Effectiveness of Autologous Platelet Concentrates in Management of Young Immature Necrotic Permanent Teeth—A Systematic Review and Meta-Analysis

 , , ,
, , ,  ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Study Selection
- Randomized clinical trials (RCTs);
- Studies with presence of at least one experimental group where APCs were used for treatment of young immature necrotic permanent teeth, compared to a control group using either blood-clot regeneration (BC) or any biomimetic agents;
- Studies with at least three subjects per group;
- Studies in English language only.
- Case reports, comments, conference proceedings, and nonrandomized clinical studies;
- Studies comparing APCs in either group with different preparation protocols or mode of delivery;
- Studies experimenting on vital teeth;
- Animal studies.
2.3. Data Extraction
2.4. Assessment of the Risk of Bias of the Studies
2.5. Analysis of Results
3. Results
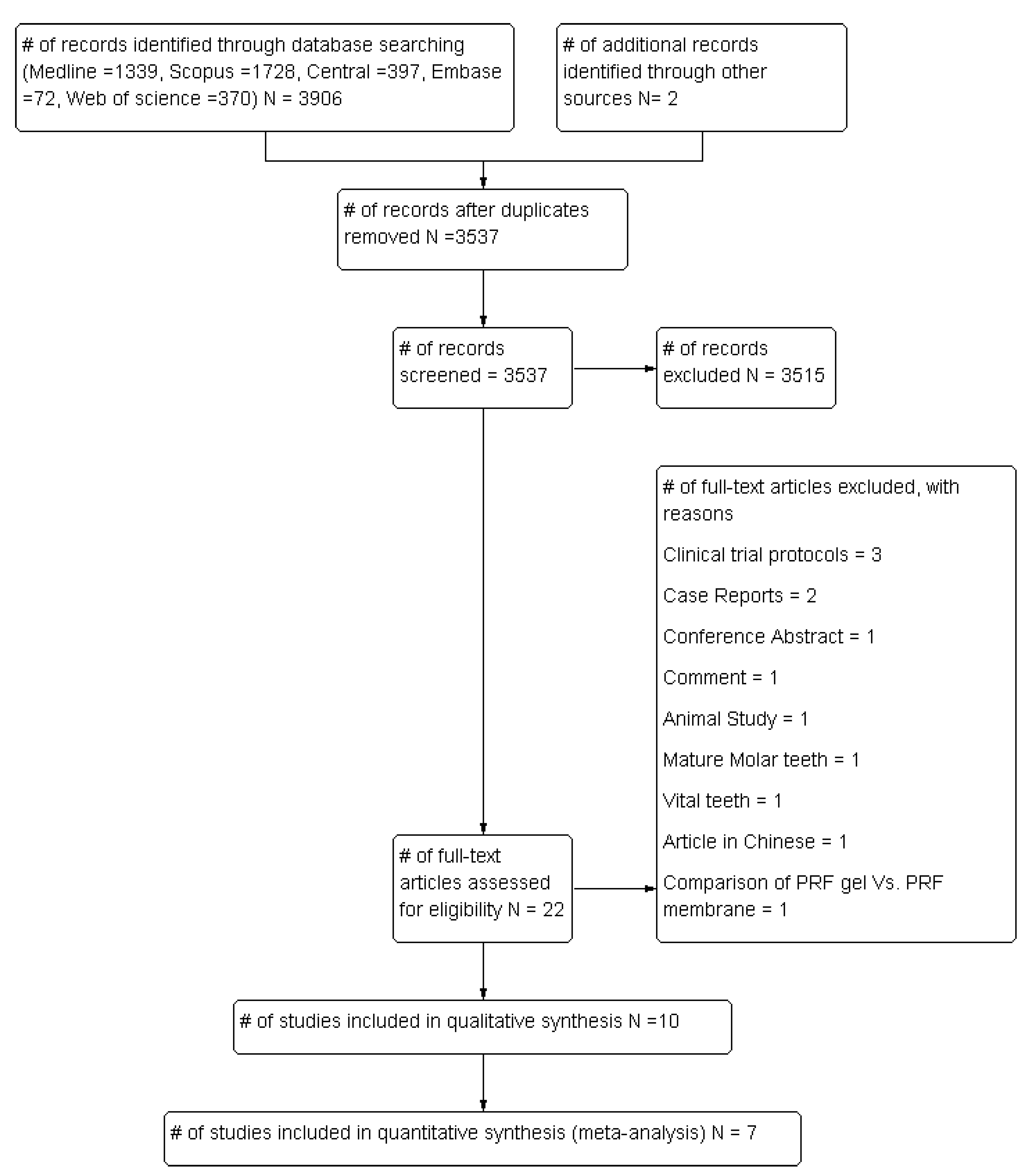
3.1. Selection of Studies
3.2. Characteristics of the Studies
3.3. Analysis of Risk of Bias of the Studies
3.4. Synthesis of Results (Meta-Analysis)
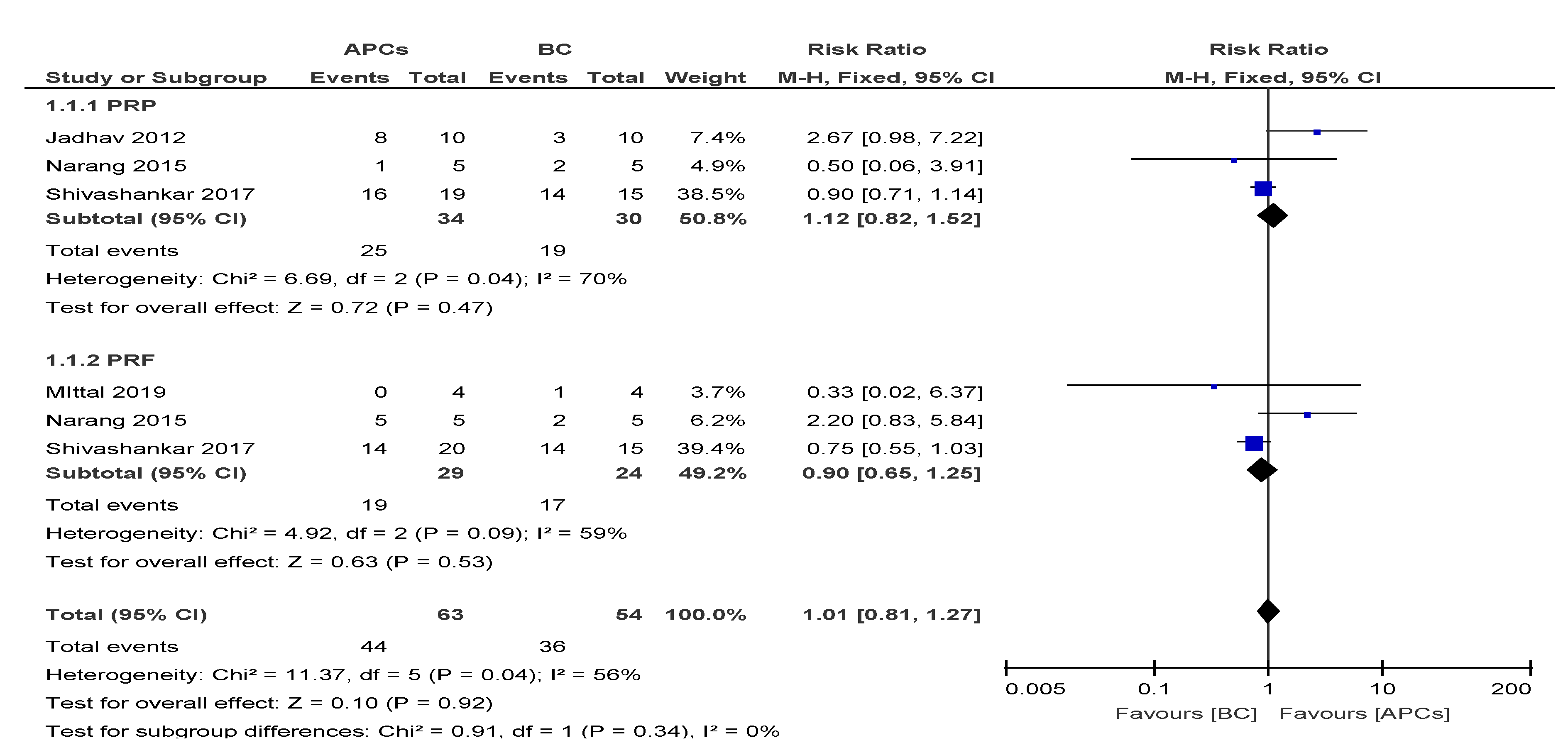
3.4.1. Dentinal Wall Thickness (DWT)
3.4.2. Increase in Root Length (RL)
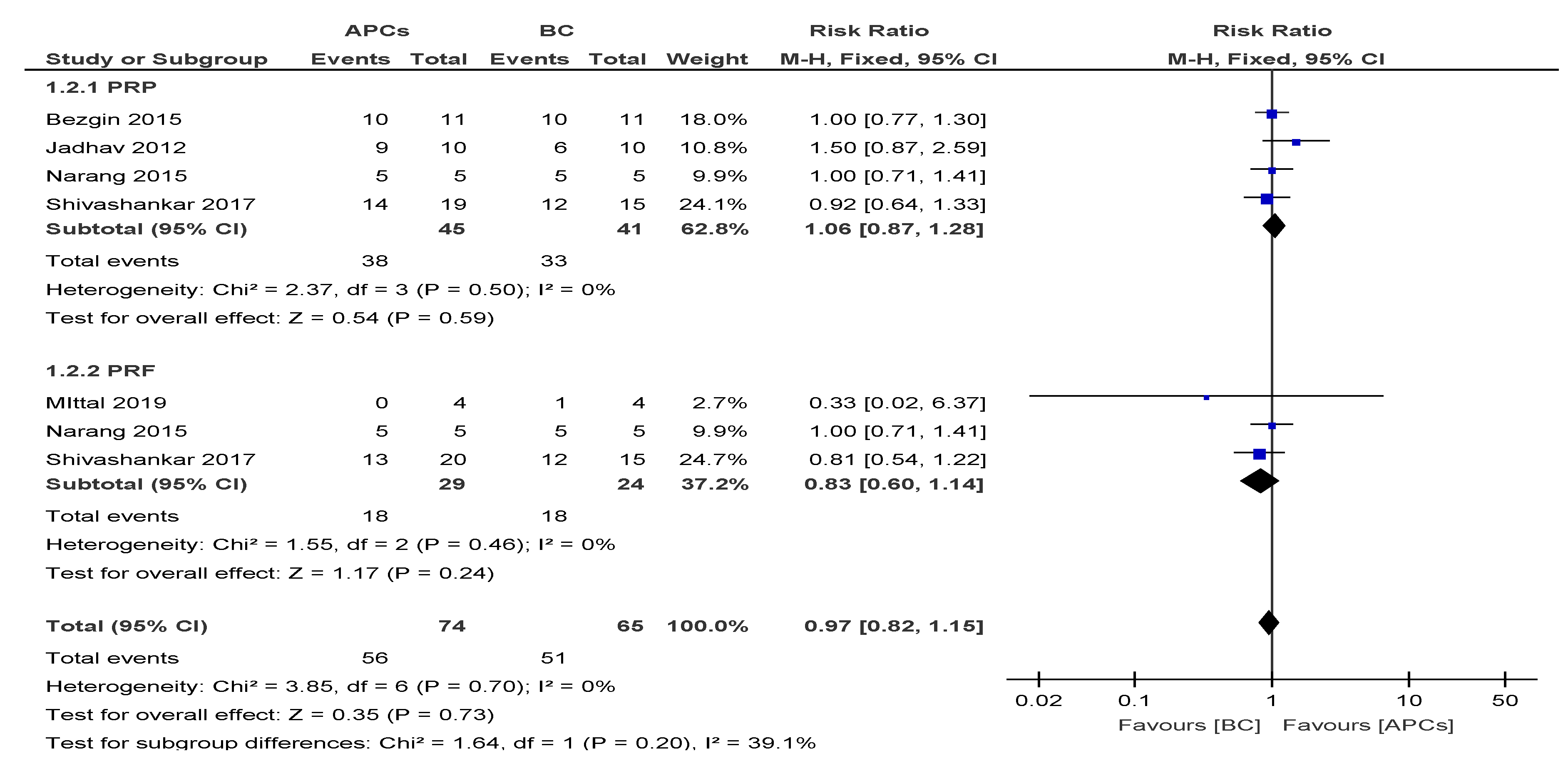
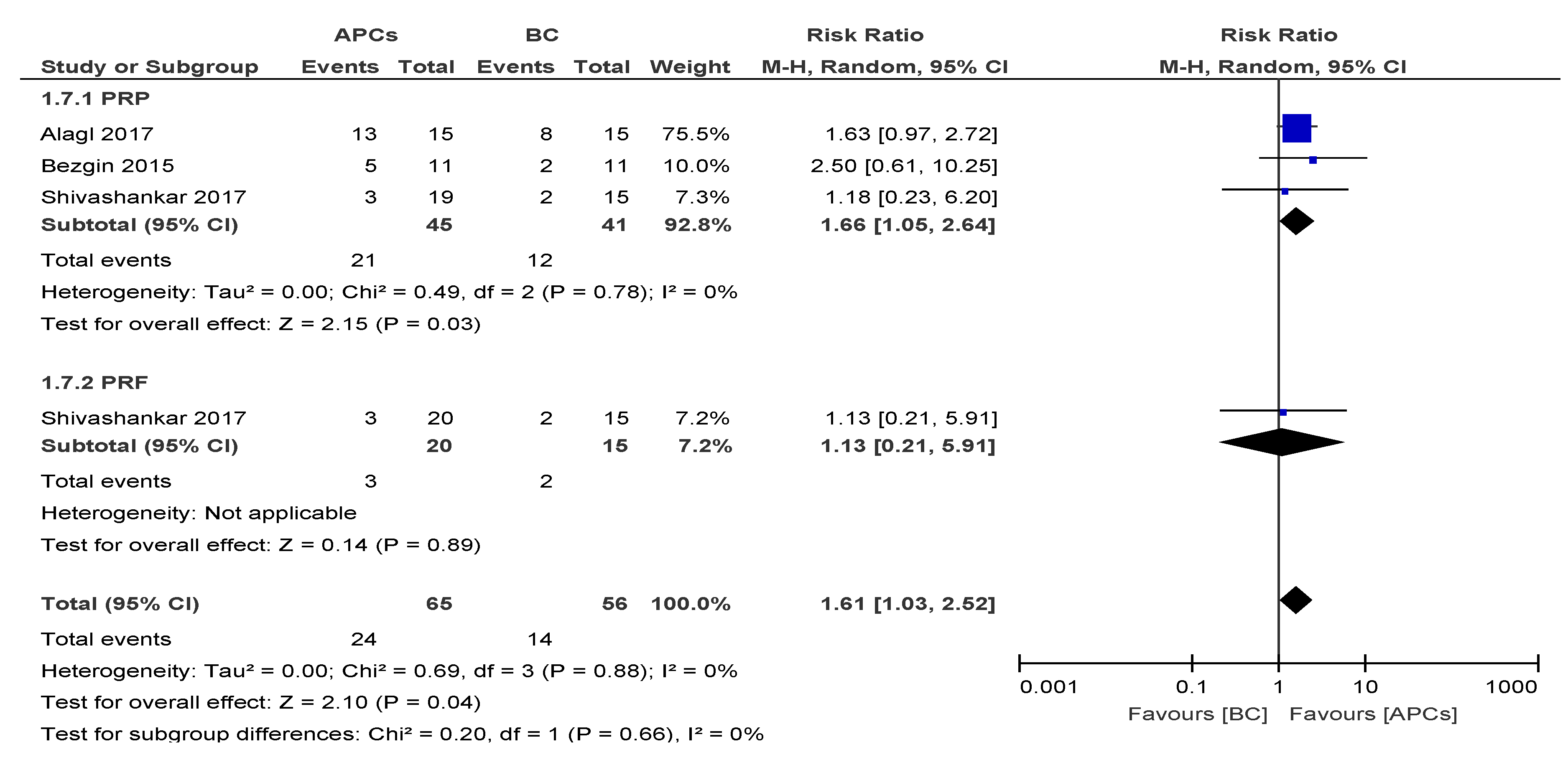
3.4.3. Apical Closure (AC)
3.4.4. Vitality Response
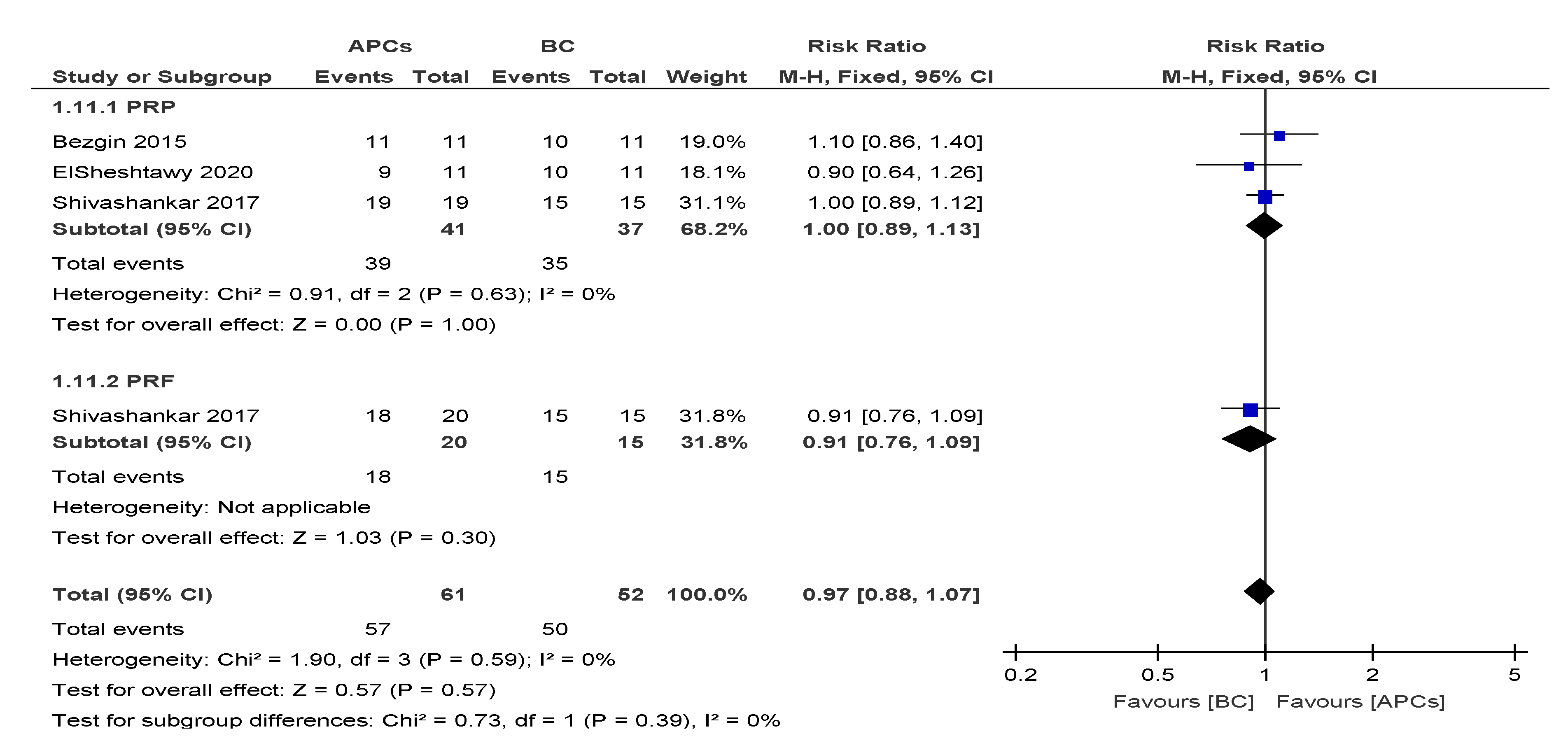
3.4.5. Success Rate (SR)
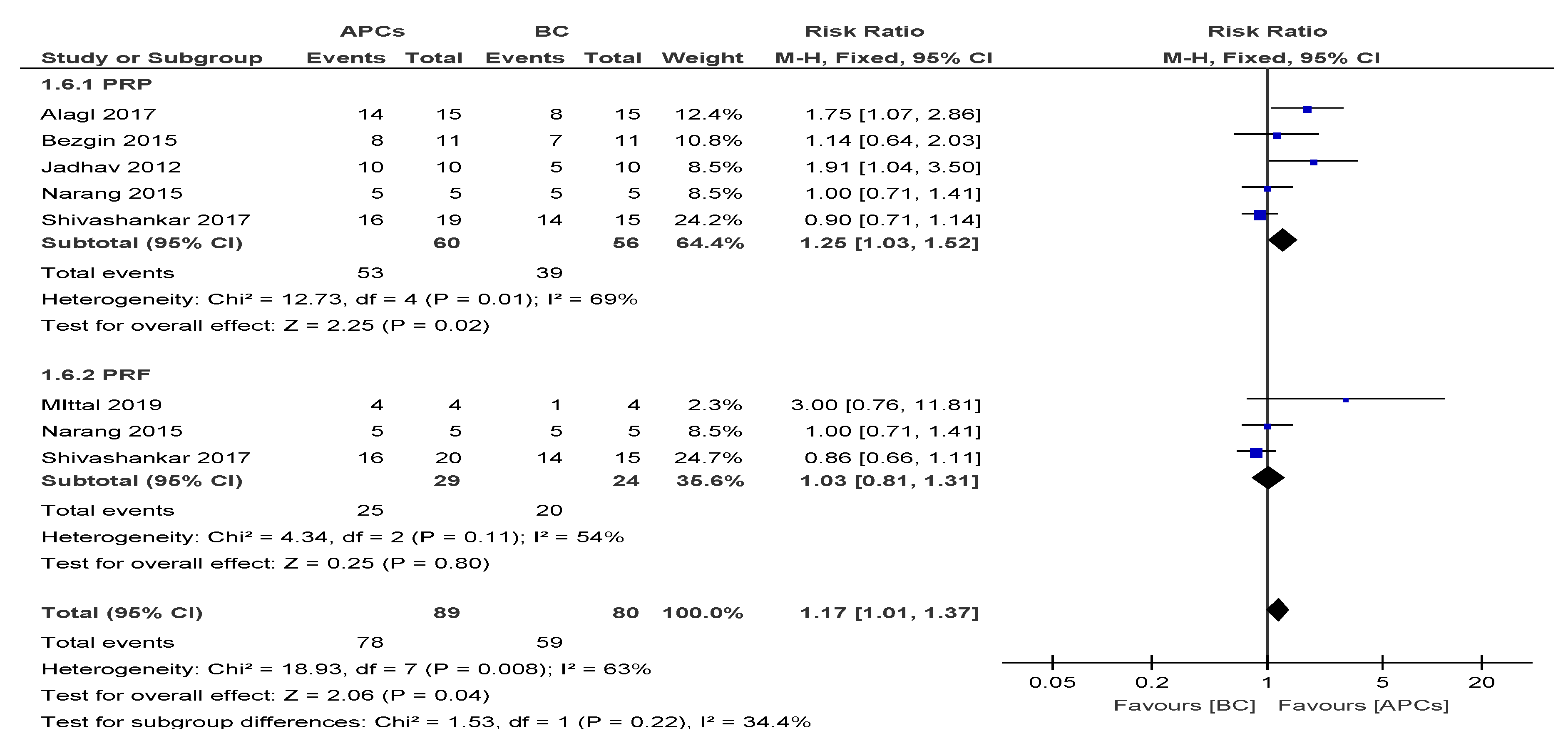
3.4.6. Calcific Barrier Formation (CB)
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Andreasen, J.O.; Farik, B.; Munksgaard, E.C. Long-term calcium hydroxide as a root canal dressing may increase risk of root fracture. Dent. Traumatol. 2002, 18, 134–137. [Google Scholar] [CrossRef] [PubMed]
- Kunert, M.; Lukomska-Szymanska, M. Bio-Inductive Materials in Direct and Indirect Pulp Capping—A Review Article. Materials 2020, 13, 1204. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Krawczyk-Stuss, M.; Ostrowska, A.; Lapinska, B.; Nowak, J.; Bołtacz-Rzepkowska, E. Evaluation of Shear Bond Strength of the Composite to Biodentine with Different Adhesive Systems. Dent. Med. Probl. 2015, 52, 434–439. [Google Scholar] [CrossRef] [Green Version]
- Lin, J.; Zeng, Q.; Wei, X.; Zhao, W.; Cui, M.; Gu, J.; Lu, J.; Yang, M.; Ling, J. Regenerative Endodontics Versus Apexification in Immature Permanent Teeth with Apical Periodontitis: A Prospective Randomized Controlled Study. J. Endod. 2017, 43, 1821–1827. [Google Scholar] [CrossRef]
- Cvek, M. Prognosis of luxated non-vital maxillary incisors treated with calcium hydroxide and filled with gutta-percha. A retrospective clinical study. Dent. Traumatol. 1992, 8, 45–55. [Google Scholar] [CrossRef]
- Bucchi, C.; Marcé-Nogué, J.; Galler, K.M.; Widbiller, M. Biomechanical performance of an immature maxillary central incisor after revitalization: A finite element analysis. Int. Endod. J. 2019, 52, 1508–1518. [Google Scholar] [CrossRef]
- Murray, P.E.; Garcia-Godoy, F.; Hargreaves, K.M. Regenerative Endodontics: A Review of Current Status and a Call for Action. J. Endod. 2007, 33, 377–390. [Google Scholar] [CrossRef]
- Kaushik, S.N.; Kim, B.; Walma, A.M.C.; Choi, S.C.; Wu, H.; Mao, J.J.; Jun, H.-W.; Cheon, K. Biomimetic microenvironments for regenerative endodontics. Biomater. Res. 2016, 20, 14. [Google Scholar] [CrossRef] [Green Version]
- Murray, P. Platelet-Rich Plasma and Platelet-Rich Fibrin Can Induce Apical Closure More Frequently Than Blood-Clot Revascularization for the Regeneration of Immature Permanent Teeth: A Meta-Analysis of Clinical Efficacy. Front. Bioeng. Biotechnol. 2018, 6. [Google Scholar] [CrossRef] [Green Version]
- American Association of Endodontists. AAE Clinical Considerations for a Regenerative Procedure. Available online: https://www.aae.org/specialty/wp-content/uploads/sites/2/2018/06/ConsiderationsForRegEndo_AsOfApril2018.pdf (accessed on 4 October 2020).
- Ezzatt, O.M. Autologous Platelet Concentrate Preparations in Dentistry. Biomed. J. Sci. Tech. Res. 2018, 8, 1–10. [Google Scholar] [CrossRef]
- Ehrenfest, D.M.D.; Andía, I.; Zumstein, M.A.; Zhang, C.-Q.; Pinto, N.R.; Bielecki, T. Classification of platelet concentrates (Platelet-Rich Plasma-PRP, Platelet-Rich Fibrin-PRF) for topical and infiltrative use in orthopedic and sports medicine: Current consensus, clinical implications and perspectives. Muscle Ligaments Tendons J. 2014, 4, 3–9. [Google Scholar] [CrossRef] [Green Version]
- Anitua, E.; Sánchez, M.; Nurden, A.T.; Nurden, P.; Orive, G.; Andía, I. New insights into and novel applications for platelet-rich fibrin therapies. Trends Biotechnol. 2006, 24, 227–234. [Google Scholar] [CrossRef] [PubMed]
- Narang, I.; Mittal, N.; Mishra, N. A comparative evaluation of the blood clot, platelet-rich plasma, and platelet-rich fibrin in regeneration of necrotic immature permanent teeth: A clinical study. Contemp. Clin. Dent. 2015, 6, 63–68. [Google Scholar] [CrossRef]
- Del Fabbro, M.; Lolato, A.; Panda, S.; Corbella, S.; Satpathy, A.; Das, A.C.; Kumar, M.; Taschieri, S. Methodological Quality Assessment of Systematic Reviews on Autologous Platelet Concentrates for the Treatment of Periodontal Defects. J. Évid. Based Dent. Pr. 2017, 17, 239–255. [Google Scholar] [CrossRef] [PubMed]
- Panda, S.; Karanxha, L.; Goker, F.; Satpathy, A.; Taschieri, S.; Angelo, F.L.; Das, A.C.; Kumar, M.; Panda, S.; Del Fabbro, M. Autologous Platelet Concentrates in Treatment of Furcation Defects-A Systematic Review and Meta-Analysis. Int. J. Mol. Sci. 2019, 20, 1347. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Panda, S.; Sankari, M.; Satpathy, A.; Jayakumar, D.; Mozzati, M.; Mortellaro, C.; Gallesio, G.; Taschieri, S.; Del Fabbro, M. Adjunctive Effect of Autologus Platelet-Rich Fibrin to Barrier Membrane in the Treatment of Periodontal Intrabony Defects. J. Craniofacial Surg. 2016, 27, 691–696. [Google Scholar] [CrossRef] [PubMed]
- Panda, S.; Doraiswamy, J.; Malaiappan, S.; Varghese, S.; Del Fabbro, M. Additive effect of autologous platelet concentrates in treatment of intrabony defects: A systematic review and meta-analysis. J. Investig. Clin. Dent. 2014, 7, 13–26. [Google Scholar] [CrossRef]
- Chatterjee, S.S.; Das, A.C.; Panda, S. Platelet Rich Fibrin: A Promising Innovation in Periodontics. Indian J. Public Heal. Res. Dev. 2019, 10, 772. [Google Scholar] [CrossRef]
- Del Fabbro, M.; Karanxha, L.; Panda, S.; Bucchi, C.; Doraiswamy, J.N.; Sankari, M.; Ramamoorthi, S.; Varghese, S.; Taschieri, S. Autologous platelet concentrates for treating periodontal infrabony defects. Cochrane Database Syst. Rev. 2018, 11, CD011423. [Google Scholar] [CrossRef]
- Del Fabbro, M.; Panda, S.; Jayakumar, N.D.; Sankari, M.; Varghese, S.; Ramamoorthi, S.; Ceci, C.; Ceresoli, V.; Taschieri, S. Autologous platelet concentrates for treatment of periodontal defects. Cochrane Database Syst. Rev. 2014. [Google Scholar] [CrossRef]
- Supplement, D.; Testori, T.; Panda, S.; Clauser, T.; Scaini, R.; Zuffetti, F.; Capelli, M.; Taschieri, S.; Mortellaro, C.; Del Fabbro, M. Short implants and platelet-rich fibrin for transcrestal sinus floor elevation: A prospective multicenter clinical study. J. Biol. Regul. Homeost. Agents 2020, 33, 121–135. [Google Scholar]
- Del Fabbro, M.; Bortolin, M.; Taschieri, S. Is autologous platelet concentrate beneficial for post-extraction socket healing? A systematic review. Int. J. Oral Maxillofac. Surg. 2011, 40, 891–900. [Google Scholar] [CrossRef] [PubMed]
- Del Fabbro, M.; Panda, S.; Taschieri, S. Adjunctive Use of Plasma Rich in Growth Factors for Improving Alveolar Socket Healing: A Systematic Review. J. Évid. Based Dent. Pr. 2018, 19, 166–176. [Google Scholar] [CrossRef] [PubMed]
- Del Fabbro, M.; Lolato, A.; Bucchi, C.; Taschieri, S.; Weinstein, R.L.; Information, P.E.K.F.C. Autologous Platelet Concentrates for Pulp and Dentin Regeneration: A Literature Review of Animal Studies. J. Endod. 2016, 42, 250–257. [Google Scholar] [CrossRef]
- Lolato, A.; Bucchi, C.; Taschieri, S.; El Kabbaney, A.; Del Fabbro, M. Platelet concentrates for revitalization of immature necrotic teeth: A systematic review of the clinical studies. Platelets 2016, 27, 383–392. [Google Scholar] [CrossRef]
- Metlerska, J.; Fagogeni, I.; Nowicka, A. Efficacy of Autologous Platelet Concentrates in Regenerative Endodontic Treatment: A Systematic Review of Human Studies. J. Endod. 2019, 45, 20–30. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; A Ioannidis, J.P.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: Explanation and elaboration. BMJ 2009, 339, b2700. [Google Scholar] [CrossRef] [Green Version]
- Elsheshtawy, A.S.; Nazzal, H.; El Shahawy, O.I.; El Baz, A.A.; Ismail, S.M.; Kang, J.; Ezzat, K.M. The effect of platelet-rich plasma as a scaffold in regeneration/revitalization endodontics of immature permanent teeth assessed using 2-dimensional radiographs and cone beam computed tomography: A randomized controlled trial. Int. Endod. J. 2020, 53, 905–921. [Google Scholar] [CrossRef]
- Mittal, N.; Parashar, V. Regenerative Evaluation of Immature Roots using PRF and Artificial Scaffolds in Necrotic Permanent Teeth: A Clinical Study. J. Contemp. Dent. Pr. 2019, 20, 720–726. [Google Scholar] [CrossRef]
- Ragab, R.A.; El Lattif, A.E.A.; Dokky, N.A.E.W.E. Comparative Study between Revitalization of Necrotic Immature Permanent Anterior Teeth with and without Platelet Rich Fibrin: A Randomized Controlled Trial. J. Clin. Pediatr. Dent. 2019, 43, 78–85. [Google Scholar] [CrossRef]
- Ulusoy, A.T.; Turedi, I.; Cimen, M.; Cehreli, Z.C. Evaluation of Blood Clot, Platelet-rich Plasma, Platelet-rich Fibrin, and Platelet Pellet as Scaffolds in Regenerative Endodontic Treatment: A Prospective Randomized Trial. J. Endod. 2019, 45, 560–566. [Google Scholar] [CrossRef]
- Rizk, H.M.; Al-Deen, M.S.S.; Emam, A.A. Regenerative Endodontic Treatment of Bilateral Necrotic Immature Permanent Maxillary Central Incisors with Platelet-rich Plasma versus Blood Clot: A Split Mouth Double-blinded Randomized Controlled Trial. Int. J. Clin. Pediatr. Dent. 2019, 12, 332–339. [Google Scholar] [CrossRef]
- Shivashankar, V.Y.; Johns, D.A.; Maroli, R.K.; Sekar, M.; Chandrasekaran, R.; Karthikeyan, S.; Renganathan, S.K. Comparison of the Effect of PRP, PRF and Induced Bleeding in the Revascularization of Teeth with Necrotic Pulp and Open Apex: A Triple Blind Randomized Clinical Trial. J. Clin. Diagn. Res. 2017, 11, ZC34–ZC39. [Google Scholar] [CrossRef]
- Alagl, A.; Bedi, S.; Hassan, K.; Alhumaid, J. Use of platelet-rich plasma for regeneration in non-vital immature permanent teeth: Clinical and cone-beam computed tomography evaluation. J. Int. Med Res. 2017, 45, 583–593. [Google Scholar] [CrossRef]
- Bezgin, T.; Yilmaz, A.D.; Celik, B.N.; Kolsuz, M.E.; Sönmez, I.S. Efficacy of Platelet-rich Plasma as a Scaffold in Regenerative Endodontic Treatment. J. Endod. 2015, 41, 36–44. [Google Scholar] [CrossRef]
- Jadhav, G.; Shah, N.; Logani, A. Revascularization with and without Platelet-rich Plasma in Nonvital, Immature, Anterior Teeth: A Pilot Clinical Study. J. Endod. 2012, 38, 1581–1587. [Google Scholar] [CrossRef]
- Dohan, D.M.; Choukroun, J.; Diss, A.; Dohan, S.L.; Dohan, A.; Mouhyi, J.; Gogly, B. Platelet-rich fibrin (PRF): A second-generation platelet concentrate. Part I: Technological concepts and evolution. Oral Surgery Oral Med. Oral Pathol. Oral Radiol. Endodontology 2006, 101, e37–e44. [Google Scholar] [CrossRef]
- Chrepa, V.; Joon, R.; Austah, O.; Diogenes, A.; Hargreaves, K.M.; Ezeldeen, M.; Ruparel, N.B. Clinical Outcomes of Immature Teeth Treated with Regenerative Endodontic Procedures—A San Antonio Study. J. Endod. 2020, 46, 1074–1084. [Google Scholar] [CrossRef]
- Galler, K.; Krastl, G.; Simon, S.; Van Gorp, G.; Meschi, N.; Vahedi, B.; Lambrechts, P.; Dummer, P.M. European Society of Endodontology Position Statement: Revitalisation Procedures. Int. Endod. J. 2016, 49, 717–723. [Google Scholar] [CrossRef]
- Shokouhinejad, N.; Khoshkhounejad, M.; Alikhasi, M.; Bagheri, P.; Camilleri, J. Prevention of coronal discoloration induced by regenerative endodontic treatment in an ex vivo model. Clin. Oral Investig. 2017, 22, 1725–1731. [Google Scholar] [CrossRef] [Green Version]
- De-Jesus-Soares, A.; Prado, M.C.; Nardello, L.C.; Pereira, A.C.; Cerqueira-Neto, A.C.C.; Nagata, J.Y.; Martinez, E.F.; Frozoni, M.; Gomes, B.P.A.; Pinheiro, E.T. Clinical and Molecular Microbiological Evaluation of Regenerative Endodontic Procedures in Immature Permanent Teeth. J. Endod. 2020. [Google Scholar] [CrossRef] [PubMed]
- Almutairi, W.; Yassen, G.H.; Aminoshariae, A.; Williams, K.A.; Mickel, A. Regenerative Endodontics: A Systematic Analysis of the Failed Cases. J. Endod. 2019, 45, 567–577. [Google Scholar] [CrossRef] [PubMed]
- Del Fabbro, M.; Bortolin, M.; Taschieri, S.; Ceci, C.; Weinstein, R.L. Antimicrobial properties of platelet-rich preparations. A systematic review of the current pre-clinical evidence. Platelets 2016, 27, 276–285. [Google Scholar] [CrossRef]
- Kang, Y.-H.; Jeon, S.H.; Park, J.-Y.; Chung, J.H.; Choung, Y.-H.; Choung, H.-W.; Kim, E.-S.; Choung, P.-H. Platelet-Rich Fibrin is a Bioscaffold and Reservoir of Growth Factors for Tissue Regeneration. Tissue Eng. Part A 2011, 17, 349–359. [Google Scholar] [CrossRef] [PubMed]
- Kobayashi, E.; Flückiger, L.; Fujioka-Kobayashi, M.; Sawada, K.; Sculean, A.; Schaller, B.; Miron, R.J. Comparative release of growth factors from PRP, PRF, and advanced-PRF. Clin. Oral Investig. 2016, 20, 2353–2360. [Google Scholar] [CrossRef] [PubMed]
- Savović, J.; Turner, R.M.; Mawdsley, D.; Jones, H.E.; Beynon, R.; Higgins, J.P.T.; Sterne, J.A.C. Association Between Risk-of-Bias Assessments and Results of Randomized Trials in Cochrane Reviews: The ROBES Meta-Epidemiologic Study. Am. J. Epidemiol. 2017, 187, 1113–1122. [Google Scholar] [CrossRef] [PubMed]
- Martin, D.E.; De Almeida, J.F.A.; Henry, M.A.; Khaing, Z.Z.; Schmidt, C.E.; Teixeira, F.B.; Diogenes, A.; De Almeida, J.F.A. Concentration-dependent Effect of Sodium Hypochlorite on Stem Cells of Apical Papilla Survival and Differentiation. J. Endod. 2014, 40, 51–55. [Google Scholar] [CrossRef] [PubMed]
- Galler, K.M.; Widbiller, M.; Buchalla, W.; Eidt, A.; Hiller, K.-A.; Hoffer, P.C.; Schmalz, G. EDTA conditioning of dentine promotes adhesion, migration and differentiation of dental pulp stem cells. Int. Endod. J. 2015, 49, 581–590. [Google Scholar] [CrossRef] [PubMed]
- Rahhal, J.G.; Rovai, E.S.; Holzhausen, M.; Caldeira, C.L.; Santos, C.F.; Sipert, C.R. Root canal dressings for revascularization influence in vitro mineralization of apical papilla cells. J. Appl. Oral Sci. 2019, 27, e20180396. [Google Scholar] [CrossRef]
- Kim, J.-H.; Kim, Y.; Shin, S.-J.; Park, J.-W.; Jung, I.-Y. Tooth Discoloration of Immature Permanent Incisor Associated with Triple Antibiotic Therapy: A Case Report. J. Endod. 2010, 36, 1086–1091. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author | Type of Study | Country | n patient | n Teeth | Groups of Study | n per Group | Tooth | Etiology of Pulpal Necrosis | Follow-up Time in Months |
|---|---|---|---|---|---|---|---|---|---|
| ElSheshtawy et al. 2020 [29] | RCT, Parallel | Egypt | 26 | 26 | A. PRP | 11 | Incisor | Secondary to trauma and dens invaginatus | 12 |
| B. BC | 11 | ||||||||
| Mittal et al. 2019 [30] | RCT, Parallel | India | 16 | 16 | A. PRF | 4 | Incisor | Secondary to trauma/caries | 12 |
| B. BC | 4 | ||||||||
| Ragab et al. 2019 [31] | RCT, Parallel | Egypt | 22 | 22 | A. PRF | 11 | Incisor | Secondary to trauma | 12 |
| B. BC | 11 | ||||||||
| Ulusoy et al. 2019 [32] | RCT, Parallel | Turkey | 77 | 77 | A. PRP | 18 | Incisor | Secondary to trauma | Until complete healing 10–49 |
| B. PRF | 17 | ||||||||
| C. PP | 17 | ||||||||
| D. BC | 21 | ||||||||
| Rizk et al. 2019 [33] | RCT, Parallel | Egypt | 26 | 26 | A. PRP | 13 | Incisor | Secondary to trauma | 12 |
| B. PRF | 12 | ||||||||
| Shivashankar et al. 2017 [34] | RCT, Parallel | India | 60 | 60 | A. PRF | 20 | Incisor | Secondary to trauma/caries | 12 |
| B. BC | 15 | ||||||||
| C. PRP | 19 | ||||||||
| Alagl et al. 2017 [35] | RCT, Split Mouth | Saudi Arabia | 16 | 32 | A. PRP | 15 | Incisor and premolars | Secondary to trauma/caries | 12 |
| B. BC | 15 | ||||||||
| Bezgin et al. 2015 [36] | RCT, Parallel | Turkey | 20 | 22 | A. PRP | 11 | Incisor and premolars | Secondary to trauma/caries | 18 |
| B. BC | 11 | ||||||||
| Narang et al. 2015 [37] | RCT, Parallel | India | 20 | 20 | A. MTA | 5 | NR | Secondary to trauma/caries | 18 |
| B. BC | 5 | ||||||||
| C. PRF | 5 | ||||||||
| D. PRP | 5 | ||||||||
| Jadhav et al. 2012 [38] | RCT, Parallel | India | 20 | 20 | A. PRP | 10 | Incisor | Secondary to trauma/caries | 12 |
| B. BC | 10 |
| Author | Presence of Periapical Lesion | Instrumentation | Irrigation Methods | Intra-Canal Medication | Recall Time (Weeks) | Preparation Protocol of APC | Access Restoration |
|---|---|---|---|---|---|---|---|
| ElSheshtawy et al. 2020 [29] | Yes | No | 20 mL of 5.25% sodium hypochlorite. At recall, 20 mL of 2.5% sodium hypochlorite, followed by 20 mL sterile saline and 10 mL of 17% EDTA solution. | Triple Antibiotic Paste | NR | PRP was prepared according to Dohan et al. [39], after which concentrated platelet-rich plasma (cPRP) was prepared and introduced inside dry root canals using a sterile 30 G syringe. The canal was then backfilled with cPRP to a level just beneath the CEJ and left to clot for 10 min. | MTA, using a layer of reinforced glass ionomer (Riva self-cure, SDI limited, Bayswater, Victoria, Australia) followed by resin composite (Filtek z250 universal restorative, 3 mol L 1ESPE, St. Paul, MN, USA). |
| Mittal et al. 2019 [30] | Yes | Minimal (#30 K file) | 2.5% sodium hypochlorite (copious irrigation). | Double Antibiotic Paste | 4 weeks | PRF was prepared by drawing 5 mL of venous blood from the patient, collected in a dried glass test tube, and centrifuged at 2700 rpm for 12 min. | Glass ionomer cement followed by composite resin. |
| Ragab et al. 2019 [31] | Yes | No | 20 mL of 5.25% sodium hypochlorite followed by 20 mL sterile saline. | Double Antibiotic Paste | 3 weeks | PRF was prepared by drawing 12 mL sample of whole blood intravenously from the patient’s right antecubital vein and centrifuged under 3000 rpm for 12 min. | MTA plus Light Cure Glass ionomer cement. |
| Ulusoy et al. 2019 [32] | Yes | No | 20 mL 1.25% sodium hypochlorite. At recall, 2% chlorhexidine, saline and 1 mL 17% EDTA. | Triple Antibiotic Paste | 4 weeks | PRP: Citrated blood was centrifuged in a standard laboratory centrifuge PK 130 (ALC International; Cologno Monzese, Italy) for 15 min at 1250 revolutions per minute (rpm) to obtain PRP without erythrocytes and leukocytes. PRF: 10 mL blood was collected in a sterile tube without anticoagulant and centrifuged immediately for 10 min at a speed of 3000 rpm (Andreas Hettich Group, Ltd., Tuttlingen, Germany). | MTA coronal barrier was sealed with a thin glass ionomer base, and final coronal restorations were placed at the same visit using acid etch composite resin. |
| Rizk et al. 2019 [33] | Yes | No | 20 mL 2% sodium hypochlorite for 5 min, followed by 20 mL 17% EDTA. | Triple Antibiotic Paste | 3 weeks | PRP was prepared according to the description by Dohan et al. [39]. PRP was combined with equal volumes of sterile solution containing 10% calcium chloride and sterile bovine thrombin (100 U/mL) to achieve coagulation. PRF: 10 mL blood was collected in a sterile tube without anticoagulant and centrifuged immediately for 10 min at a speed of 3000 rpm. | An MTA orifice plug extending 2–3 mm in the canal was used to seal the canal orifice then glass ionomer (GC America, Alsip, IL) and composite (Z 250, 3 M ESPE) to give an effective and durable seal. |
| Shivashankar et al. 2017 [34] | No | Minimal | 5.25% sodium hypochlorite (copious irrigation). | Triple Antibiotic Paste | 3 weeks | NR | NR |
| Alagl et al. 2017 [35] | Yes | No | 2.5% sodium hypochlorite (20 mL), sterile saline (20 mL), and 0.12% chlorhexidine (10 mL), followed by 17% EDTA after 3 weeks. | Triple Antibiotic Paste | 3 weeks | PRP was prepared according to the description by Dohan et al. [39]. PRP was combined with equal volumes of sterile solution containing 10% calcium chloride and sterile bovine thrombin (100 U/mL) to achieve coagulation. | NR |
| Bezgin et al. 2015 [36] | Yes | No | 2.5% sodium hypochlorite (20 mL), sterile saline (20 mL), and 0.12% chlorhexidine (10 mL), followed by 5% EDTA (20 mL) after 3 weeks. | Triple Antibiotic Paste | 3 weeks | PRP was prepared according to the description by Dohan et al. [39]. PRP was combined with equal volumes of sterile solution containing 10% calcium chloride and sterile bovine thrombin (100 U/mL) to achieve coagulation. | Final restoration was completed with white MTA (Angelus, Londrina, Brazil), reinforced glass ionomer cement (Ketac Molar Easymix; 3M ESPE, Seefeld, Germany), and composite resin (Filtek Supreme XT; 3M ESPE, St Paul, MN, USA). |
| Narang et al. 2015 [37] | Yes | Minimal | 2.5% sodium hypochlorite (copious irrigation) | Triple Antibiotic Paste | 4 weeks | NR | Resin-modified glass ionomer cement was placed extending 3–4 mm in the canal. Access cavity was sealed with composite (Clearfil Majesty, Kuraray Medical Inc., Tokyo, Japan). |
| Jadhav et al. 2012 [38] | No | Minimal (#60 H file) | 2.5% sodium hypochlorite (copious irrigation). | Triple Antibiotic Paste | NR | PRP: 8 mL of blood drawn by venipuncture of the antecubital vein was collected in a 10 mL sterile glass tube coated with an anticoagulant (acid citrate dextrose) and centrifuged at 2400 rpm for 10 min to separate PRP and platelet-poor plasma (PPP) from the red blood cell fraction. The top-most layer (PRP + PPP) was transferred to another tube and again centrifuged at 3600 rpm for 15 min to separate the PRP to precipitate at the bottom of the glass tube. This was mixed with 1 mL 10% calcium chloride to activate the platelets and to neutralize the acidity of acid citrate dextrose. | Resin-modified glass ionomer cement (Photac-Fill; 3M ESPE, St Paul, MN, USA) |
| Author. | Year | Random Sequence Generation (Selection Bias) | Allocation Concealment (Selection Bias) | Blinding of Participants and Personnel (Performance Bias) | Blinding of Outcome Assessment (Detection Bias) | Incomplete Outcome Data (Attrition Bias) | Selective Reporting (Reporting Bias) | Overall Risk |
|---|---|---|---|---|---|---|---|---|
| ElSheshtawy et al. 2020 [29] | 2020 | Low | Low | Low | Low | Low | Low | Low |
| Mittal et al. 2019 [30] | 2019 | Low | Unclear | Low | Low | Low | Low | Moderate |
| Ragab et al. 2019 [31] | 2019 | Low | Unclear | Unclear | Low | Unclear | Low | Moderate |
| Rizk et al. 2019 [33] | 2019 | Low | Low | Unclear | Low | Low | Low | Moderate |
| ] Ulusoy et al. 2019 [32] | 2019 | Low | Unclear | Unclear | Low | Low | Low | Moderate |
| Alagl et al. 2017 [35] | 2017 | Low | Unclear | Unclear | Unclear | Low | Low | Moderate |
| Shivashankar et al. 2017 [34] | 2017 | Low | Low | Low | Low | Low | Low | Low |
| Bezgin et al. 2015 [36] | 2015 | Low | Unclear | Unclear | Unclear | Low | Low | Moderate |
| Narang et al. 2015 [37] | 2015 | Low | Unclear | Unclear | Low | Low | Low | Moderate |
| Jadhav et al. 2012 [38] | 2012 | Low | Unclear | Unclear | Unclear | Low | Low | Moderate |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Panda, S.; Mishra, L.; Arbildo-Vega, H.I.; Lapinska, B.; Lukomska-Szymanska, M.; Khijmatgar, S.; Parolia, A.; Bucchi, C.; Fabbro, M.D. Effectiveness of Autologous Platelet Concentrates in Management of Young Immature Necrotic Permanent Teeth—A Systematic Review and Meta-Analysis. Cells 2020, 9, 2241. https://doi.org/10.3390/cells9102241
Panda S, Mishra L, Arbildo-Vega HI, Lapinska B, Lukomska-Szymanska M, Khijmatgar S, Parolia A, Bucchi C, Fabbro MD. Effectiveness of Autologous Platelet Concentrates in Management of Young Immature Necrotic Permanent Teeth—A Systematic Review and Meta-Analysis. Cells. 2020; 9(10):2241. https://doi.org/10.3390/cells9102241
Chicago/Turabian StylePanda, Saurav, Lora Mishra, Heber Isac Arbildo-Vega, Barbara Lapinska, Monika Lukomska-Szymanska, Shahnawaz Khijmatgar, Abhishek Parolia, Cristina Bucchi, and Massimo Del Fabbro. 2020. "Effectiveness of Autologous Platelet Concentrates in Management of Young Immature Necrotic Permanent Teeth—A Systematic Review and Meta-Analysis" Cells 9, no. 10: 2241. https://doi.org/10.3390/cells9102241
APA StylePanda, S., Mishra, L., Arbildo-Vega, H. I., Lapinska, B., Lukomska-Szymanska, M., Khijmatgar, S., Parolia, A., Bucchi, C., & Fabbro, M. D. (2020). Effectiveness of Autologous Platelet Concentrates in Management of Young Immature Necrotic Permanent Teeth—A Systematic Review and Meta-Analysis. Cells, 9(10), 2241. https://doi.org/10.3390/cells9102241