
A Systematic Review on Drugs Acting as Nicotinic Acetylcholine Receptor Agonists in the Treatment of Dementia

 ,
,  , ,
, ,  ,
,  ,
,  , ,
, ,
Abstract
:1. Introduction
1.1. Nicotinic Acetylcholine Receptors in CNS
1.2. Nicotinic Acetylcholine Receptors in Dementia
2. Materials and Methods
2.1. Methods
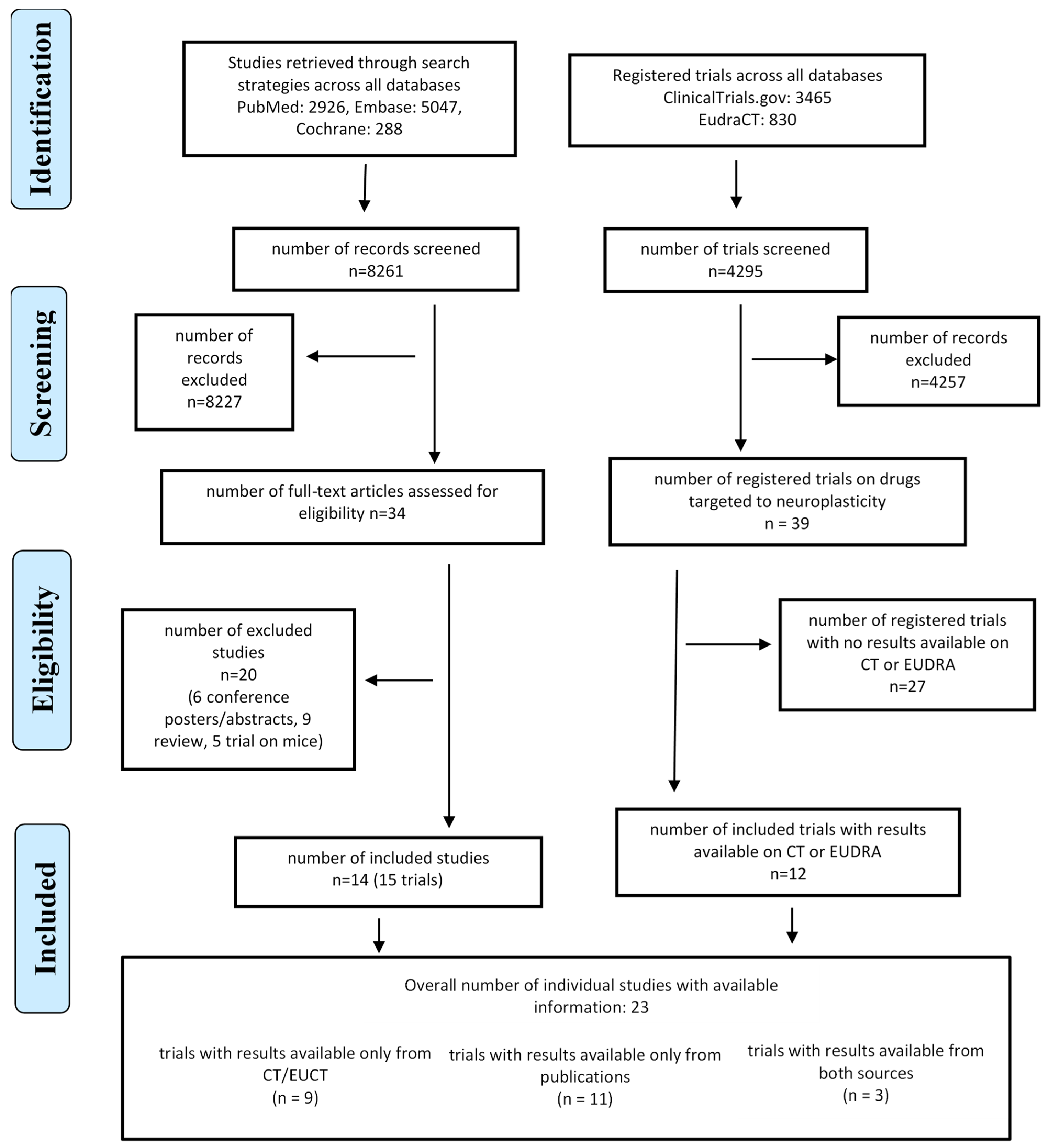
2.2. Search Strategy and Selection Criteria
2.3. Study Selection
2.4. Data Extraction and Quality Assessment
2.5. Data Synthesis and Analysis
3. Results
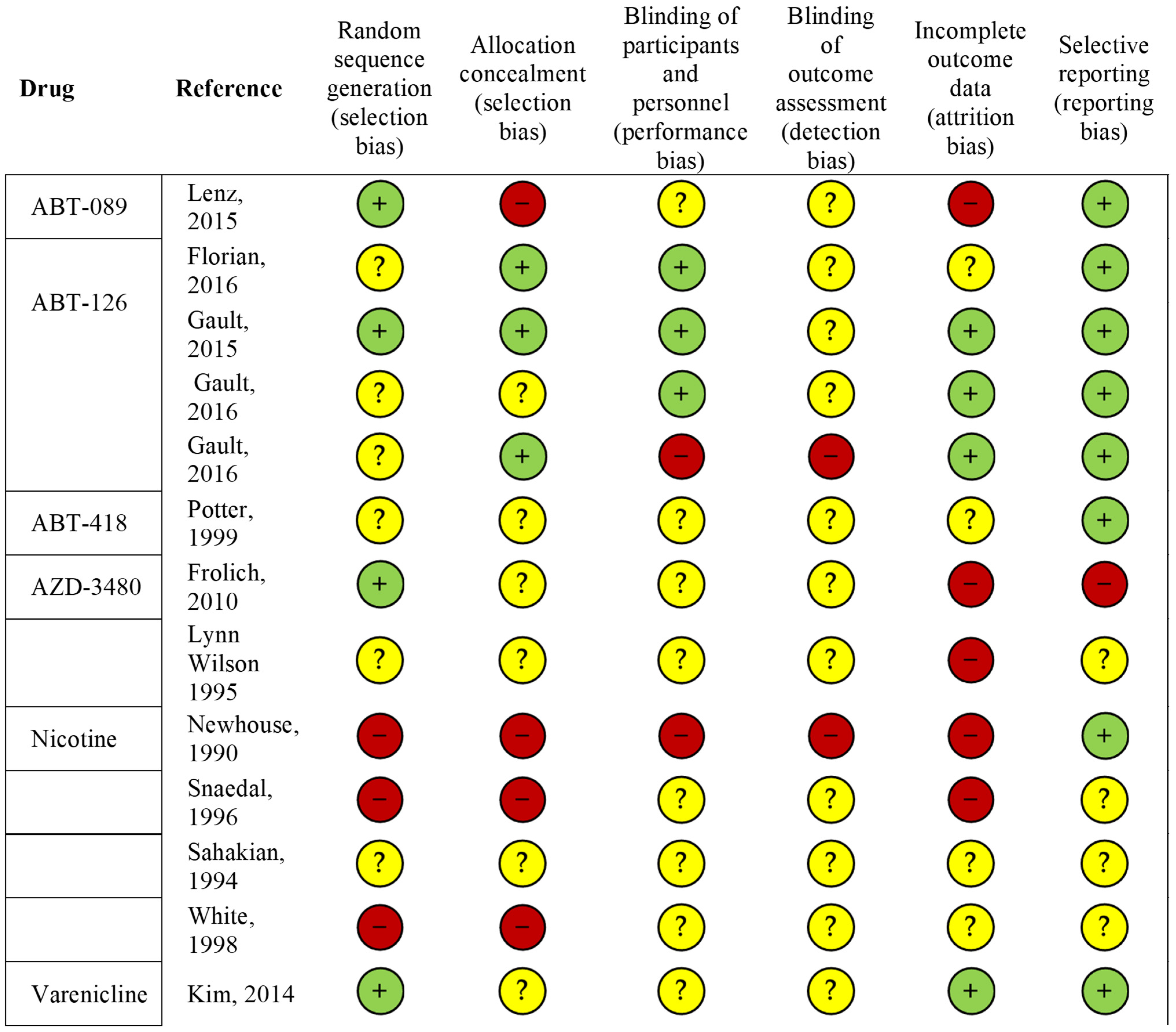
3.1. Methodological Quality of Published Studies
3.2. Drug Mechanisms of Action
3.3. Safety
3.4. Efficacy
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Hebert, L.E.; Weuve, J.; Scherr, P.A.; Evans, D.A. Alzheimer disease in the United States (2010–2050) estimated using the 2010 census. Neurology 2013, 80, 1778–1783. [Google Scholar] [CrossRef]
- Scheltens, P.; De Strooper, B.; Kivipelto, M.; Holstege, H.; Chételat, G.; Teunissen, C.E.; Cummings, J.; van der Flier, W.M. Alzheimer’s disease. Lancet 2021, 397, 1577–1590. [Google Scholar] [CrossRef]
- Beason-Held, L.L.; Goh, J.O.; An, Y.; Kraut, M.A.; O’Brien, R.J.; Ferrucci, L.; Resnick, S.M. Changes in Brain Function Occur Years before the Onset of Cognitive Impairment. J. Neurosci. 2013, 33, 18008–18014. [Google Scholar] [CrossRef]
- Drachman, D.A.; Noffsinger, D.; Sahakian, B.J.; Kurdziel, S.; Fleming, P. Aging, memory, and the cholinergic system: A study of dichotic listening. Neurobiol. Aging 1980, 1, 39–43. [Google Scholar] [CrossRef]
- Bartus, R.T.; Dean, R.L.; Beer, B.; Lippa, A.S. The Cholinergic Hypothesis of Geriatric Memory Dysfunction. Science 1982, 217, 408–417. [Google Scholar] [CrossRef] [PubMed]
- Dou, K.X.; Tan, M.S.; Tan, C.C.; Cao, X.P.; Hou, X.H.; Guo, Q.H.; Tan, L.; Mok, V.; Yu, J.T. Comparative safety and effectiveness of cholinesterase inhibitors and memantine for Alzheimer’s disease: A network meta-analysis of 41 randomized controlled trials. Alzheimer’s Res. Ther. 2018, 10, 126. [Google Scholar] [CrossRef] [PubMed]
- Henderson, B.J.; Lester, H.A. Inside-out neuropharmacology of nicotinic drugs. Neuropharmacology 2015, 96, 178–193. [Google Scholar] [CrossRef]
- Grady, S.R.; Salminen, O.; Laverty, D.C.; Whiteaker, P.; McIntosh, J.M.; Collins, A.C.; Marks, M.J. The Subtypes of Nicotinic Acetylcholine Receptors on Dopaminergic Terminals of Mouse Striatum. Biochem. Pharmacol. 2007, 74, 1235. [Google Scholar] [CrossRef] [PubMed]
- Bertrand, D.; Terry, A.V. The wonderland of neuronal nicotinic acetylcholine receptors. Biochem. Pharmacol. 2018, 151, 214–225. [Google Scholar] [CrossRef]
- Gay, E.A.; Yakel, J.L. Gating of nicotinic ACh receptors; new insights into structural transitions triggered by agonist binding that induce channel opening. J. Physiol. 2007, 584, 727. [Google Scholar] [CrossRef]
- Millar, N.S. RIC-3: A nicotinic acetylcholine receptor chaperone. Br. J. Pharmacol. 2008, 153, S177–S183. [Google Scholar] [CrossRef]
- Terry, A.V.; Jones, K.; Bertrand, D. Nicotinic acetylcholine receptors in neurological and psychiatric diseases. Pharmacol. Res. 2023, 191, 106764. [Google Scholar] [CrossRef]
- Shimohama, S.; Taniguchi, T.; Fujiwara, M.; Kameyama, M. Biochemical Characterization of α-Adrenergic Receptors in Human Brain and Changes in Alzheimer-Type Dementia. J. Neurochem. 1986, 47, 1294–1301. [Google Scholar] [CrossRef]
- Court, J.A.; Piggott, M.A.; Lloyd, S.; Cookson, N.; Ballard, C.G.; McKeith, I.G.; Perry, R.H.; Perry, E.K. Nicotine binding in human striatum: Elevation in schizophrenia and reductions in dementia with Lewy bodies, Parkinson’s disease and Alzheimer’s disease and in relation to neuroleptic medication. Neuroscience 2000, 98, 79–87. [Google Scholar] [CrossRef]
- Paterson, D.; Nordberg, A. Neuronal nicotinic receptors in the human brain. Prog. Neurobiol. 2000, 61, 75–111. [Google Scholar] [CrossRef] [PubMed]
- Picciotto, M.R.; Caldarone, B.J.; Brunzell, D.H.; Zachariou, V.; Stevens, T.R.; King, S.L. Neuronal nicotinic acetylcholine receptor subunit knockout mice: Physiological and behavioral phenotypes and possible clinical implications. Pharmacol. Ther. 2001, 92, 89–108. [Google Scholar] [CrossRef]
- Sher, E.; Chen, Y.; Sharples, T.J.W.; Broad, L.M.; Benedetti, G.; Zwart, R.; McPhie, G.I.; Pearson, K.H.; Baldwinson, T.; De Filippi, G. Physiological Roles of Neuronal Nicotinic Receptors Subtypes: New Insights on the Nicotinic Modulation of Neurotransmitter Release, Synaptic Transmission and Plasticity. Curr. Top. Med. Chem. 2005, 4, 283–297. [Google Scholar] [CrossRef] [PubMed]
- Leanza, G.; Muir, J.; Nilsson, O.G.; Wiley, R.G.; Dunnett, S.B.; Björklund, A. Selective Immunolesioning of the Basal Forebrain Cholinergic System Disrupts Short-term Memory in Rats. Eur. J. Neurosci. 1996, 8, 1535–1544. [Google Scholar] [CrossRef]
- Guan, Z.Z.; Zhang, X.; Ravid, R.; Nordberg, A. Decreased Protein Levels of Nicotinic Receptor Subunits in the Hippocampus and Temporal Cortex of Patients with Alzheimer’s Disease. J. Neurochem. 2000, 74, 237–243. [Google Scholar] [CrossRef] [PubMed]
- Whitehouse, P.J.; Martino, A.M.; Antuono, P.G.; Lowenstein, P.R.; Coyle, J.T.; Price, D.L.; Kellar, K.J. Nicotinic acetylcholine binding sites in Alzheimer’s disease. Brain Res. 1986, 371, 146–151. [Google Scholar] [CrossRef] [PubMed]
- Kadir, A.; Almkvist, O.; Wall, A.; Långström, B.; Nordberg, A. PET imaging of cortical 11C-nicotine binding correlates with the cognitive function of attention in Alzheimer’s disease. Psychopharmacology 2006, 188, 509–520. [Google Scholar] [CrossRef]
- Sabri, O.; Meyer, P.M.; Gräf, S.; Hesse, S.; Wilke, S.; Becker, G.A.; Rullmann, M.; Patt, M.; Luthardt, J.; Wagenknecht, G.; et al. Cognitive correlates of α4β2 nicotinic acetylcholine receptors in mild Alzheimer’s dementia. Brain 2018, 141, 1840. [Google Scholar] [CrossRef] [PubMed]
- Liu, Q.; Huang, Y.; Xue, F.; Simard, A.; DeChon, J.; Li, G.; Zhang, J.; Lucero, L.; Wang, M.; Sierks, M.; et al. A Novel Nicotinic Acetylcholine Receptor Subtype in Basal Forebrain Cholinergic Neurons with High Sensitivity to Amyloid Peptides. J. Neurosci. 2009, 29, 918. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.Y.; Lee, D.H.S.; D’Andrea, M.R.; Peterson, P.A.; Shank, R.P.; Reitz, A.B. β-Amyloid1–42 Binds to α7 Nicotinic Acetylcholine Receptor with High Affinity: IMPLICATIONS FOR ALZHEIMER’S DISEASE PATHOLOGY. J. Biol. Chem. 2000, 275, 5626–5632. [Google Scholar] [CrossRef] [PubMed]
- Nagele, R.G.; D’Andrea, M.R.; Anderson, W.J.; Wang, H.Y. Intracellular accumulation of β-amyloid1-42 in neurons is facilitated by the α7 nicotinic acetylcholine receptor in Alzheimer’s disease. Neuroscience 2002, 110, 199–211. [Google Scholar] [CrossRef] [PubMed]
- Deutsch, S.I.; Burket, J.A.; Benson, A.D. Targeting the α7 nicotinic acetylcholine receptor to prevent progressive dementia and improve cognition in adults with Down’s syndrome. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 2014, 54, 131–139. [Google Scholar] [CrossRef]
- Ma, K.G.; Qian, Y.H. Alpha 7 nicotinic acetylcholine receptor and its effects on Alzheimer’s disease. Neuropeptides 2019, 73, 96–106. [Google Scholar] [CrossRef] [PubMed]
- Mekli, K.; Lophatananon, A.; Maharani, A.; Nazroo, J.Y.; Muir, K.R. Association between an inflammatory biomarker score and future dementia diagnosis in the population-based UK Biobank cohort of 500,000 people. PLoS ONE 2023, 18, e0288045. [Google Scholar] [CrossRef]
- Benfante, R.; Di Lascio, S.; Cardani, S.; Fornasari, D. Acetylcholinesterase inhibitors targeting the cholinergic anti-inflammatory pathway: A new therapeutic perspective in aging-related disorders. Aging Clin. Exp. Res. 2019, 33, 823–834. [Google Scholar] [CrossRef]
- Pavlov, V.A.; Parrish, W.R.; Rosas-Ballina, M.; Ochani, M.; Puerta, M.; Ochani, K.; Chavan, S.; Al-Abed, Y.; Tracey, K.J. Brain acetylcholinesterase activity controls systemic cytokine levels through the cholinergic anti-inflammatory pathway. Brain. Behav. Immun. 2009, 23, 41–45. [Google Scholar] [CrossRef]
- Piovesana, R.; Intriago, M.S.S.; Dini, L.; Tata, A.M. Cholinergic Modulation of Neuroinflammation: Focus on α7 Nicotinic Receptor. Int. J. Mol. Sci. 2021, 22, 4912. [Google Scholar] [CrossRef]
- De Simone, R.; Ajmone-Cat, M.A.; Carnevale, D.; Minghetti, L. Activation of α7 nicotinic acetylcholine receptor by nicotine selectively up-regulates cyclooxygenase-2 and prostaglandin E2 in rat microglial cultures. J. Neuroinflam. 2005, 2, 4. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. (Eds.) Cochrane Handbook for Systematic Reviews of Interventions Version 6.4 (Updated August 2023). Cochrane. 2023. Available online: www.training.cochrane.org/handbook (accessed on 1 December 2023).
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, 71. [Google Scholar] [CrossRef] [PubMed]
- Newhouse, P.A.; Sunderland, T.; Narang, P.K.; Mellow, A.M.; Fertig, J.B.; Lawlor, B.A.; Murphy, D.L. Neuroendocrine, physiologic, and behavioral responses following intravenous nicotine in nonsmoking healthy volunteers and in pa-tients with alzheimer’s disease. Psychoneuroendocrinology 1990, 15, 471–484. [Google Scholar] [CrossRef] [PubMed]
- Snaedal, J.; Johannesson, T.; Jornson, J.E.; Gylfadottir, G. The effects of nicotine in dermal plaster on cognitive functions in patients with Alzheimer’s disease. Dementia 1996, 7, 47–52. [Google Scholar] [CrossRef]
- Sahakian, B.J.; Coull, J.T. Nicotine and tetrahydroaminoacradine: Evidence for improved attention in patients with dementia of the Alzheimer type. Drug Dev. Res. 1994, 31, 80–88. [Google Scholar] [CrossRef]
- White, A.R.; Resch, K.L.; Ernst, E. Randomized Trial of Acupuncture for Nicotine Withdrawal Symptoms. Arch. Intern. Med. 1998, 158, 2251–2255. [Google Scholar] [CrossRef]
- Potter, A.; Corwin, J.; Lang, J.; Piasecki, M.; Lenox, R.; Newhouse, P.A. Acute effects of the selective cholinergic channel activator (nicotinic agonist) ABT-418 in Alzheimer’s disease. Psychopharmacology 1999, 142, 334–342. [Google Scholar] [CrossRef]
- Newhouse, P.; Kellar, K.; Aisen, P.; White, H.; Wesnes, K.; Coderre, E.; Pfaff, A.; Wilkins, H.; Howard, D.; Levin, E.D. Nicotine treatment of mild cognitive impairment. Neurology 2012, 78, 91–101. [Google Scholar] [CrossRef]
- Kim, S.Y.; Choi, S.H.; Rollema, H.; Schwam, E.M.; McRae, T.; Dubrava, S.; Jacobsen, J. Phase II Crossover Trial of Varenicline in Mild-to-Moderate Alzheimer’s Disease. Dement. Geriatr. Cogn. Disord. 2014, 37, 232–245. [Google Scholar] [CrossRef]
- Lenz, R.A.; Pritchett, Y.L.; Berry, S.M.; Llano, D.A.; Han, S.; Berry, D.A.; Sadowsky, C.H.; Abi-Saab, W.M.; Saltarelli, M.D. Adaptive, Dose-finding Phase 2 Trial Evaluating the Safety and Efficacy of ABT-089 in Mild to Moderate Alzheimer Disease. Alzheimer Dis. Assoc. Disord. 2015, 29, 192–199. [Google Scholar] [CrossRef] [PubMed]
- Florian, H.; Meier, A.; Gauthier, S.; Lipschitz, S.; Lin, Y.; Tang, Q.; Othman, A.A.; Robieson, W.Z.; Gault, L.M. Efficacy and Safety of ABT-126 in Subjects with Mild-to-Moderate Alzheimer’s Disease on Stable Doses of Acetylcholinesterase Inhibitors: A Randomized, Double-Blind, Placebo-Controlled Study. J. Alzheimers. Dis. 2016, 51, 1237–1247. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.Y.; Pei, Z.; Lee, K.C.; Lopez-Brignoni, E.; Nikolov, B.; Crowley, C.A.; Marsman, M.R.; Barbier, R.; Friedmann, N.; Burns, L.H. PTI-125 Reduces Biomarkers of Alzheimer’s Disease in Patients. J. Prev. Alzheimer’s Dis. 2020, 7, 256–264. [Google Scholar] [CrossRef] [PubMed]
- Gault, L.M.; Ritchie, C.W.; Robieson, W.Z.; Pritchett, Y.; Othman, A.A.; Lenz, R.A. A phase 2 randomized, controlled trial of the α7 agonist ABT-126 in mild-to-moderate Alzheimer’s dementia. Alzheimer’s Dement. Transl. Res. Clin. Interv. 2015, 1, 81–90. [Google Scholar] [CrossRef] [PubMed]
- Gault, L.M.; Lenz, R.A.; Ritchie, C.W.; Meier, A.; Othman, A.A.; Tang, Q.; Berry, S.; Pritchett, Y.; Robieson, W.Z. ABT-126 monotherapy in mild-to-moderate Alzheimer’s dementia: Randomized double-blind, placebo and active controlled adaptive trial and open-label extension. Alzheimer’s. Res. Ther. 2016, 8, 44. [Google Scholar] [CrossRef] [PubMed]
- Frölich, L.; Ashwood, T.; Nilsson, J.; Eckerwall, G. Effects of AZD3480 on Cognition in Patients with Mild-to-Moderate Alzheimer’s Disease: A Phase IIb Dose-Finding Study. J. Alzheimer’s Dis. 2011, 24, 363–374. [Google Scholar] [CrossRef] [PubMed]
- Wilson, A.L.; Langley, L.K.; Monley, J.; Bauer, T.; Rottunda, S.; McFalls, E.; Kovera, C.; McCarten, J.R. Nicotine patches in Alzheimer’s disease: Pilot study on learning, memory, and safety. Pharmacol. Biochem. Behav. 1995, 51, 509–514. [Google Scholar] [CrossRef]
- Alhowail, A. Molecular insights into the benefits of nicotine on memory and cognition (Review). Mol. Med. Rep. 2021, 23, 398. [Google Scholar] [CrossRef]
- Unwin, N. Nicotinic acetylcholine receptor and the structural basis of neuromuscular transmission: Insights from Torpedo postsynaptic membranes. Q. Rev. Biophys. 2013, 46, 283–322. [Google Scholar] [CrossRef]
- Broide, R.S.; Winzer-Serhan, U.H.; Chen, Y.; Leslie, F.M. Distribution of α7 Nicotinic Acetylcholine Receptor Subunit mRNA in the Developing Mouse. Front. Neuroanat. 2019, 13, 465985. [Google Scholar] [CrossRef] [PubMed]
- Grossberg, G.T. Cholinesterase Inhibitors for the Treatment of Alzheimer’s Disease:: Getting On and Staying On. Curr. Ther. Res. 2003, 64, 216–235. [Google Scholar] [CrossRef] [PubMed]
- Cheng, Q.; Yakel, J.L. The effect of α7 nicotinic receptor activation on glutamatergic transmission in the hippocampus. Biochem. Pharmacol. 2015, 97, 439–444. [Google Scholar] [CrossRef] [PubMed]
- Giese, K.P.; Mizuno, K. The roles of protein kinases in learning and memory. Learn. Mem. 2013, 20, 540–552. [Google Scholar] [CrossRef] [PubMed]
- Brunet, A.; Datta, S.R.; Greenberg, M.E. Transcription-dependent and -independent control of neuronal survival by the PI3K–Akt signaling pathway. Curr. Opin. Neurobiol. 2001, 11, 297–305. [Google Scholar] [CrossRef] [PubMed]
- Shu, Y.; Zhang, H.; Kang, T.; Zhang, J.J.; Yang, Y.; Liu, H.; Zhang, L. PI3K/Akt Signal Pathway Involved in the Cognitive Impairment Caused by Chronic Cerebral Hypoperfusion in Rats. PLoS ONE 2013, 8, e81901. [Google Scholar] [CrossRef] [PubMed]
- Diez, H.; Garrido, J.J.; Wandosell, F. Specific Roles of Akt iso Forms in Apoptosis and Axon Growth Regulation in Neurons. PLoS ONE 2012, 7, e32715. [Google Scholar] [CrossRef]
- Horwood, J.M.; Dufour, F.; Laroche, S.; Davis, S. Signalling mechanisms mediated by the phosphoinositide 3-kinase/Akt cascade in synaptic plasticity and memory in the rat. Eur. J. Neurosci. 2006, 23, 3375–3384. [Google Scholar] [CrossRef]
- Chiang, H.C.; Wang, L.; Xie, Z.; Yau, A.; Zhong, Y. PI3 kinase signaling is involved in Aβ-induced memory loss in Drosophila. Proc. Natl. Acad. Sci. USA 2010, 107, 7060–7065. [Google Scholar] [CrossRef]
- Yi, J.H.; Baek, S.J.; Heo, S.; Park, H.J.; Kwon, H.; Lee, S.; Jung, J.; Jeon, S.J.; Kim, B.C.; Lee, Y.C.; et al. Direct pharmacological Akt activation rescues Alzheimer’s disease like memory impairments and aberrant synaptic plasticity. Neuropharmacology 2018, 128, 282–292. [Google Scholar] [CrossRef]
- Srivareerat, M.; Tran, T.T.; Salim, S.; Aleisa, A.M.; Alkadhi, K.A. Chronic nicotine restores normal Aβ levels and prevents short-term memory and E-LTP impairment in Aβ rat model of Alzheimer’s disease. Neurobiol. Aging 2011, 32, 834–844. [Google Scholar] [CrossRef]
- Yoshimura, R.; Nakamura, J. [Nicotine dependence and its molecular pharmacology]. Nihon Rinsho. 2013, 71, 473–476. [Google Scholar]
- Tonstad, S.; Arons, C.; Rollema, H.; Berlin, I.; Hajek, P.; Fagerström, K.; Els, C.; McRae, T.; Russ, C. Varenicline: Mode of action, efficacy, safety and accumulated experience salient for clinical populations. Curr. Med. Res. Opin. 2020, 36, 713–730. [Google Scholar] [CrossRef]
- Dani, J.A.; Harris, R.A. Nicotine addiction and comorbidity with alcohol abuse and mental illness. Nat. Neurosci. 2005, 8, 1465–1470. [Google Scholar] [CrossRef]
- Laviolette, S.R.; Van Der Kooy, D. The neurobiology of nicotine addiction: Bridging the gap from molecules to behaviour. Nat. Rev. Neurosci. 2004, 5, 55–65. [Google Scholar] [CrossRef]
- Rollema, H.; Chambers, L.K.; Coe, J.W.; Glowa, J.; Hurst, R.S.; Lebel, L.A.; Lu, Y.; Mansbach, R.S.; Mather, R.J.; Rovetti, C.C.; et al. Pharmacological profile of the α4β2 nicotinic acetylcholine receptor partial agonist varenicline, an effective smoking cessation aid. Neuropharmacology 2007, 52, 985–994. [Google Scholar] [CrossRef]
- Coe, J.W.; Brooks, P.R.; Vetelino, M.G.; Wirtz, M.C.; Arnold, E.P.; Huang, J.; Sands, S.B.; Davis, T.I.; Lebel, L.A.; Fox, C.B.; et al. Varenicline: An alpha;4β2 nicotinic receptor partial agonist for smoking cessation. J. Med. Chem. 2005, 48, 3474–3477. [Google Scholar] [CrossRef]
- Rueter, L.E.; Anderson, D.J.; Briggs, C.A.; Donnelly-Roberts, D.L.; Gintant, G.A.; Gopalakrishnan, M.; Lin, N.H.; Osinski, M.A.; Reinhart, G.A.; Buckley, M.J.; et al. ABT-089: Pharmacological properties of a neuronal nicotinic acetylcholine receptor agonist for the potential treatment of cognitive disorders. CNS Drug Rev. 2004, 10, 167–182. [Google Scholar] [CrossRef]
- Sullivan, J.P.; Donnelly-Roberts, D.; Briggs, C.A.; Anderson, D.J.; Gopalakrishnan, M.; Xue, I.C.; Piattoni-Kaplan, M.; Molinari, E.; Campbell, J.E.; Mckenna, D.G.; et al. ABT-089 [2-Methyl-3-(2-(S)-pyrrolidinylmethoxy)pyridine]: I. A Potent and Selective Cholinergic Channel Modulator with Neuroprotective Properties. J. Pharmacol. Exp. Ther. 1997, 283, 235–246. [Google Scholar] [PubMed]
- Marks, M.J.; Farnham, D.A.; Grady, S.R.; Collins, A.C. Nicotinic receptor function determined by stimulation of rubidium efflux from mouse brain synaptosomes. J. Pharmacol. Exp. Ther. 1993, 264, 542–552. [Google Scholar] [PubMed]
- Decker, M.W.; Bannon, A.W.; Curzon, P.; Gunther, K.L.; Brioni, J.D.; Holladay, M.W.; Lin, N.-H.; Li, Y.; Daanen, J.F.; Buccafusco, J.J.; et al. ABT-089 [2-Methyl-3-(2-(S)-pyrrolidinylmethoxy)pyridine dihydrochloride]: II. A Novel Cholinergic Channel Modulator with Effects on Cognitive Performance in Rats and Monkeys. J. Pharmacol. Exp. Ther. 1997, 283, 247–258. [Google Scholar] [PubMed]
- Dunbar, G.; Boeijinga, P.H.; Demazières, A.; Cisterni, C.; Kuchibhatla, R.; Wesnes, K.; Luthringer, R. Effects of TC-1734 (AZD3480), a selective neuronal nicotinic receptor agonist, on cognitive performance and the EEG of young healthy male volunteers. Psychopharmacology 2007, 191, 919–929. [Google Scholar] [CrossRef]
- Obinu, M.C.; Reibaud, M.; Miquet, J.M.; Pasquet, M.; Rooney, T. Brain-selective stimulation of nicotinic receptors by TC-1734 enhances ACh transmission from frontoparietal cortex and memory in rodents. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 2002, 26, 913–918. [Google Scholar] [CrossRef] [PubMed]
- Gatto, G.J.; Bohme, G.A.; Caldwell, W.S.; Letchworth, S.R.; Traina, V.M.; Obinu, M.C.; Laville, M.; Reibaud, M.; Pradier, L.; Dunbar, G.; et al. TC-1734: An orally active neuronal nicotinic acetylcholine receptor modulator with antidepressant, neuroprotective and long-lasting cognitive effects. CNS Drug Rev. 2004, 10, 147–166. [Google Scholar] [CrossRef]
- Bitner, R.; Anderson, D.; Drescher, K.; Kohlhaas, K.; Gronlien, H.; Hu, M.; Li, J.; Markosyan, S.; Marsh, K.; Mohler, E.; et al. P4–310: Preclinical characterization of a selective alpha-7 neuronal nicotinic acetylcholine receptor agonist ABT-126: A novel therapeutic agent for the treatment of cognitive impairment in Alzheimer’s disease and schizophrenia. Alzheimer’s Dement. 2013, 9, P817–P818. [Google Scholar] [CrossRef]
- Damaj, M.I.; Creasy, K.R.; Welch, S.P.; Rosecrans, J.A.; Aceto, M.D.; Martin, B.R. Comparative pharmacology of nicotine and ABT-418, a new nicotinic agonist. Psychopharmacology 1995, 120, 483–490. [Google Scholar] [CrossRef] [PubMed]
- Arneric, S.P.; Sullivan, J.P.; Briggs, C.A.; Donnelly-Roberts, D.; Anderson, D.J.; Raszkiewicz, J.L.; Hughes, M.L.; Cadman, E.D.; Adams, P.; Garvey, D.S.; et al. (S)-3-methyl-5-(1-methyl-2-pyrrolidinyl) isoxazole (ABT 418): A novel cholinergic ligand with cognition-enhancing and anxiolytic activities: I. In vitro characterization. J. Pharmacol. Exp. Ther. 1994, 270, 310–318. [Google Scholar]
- Decker, M.W.; Brioni, J.D.; Sullivan, J.P.; Buckley, M.J.; Radek, R.J.; Raszkiewicz, J.L.; Kang, C.H.; Kim, D.J.; Giardina, W.J.; Wasicak, J.T. (S)-3-methyl-5-(1-methyl-2-pyrrolidinyl)isoxazole (ABT 418): A novel cholinergic ligand with cognition-enhancing and anxiolytic activities: II. In vivo characterization. J. Pharmacol. Exp. Ther. 1994, 270, 319–328. [Google Scholar]
- Wang, H.Y.; Bakshi, K.; Frankfurt, M.; Stucky, A.; Goberdhan, M.; Shah, S.M.; Burns, L.H. Reducing Amyloid-Related Alzheimer’s Disease Pathogenesis by a Small Molecule Targeting Filamin A. J. Neurosci. 2012, 32, 9773–9784. [Google Scholar] [CrossRef]
- Wang, H.Y.; Lee, K.C.; Pei, Z.; Khan, A.; Bakshi, K.; Burns, L.H. PTI-125 binds and reverses an altered conformation of filamin A to reduce Alzheimer’s disease pathogenesis. Neurobiol. Aging 2017, 55, 99–114. [Google Scholar] [CrossRef]
- Dunbar, G.C.; Kuchibhatla, R.V.; Lee, G. A randomized double-blind study comparing 25 and 50 mg TC-1734 (AZD3480) with placebo, in older subjects with age-associated memory impairment. J. Psychopharmacol. 2011, 25, 1020–1029. [Google Scholar] [CrossRef]
- Wang, H.-Y.; Bakshi, K.; Frankfurt, M.; Stucky, A.; Goberdhan, M.; Shah, S.M.; Burns, L.H. Reducing Amyloid-Related Alzheimer’s Disease Pathogenesis by a Small Molecule Targeting Filamin A. J. Neurosci. 2012, 32, 9773–9784, Erratum in J. Neurosci. 2022, 42, 529. [Google Scholar] [CrossRef]
- Salardini, A. An Overview of Primary Dementias as Clinicopathological Entities. Semin. Neurol. 2019, 39, 153–166. [Google Scholar] [CrossRef]
- Fleisher, A.S.; Sowell, B.B.; Taylor, C.; Gamst, A.C.; Petersen, R.C.; Thal, L.J. Clinical predictors of progression to Alzheimer disease in amnestic mild cognitive impairment. Neurology 2007, 68, 1588–1595. [Google Scholar] [CrossRef]
- Bai, W.; Chen, P.; Cai, H.; Zhang, Q.; Su, Z.; Cheung, T.; Jackson, T.; Sha, S.; Xiang, Y.T. Worldwide prevalence of mild cognitive impairment among community dwellers aged 50 years and older: A meta-analysis and systematic review of epidemiology studies. Age Ageing 2022, 51, afac173. [Google Scholar] [CrossRef]
- Lacorte, E.; Ancidoni, A.; Zaccaria, V.; Remoli, G.; Tariciotti, L.; Bellomo, G.; Sciancalepore, F.; Corbo, M.; Lombardo, F.L.; Bacigalupo, I.; et al. Safety and Efficacy of Monoclonal Antibodies for Alzheimer’s Disease: A Systematic Review and Meta-Analysis of Published and Unpublished Clinical Trials. J. Alzheimer’s Dis. 2022, 87, 101–129. [Google Scholar] [CrossRef]
- Piscopo, P.; Crestini, A.; Carbone, E.; Rivabene, R.; Ancidoni, A.; Lo Giudice, M.; Corbo, M.; Vanacore, N.; Lacorte, E. A systematic review on drugs for synaptic plasticity in the treatment of dementia. Ageing Res. Rev. 2022, 81, 101726. [Google Scholar] [CrossRef] [PubMed]
- Buccafusco, J.J.; Beach, J.W.; Terry, A.V. Desensitization of nicotinic acetylcholine receptors as a strategy for drug development. J. Pharmacol. Exp. Ther. 2009, 328, 364–370. [Google Scholar] [CrossRef] [PubMed]
- Buisson, B.; Bertrand, D. Open-Channel Blockers at the Human α4β2 Neuronal Nicotinic Acetylcholine Receptor. Mol. Pharmacol. 1998, 53, 555–563. [Google Scholar] [CrossRef] [PubMed]
- Buisson, B.; Bertrand, D. Chronic exposure to nicotine upregulates the human (alpha)4((beta)2 nicotinic acetylcholine receptor function. J. Neurosci. 2001, 21, 1819–1829. [Google Scholar] [CrossRef]
- Burns, L.H.; Pei, Z.; Wang, H. Targeting α7 nicotinic acetylcholine receptors and their protein interactions in Alzheimer’s disease drug development. Drug Dev. Res. 2023, 84, 1085–1095. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Identifier | Intervention | Duration | Placebo | Estimated Enrollment (Participants) | Age (Years) | Diagnosis | MMSE at Baseline | Primary Outcome | Secondary Outcome | Status |
|---|---|---|---|---|---|---|---|---|---|---|
| 1 NCT02720445 Phase 2 | Nicotine Transdermal Patch | FP: 2016 LUP: 2023 | Y | 380 | 55–90 | MCI | 24–30 | Conners’ Continuous Performance Task (CPT) | MCI-CGIC, CBB, NYU Paragraph Recall, CDR-SOB, GDS, ADCS-ADL, OASR/OABCL, CSF Biomarkers, vMRI | Recruiting, No Study Results |
| 2 NCT00091468 Phase 1 | Nicotine Transdermal Patch | FP: 2004 LUP: 2008 | Y | 75 | 55–90 | MCI | 24–30 | Safety | Cognitive performance, global function | Unknown, No Study Results |
| 3 NCT03865121 Phase2 | Nicotine Transnasal | FP: 2019 LUP: 2019 | N | 6 | >60 | PD | / | MDS-UPDRS | Efficacy, MDS-UPDRS | Completed, No Study Results |
| 4 NCT01560754 Phase 2 | Nicotine Transdermal | FP: 2012 LUP: 2015 | Y | 160 | >30 | Early PD | / | UPDRS I-III | UPDRS I-III, (PDQ-8), AEs, SCOPA-COG, BDI-II, PDSS | Unknown, Results Submitted |
| 5 NCT00744978 Phase 2 | Varenicline | FP: 2008 LUP: 2011 | Y | 66 | 55–85 | Mild-to-moderate AD | 14–26 | ADAS-Cog 75 | ADAS-Cog 75, ADAS-Cog 70, CGI-I, NPI, CogState, CPAL, | Completed, With Results |
| 6 NCT00414622 Phase 2 | GTS-21 (DMXB-A) | FP: 2006 LUP: 2007 | Y | 60 | 50–80 | AD | / | CDR | ADAS-Cog | Completed, Results Submitted |
| 7 NCT02246075 Phase 2 | EVP-6124/memantine encenicline | FP: 2014 LUP: 2015 | Y | 0 | 55–85 | AD, dementia cognition | 12–26 | Safety, tolerability | MMSE | Withdrawn (Forum has decided not to proceed with this study at this time.) |
| 8 NCT00766363 Phase 2 | EVP-6124 | FP: 2011 LUP: 2012 | Y | 49 | 50–90 | Mild-to-moderate AD | 18–26 | Safety and tolerability | PK | Completed, With Results |
| 9 NCT01073228 Phase 2 | EVP-6124 | FP: 2010 LUP: 2014 | Y | 409 | 50–85 | Mild-to-moderate AD | 14–24 | ADAS-cog-13 Time Frame: Day -7 | ADAS-cog-13 Time Frame: Day—4, Controlled Oral Word Association TEìest, Clinical Dementia Rating Scale Sum of Boxes, Alzheimer’s Disease Cooperative Study-Activities of Daily Living, NPI, MMSE | Completed, No Study Results |
| 10 NCT02004392 Phase 3 | EVP-6124 | FP: 2013 LUP: 2016 | Y | 348 | 55–85 | AD, dementia | / | Safety | MMSE, NPI, EQ-5D, RUD-Lite 3.3, ZBI | Terminated (Study has been suspended due to clinical hold.) |
| 11 NCT01969123 Phase 3 Eudra: 2013-002618-10 | EVP-6124 | FP: 2013 LUP: 2016 | Y | 474 | 55–85 | AD, dementia | 14–24 | ADAS-Cog-13, CDR-SB, safety, tolerability | DAD, NPI, MMSE, COWAT | Terminated (Study has been suspended due to clinical hold.) |
| 12 NCT01969136 Phase 3 Eudra: 2013-002653-30 | EVP-6124 | FP: 2013 LUP: 2016 | Y | 403 | 55–85 | AD, dementia | 14–24 | ADAS-Cog-13, CDR-SB, safety, tolerability | DAD, NPI, MMSE, COWAT | Terminated (Study has been suspended due to clinical hold.) |
| 13 NCT00809510 Phase 2 Non-Randomized Open-Label | ABT-089 Pozanicline | FP: 2008 LUP: 2011 | N | 63 | 55–90 | AD | / | Safety | ADAS-Cog, MMSE, QoL-AD, CIBIC-Plus | Terminated |
| 14 NCT00555204 Phase 2 | ABT-089 | FP: 2007 LUP: 2011 | Y | 337 | 55–90 | AD | 12–26 | Safety and tolerability | PK, PD | Terminated |
| 15 NCT00069849 Phase 2 | ABT-089 | FP: 2003 LUP: 2006 | N | 64 | 50–85 | AD | 12–26 | MMSE | / | Terminated |
| 16 NCT01676935 Phase 2 Open-label Eudra: 2011-004780-75 | ABT-126 Nelonicline | FP: 2012 LUP: 2021 | N | 349 | 55–90 | AD | / | AE, laboratory data, vital signs, physical examinations, brief neurological and psychiatric assessments, Columbia-Suicide Severity Rating Scale, Cornell Scale for Depression in Dementia, electrocardiogram | / | Terminated (Data obtained from the M11-427 study are not critical to the continued evaluation of ABT-126.) |
| 17 NCT01690195 Phase 2 Open-label Eudra: 2012-000537-39 | ABT-126 | FP: 2012 LUP: 2021 | N | 343 | 55–90 | AD | / | AE, laboratory data, vital signs, physical examinations, brief neurological and psychiatric assessments, Columbia-Suicide Severity Rating Scale, Cornell Scale for Depression in Dementia, electrocardiogram | / | Terminated |
| 18 NCT01549834 Phase 2 Eudra: 2011-004849-40 | ABT-126 | FP: 2012 LUP: 2014 | Y | 434 | 55–90 | AD | 12–24 | MMSE, ADCS-ADL, DEMQOL, CIBIC-plus, NPI, PPQSA, RUD-Lite, EuroQol-5D Questionnaires WMS-III, working memory index | / | Completed |
| 19 NCT01527916 Phase 2 Eudra: 2011-002004-32 | ABT-126 | FP: 2012 LUP: 2014 | Y | 438 | 55–90 | AD | 10–24 | ADAS-Cog | ADCS-ADL, DEMQOL, CIBIC-plus, NPI, MMSE, PPQSA, WMS-III, EuroQol-5D Questionnaires | Completed |
| 20 NCT00948909 Phase 2 Eudra: 2009-011424-64 | ABT-126/Donepezil | FP: 2009 LUP: 2013 | Y | 274 | 55–90 | AD | 10–24 | ADAS-Cog | ADCS-ADL, MMSE, QoL-AD, CIBIC-plus, NPI, CSDD, ADAS-Cog | Completed |
| 21 NCT01764243 Phase 2 | MT-4666 | FP: 2013 LUP: 2015 | Y | 450 | 50–85 | Probable AD | 10–24 | ADAS-cog-13 | CDR-SB, ADCS-ADL, ADAS-cog-11, MMSE, NPI, Modified Crichton Scale | Completed, No Results |
| 22 NCT02327182 Phase 3 | MT-4666 | FP: 2014 LUP: 2015 | N | 117 | 55–85 | AD | 14–24 | Safety | MMSE, NPI | Terminated (This study was terminated due to the benefit–risk balance of MT-4666.) |
| 23 NCT01466088 Phase 2 Eudra: 2011-000487-10 | AZD3480/Donepezil | FP: 2011 LUP: 2015 | N | 386 | 60–85 | AD | 12–22 | ADAS-Cog, CIBIC+, ADCS-ADL | NPI, MMSE, ADRQL | Completed, No Study Results |
| 24 NCT00501111 Phase 2 Eudra: 2007-000835-24 | AZD3480/Donepezil | FP: 2007 LUP: 2014 | Y | 659 | 60–85 | AD | / | ADAS-Cog | CDR, MMSE, ADCS-CGIC | Completed, Results Submitted |
| 25 NCT04079803 Phase 2 | PTI-125 | FP: 2020 LUP: 2023 | Y | 64 | 50–85 | Mild-to-moderate AD | 16–26 | Change from baseline in CSF Abeta42, Total Tau, P-tau181, Neurogranin, Neurofilament Light Chain, YKL-40 | Cognitive test assessing episodic memory, Cognitive assessment of spatial working memory, CSF IL-6, sTREM2, HMGB1, Albumin, IgG | Completed, With Results |
| 26 NCT04388254 Phase 2 | PTI-125 | FP: 2020 LUP: 2023 | N | 200 | 50–85 | Mild-to-moderate AD | 16–26 | Change from baseline in CSF P-tau, Total Tau, Abeta42, Neurofilament Light Chain, Neurogranin, YKL-40, Soluble TREM2 and HMGB1 | NPI, Change from baseline in Total Tau, P-tau, Abeta42, P-tau181, Neurofilament Light Chain, Neurogranin, YKL-40, Soluble TREM2 and HMGB1 during open-label period, Cerebrospinal fluid biomarkers of AD | Active, Not Recruiting, No Study Results |
| 27 NCT05026177 Phase 3 | PTI-125 REFOCUS-ALZ | FP: 2021 LUP: 2023 | Y | 1083 | 50–87 | AD | 16–27 | ADAS-Cog12, ADCS-ADL | iADRS, NPI, MMSE, CDR-SB, ZBI, CSF Neurogranin, Neurofilament Light Chain, Total Tau, P-tau181, Soluble triggering receptor expressed on myeloid cells 2 (sTREM2), and Aβ1-42, MRI, amyloid and tau PET, Plasma biomarkers P-tau181 and Neurofilament Light Chain, Plasma biomarker SavaDx | Recruiting, No Study Results |
| 28 NCT05575076 Phase 3 Open-label | PTI-125 | FP: 2022 LUP: 2023 | N | 1600 | 51–89 | AD | / | AE | / | Enrollment By Invitation, No Study Results |
| 29 NCT04994483 Phase 3 | PTI-125 RETHINK-ALZ | FP: 2021 | Y | 750 | 50–87 | Mild-to-moderate AD | 16–27 | ADAS-Cog 22 items | Change from baseline in iADRS, NPI, MMSE, CDR-SB, ZBI, Plasma phospho-tau181 and/or phospho-tau217, Neurofilament Light Chain, Plasma SavaDx biomarker (to detect altered filamin A) | Active, Not Recruiting, No Study Results |
| 30 NCT03748706 Phase 2 Open-label | PTI-125 Simufilan | FP: 2018 LUP: 2021 | N | 13 | 50–85 | AD | 16–24 | Cmax, Tmax, Clast, Tlast, AUClast, Plasma half-life | CSF Biomarkers, SavaDx Biomarker | Completed, With Results |
| 31 NCT00001933 Phase 2 | Nefiracetam | FP: 1999 LUP: 2008 | Y | 50 | Child, Adult, Older Adult | AD | 12–25 | Efficacy, safety, tolerability | Nefiracetam enhances the activity of nicotinic acetylcholine receptors by interacting with a protein kinase C pathway and accelerates acetylcholine turnover and release. Efficacy in patients with mild-to-moderate dementia will be assessed through application of standardized neuropsychological test instruments | Completed, No Study Results |
| 32 NCT00884507 Phase 2 Eudra: 2008-004012-13 | RO5313534/Donepezil MEM3454 | FP: 2009 LUP: 2016 | Y | 389 | >50 | AD | 13–22 | ADAS-Cog | CANTAB tests, MMSE total score, ADCS CGIC, Behave-AD-FW, ADCS-ADL, Zarit Burden interview, AEs, lab parameters, suicidal risk, concomitant medications, physical and neurological examinations | Completed, No Study Results |
| 33 NCT00454870 Phase 2 | RO5313534 | FP: 2007 LUP: 2008 | Y | 80 | 50–80 | AD | 16–26 | Safety, efficacy, PK, tolerability | / | Completed, No Study Results |
| 34 NCT00602680 Phase 2 EUDRA: 2007-001639-80 | SSR180711C/Donepezil | FP: 2008 LUP: 2009 | Y | 1 | 55–90 | AD | / | Change in cognitive performance | Cognitive, global, function and behavioral assessments | Terminated (Insufficient expected benefit–risk balance), No Study Results |
| 35 NCT01039701 Phase 2 EUDRA: 2009-015525-37 | AZD1446/Donepezil | FP: 2009 LUP: 2010 | Y | 99 | 60–85 | Mild-to-moderate AD | / | AEs | PK of AZD1446 as an add-on treatment to donepezil in AD patients, effects of three-dose regimens of AZD1446 compared to placebo as an add-on treatment to donepezil on changes in global functioning using ADCS-CGIC | Completed, Results Submitted |
| 36 NCT01125683 Phase 2 EUDRA: 2010-018273-38 | AZD1446/Donepezil | FP: 2010 LUP: 2011 | Y | 40 | 55–85 | AD | 18–24 | Effect of single and multiple dosing of AZD1446 and a single dose of donepezil on quantified qEEG and ERP in patients with mild-to-moderate AD | Measure the relationship between plasma concentration of AZD1446/donepezil and qEEG and ERP, evaluate the correlation between changes in qEEG/ERP and changes in Cognition, Safety, AEs, Vital Signs, ECG, Clinical Chemistry, Hematology, Urinalysis and Physical Examination | Terminated (Poor recruitment), Results Submitted |
| 37 NCT01254448 Phase 1 | TC-5619 | FP: 2010 LUP: 2013 | Y | 38 | 55–80 | AD | 12–22 | AEs, safety and tolerability | PK, Markers of inflammation in cerebrospinal fluid and plasma | Completed, No Study Results |
| 38 NCT00582855 Phase 2 EUDRA: 2007-001846-42 | AQW051 | FP: 2007 LUP: 2016 | Y | 54 | 55–85 | Mild AD, aMCI | / | Validated computerized cognitive assessment scores | ADAS-Cog, Quality of Life-Alzheimer Disease Scale and the Disability Assessment for Dementia Scale | Terminated, No Study Results |
| 39 NCT04810104 Phase 2 EUDRA: 2019-002423-15 | AZD0328 | FP: 2021 LUP: 2022 | Y | 0 | 50–80 | PD with MCI | / | Attentional Intensity Index | Attentional Intensity Index, Sustained Attention Index, Working Memory Index, Episodic Memory Index, Memory Speed Retrieval Index, MoCA, MDS-UPDRS Part III, Non-Motor Symptom Scale, MCI-CGIC, HADS, AEs, SAEs, ECG | Withdrawn Due To COVID-19 |
| Reference | Study Design | Study Population | Diagnostic Criteria | Objective(s) | Treatment Duration | Intervention | AEs/SAEs | Number of Dropouts | Efficacy Results |
|---|---|---|---|---|---|---|---|---|---|
| ND | |||||||||
| Newhouse et al., 1990 [35] | A single-blind investigation | 11 nonsmoking AD patients (7 F, 4 M; age 58–80; mean age 65.9 + 8.3) | DSM-III-R criteria (American Psychiatric Association, 1987), NINCDS-ADRDA, Global Deterioration Scale | Neurohormonal and behavioral responses to intravenous (IV) nicotine | 60 min | Nicotine 0.125, 0.25 and 0.5 I.tg/kg/min and placebo (the equivalent volume of 0.9% saline) | / | / | Anxiety self-ratings vs. placebo (p = 0.004) after the 0.5 μg dose at +30 min (p < 0.01) and +60 rain (p < 0.05) after 0.25 μg (p < 0.05) +60 min intragroup (p = 0.008) 0.5 and 0.25 μg doses. NIMH Self-Rating Scale (p < 0.05). VAS scale, the anxiety (p < 0.05) intergroup vs. placebo 0.25 μg (+30 min) 0.5 μg (+30 and 60 min) |
| Snaedal et al., 1996 [36] | Placebo-controlled, double-blind study with a cross-over design | 24 subjects with probable AD (mean age 80.4 ± 6.2) | NINCDS-ADRDA, MMSE 12–28 | Effects of nicotine transdermal patch on cognitive functions | 4 weeks + 2-week washout | Nicotine dermal plasters 21 mg | 2 AEs in intervention group | 3 dropouts | RAVLT intergroup vs. placebo: p < 0.05, short-term memory placebo vs. intervention p < 0.01 |
| Sahakian et al., 1994 [37] | Single-blind, placebo-controlled study | 22 subjects with probable AD, 24 normal elderly subjects | NINCDS-ADRDA for AD, CDRS | Effects of three acute doses of nicotine (0.4, 0.6, 0.8 mg) administered to participants with AD and normal controls | 40 min | (1) Subcutaneous nicotine 0.4 mg; (2) Subcutaneous nicotine 0.6 mg; (3) Subcutaneous nicotine 0.8 mg; (4) Placebo. | / | / | RVIP intergroup treatment vs. placebo: p < 0.001, intergroup 0.4 mg vs. placebo p > 0.05, DRMLO intergroup intervention vs. placebo p < 0.02 |
| White et al., 1998 [38] | Placebo-controlled, double-blind cross-over study | 8 subjects with mild-to-moderate AD | NINCDS-ADRDA, CDR | Effects of nicotine patch on cognitive performance | 4 weeks + 2-week washout | (1) Nicotine patch 5 mg; (2) Nicotine patch 10 mg; (3) Placebo. | / | 2 dropouts | ADAS-cognitive placebo: 23 ± 4.3 nicotine 22.5 ± 3.8 p = 0.65, ADAS-non-cognitive placebo 4.8 ± 1.7 nicotine 4.8 ± 1.2 p = 0.92, PDS placebo 108.5 ± 16.9, nicotine 106.4 ± 12.0 p = 0.71, ADLs placebo 9.8 ± 1.6 nicotine 9.9 ± 1.5 p = 0.95, IADLs placebo 22.6 ± 2.2 nicotine 22.2 ± 1.9 p = 0.56, CGI-caregiver placebo 4.0 ± 0.3 nicotine 3.8 ± 0.2 p = 0.1, CGI-physician placebo 4.0 ± 0.2 nicotine placebo 3.9 ± 0.1 p = 0.38, Simple reaction time placebo 923 ± 164 nicotine 748 ± 86 p = 0.17, Choice reaction time placebo 997 ± 169 nicotine 1024 ± 178 p = 0.82, Spatial processing placebo 4543 ± 675 nicotine 4746 ± 438 p = 0.60, Delayed matching placebo 51.5 ± 8.2 nicotine 49.5 ± 4.8 p = 0.69, Stroop color and word test placebo −1.1 ± 1.4 nicotine 0.5 ± 1.4 p = 0.22, Sternberg memory test placebo 54.7 ± 2.9 nicotine 58.5 ± 4.9 p = 0.18, Digit span placebo 11.4 ± 1.6 nicotine 10.7 ± 1.6 p = 0.14. ADAS-cognitive intergroup −0.5 (0.5), ADAS-non-cognitive 0 (0.5), PDS placebo −2.1 (4.9), ADLs 0.1 (0.1) 9.8, IADLs −0.4 (0.3), CGI-caregiver −0.2 (0.1), CGI-physician placebo −0.1 (0.1), Simple reaction time placebo −175 (11), Choice reaction time placebo 27 (11), Spatial processing placebo 203 (237), Delayed matching placebo −2 (4.6), Stroop color and word test 1.6, Sternberg memory test placebo 4.2 (2.0), Digit span placebo −0.7. Composite attention nicotine administration p < 0.025. The subjects’ scores rose from 1.19 ± 0.47 (mean ± SEM) with placebo to 1.55 ± 0.47 with nicotine. Nicotine-induced decline in the response bias measure p < 0.07. |
| Potter et al., 1999 [39] | Double-blind, within-subjects, repeated-measures design | 6 subjects with probable AD (Gender: N.D.; Mean age: 72.7 ± 10.7) | NINDS-ADRDA criteria MMSE: 21.4 ± 3.0 Mean global deterioration: 3.2 | SRT, RAT, SMT, CPT, Psychomotor ability, SAV | 4 days | (1) Placebo; (2) ABT-418 6 mg; (3) ABT-418 12 mg; (4) ABT-418 23 mg. Four dosing days, each separated by 48 h. Drug or placebo administered continuously for 6 h | Not reported | None | SRT: Placebo = −3.8 ABT-418 6 mg = −1.0 ABT-418 12 mg = +0.5 ABT-418 23 mg = +2.8 p < 0.05 vs. placebo SRT recall failure: Placebo = +4.5 ABT-418 6 mg = −2.0 ABT-418 12 mg = −0.3 ABT-418 23 mg = −2.7 SMT: Placebo = −5.67 ABT-418 6 mg = −4.17 ABT-418 12 mg = +0.33 ABT-418 23 mg = +1.33 RAT: Placebo = +2.34 ABT-418 6 mg = −4.50 ABT-418 12 mg = +1.23 ABT-418 23 mg = −2.33 CPT: Placebo = −0.018 ABT-418 6 mg = −0.027 ABT-418 12 mg = −0.084 ABT-418 23 mg = −0.075 SAV anxiety: Placebo = +2.5 ABT-418 6 mg = −13.67 ABT-418 12 mg = −3.17 ABT-418 23 mg = −6.67 SAV fear: Placebo = +8.5 ABT-4186 mg = +9.5 ABT-418 12 mg = +9.34 ABT-418 23 mg = −4.67 |
| Phase I | |||||||||
| Newhouse et al., 2012 [40] (NCT00091468) | Double-blind, parallel-group, placebo-controlled, randomized, pilot clinical trial | 100 subjects with MCI recruited, 74 randomized: 45 M, 29 F. Treatment: 25 M, 14 F. Mean age: 76.2 ± 8.5. Placebo: 20 M, 15 F. Age: 75.7 ± 6.5 | Logical Memory II Subscale (Delayed Paragraph Recall) from the Wechsler Memory Scale–Revised, MMSE 24–30, CDR 0.5–1.0 | Preliminary safety and efficacy of transdermal nicotine in cognitive performance and clinical outcomes in participants with MCI | 6 months | (1) Transdermal nicotine patch 5 mg, 10 mg, 15 mg; (2) Placebo. | Total AEs: (1) Treatment: 82. (2) Placebo: 52. | Treatment: 5. Placebo: 2. | Continuous performance: No. of omissions in intragroup treatment: −0.5 (1) Intragroup Placebo: 13.3 (8.9) Intergroup Treatment vs. Placebo: −2.57 (1.35) Percent of omissions: Intragroup treatment: 0.2 (0.3) Intragroup Placebo: 4.1 (2.7) Intergroup treatment vs. Placebo: −0.8 (0.4) Number of commissions intragroup treatment: −1.4 (0.1) Intragroup Placebo: −1.5 (0.3) Intergroup Treatment vs. Placebo: −0.4 (0.6) Percent of commissions intragroup treatment: −4 (0.2) Intragroup Placebo: −23.7 (1.6) Intergroup Treatment vs. Placebo: 15.5 (1.2) Hit reaction time intragroup treatment: −33 (15) Intragroup Placebo: 7 Intergroup Treatment vs. Placebo: −21 (2) Paragraph recall immediate intragroup treatment: −1.5 Intragroup Placebo: −0.5 Intergroup Treatment vs. Placebo: −0.6 Paragraph recall delayed intragroup treatment: −0.2 Intragroup Placebo: −0.3 Intergroup Treatment vs. Placebo: 0 Cognitive Drug Research Battery individual item scores simple reaction time intragroup treatment: 20 (0.2) Intragroup Placebo: −5 (3) Intergroup Treatment vs. Placebo: −3 (4) Cognitive Drug Research Battery individual item scores choice reaction time intragroup treatment: −9 (0.2) Intragroup Placebo: −10 (3) Intergroup Treatment vs. Placebo: −23 (8) Delayed picture recognition sensitivity intragroup treatment: −0.05 (0.01) Intragroup Placebo: −0.03 (0.01) Intergroup Treatment vs. Placebo: 0.06 (0.01) Delayed word recognition sensitivity intragroup treatment: 0.04 (0.02) Intragroup Placebo: −0.03 Intergroup Treatment vs. Placebo: 0.01 (0.01) Spatial memory reaction time intragroup treatment: −40 (10) Intragroup Placebo: −82 (26) Intergroup Treatment vs. Placebo: −139 (88) Spatial memory sensitivity intragroup treatment: 0 Intragroup Placebo: −0.02 Intergroup Treatment vs. Placebo: 0.09 (0.02) Digital vigilance accuracy intragroup treatment: −1.69 (0.7) Intragroup Placebo: −1.9 (0.3) Intergroup Treatment vs. Placebo: −1.09 (0.3) Digital Vigilance reaction time intragroup treatment: 9 (2) Intragroup Placebo: −14 Intergroup Treatment vs. Placebo: −6 (3) Immediate word recall intragroup treatment: 0.02 (0.07) Intragroup Placebo: −0.02 (0.04) Intergroup Treatment vs. Placebo: −0.19 (0.04) Delayed word recall intragroup treatment: 0.66 (0.09) Intragroup Placebo: 0.24 (0.01) Intergroup Treatment vs. Placebo: 0.10 (0.08) |
| Phase II | |||||||||
| Kim et al., 2014 [41] (NCT00744978) | Multi-center, double-blind, two-period, cross-over, randomized study | 66 subjects with probable AD: 32 varenicline to placebo, age 71.5 (55–85); 34 placebo to varenicline, age 73.9 (61–85) | NINCDS-ADRDA, MMSE 14–26 | Effect of varenicline on cognition in participants with mild-to-moderate probable AD | 12 weeks + 3-week washout | (1) Placebo; (2) Varenicline 1 mg. | Period 1: Treatment AEs 4 (12.9%) Period 2: Treatment AEs 1 (3.2%) Period 2: Placebo group: AEs 1 (3.2%) | Treatment group Lost to follow-up 1 (3.2%) Placebo group: Refusal to participate 2 (6.1%) Other 2 (6.1%) | ADAS-Cog 75 intergroup treatment vs. placebo: –0.42, p = 0.3873 ADAS-Cog 70 intergroup treatment vs. placebo: –0.37 p = 0.4339 NPI intergroup treatment vs. placebo: 1.28 p = 0.0468 NPI caregiver distress intergroup treatment vs. placebo: 0.42 p = 0.2624 CGI-I intergroup treatment vs. placebo: 0.00 p = 0.9745 CogState tasks intergroup treatment vs. placebo: Visual learning –0.01 p = 0.5008, Detection −0.00 p = 0.7226, Identification 0.00 p = 0.8525, One-back working memory –0.02 p = 0.5450, Continuous paired associate learning, n errors –1.31 p = 0.6251 ADAS-Cog 75 intragroup treatment: −1.14 placebo: –0.73 ADAS-Cog 70 intragroup treatment: −1.05 placebo: –0.61 NPI intragroup treatment: 1.01 placebo: −0.44 NPI caregiver distress scores intragroup treatment: 0.00 placebo: −0.31 |
| Lenz et al., 2015 [42] (NCT00555204) | Phase 2, placebo-controlled, double-blind, multi-center study | 337 subjects with probable AD or amnestic MCI: (1) Placebo: 101 (60 F/41 M, age 75.0 ± 8.56); (2) ABT-089 5 mg: 12 (7 F/5 M, mean age 71.3 ± 9.85); (3) ABT-089 10 mg: 19 (12 F/7 M, mean age 76.4 ± 6.24); (4) ABT-089 15 mg: 34 (18 F/ 16 M, mean age 77.8 ± 7.48); (5) ABT-089 20 mg: 34 (20 F/14 M, mean age 75.6 ± 7.56); (6) ABT-089 30 mg: 57 (28 F/30 M, mean age 75.4 ± 7.55); (7) ABT-089 35 mg: 77 (39 F/38 M, mean age 76.0 ± 7.87). | NINDS-ADRDA criteria, MMSE: 12–26 | Safety and efficacy of ABT-089 in cognitive function MMSE, ADAS-cog, CIBIC-plus, ADCS-ADL, NPI, CSDD, CDR | 12 weeks | (1) Placebo; (2) ABT-089 5 mg; (3) ABT-089 10 mg; (4) ABT-089 15 mg; (5) ABT-089 20 mg; (6) ABT-089 30 mg; (7) ABT-089 35 mg. | AEs: (1) 61 (2) 138 SAEs: Not reported | 106 | ADAS-Cog: ABT-089 5 mg = −1.87 ABT-089 10 mg = +0.22 ABT-089 15 mg = +0.43 ABT-089 20 mg = −0.23 ABT-089 30 mg = +0.03 ABT-089 35 mg = +0.10 MMSE: ABT-089 5 mg = −0.14 ABT-089 10 mg = −0.89 ABT-089 15 mg = −0.59 ABT-089 20 mg = −0.43 ABT-089 30 mg = −0.19 ABT-089 35 mg = −0.12 CSDD: ABT-089 5 mg = +0.29 ABT-089 10 mg = +0.44 ABT-089 15 mg = +0.08 ABT-089 20 mg = −0.26 ABT-089 30 mg = +0.56 ABT-089 35 mg = +0.28 ADCS-ADL: ABT-089 5 mg = −0.21 ABT-089 10 mg = −0.03 ABT-089 15 mg = +2.26 ABT-089 20 mg = +0.68 ABT-089 30 mg = −0.10 ABT-089 35 mg = −0.72 NPI: ABT-089 5 mg = +3.77 ABT-089 10 mg = +1.80 ABT-089 15 mg = −2.15 ABT-089 20 mg = −1.15 ABT-089 30 mg = +0.99 ABT-089 35 mg = +1.50 CIBIC-Plus: ABT-089 5 mg = +0.09 ABT-089 10 mg = −0.09 ABT-089 15 mg = +0.01 ABT-089 20 mg = −0.08 ABT-089 30 mg = −0.01 ABT-089 35 mg = −0.02 |
| Florian et al., 2016 [43] (NCT01549834) | Phase 2, randomized, double-blind, placebo-controlled multi-center study | 565 subjects: 434 (76.8%) mild-to-moderate Alzheimer’s Disease, Age 55–90 (1) ABT-126 25 mg:143 (2) ABT-126 75 mg:145 (2) Placebo:146 | NINCDS/ADRDA criteria, MMSE score 12–24 | Efficacy of ABT-126 as add-on therapy to AChEIs | 24 weeks | (1) ABT-126 25 mg (2) ABT-126 75 mg (3) Placebo once daily | At least one AE was reported for 294 subjects (67.7%) in the study ABT-126 25 mg group, 7 subjects (4.9%), ABT-126 75 mg group, 11 subjects (7.6%), placebo group 9 subjects (6.2%). ABT-126 75 mg group experienced psychiatric disorders compared with the placebo group 3.4% vs. 0% p = 0.030, two-sided | 57 (13.1%) prematurely discontinued study drug | ADAS-Cog 11-item total score Adjusted mean 1.37 (placebo) 0.57 (25 mg ABT-126, p = 0.087, one-sided). ADAS-Cog 11-item total score for the 25 mg ABT-126 group was significant compared with placebo at week 4 (−0.54 vs. 0.66 p = 0.010, one-sided). The adjusted mean for ADAS-Cog 11-item total score in the mild AD population (MMSE ≤ 19) subgroup was significantly improved for 25 mg ABT-126 (p < 0.05, one-sided) compared with placebo at weeks 4 (−0.95 vs. 0.68), 8 (1.08 vs. 0.41), 12 (−0.96 vs. 0.41) and 24 (0.62 vs. 0.81) |
| Wang et al., 2020 [44] | Blinded, randomized, placebo-controlled, clinical trial, open-label, phase 2a, safety, pharmacokinetics and biomarker study | 13 mild-to-moderate Alzheimer’s Disease patients, age 50–85 (9 F, 4 M; 3 black; 10 white; 6 Hispanic; 7 non-Hispanic) | Mini-Mental State Exam ≥ 16 and ≤24 with a cerebrospinal fluid total tau/Aβ1-42 ratio ≥ 0.30 | Safety, tolerability and effect of PTI-125 on participants with mild-to-moderate AD | 28 days | (1) 100 mg oral PTI-125 b.i.d. for 28 consecutive days; (2) Placebo. | None | None | Total tau, neurogranin and neurofilament light chain decreased by 20%, 32% and 22%, respectively. P-tau (pT181) decreased 34%. Cerebrospinal fluid biomarkers YKL-40 and interleukin-6, interleukin-1ß and TNFα decreased 9%, 14%, 11% and 5%, respectively. Plasma All reductions were of slightly lower magnitude in plasma, except for neurogranin, which was reduced 40.7%. Tau phosphorylation at pT181-tau, pS202-tau and pT231-tau was significantly reduced in plasma by 12.5%, 14.0% and 16.3%, respectively. |
| Gault et al., 2015 [45] (NCT00948909) Phase II | Phase 2, double-blind, parallel, randomized, placebo- and active-controlled study | 274 subjects with probable AD, age 73.9 ± 7.92 (1) placebo: 68 age: 73.6 ± 8.23 (2) ABT-126 5 mg: 68 age 74 ± 7.47 (3) ABT-126 25 mg: 75.7 ± 7.35 (4) Donepezil 10 mg: 68 age 72.4 ± 8.42 | Age 55–90 years National Institute of Neurological and Communicative Disorders and Stroke and the Alzheimer’s Disease and Related Disorders Association criteria for probable AD, MMSE score 10–24, CSDD 10 Modified Hachinski Ischemic Scale score of 4 | 11-item ADAS-Cog, 13-item ADAS-Cog, MMSE, CIBIS, Neuropsychiatric Inventory, ADSC-ADL, Safety | 12 weeks | (1) Placebo (2) ABT-126 5 mg (3) ABT-126 25 mg (4) Donepezil 10 mg | (1) AEs: 2 (2) AEs:1 (3) AEs:1 (4) AEs:5 | (1) 1 (3) 3 (4) 1 | 11-item ADAS-Cog total score vs. placebo: ABT-126 25 mg: −1.86 ± 0.64 (p = 0.95) 11-item ADAS-Cog total score maximum likelihood repeated-measures vs. placebo: ABT-126 25 mg: −0.84 at week 4 (90% confidence interval [CI] −1.92 to 0.23, p = 0.098), −1.11 at week 8 (90% CI −2.47 to 0.26, p = 0.091) and −1.14 at week 12 (90% CI −2.65 to 0.37, p= 0.107) 13-item ADAS-Cog total score vs. placebo: ABT-126 25 mg: −2.60 ± 0.75 (p = 0.042) 13-item ADAS-Cog total Score maximum likelihood repeated-measures vs. placebo: ABT-126 25 mg: −2.13 at week 4 (90% confidence interval [CI] −3.36 to −0.89, p = 0.002), −2.06 at week 8 (90% CI −3.69 to −0.44, p = 0.018) and −1.61 at week 12 (90% CI −3.38 to 0.17, p= 0.068) |
| Gault et al., 2016 [46] (NCT01676935) Phase IIb | Randomized, double-blind, placebo-controlled trial | 438 subjects with probable AD: (1) Placebo: 104 age 73.2 ± 7.39 (2) ABT-126 25 mg: 77 age 73.0 ± 7.62 (3) ABT-126 50 mg: 107 age 73.9 ± 8.26 (4) ABT-126 75 mg: 73 age 76.2± 8.14 (5) Donepezil 10 mg: 75 age 75.1 ± 7.75 | NINCDS/ADRDA, MMSE 10–14, CSDD ≤ 10, MHIS ≤ 4 | ADAS-Cog, AEs and safety | 24 weeks | (1) Placebo (2) ABT-126 25 mg (3) ABT-126 50 mg (4) ABT-126 75 mg (5) Donepezil 10 mg | (1) 56 (2) 42 (3) 62 (4) 38 (5) 47 | Total of 35 | CIBICPlus vs. placebo at week 24 ABT-126 75 mg: −0.38 ± 0.13 (p = 0.002) ADSC-ADL vs. placebo at week 24 ABT-126 50 mg: 2.30 ± 1.04 (p = 0.013) |
| Frolich et al., 2011 [47] NCT00501111 Phase IIb | Multi-center, double-blind, double-dummy, randomized, placebo-controlled, parallel- group trial | Patients with probable AD: (1) Placebo: 164 age 73.5 ± 6.43 (2) AZD3480 5 mg: 80 age 74.0 ± 6.01 (3) AZD3480 20 mg: 80 age 73.8 ± 6.51 (4) AZD3480 35/100 mg: 84 age 72.7 ± 6.24 (5) Donepezil 5/10 mg: 161 age 73.9 ± 6.48 | NINCDS-ADRDA, MMSE 12–26 | ADAS-Cog, ADCS-CGIC, MMSE, DAD | 12 weeks | (1) Placebo (2) AZD3480 5 mg (3) AZD3480 20 mg (4) AZD3480 35/100 mg (5) Donepezil 5/10 mg | (1) 60 (2) 21 (3) 23 (4) 34 (5) 60 | (1) 6 (2) 7 (3) 7 (4) 19 (5) 22 | Sub-analysis excluding very mild patients MMSE 25–26 resulted in slightly increased estimates of the effect size: −1.4, 95% CI: (−3.0; 0.2; p = 0.040) for AZD3480 20 mg. MMSE vs. placebo at week 12 AZD3480 20 mg: 0.8 ± 0.35 (p = 0.009) AZD3480 5 mg: 0.4 ± 0.35 (p = 0.091) ADCS-CGIC vs. placebo at week 12 AZD3480 20 mg: −0.5 ± 0.14 (p < 0.001) AZD3480 35/100 mg: −0.2 ± 0.14 (p = 0.070) Caregiver-reported outcomes DAD AZD3480 35/100 mg: 2.9 ± 2.15 (p = 0.090) |
| Pilot study | |||||||||
| Lynn Wilson et al., 1995 [48] | A double-blind, placebo-controlled trial | 7 subjects (5 M, 2 W) with probable AD, age 78.6 | DSM-III-R Guidelines, NINCDS- ADRDA Work Group, MMSE 14–22 | Effect of sustained nicotine administration on behavior, cognition and physiology | 22 days: 7 days placebo, 8 days nicotine, 7 days washout | (1) Placebo (2) Nicotine transdermal patch 22 mg | / | / | Learning errors intragroup nicotine: p < 0.05. On-task behavior intragroup nicotine increase of 14.0% (mean). Behavior observations intragroup nicotine 79.0% (mean) |
| Molecule | Mechanism of Action | Therapeutic Effect Summary |
|---|---|---|
| Nicotine |
| In mild-to-moderate AD, the trials show a small effect on attention. However, no improvement was reported on memory, behavior and global cognition. Preliminary evidence shows a potential effect of nicotine on cognitive functions in people with MCI. |
| ABT-089 |
| No improvement reported in mild-to-moderate AD. |
| AZD3480 |
| One trial failed to show efficacy in reducing cognitive decline. However, some effect was reported in secondary outcomes (MMSE, ADCS-CGIC). |
| Varenicline |
| In one study, a single dose (1 mg BID for 4 weeks) showed no effect on memory, behavior and global cognition. |
| ABT-126 |
| Different drug doses (5, 10, 25, 50, 75 mg) showed no statistically significant ability to reduce cognitive decline in mild-to-moderate AD. |
| ABT-418 |
| Some effect was reported in different verbal learning and retrieval scores (selective reminding task: total recall; selective reminding task: recall failures), but the effect in several areas of memory impairment in dementia has yet to be tested. |
| PTI-125 |
| An improvement in some biomarkers (total tau, p-tau181, neurofilament light chain, neurogranin, YKL-40, IL-6, IL-1β and TNFα) associated with AD was reported. The effects on cognitive decline are undergoing assessment, although the preliminary results seem encouraging. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Crestini, A.; Carbone, E.; Rivabene, R.; Ancidoni, A.; Rosa, P.; Tata, A.M.; Fabrizi, E.; Locuratolo, N.; Vanacore, N.; Lacorte, E.; et al. A Systematic Review on Drugs Acting as Nicotinic Acetylcholine Receptor Agonists in the Treatment of Dementia. Cells 2024, 13, 237. https://doi.org/10.3390/cells13030237
Crestini A, Carbone E, Rivabene R, Ancidoni A, Rosa P, Tata AM, Fabrizi E, Locuratolo N, Vanacore N, Lacorte E, et al. A Systematic Review on Drugs Acting as Nicotinic Acetylcholine Receptor Agonists in the Treatment of Dementia. Cells. 2024; 13(3):237. https://doi.org/10.3390/cells13030237
Chicago/Turabian StyleCrestini, Alessio, Elena Carbone, Roberto Rivabene, Antonio Ancidoni, Paolo Rosa, Ada Maria Tata, Elisa Fabrizi, Nicoletta Locuratolo, Nicola Vanacore, Eleonora Lacorte, and et al. 2024. "A Systematic Review on Drugs Acting as Nicotinic Acetylcholine Receptor Agonists in the Treatment of Dementia" Cells 13, no. 3: 237. https://doi.org/10.3390/cells13030237
APA StyleCrestini, A., Carbone, E., Rivabene, R., Ancidoni, A., Rosa, P., Tata, A. M., Fabrizi, E., Locuratolo, N., Vanacore, N., Lacorte, E., & Piscopo, P. (2024). A Systematic Review on Drugs Acting as Nicotinic Acetylcholine Receptor Agonists in the Treatment of Dementia. Cells, 13(3), 237. https://doi.org/10.3390/cells13030237