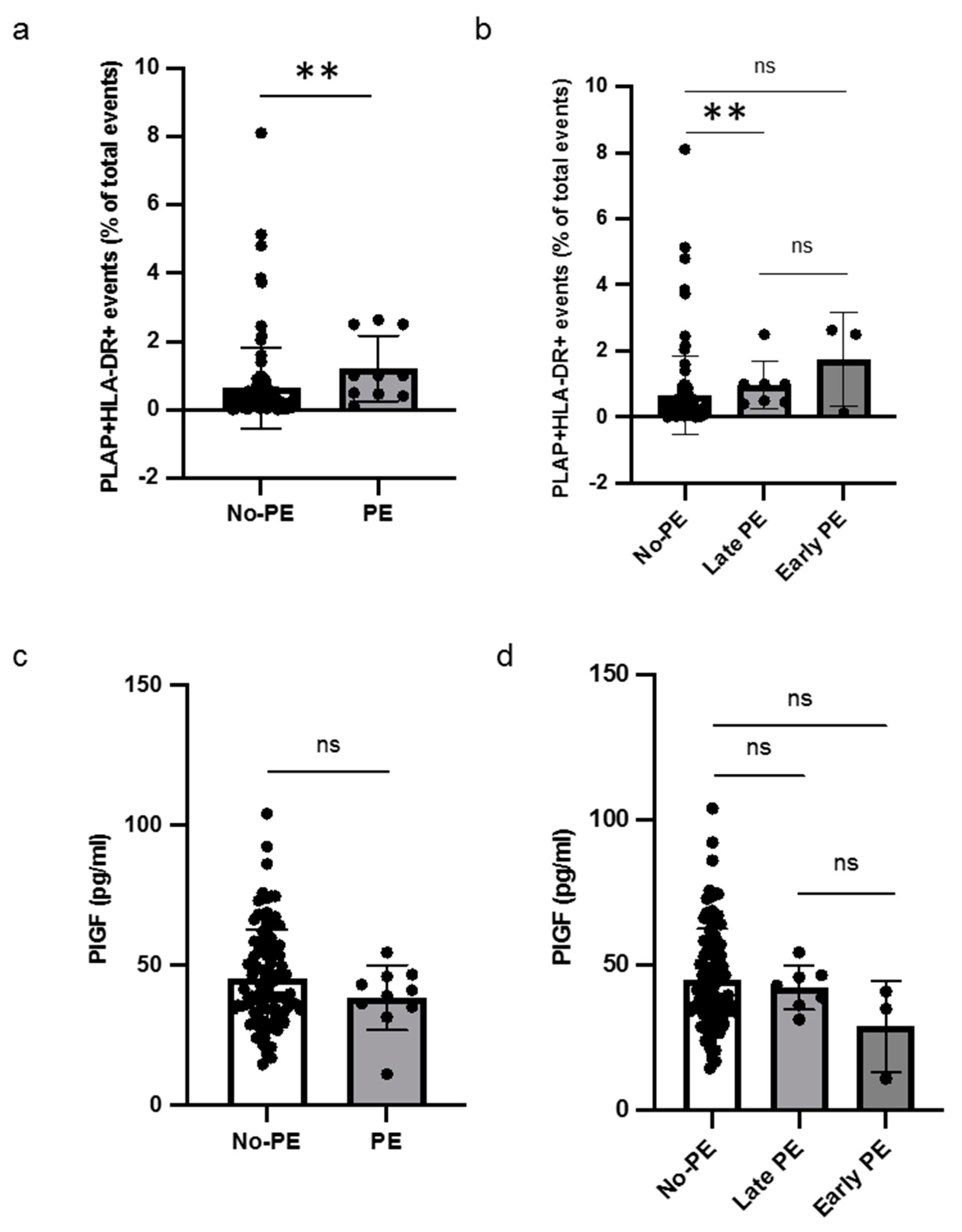
3.4. Levels of HLA-DR+ STEVs and PlGF in PE
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Duley, L. The global impact of pre-eclampsia and eclampsia. Semin. Perinatol. 2009, 33, 130–137. [Google Scholar] [CrossRef] [PubMed]
- Magee, L.A.; Brown, M.A.; Hall, D.R.; Gupte, S.; Hennessy, A.; Karumanchi, S.A.; Kenny, L.C.; McCarthy, F.; Myers, J.; Poon, L.C.; et al. The 2021 International Society for the Study of Hypertension in Pregnancy classification, diagnosis & management recommendations for international practice. Pregnancy Hypertens. 2021, 27, 148–169. [Google Scholar]
- Redman, C.W.; Sargent, I.L. Immunology of pre-eclampsia. J. Reprod. Immunol. 2010, 63, 534–543. [Google Scholar] [CrossRef] [PubMed]
- Saito, S.S.; Sakai, M.; Sasaki, Y.; Nakashima, A.; Shiozaki, A. Inadequate tolerance induction may induce pre-eclampsia. Am. J. Reprod. Immunol. 2007, 76, 30–39. [Google Scholar] [CrossRef] [PubMed]
- Sargent, I.L.; Borzychowski, A.M.; Redman, C.W.G. NK cells and human pregnancy—An inflammatory view. Trends Immunol. 2006, 27, 399–404. [Google Scholar] [CrossRef] [PubMed]
- Tersigni, C.; Redman, C.W.; Dragovic, R.; Tannetta, D.; Scambia, G.; Di Simone, N.; Sargent, I.; Vatish, M. HLA-DR is aberrantly expressed at feto-maternal interface in pre-eclampsia. J. Reprod. Immunol. 2018, 129, 48–52. [Google Scholar] [CrossRef] [PubMed]
- Tersigni, C.; Lucchetti, D.; Franco, R.; Colella, F.; Neri, C.; Crispino, L.; Sgambato, A.; Lanzone, A.; Scambia, G.; Vatish, M.; et al. Circulating Placental Vesicles Carry HLA-DR in Pre-Eclampsia: A New Potential Marker of the Syndrome. Front. Immunol. 2021, 12, 717879. [Google Scholar] [CrossRef] [PubMed]
- Rolnik, D.L.; Wright, D.; Poon, L.C.Y.; Syngelaki, A.; O’Gorman, N.; de Paco Matallana, C.; Akolekar, R.; Cicero, S.; Janga, D.; Singh, M.; et al. ASPRE trial: Performance of screening for preterm pre-eclampsia. Ultrasound Obstet. Gynecol. 2017, 50, 492–495. [Google Scholar] [CrossRef] [PubMed]
- Akolekar, R.; Syngelaki, A.; Poon, L.; Wright, D.; Nicolaides, K.H. Competing risks modelin early screening for preeclampsia by biophysical and biochemical markers. Fetal Diagn. Ther. 2013, 33, 8–15. [Google Scholar] [CrossRef] [PubMed]
- Brown, M.A.; Magee, L.A.; Kenny, L.C.; Karumanchi, S.A.; McCarthy, F.P.; Saito, S.; Hall, D.R.; Warren, C.E.; Adoyi, G.; Ishaku, S. The hypertensive disorders of pregnancy: ISSHP classification, diagnosis & management recommendations for international practice. Pregnancy Hypertens. 2018, 13, 291–310. [Google Scholar] [PubMed]
- Tannetta, D.; Collett, G.; Vatish, M.; Redman, C.; Sargent, I. Syncytiotrophoblast extracellular vesicles-Circulating biopsies reflecting placental health. Placenta 2017, 52, 134–138. [Google Scholar] [CrossRef] [PubMed]
- Sammar, M.; Dragovic, R.; Meiri, H.; Vatish, M.; Sharabi-Nov, A.; Sargent, I.; Redman, C.; Tannetta, D. Reduced placental protein 13 (PP13) in placental derived syncytiotrophoblast extracellular vesicles in preeclampsia—A novel tool to study the impaired cargo transmission of the placenta to the maternal organs. Placenta 2018, 66, 17–25. [Google Scholar] [CrossRef] [PubMed]
- Licini, C.; Avellini, C.; Picchiassi, E.; Mensà, E.; Fantone, S.; Ramini, D.; Tersigni, C.; Tossetta, G.; Castellucci, C.; Tarquini, F.; et al. Pre-eclampsia predictive ability of maternal miR-125b: A clinical and experimental study. Transl. Res. 2021, 228, 13–27. [Google Scholar] [CrossRef] [PubMed]
- Jiang, S.; Zhang, W.; Cao, Q.; Rahbar, M.; Cooke, W.; Ono, M.; Fujimaki, K.; Saito, A.; Itonaga, M.; Oda, K.; et al. ExoCounter Assays Identify Women Who May Develop Early-Onset Preeclampsia From 12.5 μL First-Trimester Serum by Characterizing Placental Small Extracellular Vesicles. Hypertension 2023, 80, 1439–1451. [Google Scholar] [CrossRef]
- Sarker, S.; Scholz-Romero, K.; Perez, A.; Illanes, S.E.; Mitchell, M.D.; Rice, G.E.; Salomon, C. Placenta-derived exosomes continuously increase in maternal circulation over the first trimester of pregnancy. J. Transl. Med. 2014, 12, 204. [Google Scholar] [CrossRef] [PubMed]
- Salomon, C.; Guanzon, D.; Scholz-Romero, K.; Longo, S.; Correa, P.; Illanes, S.E.; Rice, G.E. Placental Exosomes as Early Biomarker of Preeclampsia: Potential Role of Exosomal MicroRNAs Across Gestation. J. Clin. Endocrinol. Metab. 2017, 102, 3182–3194. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Low Risk (n = 90) | High Risk (n = 17) | p | |
|---|---|---|---|
| Age (years) | 33.5 ± 4.5 | 34.25 ± 4.4 | 0.4 |
| BMI (Kg/m2) | 23.1 ± 11.8 | 24.7 ± 11.1 | 0.6 |
| Race | |||
| White | 84 (93.4%) | 16 (94%) | |
| Black | 2 (2.2%) | 1 (6%) | |
| South Asian | 3 (3.3%) | 0 | |
| East Asian | 1 (1.1%) | 0 | |
| Proteinuria (%) | 1(1.1%) | 2 (12%) | <0.05 |
| Medical history | |||
| Previous PE | 0 | 2 (12%) | <0.0001 |
| Family history of PE | 4 (4.44%) | 0 | 0.5 |
| Chronic hypertension | 0 | 4 (23.5%) | <0.0001 |
| DM Type I | 1 (1.1%) | 1 (6%) | 0.2 |
| DM Type II | 1 (1.1%) | 2 (11.8%) | <0.05 |
| GDM | 11 (12.2%) | 4 (23.5%) | <0.05 |
| SLE/APS/RA | 3 (3.3%) | 1 (6%) | 0.7 |
| Cigarette smoking (%) | 2 (2.2%) | 2(12%) | 0.09 |
| Method of conception | |||
| Spontaneous | 89 (98.8%) | 16 (94%) | 0.2 |
| ART | 1 (1.1%) | 1 (6%) | 0.2 |
| Nulliparous | 59 (65.5%) | 10 (59%) | 0.2 |
| Anti-hypertensive drugs | |||
| Labetalol | 1 (1.1%) | 3 (17.6%) | <0.01 |
| Metildopa | 1 (1.1%) | 5 (29%) | <0.001 |
| Nifedipina | 0 | 1 (6%) | <0.01 |
| Aspirin | 11 (12.2%) | 14 (82%) | <0.0001 |
| Heparin | 3 (3.3%) | 3 (17.6%) | <0.05 |
| Biomarker | |||
| MAP (mmHg) | 98.4 ± 12.5 | 105.2 ± 11.5 | <0.01 |
| UtA-PI | 1.6 ± 0.6 | 2.1 ± 0.5 | <0.01 |
| PlGF (pg/mL) | 45.8 ± 17.1 | 39.0 ± 19.0 | 0.2 |
| PAPP-A (IU/L) | 2.9 ± 1.6 | 1.7 ± 0.9 | <0.05 |
| PE | 1 (1.1%) | 9 (53%) | <0.0001 |
| Early (<34 weeks) | 0 | 3 (33%) | <0.01 |
| Late (>34 weeks) | 1 (1.1%) | 6 (66%) | <0.01 |
| GA delivery (weeks) | 39.1 ± 2.0 | 36.2 ± 5.5 | <0.0001 |
| Neonatal Weight (g) | 3217.6 ± 601.6 | 2684.8 ± 833.4 | <0.0001 |
| Percentile (°) | 44.6 ± 26.7 | 23.1 ± 21.4 | <0.001 |
| Non-PE (n = 97) | PE (n = 10) | p | |
|---|---|---|---|
| Age (years) | 33.27 ± 4.34 | 36.3 ± 7.89 | 0.3 |
| BMI (Kg/m2) | 23.30 ± 11.81 | 24 ± 12 | 0.5 |
| Race | |||
| White | 91 (93.9%) | 9 (90%) | |
| Black | 1 (1%) | 1 (10%) | |
| South Asian | 4 (4.1%) | 0 | |
| East Asian | 1 (1%) | 0 | |
| Proteinuria (%) | 0 | 3 (30%) | <0.01 |
| Medical history | |||
| Previous PE | 2 (2.1%) | 0 | 0.8 |
| Family history of PE | 4 (4.1%) | 0 | 0.7 |
| Chronic hypertension | 2 (2.1%) | 2 (20%) | <0.05 |
| DM Type I | 2 (2.1%) | 0 | 0.8 |
| DM Type II | 3 (3.1%) | 0 | 0.7 |
| GDM | 14 (14.4%) | 1 (10%) | 0.5 |
| SLE/APS/RA | 3 (3.1%) | 1 (10%) | 0.4 |
| Cigarette smoking (%) | 3 (3.1%) | 1 (10%) | 0.4 |
| Method of conception | |||
| Spontaneous | 96 (98.9%) | 9 (90%) | <0.05 |
| ART | 1 (1.03%) | 1 (10%) | 0.09 |
| Nulliparous | 64 (66%) | 5 (50%) | 0.06 |
| Anti-hypertensive drugs | |||
| Labetalol | 0 | 4 (40%) | <0.0001 |
| Metildopa | 2 (2.1%) | 4 (40%) | <0.0001 |
| Nifedipina | 0 | 1 (10%) | |
| Aspirin | 14 (14.4%) | 8 (80%) | <0.0001 |
| Heparin | 3 (3.1%) | 3 (30%) | <0.01 |
| Biomarker | |||
| MAP (mmHg) | 97.06 ± 10.08 | 119.75 ± 10.34 | <0.0001 |
| UtA-PI | 1.69 ± 0.56 | 1.82 ± 0.84 | 0.6 |
| PlGF (pg/mL) | 45.31 ± 17.33 | 38.65 ± 19.07 | 0.4 |
| PAPP-A (IU/L) | 2.79 ± 1.60 | 1.12 ± 0.49 | <0.01 |
| GA delivery (weeks) | 38.96 ± 2.61 | 34.9 ± 3.98 | <0.0001 |
| Neonatal weight (g) | 3223.33 ± 575.49 | 2108.75 ± 1071.8 | <0.0001 |
| Percentile (°) | 44.64 ± 25.99 | 8.5 ± 15.94 | <0.01 |
| HLA-DR- (n = 91) | HLA-DR+ (n = 16) | p | |
|---|---|---|---|
| Age (years) | 33.6 ± 4.3 | 31.6 ± 5.6 | 0.2 |
| BMI (Kg/m2) | 23.1 ± 5.0 | 23 ± 5.4 | 0.5 |
| Race | |||
| White | 87 (95.6%) | 16 (100%) | |
| Black | 2 (2.2%) | 0 | |
| South Asian | 1 (1.1%) | 0 | |
| East Asian | 1 (1.1%) | 0 | |
| Proteinuria (%) | 2 (2.2%) | 1 (6.3%) | 0.4 |
| Medical history | |||
| Previous PE | 2 (2.2%) | 0 | 0.6 |
| Family history of PE | 3 (3.3%) | 1 (6.3%) | 0.5 |
| Chronic hypertension | 3 (3.3%) | 1 (6.3%) | 0.5 |
| DM Type I | 2 (2.2%) | 0 | 0.6 |
| DM Type II | 3 (3.3%) | 0 | 0.5 |
| GDM | 15 (16.5%) | 0 | 0.1 |
| SLE/APS/RA | 3 (3.3%) | 1 (6.3%) | 0.5 |
| Cigarette smoking (%) | 4 (4.4%) | 0 | 0.5 |
| Method of conception | |||
| Spontaneous | 90 (98.9%) | 15 (93.7%) | 0.1 |
| ART | 1 (1.1%) | 1 (6.3%) | 0.1 |
| Nulliparous | 60 (65.9%) | 9 (56%) | 0.6 |
| Anti-hypertensive drugs | |||
| Labetalol | 2 (2.2%) | 2 (12.5%) | 0.05 |
| Metildopa | 5 (5.5%) | 1(6.3%) | 0.9 |
| Nifedipina | 0 | 1 (6.3%) | |
| Aspirin | 21 (23%) | 4 (25%) | 0.8 |
| Heparin | 5 (5.5%) | 1 (6.3%) | 0.9 |
| Biomarker | |||
| MAP (mmHg) | 97.4 ± 9.2 | 106.1 ± 20.4 | 0.1 |
| UtA-PI | 1.7 ± 0.6 | 1.6 ± 0.5 | 0.4 |
| PlGF (pg/mL) | 45.1± 17.4 | 44.8 ± 17.8 | 0.9 |
| PAPP-A (IU/L) | 2.7 ± 1.6 | 2.6 ± 1.7 | 0.7 |
| PE | 4 (4.4%) | 6 (37.5%) | <0.0001 |
| Early (<34 weeks) | 1 (25%) | 2 (33.3%) | 0.7 |
| Late (>34 weeks) | 3 (75%) | 4 (66.6%) | 0.7 |
| GA delivery (weeks) | 38.7 ± 2.7 | 38.8 ± 3.0 | 0.8 |
| Neonatal weight (g) | 3152.4 ± 594.9 | 3102.7 ± 888.8 | 0.6 |
| Percentile (°) | 41.9 ± 26.4 | 40.3 ± 29.4 | 0.8 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Onori, M.; Franco, R.; Lucchetti, D.; Tartaglia, S.; Buongiorno, S.; Beneduce, G.; Sannino, F.; Baroni, S.; Urbani, A.; Lanzone, A.; et al. Association between Plasma HLA-DR+ Placental Vesicles and Preeclampsia: A Pilot Longitudinal Cohort Study. Cells 2024, 13, 196. https://doi.org/10.3390/cells13020196
Onori M, Franco R, Lucchetti D, Tartaglia S, Buongiorno S, Beneduce G, Sannino F, Baroni S, Urbani A, Lanzone A, et al. Association between Plasma HLA-DR+ Placental Vesicles and Preeclampsia: A Pilot Longitudinal Cohort Study. Cells. 2024; 13(2):196. https://doi.org/10.3390/cells13020196
Chicago/Turabian StyleOnori, Marianna, Rita Franco, Donatella Lucchetti, Silvio Tartaglia, Silvia Buongiorno, Giuliana Beneduce, Fabio Sannino, Silvia Baroni, Andrea Urbani, Antonio Lanzone, and et al. 2024. "Association between Plasma HLA-DR+ Placental Vesicles and Preeclampsia: A Pilot Longitudinal Cohort Study" Cells 13, no. 2: 196. https://doi.org/10.3390/cells13020196
APA StyleOnori, M., Franco, R., Lucchetti, D., Tartaglia, S., Buongiorno, S., Beneduce, G., Sannino, F., Baroni, S., Urbani, A., Lanzone, A., Scambia, G., Di Simone, N., & Tersigni, C. (2024). Association between Plasma HLA-DR+ Placental Vesicles and Preeclampsia: A Pilot Longitudinal Cohort Study. Cells, 13(2), 196. https://doi.org/10.3390/cells13020196