MicroRNAs as Diagnostic and Prognostic Biomarkers in Ischemic Stroke—A Comprehensive Review and Bioinformatic Analysis

 , ,
, ,  , ,
, ,
Abstract
:1. Introduction
2. Circulating miRNAs and Stroke
2.1. PCR-Based Analysis for miRNA Expression
2.2. MiRNA Profiling and RNA Sequencing Strategy
3. Future Perspectives for Using miRNAs in Diagnosis and Prognosis in Ischemic Stroke
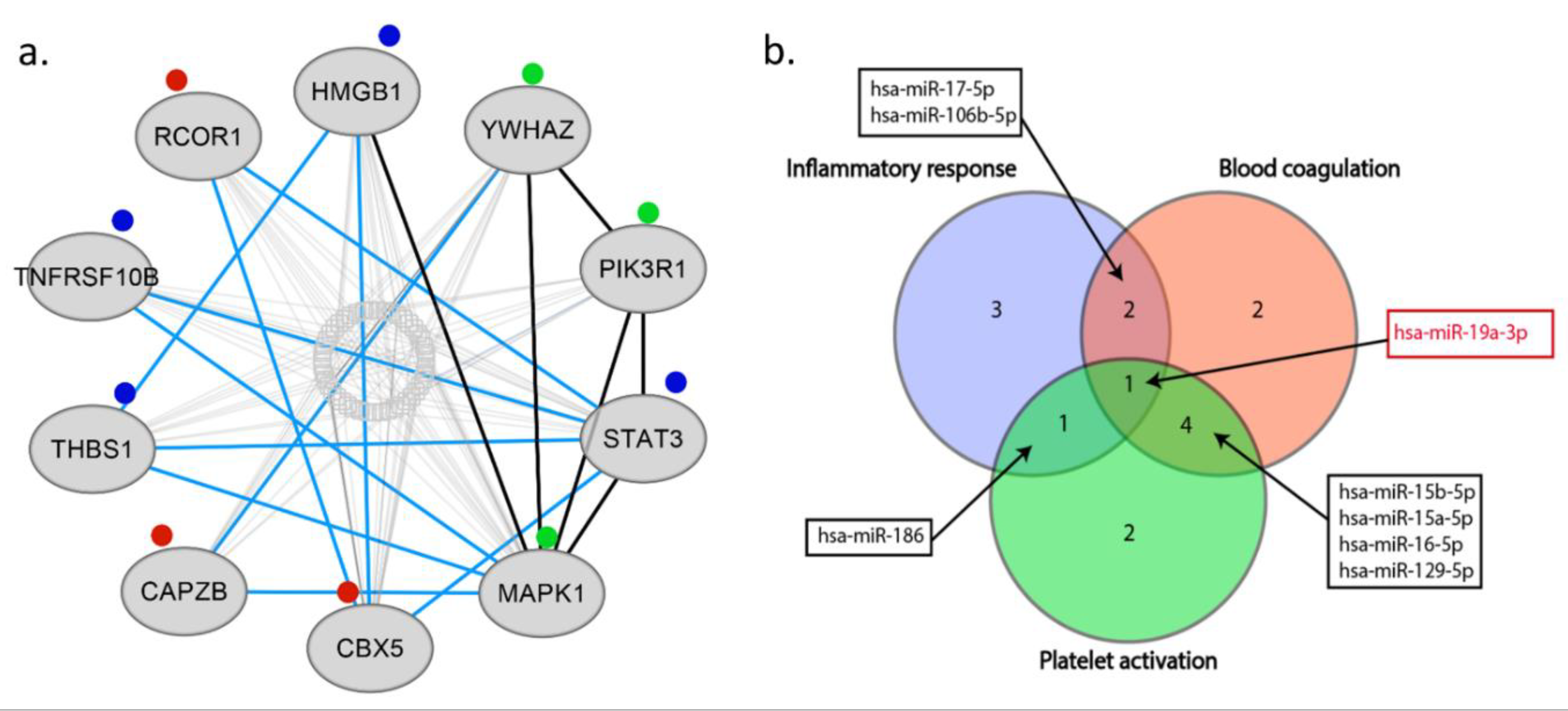
4. Bioinformatics Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Benjamin, E.J.; Blaha, M.J.; Chiuve, S.E.; Cushman, M.; Das, S.R.; Deo, R.; de Ferranti, S.D.; Floyd, J.; Fornage, M.; Gillespie, C.; et al. American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Heart Disease and Stroke Statistics-2017 Update: A Report from the American Heart Association. Circulation 2017, 135, 146–603. [Google Scholar] [CrossRef] [PubMed]
- De Rosa, S.; Sievert, H.; Sabatino, J.; Polimeni, A.; Sorrentino, S.; Indolfi, C. Percutaneous Closure Versus Medical Treatment in Stroke Patients with Patent Foramen Ovale: A Systematic Review and Meta-analysis. Ann. Intern. Med. 2018, 168, 343–350. [Google Scholar] [CrossRef] [PubMed]
- European Cardiovascular Disease Statistics, 2017th ed.; European Heart Network: Brussels, Belgium, 2017.
- Luengo-Fernandez, R.; Gray, A.M.; Bull, L.; Welch, S.; Cuthbertson, F.; Rothwell, P.M. Quality of life after TIA and stroke: Ten-year results of the Oxford Vascular Study. Neurology 2013, 81, 1588–1595. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beal, C.C. Gender and stroke symptoms: A review of the current literature. J. Neurosci. Nurs. 2010, 42, 80–87. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Xiao, Y.; Lin, Z.; Xiao, X.; He, C.; Bihl, J.C.; Zhao, B.; Ma, X.; Chen, Y. The Role of Circulating Platelets Microparticles and Platelet Parameters in Acute Ischemic Stroke Patients. J. Stroke Cerebrovasc. Dis. 2015, 24, 2313–32320. [Google Scholar] [CrossRef] [PubMed]
- Pordzik, J.; Pisarz, K.; De Rosa, S.; Jones, A.D.; Eyileten, C.; Indolfi, C.; Malek, L.; Postula, M. The Potential Role of Platelet-Related microRNAs in the Development of Cardiovascular Events in High-Risk Populations, Including Diabetic Patients: A Review. Front. Endocrinol. 2018, 9, 74. [Google Scholar] [CrossRef] [PubMed]
- Janssen, H.L.; Reesink, H.W.; Lawitz, E.J.; Zeuzem, S.; Rodriguez-Torres, M.; Patel, K.; van der Meer, A.J.; Patick, A.K.; Chen, A.; Zhou, Y.; et al. Treatment of HCV infection by targeting microRNA. N. Engl. J. Med. 2013, 368, 1685–1694. [Google Scholar] [CrossRef] [PubMed]
- Bader, A.G. miR-34—A microRNA replacement therapy is headed to the clinic. Front. Genet. 2012, 3, 120. [Google Scholar] [CrossRef] [PubMed]
- Bushati, N.; Cohen, S.M. MicroRNAs in neurodegeneration. Curr. Opin. Neurobiol. 2008, 18, 292–296. [Google Scholar] [CrossRef] [PubMed]
- Nelson, P.T.; Wang, W.X.; Rajeev, B.W. MicroRNAs (miRNAs) in neurodegenerative diseases. Brain Pathol. 2008, 18, 130–138. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.-J. Exceptional stories of microRNAs. Exp. Biol. Med. 2013, 238, 339–343. [Google Scholar] [CrossRef] [PubMed]
- De Rosa, S.; Indolfi, C. Circulating microRNAs as Biomarkers in Cardiovascular Diseases. In Experientia Supplementum; Springer: Basel, Switzerland, 2015; Volume 106, pp. 139–149. [Google Scholar]
- Di Ieva, A.; Butz, H.; Niamah, M.; Rotondo, F.; De Rosa, S.; Sav, A.; Yousef, G.M.; Kovacs, K.; Cusimano, M.D. MicroRNAs as biomarkers in pituitary tumors. Neurosurgery 2014, 75, 181–189, discussion 188–189. [Google Scholar] [CrossRef] [PubMed]
- De Rosa, S.; Curcio, A.; Indolfi, C. Emerging role of microRNAs in cardiovascular diseases. Circ. J. 2014, 78, 567–575. [Google Scholar] [CrossRef] [PubMed]
- Fichtlscherer, S.; De Rosa, S.; Fox, H.; Schwietz, T.; Fischer, A.; Liebetrau, C.; Weber, M.; Hamm, C.W.; Röxe, T.; Müller-Ardogan, M.; et al. Circulating microRNAs in patients with coronary artery disease. Circ. Res. 2010, 107, 677–684. [Google Scholar] [CrossRef] [PubMed]
- De Rosa, R.; De Rosa, S.; Leistner, D.; Boeckel, J.N.; Keller, T.; Fichtlscherer, S.; Dimmeler, S.; Zeiher, A.M. Transcoronary Concentration Gradient of microRNA-133a and Outcome in Patients with Coronary Artery Disease. Am. J. Cardiol. 2017, 120, 15–24. [Google Scholar] [CrossRef] [PubMed]
- Sluijter, J.P.; Doevendans, P.A. Circulating microRNA profiles for detection of peripheral arterial disease: Small new biomarkers for cardiovascular disease. Circ. Cardiovasc. Genet. 2013, 6, 441–443. [Google Scholar] [CrossRef]
- Sorrentino, S.; Iaconetti, C.; De Rosa, S.; Polimeni, A.; Sabatino, J.; Gareri, C.; Passafaro, F.; Mancuso, T.; Tammè, L.; Mignogna, C.; et al. Hindlimb Ischemia Impairs Endothelial Recovery and Increases Neointimal Proliferation in the Carotid Artery. Sci. Rep. 2018, 8, 761. [Google Scholar] [CrossRef]
- De Rosa, S.; Fichtlscherer, S.; Lehmann, R.; Assmus, B.; Dimmeler, S.; Zeiher, A.M. Transcoronary concentration gradients of circulating microRNAs. Circulation 2011, 124, 1936–1944. [Google Scholar] [CrossRef]
- Corsten, M.F.; Dennert, R.; Jochems, S.; Kuznetsova, T.; Devaux, Y.; Hofstra, L.; Wagner, D.R.; Staessen, J.A.; Heymans, S.; Schroen, B. Circulating MicroRNA-208b and MicroRNA-499 reflect myocardial damage in cardiovascular disease. Circ. Cardiovasc. Genet. 2010, 3, 499–506. [Google Scholar] [CrossRef]
- De Rosa, S.; Eposito, F.; Carella, C.; Strangio, A.; Ammirati, G.; Sabatino, J.; Abbate, F.G.; Iaconetti, C.; Liguori, V.; Pergola, V.; et al. Transcoronary concentration gradients of circulating microRNAs in heart failure. Eur. J. Heart Fail. 2018, 20, 1000–1010. [Google Scholar] [CrossRef]
- Tijsen, A.J.; Creemers, E.E.; Moerland, P.D.; de Windt, L.J.; van der Wal, A.C.; Kok, W.E.; Pinto, Y.M. MiR423-5p as a circulating biomarker for heart failure. Circ. Res. 2010, 106, 1035–1039. [Google Scholar] [CrossRef] [PubMed]
- Jaguszewski, M.; Osipova, J.; Ghadri, J.R.; Napp, L.C.; Widera, C.; Franke, J.; Fijalkowski, M.; Nowak, R.; Fijalkowska, M.; Volkmann, I.; et al. A signature of circulating microRNAs differentiates takotsubo cardiomyopathy from acute myocardial infarction. Eur. Heart J. 2014, 35, 999–1006. [Google Scholar] [CrossRef] [PubMed]
- Gareri, C.; De Rosa, S.; Indolfi, C. MicroRNAs for Restenosis and Thrombosis After Vascular Injury. Circ. Res. 2016, 118, 1170–1184. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Polimeni, A.; De Rosa, S.; Indolfi, C. Vascular miRNAs after balloon angioplasty. Trends Cardiovasc. Med. 2013, 23, 9–14. [Google Scholar] [CrossRef] [PubMed]
- De Rosa, S.; Arcidiacono, B.; Chiefari, E.; Brunetti, A.; Indolfi, C.; Foti, D.P. Type 2 Diabetes Mellitus and Cardiovascular Disease: Genetic and Epigenetic Links. Front. Endocrinol. 2018, 9, 2. [Google Scholar] [CrossRef] [PubMed]
- Zampetaki, A.; Kiechl, S.; Drozdov, I.; Willeit, P.; Mayr, U.; Prokopi, M.; Mayr, A.; Weger, S.; Oberhollenzer, F.; Bonora, E.; et al. Plasma microRNA profiling reveals loss of endothelial miR-126 and other microRNAs in type 2 diabetes. Circ. Res. 2010, 107, 810–817. [Google Scholar] [CrossRef] [PubMed]
- Carino, A.; De Rosa, S.; Sorrentino, S.; Polimeni, A.; Sabatino, J.; Caiazzo, G.; Torella, D.; Spaccarotella, C.; Mongiardo, A.; Strangio, A.; et al. Modulation of Circulating MicroRNAs Levels during the Switch from Clopidogrel to Ticagrelor. Biomed. Res. Int. 2016, 2016, 3968206. [Google Scholar] [CrossRef] [PubMed]
- Streit, S.; Michalski, C.W.; Erkan, M.; Kleeff, J.; Friess, H. Northern blot analysis for detection and quantification of RNA in pancreatic cancer cells and tissues. Nat. Protoc. 2009, 4, 37–43. [Google Scholar] [CrossRef] [PubMed]
- Várallyay, E.; Burgyán, J.; Havelda, Z. MicroRNA detection by northern blotting using locked nucleic acid probes. Nat. Protoc. 2008, 3, 190–196. [Google Scholar] [CrossRef] [PubMed]
- Ferraro, D.; Champ, J.; Teste, B.; Serra, M.; Malaquin, L.; Viovy, J.L.; de Cremoux, P.; Descroix, S. Microfluidic platform combining droplets and magnetic tweezers: Application to HER2 expression in cancer diagnosis. Sci. Rep. 2016, 6, 25540. [Google Scholar] [CrossRef] [PubMed]
- Eminaga, S.; Christodoulou, D.C.; Vigneault, F.; Church, G.M.; Seidman, J.G. Quantification of microRNA expression with next-generation sequencing. Curr. Protoc. Mol. Biol. 2013, 103, 4–17. [Google Scholar] [CrossRef] [PubMed]
- Chugh, P.; Dittmer, D.P. Potential Pitfalls in microRNA Profiling. Wiley Interdiscip. Rev. RNA 2012, 3, 601–616. [Google Scholar] [CrossRef] [PubMed]
- Yang, H.; Hui, A.; Pampalakis, G.; Soleymani, L.; Liu, F.F.; Sargent, E.H.; Kelley, S.O. Direct, electronic microRNA detection for the rapid determination of differential expression profiles. Angew. Chem. Int. Ed. Engl. 2009, 48, 8461–8464. [Google Scholar] [CrossRef] [PubMed]
- Roy, S.; Soh, J.H.; Gao, Z. A microfluidic-assisted microarray for ultrasensitive detection of miRNA under an optical microscope. Lab Chip 2011, 11, 1886–1894. [Google Scholar] [CrossRef] [PubMed]
- Dong, H.; Jin, S.; Ju, H.; Hao, K.; Xu, L.P.; Lu, H.; Zhang, X. Trace and label-free microRNA detection using oligonucleotide encapsulated silver nanoclusters as probes. Anal. Chem. 2012, 84, 8670–8674. [Google Scholar] [CrossRef] [PubMed]
- Tran, H.V.; Piro, B.; Reisberg, S.; Tran, L.D.; Duc, H.T.; Pham, M.C. Label-free and reagentless electrochemical detection of microRNAs using a conducting polymer nanostructured by carbon nanotubes: Application to prostate cancer biomarker miR-141. Biosens. Bioelectron. 2013, 49, 164–169. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.; Ridzon, D.A.; Broomer, A.J.; Zhou, Z.; Lee, D.H.; Nguyen, J.T.; Barbisin, M.; Xu, N.L.; Mahuvakar, V.R.; Andersen, M.R.; et al. Real-time quantification of microRNAs by stem-loop RT-PCR. Nucleic Acids Res. 2005, 33, e179. [Google Scholar] [CrossRef] [PubMed]
- Kang, K.; Peng, X.; Luo, J.; Gou, D. Identification of circulating miRNA biomarkers based on global quantitative real-time PCR profiling. J. Anim. Sci. Biotechnol. 2012, 3, 4. [Google Scholar] [CrossRef] [Green Version]
- Long, G.; Wang, F.; Li, H.; Yin, Z.; Sandip, C.; Lou, Y.; Wang, Y.; Chen, C.; Wang, D.W. Circulating miR-30a, miR-126 and let-7b as biomarker for ischemic stroke in humans. BMC Neurol. 2013, 13, 178. [Google Scholar] [CrossRef]
- Li, Y.; Maegdefessel, L. My heart will go on-beneficial effects of anti-MiR-30 after myocardial infarction. Ann. Transl. Med. 2016, 4, 144. [Google Scholar] [CrossRef]
- Peng, G.; Yuan, Y.; Wu, S.; He, F.; Hu, Y.; Luo, B. MicroRNA let-7e is a potential circulating biomarker of acute stage ischemic stroke. Transl. Stroke Res. 2015, 6, 437–445. [Google Scholar] [CrossRef] [PubMed]
- Huang, S.; Lv, Z.; Guo, Y.; Li, L.; Zhang, Y.; Zhou, L.; Yang, B.; Wu, S.; Zhang, Y.; Xie, C.; et al. Identification of blood Let-7e-5p as a biomarker for ischemic stroke. PLoS ONE 2016, 11, e0163951. [Google Scholar] [CrossRef] [PubMed]
- Gong, Z.; Zhao, S.; Zhang, J.; Xu, X.; Guan, W.; Jing, L.; Liu, P.; Lu, J.; Teng, J.; Peng, T.; et al. Initial research on the relationship between let-7 family members in the serum and massive cerebral infarction. J. Neurol. Sci. 2016, 361, 150–157. [Google Scholar] [CrossRef] [PubMed]
- Panda, A.C.; Grammatikakis, I.; Kim, K.M.; De, S.; Martindale, J.L.; Munk, R.; Yang, X.; Abdelmohsen, K.; Gorospe, M. Identification of senescence-associated circular RNAs (SAC-RNAs) reveals senescence suppressor CircPVT1. Nucleic Acids Res. 2017, 45, 4021–4035. [Google Scholar] [CrossRef] [PubMed]
- Leung, L.Y.; Chan, C.P.; Leung, Y.K.; Jiang, H.L.; Abrigo, J.M.; Wang, D.F.; Chung, J.S.; Rainer, T.H.; Graham, C.A. Comparison of miR-124-3p and miR-16 for early diagnosis of hemorrhagic and ischemic stroke. Clin. Chim. Acta 2014, 433, 139–144. [Google Scholar] [CrossRef] [PubMed]
- Wu, J.; Du, K.; Lu, X. Elevated expressions of serum miR-15a, miR-16, and miR-17-5p are associated with acute ischemic stroke. Int. J. Clin. Exp. Med. 2015, 8, 21071–21079. [Google Scholar]
- Spinetti, G.; Fortunato, O.; Caporali, A.; Shantikumar, S.; Marchetti, M.; Meloni, M.; Descamps, B.; Floris, I.; Sangalli, E.; Vono, R.; et al. MicroRNA-15a and microRNA-16 impair human circulating proangiogenic cell functions and are increased in the proangiogenic cells and serum of patients with critical limb ischemia. Circ. Res. 2013, 112, 335–346. [Google Scholar] [CrossRef]
- Liu, L.F.; Liang, Z.; Lv, Z.R.; Liu, X.H.; Bai, J.; Chen, J.; Chen, C.; Wang, Y. MicroRNA-15a/b are upregulated in response to myocardial ischemia/reperfusion injury. J. Geriatr. Cardiol. 2012, 9, 28–32. [Google Scholar]
- Yin, K.J.; Fan, Y.; Hamblin, M.; Zhang, J.; Zhu, T.; Li, S.; Hawse, J.R.; Subramaniam, M.; Song, C.Z.; Urrutia, R.; et al. KLF11 mediates PPARgamma cerebrovascular protection in ischaemic stroke. Brain 2013, 136, 1274–1287. [Google Scholar] [CrossRef]
- Liu, X.S.; Chopp, M.; Wang, X.L.; Zhang, L.; Hozeska-Solgot, A.; Tang, T.; Kassis, H.; Zhang, R.L.; Chen, C.; Xu, J.; et al. MicroRNA-17-92 cluster mediates the proliferation and survival of neural progenitor cells after stroke. J. Biol. Chem. 2013, 288, 12478–12488. [Google Scholar] [CrossRef]
- Jin, F.; Xing, J. Circulating pro-angiogenic and anti-angiogenic microRNA expressions in patients with acute ischemic stroke and their association with disease severity. Neurol. Sci. 2017, 38, 2015–2023. [Google Scholar] [CrossRef] [PubMed]
- Gan, C.S.; Wang, C.W.; Tan, K.S. Circulatory microRNA-145 expression is increased in cerebral ischemia. Genet. Mol. Res. 2012, 11, 147–152. [Google Scholar] [CrossRef] [PubMed]
- Jia, L.; Hao, F.; Wang, W.; Qu, Y. Circulating miR-145 is associated with plasma high-sensitivity C-reactive protein in acute ischemic stroke patients. Cell. Biochem. Funct. 2015, 33, 314–319. [Google Scholar] [CrossRef] [PubMed]
- He, W.; Chen, S.; Chen, X.; Li, S.; Chen, W. Bioinformatic analysis of potential microRNAs in ischemic stroke. J. Stroke Cerebrovasc. Dis. 2016, 25, 1753–1759. [Google Scholar] [CrossRef] [PubMed]
- Tsai, P.C.; Liao, Y.C.; Wang, Y.S.; Lin, H.F.; Lin, R.T.; Juo, S.H. Serum microRNA-21 and microRNA-221 as potential biomarkers for cerebrovascular disease. J. Vasc. Res. 2013, 50, 346–354. [Google Scholar] [CrossRef] [PubMed]
- Zhou, J.; Zhang, J. Identification of miRNA-21 and miRNA-24 in plasma as potential early stage markers of acute cerebral infarction. Mol. Med. Rep. 2014, 10, 971–976. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Zhang, Y.; Huang, J.; Chen, X.; Gu, X.; Wang, Y.; Zeng, L.; Yang, G.Y. Increase of circulating miR-223 and insulin-like growth factor-1 is associated with the pathogenesis of acute ischemic stroke in patients. BMC Neurol. 2014, 14, 77. [Google Scholar] [CrossRef] [PubMed]
- Chevillet, J.R.; Kang, Q.; Ruf, I.K.; Briggs, H.A.; Vojtech, L.N.; Hughes, S.M.; Cheng, H.H.; Arroyo, J.D.; Meredith, E.K.; Gallichotte, E.N.; et al. Quantitative and stoichiometric analysis of the microRNA content of exosomes. Proc. Natl. Acad. Sci. USA 2014, 111, 14888–14893. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Song, Y.; Huang, J.; Qu, M.; Zhang, Y.; Geng, J.; Zhang, Z.; Liu, J.; Yang, G.Y. Increased circulating exosomal miRNA-223 is associated with acute ischemic stroke. Front. Neurol. 2017, 8, 57. [Google Scholar] [CrossRef]
- Ji, Q.; Ji, Y.; Peng, J.; Zhou, X.; Chen, X.; Zhao, H.; Xu, T.; Chen, L.; Xu, Y. Increased brain-specific miR-9 and miR-124 in the serum exosomes of acute ischemic stroke patients. PLoS ONE 2016, 11, e0163645. [Google Scholar] [CrossRef]
- Liu, Y.; Zhang, J.; Han, R.; Liu, H.; Sun, D.; Liu, X. Downregulation of serum brain specific microRNA is associated with inflammation and infarct volume in acute ischemic stroke. J. Clin. Neurosci. 2015, 22, 291–295. [Google Scholar] [CrossRef] [PubMed]
- Chen, Z.; Wang, K.; Huang, J.; Zheng, G.; Lv, Y.; Luo, N.; Liang, M.; Huang, L. Upregulated serum miR-146b serves as a biomarker for acute ischemic stroke. Cell. Physiol. Biochem. 2018, 45, 397–405. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Barbacioru, C.; Hyland, F.; Xiao, W.; Hunkapiller, K.L.; Blakem, J.; Chan, F.; Gonzalez, C.; Zhang, L.; Samaha, R.R. Large scale real-time PCR validation on gene expression measurements from two commercial long-oligonucleotide microarrays. BMC Genom. 2006, 7, 59. [Google Scholar] [CrossRef]
- Moldovan, L.; Batte, K.E.; Trgovcich, J.; Wisler, J.; Marsh, C.B.; Piper, M. Methodological challenges in utilizing miRNAs as circulating biomarkers. J. Cell. Mol. Med. 2014, 18, 371–390. [Google Scholar] [CrossRef] [Green Version]
- Jickling, G.C.; Ander, B.P.; Zhan, X.; Noblett, D.; Stamova, B.; Liu, D. MicroRNA expression in peripheral blood cells following acute ischemic stroke and their predicted gene targets. PLoS ONE 2014, 9, e99283. [Google Scholar] [CrossRef]
- Li, P.; Teng, F.; Gao, F.; Zhang, M.; Wu, J.; Zhang, C. Identification of circulating microRNAs as potential biomarkers for detecting acute ischemic stroke. Cell. Mol. Neurobiol. 2015, 35, 433–447. [Google Scholar] [CrossRef]
- Zeng, L.; He, X.; Wang, Y.; Tang, Y.; Zheng, C.; Cai, H.; Liu, J.; Wang, Y.; Fu, Y.; Yang, G.Y. MicroRNA-210 overexpression induces angiogenesis and neurogenesis in the normal adult mouse brain. Gene Ther. 2014, 21, 37–43. [Google Scholar] [CrossRef]
- Ouyang, Y.B.; Xu, L.; Yue, S.; Liu, S.; Giffard, R.G. Neuroprotection by astrocytes in brain ischemia: Importance of microRNAs. Neurosci. Lett. 2014, 565, 53–58. [Google Scholar] [CrossRef] [Green Version]
- Ouyang, Y.B.; Giffard, R.G. MicroRNAs affect BCL-2 family proteins in the setting of cerebral ischemia. Neurochem. Int. 2014, 77C, 2–8. [Google Scholar] [CrossRef]
- Tan, K.S.; Armugam, A.; Sepramaniam, S.; Lim, K.Y.; Setyowati, K.D.; Wang, C.W.; Jeyaseelan, K. Expression profile of MicroRNAs in young stroke patients. PLoS ONE 2009, 4, e7689. [Google Scholar] [CrossRef]
- Sepramaniam, S.; Tan, J.R.; Tan, K.S.; DeSilva, D.A.; Tavintharan, S.; Woon, F.P.; Wang, C.W.; Yong, F.L.; Karolina, D.S.; Kaur, P.; et al. Circulating microRNAs as biomarkers of acute stroke. Int. J. Mol. Sci. 2014, 15, 1418–1432. [Google Scholar] [CrossRef] [PubMed]
- Wang, W.H.; Guan, S.; Zhang, L.Y.; Lei, S.; Zeng, Y.J. Circulating microRNAs as novel potential biomarkers for early diagnosis of acute stroke in humans. J. Stroke Cerebrovasc. Dis. 2014, 23, 2607–2613. [Google Scholar] [CrossRef]
- Tian, C.; Li, Z.; Yang, Z.; Huang, Q.; Liu, J.; Hong, B. Plasma microRNA-16 is a biomarker for diagnosis, stratification, and prognosis of hyperacute cerebral infarction. PLoS ONE 2016, 11, e0166688. [Google Scholar] [CrossRef]
- Tiedt, S.; Prestel, M.; Malik, R.; Schieferdecker, N.; Duering, M.; Kautzky, V.; Stoycheva, I.; Böck, J.; Northoff, B.H.; Klein, M.; et al. RNA-Seq identifies circulating miR-125a-5p, miR-125b-5p, and miR-143-3p as potential biomarkers for acute ischemic stroke. Circ. Res. 2017, 121, 970–980. [Google Scholar] [CrossRef]
- Mick, E.; Shah, R.; Tanriverdi, K.; Murthy, V.; Gerstein, M.; Rozowsky, J.; Kitchen, R.; Larson, M.G.; Levy, D.; Freedman, J.E. Stroke and circulating extracellular RNAs. Stroke 2017, 48, 828–834. [Google Scholar] [CrossRef] [PubMed]
- Wu, J.; Fan, C.L.; Ma, L.J.; Liu, T.; Wang, C.; Song, J.X.; Lv, Q.S.; Pan, H.; Zhang, C.N.; Wang, J.J. Distinctive expression signatures of serum microRNAs in ischaemic stroke and transient ischaemic attack patients. Thromb. Haemost. 2017, 117, 992–1001. [Google Scholar] [CrossRef]
- Agarwal, V.; Bell, G.W.; Nam, J.; Bartel, D.P. Predicting effective microRNA target sites in mammalian mRNAs. eLife 2015, 4, e05005. [Google Scholar] [CrossRef] [PubMed]
- Chou, C.H.; Shrestha, S.; Yang, C.D.; Chang, N.W.; Lin, Y.L.; Liao, K.W.; Huang, W.C.; Sun, T.H.; Tu, S.J.; Lee, W.H.; et al. miRTarBase update 2018: A resource for experimentally validated microRNA-target interactions. Nucleic Acids Res. 2018, 46, D296–D302. [Google Scholar] [CrossRef]
- Durinck, S.; Spellman, P.; Birney, E.; Huber, W. Mapping identifiers for the integration of genomic datasets with the R/Bioconductor package biomaRt. Nat. Protoc. 2009, 4, 1184–1191. [Google Scholar] [CrossRef]
- Shannon, P.; Markiel, A.; Ozier, O.; Baliga, N.S.; Wang, J.T.; Ramage, D.; Amin, N.; Schwikowski, B.; Ideker, T. Cytoscape: A software environment for integrated models of biomolecular interaction networks. Genome Res. 2003, 13, 2498–2504. [Google Scholar] [CrossRef]
- Szklarczyk, D.; Morris, J.H.; Cook, H.; Kuhn, M.; Wyder, S.; Simonovic, M.; Santos, A.; Doncheva, N.T.; Roth, A.; Bork, P.; et al. The STRING database in 2017: Quality-controlled protein-protein association networks, made broadly accessible. Nucleic Acids Res. 2017, 45, D362–D368. [Google Scholar] [CrossRef]
- Zhang, X.; Yu, H.; Lou, J.R.; Zheng, J.; Zhu, H.; Popescu, N.I.; Lupu, F.; Lind, S.E.; Ding, W.Q. MicroRNA-19 (miR-19) regulates tissue factor expression in breast cancer cells. J. Biol. Chem. 2011, 286, 1429–1435. [Google Scholar] [CrossRef]
- Weber, M.; Baker, M.B.; Patel, R.S.; Quyyumi, A.A.; Bao, G.; Searles, C.D. MicroRNA expression profile in CAD patients and the impact of ACEI/ARB. Cardiol. Res. Pract. 2011, 2011, 532915. [Google Scholar] [CrossRef]
- Doebele, C.; Bonauer, A.; Fischer, A.; Scholz, A.; Reiss, Y.; Urbich, C.; Hofmann, W.K.; Zeiher, A.M.; Dimmeler, S. Members of the microRNA-17-92 cluster exhibit a cell-intrinsic antiangiogenic function in endothelial cells. Blood 2010, 115, 4944–4950. [Google Scholar] [CrossRef] [Green Version]
- Bonauer, A.; Carmona, G.; Iwasaki, M.; Mione, M.; Koyanagi, M.; Fischer, A.; Burchfield, J.; Fox, H.; Doebele, C.; Ohtani, K.; et al. MicroRNA-92a controls angiogenesis and functional recovery of ischemic tissues in mice. Science 2009, 324, 1710–1713. [Google Scholar] [CrossRef]
- Singh, V.; Roth, S.; Veltkamp, R.; Liesz, A. HMGB1 as a key mediator of immune mechanisms in ischemic stroke. Antioxid. Redox Signal. 2016, 24, 635–651. [Google Scholar] [CrossRef]
- Diamanti, D.; Lahiri, N.; Tarditi, A.; Magnoni, L.; Fondelli, C.; Morena, E.; Malusa, F.; Pollio, G.; Diodato, E.; Tripepi, G.; et al. Reference genes selection for transcriptional profiling in blood of HD patients and R6/2 mice. J. Huntingtons Dis. 2013, 2, 185–200. [Google Scholar] [CrossRef]
- Dervishi, I.; Gozutok, O.; Murnan, K.; Gautam, M.; Heller, D.; Bigio, E.; Ozdinler, P.H. Protein-protein interactions reveal key canonical pathways, upstream regulators, interactome domains, and novel targets in ALS. Sci. Rep. 2018, 8, 14732. [Google Scholar] [CrossRef]
- Miller, J.A.; Oldham, M.C.; Geschwind, D.H. A systems level analysis of transcriptional changes in Alzheimer’s disease and normal aging. J. Neurosci. 2008, 28, 1410–1420. [Google Scholar] [CrossRef]
- Wu, C.C.; Chen, B.S. Key immune events of the pathomechanisms of early cardioembolic stroke: Multi-database mining and systems biology approach. Int. J. Mol. Sci. 2016, 17, 305. [Google Scholar] [CrossRef]
- Chang, T.Y.; Huang, T.S.; Wang, H.W.; Chang, S.J.; Lo, H.H.; Chiu, Y.L.; Wang, Y.L.; Hsiao, C.D.; Tsai, C.H.; Chan, C.H.; et al. miRNome traits analysis on endothelial lineage cells discloses biomarker potential circulating microRNAs which affect progenitor activities. BMC Genom. 2014, 15, 802. [Google Scholar] [CrossRef]
- Liang, Z.; Wu, G.; Fan, C.; Xu, J.; Jiang, S.; Yan, X.; Di, S.; Ma, Z.; Hu, W.; Yang, Y. The emerging role of signal transducer and activator of transcription 3 in cerebral ischemic and hemorrhagic stroke. Prog. Neurobiol. 2016, 137, 1–16. [Google Scholar] [CrossRef]
- Bam, M.; Yang, X.; Sen, S.; Zumbrun, E.E.; Dennis, L.; Zhang, J.; Nagarkatti, P.S.; Nagarkatti, M. Characterization of dysregulated miRNA in peripheral blood mononuclear cells from ischemic stroke patients. Mol. Neurobiol. 2018, 55, 1419–1429. [Google Scholar] [CrossRef]
- Sun, J.; Nan, G. The mitogen-activated protein kinase (MAPK) signaling pathway as a discovery target in stroke. J. Mol. Neurosci. 2016, 59, 90–98, Erratum in: J. Mol. Neurosci. 2016, 59, 430. [Google Scholar] [CrossRef]
- Wang, H.; Zhang, X.M.; Tomiyoshi, G.; Nakamura, R.; Shinmen, N.; Kuroda, H.; Kimura, R.; Mine, S.; Kamitsukasa, I.; Wada, T.; et al. Association of serum levels of antibodies against MMP1, CBX1, and CBX5 with transient ischemic attack and cerebral infarction. Oncotarget 2017, 9, 5600–5613. [Google Scholar] [CrossRef] [Green Version]
- Gao, J.B.; Tang, W.D.; Wang, H.X.; Xu, Y. Predictive value of thrombospondin-1 for outcomes in patients with acute ischemic stroke. Clin. Chim. Acta 2015, 450, 176–180. [Google Scholar] [CrossRef]
- Cevik, O.; Baykal, A.T.; Sener, A. Platelets proteomic profiles of acute ischemic stroke patients. PLoS ONE 2016, 11, e0158287. [Google Scholar] [CrossRef]
- Yang, F.H.; Pyle, W.G. Reduced cardiac CapZ protein protects hearts against acute ischemia-reperfusion injury and enhances preconditioning. J. Mol. Cell. Cardiol. 2012, 52, 761–772. [Google Scholar] [CrossRef]
- Ridker, P.M.; Everett, B.M.; Thuren, T.; MacFadyen, J.G.; Chang, W.H.; Ballantyne, C.; Fonseca, F.; Nicolau, J.; Koenig, W.; Anker, S.D.; et al. CANTOS Trial Group. Antiinflammatory Therapy with Canakinumab for Atherosclerotic Disease. N. Engl. J. Med. 2017, 377, 1119–1131. [Google Scholar] [CrossRef]
- Cirillo, P.; Golino, P.; Calabrò, P.; Calì, G.; Ragni, M.; De Rosa, S.; Cimmino, G.; Pacileo, M.; De Palma, R.; Forte, L.; et al. C-reactive protein induces tissue factor expression and promotes smooth muscle and endothelial cell proliferation. Cardiovasc. Res. 2005, 68, 47–55. [Google Scholar] [CrossRef] [Green Version]
- De Rosa, S.; Cirillo, P.; Pacileo, M.; Di Palma, V.; Paglia, A.; Chiariello, M. Leptin stimulated C-reactive protein production by human coronary artery endothelial cells. J. Vasc. Res. 2009, 46, 609–617. [Google Scholar] [CrossRef] [PubMed]
- Cirillo, P.; Golino, P.; Calabrò, P.; Ragni, M.; Forte, L.; Piro, O.; De Rosa, S.; Pacileo, M.; Chiariello, M. Activated platelets stimulate tissue factor expression in smooth muscle cells. Thromb. Res. 2003, 112, 51–57. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Ref | miRNAs | Sampling/Sampling Time Point | Number of Stroke pts/Controls | Inclusion Criteria | Exclusion Criteria | Stroke Subtype | Prognostic or Diagnostic Value | Regulation of miRNAs | Correlation |
|---|---|---|---|---|---|---|---|---|---|
| Long et al. [41] | miR-30a, miR-126, Let-7b, | Plasma/24 h, 1 w, 4 w, 24 w, 48 w | 197/50 | First-ever stroke patients with cerebral infarction | Exclusion criteria included TIA, subarachnoid hemorrhage, embolic brain infarction, brain tumors, and cerebrovascular malformation, pulmonary fibrosis, endocrine and metabolic diseases (except type 2 diabetes), inflammatory and autoimmune diseases, and serious chronic diseases, for example, hepatic cirrhosis and renal failure. Cardioembolic stroke and documented atrial fibrillationwere also excluded from the study. | LA 51, SA 48, CE 50, UDN 48 | Diagnostic value | MiR-30a and miR-126 were downregulated in 24 h, 1 w, 4 w, and 24 w. After 48 w miRNA levels increased to the baseline | No correlation was found between HDL, LDL, triglyceride, systolic and diastolic blood pressures, diabetes and smoking status and miRNAs. |
| Peng et al. [43] | miR-338, Let-7e | Serum and CSF/1–7 days (acute phase), 8–14 days (subacute phase), over 15 days (recovery) | 72/51 | Diagnosis of an initial episode of cerebral infarction based on clinical history and MRI results, ages ranging from 55 to 75 years, patient arrival at the hospital after 4.5 h but within 24 h after the event, NIHSS score of 4 to 15, and without hemorrhagic transformation. | Exclusion criteria for all enrolled patients included recurrent stroke, tumors, abnormal renal or liver function, infectious diseases, immune diseases, blood disorders, and psychiatric illness including depression and schizophrenia. | NA | Let-7e may be a biomarker in acute phase/had no prognostic value | Let-7e significantly higher at all time-points in serum. MiR-338 and Let-7e in CSF was upregulated in 8–14 days (subacute). | No correlation was found between NIHSS and Let-7e, correlation was found between CRP levels and Let-7e. |
| Huang et al. [44] | Let-7e-5p | Whole blood/24 h | Two groups: 44/44, 302/02 | First-ever IS patients | Patients with a history of stroke, peripheral arterial occlusive disease or cancer were excluded from this study. | NA | Diagnostic value for Let-7e-5p | Let-7e-5p significantly higher with IS patients than controls | Negatively correlated with ATF2, CASP3, FGFR2, NLK, PTPN7, RASGRP1 and TGFBR1 genes. |
| Gong et al. [45] | Let-7f | Serum/after 48 h and 2 w | 88/130 | Selection criteria included age >18 years, within 48 h after stroke attack, based on CT or MRI, the patient had an infarct of at least 67% of the middle cerebral artery territory, with or without the additional infarction of the anterior or posterior cerebral artery on the same side. | Exclusion criteria included unconsciousness due to metabolic disturbances or medication, any sedation or surgery, a pre-stroke score on the mRS of more than 2; and the presence of a concurrent serious illness which may affect the patient’s outcome, such as severe cardiopulmonary complications. | NA | Prognostic value | Let-7f was downregulated in IS with MCI and upregulated in IS without MCI at 48 h. | Let-7f was negatively correlated with hs-CRP in IS MCI patients, also negatively correlated with IL-6 in MCI without HT |
| Leung et al. [47] | miR-124-3p and miR-16 | Plasma/(≤6 h), (6–24 h) | 93 IS + 19 HS/23 | Patients aged 18 years old and above were included to the study, HS or IS confirmed by CT scan and/or MRI, who presented within 24 h of symptom onset. | NA | NA | Diagnostic value | MiR-124-3p levels were markedly higher in patients with HS patients compared to IS patients only in cases presenting early (≤6 h), increased miR-16 were found in patients with IS compared to those with HS in patients presenting late after symptom onset (6–24 h) | Plasma concentrations of miR-124-3p, but not miR-16, positively correlated with lesion volume on CT in HS patients; however, both plasma miR-124-3p and miR-16 did not correlate with lesion volume on MRI in IS patients. |
| Wu et al. [48] | miR-15a, miR-16, miR-17-5p | Serum/before treatment | 106/120 | The cohort included 55 men and 51 women with a mean age of 64.8 years (range, 39–88 years). | Symptoms indicative of subarachnoid hemorrhage, even if no imaging findings of hemorrhage were found on CT or MRI, intracranial hemorrhage, acute myocardial infarction, critical limb ischemia. | NA | Diagnostic value | MiR-15a, miR-16, and miR-17-5p were significantly higher in IS patients compared to control subjects | MiR-15a was significantly correlated with age, strong negative correlation between miR-16 levels and HDL and ApoA1 was found. |
| Jin F. and Xing J. [53] | miR-126, miR-17-5p, miR-17-3p, miR-18a, miR-19a, miR-20a, miR-19b-1, miR-92a, Let-7b, Let-7f, miR-130a, miR-210, miR-378, miR-296, miR-101, miR-221, miR-222, miR-328, miR-15b, miR-16, miR-26b, miR-27b, miR-218, miR-206, miR-338-3p, miR-497, miR-195a-3p, miR-185 | Plasma/24h | 106/110 | Within 24 h post the onset of symptom, diagnosed with IS according to patient history, laboratory and neurological examination, CT scan, MRI, and/or MRA. | Patients with infection, renal or hepatic failure, hematological malignancies, solid tumors, immunosuppressive therapy, or treatment with thrombolytic therapy were excluded from the study. | NA | Diagnostic value, disease severity management | MiR-126 and miR-130a decreased in the IS patients while miR-222, miR-218, and miR-185 increased in the IS patients. | MiR-126, miR-378, miR-101 negatively, miR-222, miR-218, miR-206 were positively correlated with NIHSS |
| Gan et al. [54] | miR-145 | Whole blood/NA/after one month second sampling (N = 11) | 32/14 | IS patients between the ages of 18 and 49 years were included. IS was confirmed by either MRI or CT imaging of the brain. | Excluded from the study were subjects with hemorrhage stroke. | NA | No diagnostic and prognostic value was found | Upregulation of miR-145 | No correlation was found |
| Jia et al. [55] | miR-21, miR-23a, miR-29b, miR-124, miR-145, miR-210, miR-221, miR-223, miR-483-5p | Serum/24 h | 146/96 | Patients with IS within 24 h after symptom onset were included. | Exclusion criteria included under 18 years old, being on thrombolytic or anticoagulant therapies, intracerebral hemorrhage or hemorrhagic transformation, other complicating neurological or neuropsychological diseases, cancer, comorbidity with proinflammatory conditions and clinical signs of infection at any time during the study. | NA | Diagnostic value | MiR-145 was upregulated, miR-23a and miR-221 were significantly downregulated | Positive correlation between miR-145 and hs-CRP, IL-6, infarct volume and NIHSS scores was found, serum miR-23a and miR-221 were moderate negatively correlated with plasma hs-CRP |
| Tsai et al. [57] | miR-145, miR-21, miR-221 | Serum/7 days | 167/157 | Patients with IS based on the World Health Organization criteria. The blood samples from the patients were taken within 7 days of the onset of stroke. Demographic data and histories of hypertension, diabetes, hypercholesterolemia and cigarette smoking were obtained from each study subject. | NA | NA | Diagnostic value | MiR-21 was downregulated, miR-221 was upregulated, no significance for miR-145 was found | MiR-21 expressions was correlated with miR-221 levels. |
| Zhou et al. [58] | miR-21, miR-24 | Plasma/24 h | 68/21 | ACI participated included in the study. The diagnosis of ACI was conducted based on patient history, lab examination, neurological deficit, MRI and MRA results. | Patients with a history of tumor, immune disease, blood disease, acute infectious disease, renal or liver failure were excluded. | NA | Diagnostic value | MiR-21 and miR-24 were downregulated | MiR-21 expressions were positively correlated with miR-24 level, and negatively correlated with NIHHS score |
| Chen et al. [61] | miR-223 | Exosomes/plasma/less than 72 h | 50/33 | Stroke patients included in the study. Demography feature, related previous history including hypertension, diabetes mellitus, hyperlipidemia, cardiopathy, associated laboratory test, and imaging information including blood glucose, blood lipid, electrocardiogram, cardiac ultrasonography, carotid artery ultrasonography, MRI, and MRA were also collected for analysis. | Exclusive criteria included recurrent stroke or stroke onset longer than 72 h, renal or liver failure, acute infectious disease, tumor, hematologic disease, and patients who are unable to cooperate with physical examination. | LA 25, SA 17, CE 8 | Diagnostic and prognostic value | MiR-223 was upregulated | MiR-223 was positively correlated with NIHSS score |
| Wang et al. [59] | miR-223 | Whole blood/less than 72 h | 79/75 | IS patients included in the study. | The exclusion criteria included recurrent stroke, intracranial tumor, multiple trauma, hematological system diseases, renal or liver failure, acute infectious diseases and other diseases affecting the hemogram. If the time from the onset of stroke symptoms to blood sample collection was longer than 72 h, the patient was excluded. | LA 37, SA 9, CE 5, UN 28 | Diagnostic value | MiR-223 in IS patients were greatly increased compared to the control | MiRNA-223 was negatively correlated with NIHSS scores, plasma level of IGF-1 was positively correlated with that of miRNA-223 |
| Ji et al. [62] | miR-9, miR-124 | Exosomes/plasma/the mean time of enrollment blood draw was 16.5 h. | 65/66 | IS patients were recruited after either MRI or CT imaging of the brain. | Patients with intracerebral hemorrhage or unknown etiology were excluded. | NA | Diagnostic and prognostic value | MiR-9 and miR-124 in IS patients were increased compared to the control | The levels of both miR-9 and miR-124 were positively correlated with NIHSS scores, infarct volumes and serum concentrations of IL-6. |
| Liu et al. [63] | miR-9, miR-124, miR-219 | Serum/24 h | 31/11 | Patients with IS 24 h after symptom onset were enrolled to the study. | Exclusion criteria were being under 18 years old, being on thrombolytic or anticoagulant therapies, intracerebral hemorrhage or hemorrhagic transformation, other complicating neurological or neuropsychological diseases, cancer, comorbidity with proinflammatory conditions, and clinical signs of infection at any time during the study. | NA | Inflammatory value | MiR-124 was downregulated | Both serum miR-124 and miR-9 levels within 24 h were negatively correlated with infarct volume and plasma hs-CRP levels. All three miRNAs were negatively correlated with MMP-9 levels. |
| Jickling et al. [67] | miR-122, miR-148a, Let-7i, miR-19a, miR-320d, miR-4429, miR-363, miR-487b | Whole blood/NA | 24/24 | Patients with IS were enrolled to the study. Stroke diagnosis restricted diffusion on brain MRI (positive DWI-MRI). | Patients with infection (current or within 2 weeks of stroke), immunosuppressive therapy, lymphoma, leukemia, or treatment with thrombolytic therapy were excluded from study. | LA 8, SA 8, CE 8 | Diagnostic value | In patients with IS, miR-122, miR-148a, let-7i, miR-19a, miR-320d, miR-4429 were decreased and miR-363, miR-487b were increased compared to vascular risk factor controls. | MiRNAs may regulates NF-κB and toll-like receptor signaling pathways, which are involved in immune activation, leukocyte extravasation and thrombosis. |
| Li et al. [68] | In total 115 miRNAs were screened miR-32-3p, miR-106b-5p, miR-423-5p, miR-451a, miR-1246, miR-1299, miR-3149, miR-4739, miR-224-3p, miR-377-5p, miR-518b, miR-532-5p, miR-1913 | Serum/24 h | 117/82 | IS patients (aged >45) within 24 h after stroke onset were enrolled to the study. | Exclusion criteria included other types of stroke (TIA, subarachnoid hemorrhage, brain tumors, and cerebrovascular malformation); severe systemic diseases, i.e., pulmonary fibrosis, endocrine, and metabolic diseases (except type 2 diabetes); inflammatory and autoimmune diseases; and serious chronic diseases, for example, hepatic cirrhosis and renal failure. | NA | Diagnostic value of upregulated miR-32-3p, miR-106b-5p, miR-1246, and downregulated miR-532-5p | MiR-32-3p, miR-106b-5p, miR-423-5p, miR-451a, miR-1246, miR-1299, miR-3149, miR-4739 were upregulated | MiR-106b may affect multiple pathways such as apoptosis, oxidation, angiogenesis, and neurogenesis in IS. |
| Tan et al. [72] | in total 157 miRNAs were screened hsa-let-7f, miR-126, -1259, -142-3p, -15b,-186, -519e, -768-5p hsa-let-7e, miR-1184, -1246, -1261, -1275, -1285, -1290, -181a, -25*, -513a-5p, -550, -602, -665, -891a, -933, -939, -923 | Whole blood/within 6–18 months | 19/5 | Asian stroke patients between the ages of 18 to 49 were enrolled to the study. Blood samples collected from stroke patients within 6–18 months in time scale from the index stroke. IS was confirmed either with CT or MRI of the brain. | NA | LA 8, SA 3, CE 5, UN 3 | Diagnostic value | In total 138 miRNAs were upregulated and in total 19 miRNAs were downregulated. hsa-let-7f, miR-126, -1259, -142-3p, -15b,-186, -519e, -768-5p were downregulated, hsa-let-7e, miR-1184, -1246, -1261, -1275, -1285, -1290, -181a, -25*, -513a-5p, -550, -602, -665, -891a, -933, -939, -923 were upregulated. | Among the upregulated miRNAs, the expression of miR-101, -106b, -130a, -144, -18a, -18b, -19a, -19b, -194, -22, -22, -29b, -29c and -363 were the highest for LA (mRS = 3) stroke sample and positively correlated to the profile observed for LA mRS > 2 |
| Sepramaniam et al. [73] | In total 314 miRNAs were screened. hsa-let-7e, hsa-miR-125b-2*, hsa-miR-1261, hsa-miR-129-5p, hsa-miR-1321, hsa-miR-135b, hsa-miR-145, hsa-miR-184, hsa-miR-187*, hsa-miR-196a*, hsa-miR-198, hsa-miR-200b*, hsa-miR-210, hsa-miR-214, hsa-miR-220c, hsa-miR-25*, hsa-miR-602, hsa-miR-611, hsa-miR-617, hsa-miR-623, hsa-miR-627, hsa-miR-637, hsa-miR-638, hsa-miR-659, hsa-miR-668, hsa-miR-671-5p, hsa-miR-675, hsa-miR-920, hsa-miR-933, hsa-miR-943, hsa-miR-99a, hsa-let-7a, hsa-let-7b*, hsa-let-7c, hsa-let-7d*, hsa-let-7f, hsa-let-7g, hsa-let-7i, hsa-miR-106b*, hsa-miR-126, hsa-miR-1299, hsa-miR-130a, hsa-miR-151-5p, hsa-miR-18a*, hsa-miR-182, hsa-miR-183, hsa-miR-186, hsa-miR-192, hsa-miR-20a, hsa-miR-208a, hsa-miR-22*, hsa-miR-500, hsa-miR-500*, hsa-miR-501-5p, hsa-miR-502-5p, hsa-miR-502-3p, hsa-miR-505*, hsa-miR-532-5p, hsa-miR-574-5p, hsa-miR-574-3p, hsa-miR-576-5p, hsa-miR-625, hsa-miR-629, hsa-miR-652, hsa-miR-7, hsa-miR-886-5p, hsa-miR-92a, hsa-miR-93*, hsa-miR-96 | Whole blood/24 h, 48 h, 7 days, from 2 months to 2 years from stroke onset | 169/118 | Patients with IS were enrolled to the study. IS was confirmed through either MRI or CT imaging of the brain. | NA | NA | Diagnostic value, potential diagnostic biomarkers; miR-125b-2*, -27a*, -422a, -488 and -627 | Among the significant 105 miRNAs, 58 were downregulated while 47 were upregulated. Upregulated miRNAs: hsa-let-7e, hsa-miR-125b-2*, hsa-miR-1261, hsa-miR-129-5p, hsa-miR-1321, hsa-miR-135b, hsa-miR-145, hsa-miR-184, hsa-miR-187*, hsa-miR-196a*, hsa-miR-198, hsa-miR-200b*, hsa-miR-210, hsa-miR-214, hsa-miR-220c, hsa-miR-25*, hsa-miR-602, hsa-miR-611, hsa-miR-617, hsa-miR-623, hsa-miR-627, hsa-miR-637, hsa-miR-638, hsa-miR-659, hsa-miR-668, hsa-miR-671-5p, hsa-miR-675, hsa-miR-920, and downregulated miRNAs: hsa-let-7a, hsa-let-7b*, hsa-let-7c, hsa-let-7d*, hsa-let-7f, hsa-let-7g, hsa-let-7i, hsa-miR-106b*, hsa-miR-126, hsa-miR-1299, hsa-miR-130a, hsa-miR-151-5p, hsa-miR-18a*, hsa-miR-182, hsa-miR-183, hsa-miR-186, hsa-miR-192, hsa-miR-20a, hsa-miR-208a, hsa-miR-22*, hsa-miR-500, hsa-miR-500*, hsa-miR-501-5p, hsa-miR-502-5p, hsa-miR-502-3p, hsa-miR-505*, hsa-miR-532-5p, hsa-miR-574-5p, hsa-miR-574-3p, hsa-miR-576-5p, hsa-miR-625, hsa-miR-629, hsa-miR-652, hsa-miR-7, hsa-miR-886-5p, hsa-miR-92a, hsa-miR-93*, hsa-miR-96 | |
| Wang et al. [74] | Microarray revealed 17 upregulated miRNAs and 103 downregulated miRNAs in MRI(−) acute stroke patients compared with MRI(+) acute stroke patients, 33 upregulated miRNAs and 36 downregulated miRNAs in MRI(+) acute stroke hsa-miR-106b-5P, hsa-miR-4306, hsa-miR-320e hsa-miR-320d | Plasma/0–3 h 23 patients, 3–6 h 37 patients, 6–12 h 31 patients, 12–24 h 45 patients. | 136/116 | The inclusion criteria consisted of having IS or TIA and having no history of coronary artery disease. | Patients were excluded if they had received intravenous thrombolytic or anticoagulant therapy before the initial blood samples were collected. | LA 60, SA 51, CE 23, UDN 2 | Diagnostic value of hsa-miR-106b-5P, hsa-miR-4306, hsa-miR-320e, and hsa-miR-320d | hsa-miR-106b-5p hsa-miR-4306 increased, hsa-miR-320e and hsa-miR-320d decreased which are associated with diagnostic value | NA |
| Tian et al. [75] | hsa-mir-4454, hsa-mir-140-3p, hsa-mir-106b-5p, hsa-mir-25-3p, hsa-mir-16-5p, hsa-mir-223-3p, hsa-mir-484, hsa-mir-130b-3p, hsa-mir-151a-3p, hsa-mir-130a-3p, hsa-mir-93-5p, hsa-mir-107 | Plasma/6 h | 40/30 | Inclusion criteria: time duration from stroke onset to admission was less than 6 h. | Patients with immune disease, trauma, coronary heart disease, organ failure, tumor, and infection were excluded from the study. | LA 10, SA 8, CE 14, UN 7, ODE 1 | Diagnostic and prognostic value of miR-16 | MiR-140, miR-106b, miR-130a, miR-16, miR-223, miR-93, miR-484, miR-25, miR-130b, miR-107, and miR-151 were upregulated and miR-4454 was downregulated | Plasma concentrations of miR-16 were related to TOAST criteria, OCSP criteria, and the prognosis of HACI patients |
| Tiedt et al. [76] | hsa-let-7b-3p, hsa-let-7d-3p, hsa-let-7f-5p, hsa-let-7i-5p, hsa-miR-1, hsa-miR-16-2-3p, hsa-miR-17-3p, hsa-miR-17-5p, hsa-miR-18a-3p, hsa-miR-18a-5p, hsa-miR-20a-5p, hsa-miR-26b-5p, hsa-miR-92a-3p, hsa-miR-99b-5p, hsa-miR-101-3p, hsa-miR-125a-5p, hsa-miR-125b-5p, hsa-miR-126-5p, hsa-miR-130a-3p, hsa-miR-140-3p, hsa-miR-143-3p, hsa-miR-181a-5p, hsa-miR-193a-5p, hsa-miR-378a-3p, hsa-miR-423-3p, hsa-miR-532-5p, hsa-miR-660-5p, hsa-miR-3158-3p, hsa-miR-3158-5p, hsa-miR-3184-5p hsa-miR-3688-3p, hsa-miR-3688-5p | Plasma/24 h, 48 h, 72 h, 90th day. | 260/160 | IS and TIA patients were enrolled to the study. | Patients with active malignant disease, inflammatory or infectious diseases, surgery within the last three months and prior medication with low-molecular or unfractionated heparin within the last month were excluded. Further, for the discovery sample patients with prior use of antiplatelet medication within the last month, a history of myocardial infarction, stroke, or TIA, or signs for silent CNS infarction on neuroimaging were also excluded. For the replication sample, patients with prior medication with low-molecular or unfractionated heparin within the last month were excluded. | LA 61, SA 18, CE 79, UN 96 | Diagnostic value of miR-125a-5p, miR-125b-5p, miR-143-3p | MiR-125a-5p, miR-125b-5p, and miR-143-3p were upregulated. | The transformed infarct volumes of IS patients (N = 188) were correlated with expression levels of miR-125a-5p, miR-125b-5p, and miR-143-3p. |
| Mick et al. [77] | ex-RNAs by RNASeq (331 miRNAs, 97 piRNAs, and 43 snoRNAs) for RT-qPCR analysis: miR-877-5p, miR-124-3p, miR-320d, snoRNA SNO1402, hsa-miR-656-3p, hsa-miR-941 | Plasma/NA | 2763 participants included from (Framingham Heart Study; Offspring Cohort Exam 8), unbiased next-generation sequencing conducted using plasma from 40 participants from the cohort. | Subjects were diagnosed with stroke based on review of medical records, including relevant hospitalizations, and clinic reported events by at least 2 neurologists agreeing on one of the following manifestations: definite cerebrovascular accident, atherothrombotic infarction of the brain, cerebral embolism, intracerebral hemorrhage, or subarachnoid hemorrhage. | NA | NA | NA | Observational study | miR-877-5p, miR-124-3p, and miR-320d) and one snoRNA (SNO1402) were independently associated with prevalent stroke, hsa-miR-656-3p and hsa-miR-941 were significantly associated with incident stroke |
| Chen et al. [64] | Let-7b, miR-23a, miR-126, miR-15a, miR-16, miR-17-5p, miR-19b, miR-29b, miR-339-5p, miR-21, miR-221, miR-32-3p, miR-106-5p, miR-532-5p, miR-145, miR-146b, miR-210 | Serum/24 h | 128/102 | Patients with IS within 24 h after symptoms were enrolled to the study. | Exclusion criteria were being under 18 years old, being on thrombolytic or anticoagulant therapies, intracerebral hemorrhage or hemorrhagic transformation, other complicating neurological or neuropsychological diseases, cancer, comorbidity with proinflammatory conditions, and clinical signs of infection at any time during the study. | NA | Diagnostic value for miR-146b. There is no significance of the expression of serum miRNAs among 5 IS groups in this study. It was suggested that miR-146b may be a biomarker for IS but not for separating subtypes of IS. | MiR-21, miR-145, miR-29b and miR-146b were significantly upregulated and miR-23a and miR-221 levels were significantly downregulated | Positive significant correlation was found between serum miR-146b level and plasma hs-CRP, infarct volume and NIHSS score, and serum IL-6 of patients. |
| Wu et al. [78] | 754 miRNAs were screened, 71 miRNAs were upregulated and 49 miRNAs were downregulated in IS patients | Serum/NA | 50/50 then it was confirmed with a larger cohort 177 IS, 81 TIA patients and 42 controls | IS and TIA patients were enrolled to the study. The diagnosis of IS was based on the acute occurrence of focal neurological deficit lasting for more than 24 h and was confirmed by the positive findings of brain CT and MRI. | Patients with a history of hemorrhagic infarction, peripheral arterial occlusive diseases, chronic liver/kidney diseases, primary/metastatic neoplasms or other malignant diseases were excluded. | NA | Prognostic value for miR-23b-3p and miR-29b-3p | MiR-23b-3p, miR-29b-3p, miR-181a-5p and miR-21–5p were markedly increased in IS patients. MiR-23b-3p, miR-29b-3p and miR-181a-5p were also significantly elevated in TIA patients | MiR-23b-3p levels in IS patients were positively related with discharge mRS scores, while miR-23b-3p and miR-29b-3p levels in IS patients were negatively related with discharge BI scores. |
| Ref | MicroRNA | AUC | Specificity | Sensitivity | |
|---|---|---|---|---|---|
| Long et al. [41] | miR-30a | 24 h | 0.91 | 80% | 94% |
| 1 week | 0.91 | 84% | 93% | ||
| 4 weeks | 0.92 | 84% | 90% | ||
| 24 weeks | 0.93 | 84% | 92% | ||
| miR-126 | 24 h | 0.92 | 84% | 92% | |
| 1 week | 0.94 | 86% | 90% | ||
| 4 weeks | 0.93 | 84% | 92% | ||
| 24 weeks | 0.92 | 82% | 92% | ||
| Let-7b | 24 h | 0.93 | 84% | 92% | |
| 1 week | 0.92 | 84% | 90% | ||
| 4 weeks | 0.92 | 86% | 92% | ||
| 24 weeks | 0.91 | 80% | 89% | ||
| Wu et al. [48] | miR-15a, | 0.698 | NA | NA | |
| miR-16, | 0.820 | ||||
| miR-17-5p | 0.784 | ||||
| miR-15a + miR-16 + miR-17-5p | 0.845 | ||||
| Peng et al. [43] | Let-7e | 0.86 | 73.4% | 82.8% | |
| miR-338 | 0.63 | 53.2% | 71.9% | ||
| Huang et al. [44] | Let-7e-5p | 0.82 | NA | NA | |
| Jin F. and Xing J. [53] | miR-126 | 0.654 | NA | NA | |
| miR-130a | 0.642 | ||||
| miR-222 | 0.584 | ||||
| miR-218 | 0.624 | ||||
| miR-185 | 0.601 | ||||
| miR-126 + miR-130a + miR-222 + miR-218 + miR-185 | 0.767 | ||||
| Chen et al. [61] | miR-223 | 0.859 | 78.8% | 84% | |
| Sepramaniam et al. [73] | Cohort 1 | Cohort 2 | NA | NA | |
| miR-125b-2* | 0.95 | 0.85 | |||
| miR-27a* | 0.89 | 0.86 | |||
| miR-422a | 0.92 | 0.86 | |||
| miR-488 | 0.87 | 0.86 | |||
| miR-627 | 0.84 | 0.76 | |||
| Tian et al. [75] | miR-16 (overall patients) | 0.775 | 87% | 69.7% | |
| miR-16 (LAA patients) | 0.952 | 91.3% | 100% | ||
| Wang et al. [74] | Total | MRI(+) | NA | NA | |
| hsa-miR-106b-5p | 0.999 | 0.962 | |||
| hsa-miR-4306 | 0.877 | 0.952 | |||
| hsa-miR-320e | 0.953 | 0.981 | |||
| hsa-miR-320d | 0.977 | 0.987 | |||
| Jia et al. [55] | CRP | 0.794 | NA | NA | |
| CRP+ miR-145 | 0.896 | ||||
| CRP + miR-23a | 0.816 | ||||
| CRP + miR-221 | 0.819 | ||||
| Tsai et al. [57] | miR-21/miR-221 (traditional risk factors) | 0.93 | NA | NA | |
| Ji et al. [62] | miR-9 | 0.8026 | NA | NA | |
| miR-124 | 0.6976 | ||||
| Tiedt et al. [76] | miR-125a-5p + miR-125b-5p + miR-143-3p | 0.663 (IS vs. TIA) | |||
| miR-125a-5p + miR-125b-5p + miR-143-3p + IL6 + NSE | 0.661 (IS vs. TIA) | ||||
| Chen et al. [64] | miR146b | 0.776 | NA | NA | |
| CRP | 0.782 | ||||
| IL-6 | 0.684 | ||||
| CRP+miR146b | 0.863 | ||||
| IL-6+miR146b | 0.819 | ||||
| CRP+IL-6+miR146b | 0.866 | ||||
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Eyileten, C.; Wicik, Z.; De Rosa, S.; Mirowska-Guzel, D.; Soplinska, A.; Indolfi, C.; Jastrzebska-Kurkowska, I.; Czlonkowska, A.; Postula, M. MicroRNAs as Diagnostic and Prognostic Biomarkers in Ischemic Stroke—A Comprehensive Review and Bioinformatic Analysis. Cells 2018, 7, 249. https://doi.org/10.3390/cells7120249
Eyileten C, Wicik Z, De Rosa S, Mirowska-Guzel D, Soplinska A, Indolfi C, Jastrzebska-Kurkowska I, Czlonkowska A, Postula M. MicroRNAs as Diagnostic and Prognostic Biomarkers in Ischemic Stroke—A Comprehensive Review and Bioinformatic Analysis. Cells. 2018; 7(12):249. https://doi.org/10.3390/cells7120249
Chicago/Turabian StyleEyileten, Ceren, Zofia Wicik, Salvatore De Rosa, Dagmara Mirowska-Guzel, Aleksandra Soplinska, Ciro Indolfi, Iwona Jastrzebska-Kurkowska, Anna Czlonkowska, and Marek Postula. 2018. "MicroRNAs as Diagnostic and Prognostic Biomarkers in Ischemic Stroke—A Comprehensive Review and Bioinformatic Analysis" Cells 7, no. 12: 249. https://doi.org/10.3390/cells7120249
APA StyleEyileten, C., Wicik, Z., De Rosa, S., Mirowska-Guzel, D., Soplinska, A., Indolfi, C., Jastrzebska-Kurkowska, I., Czlonkowska, A., & Postula, M. (2018). MicroRNAs as Diagnostic and Prognostic Biomarkers in Ischemic Stroke—A Comprehensive Review and Bioinformatic Analysis. Cells, 7(12), 249. https://doi.org/10.3390/cells7120249