Vasculogenic Mimicry: A Promising Prognosticator in Head and Neck Squamous Cell Carcinoma and Esophageal Cancer? A Systematic Review and Meta-Analysis



Abstract
:1. Introduction
2. Materials and Methods
2.1. Protocol and Registration
2.2. Eligibility Criteria
2.3. Search Strategy
2.4. Data Extraction and Study Items
2.5. Assessment of Reporting Quality and Risk of Bias
2.6. Data Synthesis and Statistical Analysis
3. Results
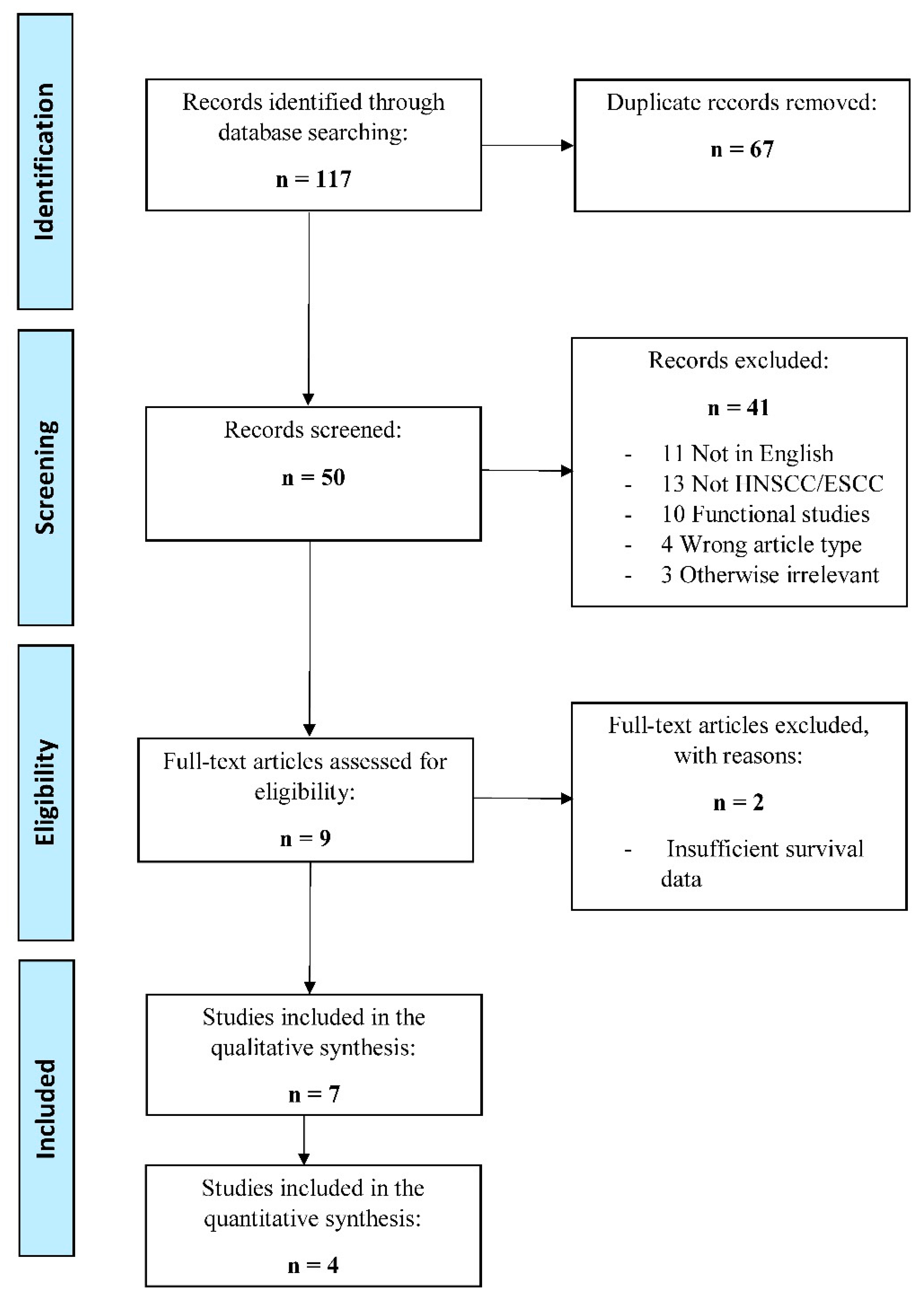
3.1. Study Selection
3.2. Study Characteristics
3.3. Quality and Bias Assessment
3.4. Identification of VM in HNSCC/ESCC Patients
3.5. Association between VM and Clinicopathological Factors
3.6. Survival Endpoints
3.7. Prognostic Value of VM in HNSCC/ESCC Patients
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marur, S.; Forastiere, A.A. Head and Neck Squamous Cell Carcinoma: Update on Epidemiology, Diagnosis, and Treatment. Mayo Clin. Proc. 2016, 91, 386–396. [Google Scholar] [CrossRef] [PubMed]
- Ferlito, A.; Shaha, A.R.; Silver, C.E.; Rinaldo, A.; Mondin, V. Incidence and sites of distant metastases from head and neck cancer. ORL J. Otorhinolaryngol. Relat. Spec. 2001, 63, 202–207. [Google Scholar] [CrossRef] [PubMed]
- Husain, N.; Neyaz, A. Human papillomavirus associated head and neck squamous cell carcinoma: Controversies and new concepts. J. Oral Biol. Craniofac. Res. 2017, 7, 198–205. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Simard, E.P.; Torre, L.A.; Jemal, A. International trends in head and neck cancer incidence rates: Differences by country, sex and anatomic site. Oral Oncol. 2014, 50, 387–403. [Google Scholar] [CrossRef] [PubMed]
- Ricciardiello, F.; Caraglia, M.; Iorio, B.; Abate, T.; Boccellino, M.; Colella, G.; Oliva, F.; Ferrise, P.; Zappavigna, S.; Faenza, M.; et al. Aggressiveness pattern and second primary tumor risk associated with basaloid squamous cell carcinoma of the larynx. Oncotarget 2017, 8, 95791–95798. [Google Scholar] [CrossRef] [Green Version]
- Lim, H.; Do Hoon Kim, H.Y.J.; Gong, E.J.; Na, H.K.; Ahn, J.Y.; Kim, M.Y.; Lee, J.H.; Choi, K.S.; Choi, K.D.; Song, H.J.; et al. Clinical significance of early detection of esophageal cancer in patients with head and neck cancer. Gut Liver 2015, 9, 159–165. [Google Scholar] [CrossRef] [Green Version]
- Napier, K.J.; Scheerer, M.; Misra, S. Esophageal cancer: A Review of epidemiology, pathogenesis, staging workup and treatment modalities. World J. Gastrointest Oncol. 2014, 6, 112–120. [Google Scholar] [CrossRef]
- Seyfried, T.N.; Huysentruyt, L.C. On the origin of cancer metastasis. Crit Rev. Oncog. 2013, 18, 43–73. [Google Scholar] [CrossRef] [Green Version]
- Lo Nigro, C.; Denaro, N.; Merlotti, A.; Merlano, M. Head and neck cancer: Improving outcomes with a multidisciplinary approach. Cancer Manag. Res. 2017, 18, 363–371. [Google Scholar] [CrossRef] [Green Version]
- Maniotis, A.J.; Folberg, R.; Hess, A.; Seftor, E.A.; Gardner, L.M.; Pe’er, J.; Trent, J.M.; Meltzer, P.S.; Hendrix, M.J. Vascular channel formation by human melanoma cells in vivo and in vitro: Vasculogenic mimicry. Am. J. Pathol. 1999, 155, 739–752. [Google Scholar] [CrossRef] [Green Version]
- Valdivia, A.; Mingo, G.; Aldana, V.; Pinto, M.P.; Ramirez, M.; Retamal, C.; Gonzalez, A.; Nualart, F.; Corvalan, A.H.; Owen, G.I. Fact or Fiction, It Is Time for a Verdict on Vasculogenic Mimicry? Front. Oncol. 2019, 9, 680. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Seftor, R.E.; Seftor, E.A.; Koshikawa, N.; Meltzer, P.S.; Gardner, L.M.; Bilban, M.; Stetler-Stevenson, W.G.; Quaranta, V.; Hendrix, M.J. Cooperative interactions of laminin 5 gamma2 chain, matrix metalloproteinase-2, and membrane type-1-matrix/metalloproteinase are required for mimicry of embryonic vasculogenesis by aggressive melanoma. Cancer Res. 2001, 61, 6322–6327. [Google Scholar] [PubMed]
- Hendrix, M.J.; Seftor, E.A.; Seftor, R.E.; Chao, J.T.; Chien, D.S.; Chu, Y.W. Tumor cell vascular mimicry: Novel targeting opportunity in melanoma. Pharmacol. Ther. 2016, 159, 83–92. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wagenblast, E.; Soto, M.; Gutiérrez-Ángel, S.; Hartl, C.A.; Gable, A.L.; Maceli, A.R.; Erard, N.; Williams, A.M.; Kim, S.Y.; Dickopf, S. A model of breast cancer heterogeneity reveals vascular mimicry as a driver of metastasis. Nature 2015, 520, 358–362. [Google Scholar] [CrossRef] [Green Version]
- Cao, Z.; Bao, M.; Miele, L.; Sarkar, F.H.; Wang, Z.; Zhou, Q. Tumour vasculogenic mimicry is associated with poor prognosis of human cancer patients: A systemic review and meta-analysis. Eur. J. Cancer. 2013, 49, 3914–3923. [Google Scholar] [CrossRef]
- Massi, D.; Franchi, A.; Paglierani, M.; Ketabchi, S.; Borgognoni, L.; Reali, U.M.; Santucci, M. Vasculogenic mimicry has no prognostic significance in pT3 and pT4 cutaneous melanoma. Hum. Pathol. 2004, 35, 496–502. [Google Scholar] [CrossRef]
- Booth, A.; Clarke, M.; Dooley, G.; Ghersi, D.; Moher, D.; Petticrew, M.; Stewart, L. The nuts and bolts of PROSPERO: An international prospective register of systematic reviews. Syst. Rev. 2012, 1, 2. [Google Scholar] [CrossRef] [Green Version]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [Green Version]
- McShane, L.M.; Altman, D.G.; Sauerbrei, W.; Taube, S.E.; Gion, M.; Clark, G.M. Statistics Subcommittee of the NCI-EORTC Working Group on Cancer Diagnostics. Reporting recommendations for tumour MARKer prognostic studies (REMARK). Br. J. Cancer 2005, 93, 387–391. [Google Scholar] [CrossRef] [Green Version]
- Munn, Z.; Moola, S.; Lisy, K.; Riitano, D.; Tufanaru, C. Methodological guidance for systematic reviews of observational epidemiological studies reporting prevalence and cumulative incidence data. Int. J. Evid. Based Healthc. 2015, 13, 147–153. [Google Scholar] [CrossRef] [PubMed]
- Wang, W.; Lin, P.; Han, C.; Cai, W.; Zhao, X.; Sun, B. Vasculogenic mimicry contributes to lymph node metastasis of laryngeal squamous cell carcinoma. J. Exp. Clin. Cancer Res. 2010, 29, 60. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chai, D.M.; Bao, Z.Q.; Hu, J.G.; Ma, L.; Feng, Z.Z.; Tao, YS. Vasculogenic mimicry and aberrant expression of HIF-lα/E-cad are associated with worse prognosis of esophageal squamous cell carcinoma. J. Huazhong Univ. Sci. Technol. Med. Sci. 2013, 33, 385–391. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Zhang, G.; Hu, P.; Deng, G.; Liu, Q.; Qiao, L.; Luo, H.; Zhang, J. Vasculogenic mimicry is associated with increased tumor-infiltrating neutrophil and poor outcome in esophageal squamous cell carcinoma. OncoTargets Ther. 2017, 10, 2923–2930. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, Z.; Song, W.; Cheng, Z.; Yang, D.; Yu, L. Expression of LGR5 in oral squamous cell carcinoma and its correlation to vasculogenic mimicry. Int. J. Clin. Exp. Pathol. 2017, 10, 11267–11275. [Google Scholar] [PubMed]
- Liu, S.Y.; Chang, L.C.; Pan, L.F.; Hung, Y.J.; Lee, C.H.; Shieh, Y.S. Clinicopathologic significance of tumor cell-lined vessel and microenvironment in oral squamous cell carcinoma. Oral Oncol. 2008, 44, 277–285. [Google Scholar] [CrossRef]
- Xu, S.; Bai, J.; Zhuan, Z.; Li, B.; Zhang, Z.; Wu, X.; Luo, X.; Yang, L. EBV-LMP1 is involved in vasculogenic mimicry formation via VEGFA/VEGFR1 signaling in nasopharyngeal carcinoma. Oncol. Rep. 2018, 40, 377–384. [Google Scholar] [CrossRef]
- Lin, P.; Wang, W.; Sun, B.C.; Cai, W.J.; Li, L.; Lu, H.H.; Han, C.R.; Zhang, J.M. Vasculogenic mimicry is a key prognostic factor for laryngeal squamous cell carcinoma: A new pattern of blood supply. Chin. Med. J. 2012, 125, 3445–3449. [Google Scholar]
- Paduch, R. The role of lymphangiogenesis and angiogenesis in tumor metastasis. Cell Oncol. 2016, 39, 397–410. [Google Scholar] [CrossRef] [Green Version]
- Qiao, L.; Liang, N.; Zhang, J.; Xie, J.; Liu, F.; Xu, D.; Yu, X.; Tian, Y. Advanced research on vasculogenic mimicry in cancer. J. Cell Mol. Med. 2015, 19, 315–326. [Google Scholar] [CrossRef]
- Montrucchio, G.; Lupia, E.; Battaglia, E.; Del Sorbo, L.; Boccellino, M.; Biancone, L.; Emanuelli, G.; Camussi, G. Platelet-activating factor enhances vascular endothelial growth factor-induced endothelial cell motility and neoangiogenesis in a murine matrigel model. Arterioscler Thromb Vasc. Biol. 2000, 20, 80–88. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, J.P.; Liao, Y.D.; Mai, D.M.; Xie, P.; Qiang, Y.Y.; Zheng, L.S.; Wang, M.Y.; Mei, Y.; Meng, D.F.; Xu, L.; et al. Tumor vasculogenic mimicry predicts poor prognosis in cancer patients: A meta-analysis. Angiogenesis. 2016, 19, 191–200. [Google Scholar] [CrossRef] [PubMed]
- Shen, Y.; Quan, J.; Wang, M.; Li, S.; Yang, J.; Lv, M.; Chen, Z.; Zhang, L.; Zhao, X.; Yang, J. Tumor vasculogenic mimicry formation as an unfavorable prognostic indicator in patients with breast cancer. Oncotarget 2017, 8, 56408–56416. [Google Scholar] [CrossRef] [PubMed]
- Guo, Q.; Yuan, Y.; Jin, Z.; Xu, T.; Gao, Y.; Wei, H.; Li, C.; Hou, W.; Hua, B. Association between Tumor Vasculogenic Mimicry and the Poor Prognosis of Gastric Cancer in China: An Updated Systematic Review and Meta-Analysis. Biomed. Res. Int. 2016, 2016, 2408645. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, Z.; Imani, S.; Shasaltaneh, M.D.; Hosseinifard, H.; Zou, L.; Fan, Y.; Wen, Q. The role of vascular mimicry as a biomarker in malignant melanoma: A systematic review and meta-analysis. BMC Cancer 2019, 19, 1134. [Google Scholar] [CrossRef] [Green Version]
- Ren, H.Y.; Shen, J.X.; Mao, X.M.; Zhang, X.Y.; Zhou, P.; Li, S.Y.; Zheng, Z.W.; Shen, D.Y.; Meng, J.R. Correlation Between Tumor Vasculogenic Mimicry and Poor Prognosis of Human Digestive Cancer Patients: A Systematic Review and Meta-Analysis. Pathol. Oncol. Res. 2019, 25, 849–858. [Google Scholar] [CrossRef]
- Yang, Z.; Sun, B.; Zhao, X.; Shao, B.; An, J.; Gu, Q.; Wang, Y.; Dong, X.; Zhang, Y.; Qiu, Z. Erythropoietin and erythropoietin receptor in hepatocellular carcinoma: Correlation with vasculogenic mimicry and poor prognosis. Int. J. Clin. Exp. Pathol. 2015, 8, 4033–4043. [Google Scholar]
- Ren, K.; Yao, N.; Wang, G.; Tian, L.; Ma, J.; Shi, X.; Zhang, L.; Zhang, J.; Zhou, X.; Zhou, G.; et al. Vasculogenic mimicry: A new prognostic sign of human osteosarcoma. Hum. Pathol. 2014, 45, 2120–2129. [Google Scholar] [CrossRef]
- Wu, S.; Yu, L.; Wang, D.; Zhou, L.; Cheng, Z.; Chai, D.; Ma, L.; Tao, Y. Aberrant expression of CD133 in non-small cell lung cancer and its relationship to vasculogenic mimicry. BMC Cancer 2012, 12, 535. [Google Scholar] [CrossRef] [Green Version]
- Liu, Z.; Sun, B.; Qi, L.; Li, H.; Gao, J.; Leng, X. Zinc finger E-box binding homeobox 1 promotes vasculogenic mimicry in colorectal cancer through induction of epithelial-to-mesenchymal transition. Cancer Sci. 2012, 103, 813–820. [Google Scholar] [CrossRef]
- van Beurden, A.; Schmitz, R.F.; van Dijk, C.M.; Baeten, C.I. Periodic acid Schiff loops and blood lakes associated with metastasis in cutaneous melanoma. Melanoma Res. 2012, 22, 424–429. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.F.; Wang, S.S.; Zheng, M.; Dai, L.L.; Wang, K.; Gao, X.L.; Cao, M.X.; Yu, X.H.; Pang, X.; Zhang, M.; et al. Hypoxia promotes vasculogenic mimicry formation by vascular endothelial growth factor A mediating epithelial-mesenchymal transition in salivary adenoid cystic carcinoma. Cell Prolif. 2019, 52, e12600. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Seftor, R.E.; Hess, A.R.; Seftor, E.A.; Kirschmann, D.A.; Hardy, K.M.; Margaryan, N.V.; Hendrix, M.J. Tumor cell vasculogenic mimicry: From controversy to therapeutic promise. Am. J. Pathol. 2012, 181, 1115–1125. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Misra, R.M.; Bajaj, M.S.; Kale, V.P. Vasculogenic mimicry of HT1080 tumour cells in vivo: Critical role of HIF-1α-neuropilin-1 axis. PLoS ONE 2012, 7, e50153. [Google Scholar] [CrossRef] [PubMed]
- Ricci, S.; Pinto, F.; Auletta, A.; Giordano, A.; Giovane, A.; Settembre, G.; Boccellino, M.; Boffo, S.; Di Carlo, A.; Di Domenico, M. The enigmatic role of matrix metalloproteinases in epithelial-to-mesenchymal transition of oral squamous cell carcinoma: Implications and nutraceutical aspects. J. Cell Biochem. 2019, 3. [Google Scholar] [CrossRef] [PubMed]
- Fernández-Cortés, M.; Delgado-Bellido, D.; Oliver, F.J. Vasculogenic Mimicry: Become an Endothelial Cell “But Not So Much”. Front. Oncol. 2019, 9, 803. [Google Scholar] [CrossRef] [Green Version]
- Tong, M.; Han, B.B.; Holpuch, A.S.; Pei, P.; He, L.; Mallery, S.R. Inherent phenotypic plasticity facilitates progression of head and neck cancer: Endotheliod characteristics enable angiogenesis and invasion. Exp. Cell Res. 2013, 319, 1028–1042. [Google Scholar] [CrossRef] [Green Version]
- Yao, X.H.; Ping, Y.F.; Bian, X.W. Contribution of cancer stem cells to tumor vasculogenic mimicry. Protein Cell. 2011, 2, 266–272. [Google Scholar] [CrossRef] [Green Version]
- Ribatti, D.; Annese, T.; Ruggieri, S.; Tamma, R.; Crivellato, E. Limitations of Anti-Angiogenic Treatment of Tumors. Transl. Oncol. 2019, 12, 981–986. [Google Scholar] [CrossRef]
- Xu, Y.; Li, Q.; Li, X.Y.; Yang, Q.Y.; Xu, W.W.; Liu, G.L. Short-term anti-vascular endothelial growth factor treatment elicits vasculogenic mimicry formation of tumors to accelerate metastasis. J. Exp. Clin. Cancer Res. 2012, 31, 16. [Google Scholar] [CrossRef] [Green Version]
- Chang, Y.S.; di Tomaso, E.; McDonald, D.M.; Jones, R.; Jain, R.K.; Munn, L.L. Mosaic blood vessels in tumors: Frequency of cancer cells in contact with flowing blood. Proc. Natl. Acad. Sci. 2000, 97, 14608–14613. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Folkman, J. Can mosaic tumor vessels facilitate molecular diagnosis of cancer? Proc. Natl. Acad. Sci. 2001, 98, 398–400. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Folberg, R.; Maniotis, A.J. Vasculogenic mimicry. Apmis 2004, 112, 508–525. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Inclusion Criteria | Exclusion Criteria |
|---|---|
|
|
|
|
|
|
|
|
| Study | Country | Tumor Type | Tumor Stage/Size | No. of Cases | No. of VM+ Cases | Compliance to REMARK † |
|---|---|---|---|---|---|---|
| [26] | Taiwan | OSCC | T1–T4 I–IV | 112 | 41 (36.60%) | Lacked items No. 1–3, 5, 6 |
| [22] | China | LSCC | T1–T4 ≤3, >3 cm | 203 | 44 (21.67%) | Lacked item No. 3 |
| [28] | China | LSCC | T1–T4 I–IV | 168 | 37 (22.02%) | Lacked item No. 3 |
| [23] | China | ESCC | I–IV | 160 | 78 (48.75%) | Fulfilled all items |
| [24] | China | ESCC | I–III | 117 | 56 (47.86%) | Fulfilled all items |
| [25] | China | OSCC | I–IV ≤2, ≤4, >4 cm | 190 | 60 (31.57%) | Lacked item No. 3 |
| [27] | China | NPC | I–IV | 40 | 23 (57.50%) | Lacked items No. 3, 5 |
| Study | Method | Tissue | Reagent Information | VM Definition | Additional Criteria |
|---|---|---|---|---|---|
| [26] | IHC, EnVision Doublestain | FFPE | CK: (Mo, MC), Dako CD34: (Mo, MC), Dako | CK+/CD34− lumens | RBCs in lumens |
| [22] | HE, IHC double staining | FFPE | CD31: (Mo), Zhongshan Biotechnology PAS: Department of Pathology, Tianjin Hospital | CD31−/PAS+ loops around cancer cells, with/without RBCs | tumor cell-lined; no hemorrhage, necrosis, perivascular inflammatory cell infiltrate |
| [28] | HE, IHC double staining | FFPE | CD31: (Mo), Zhongshan Biotechnology PAS: Department of Pathology, Tianjin Hospital | CD31−/PAS+ loops around cancer cells, with/without RBCs | HE: no signs of hemorrhage, necrosis, or perivascular cell infiltrate |
| [23] | IHC double staining | FFPE | CD34: (Mo, MC), Abcam PAS: ND | CD34−/PAS+ vessel-like structures surrounded by tumor cells in different forms (straight, curved or branched patterns) | RBCs in channels; few necrotic/inflammatory cells near the channels |
| [24] | HE, IHC double staining | FFPE | CD34: (Rb, MC), Abcam PAS: ND | CD34−/PAS+ lumens composed of tumor cells | - |
| [25] | IHC double staining | FFPE | CD34: (Mo, MC), Abcam PAS: ND | CD34−/PAS+ small vessel-like structures | No necrosis or hemorrhage near VM |
| [27] | IHC double staining | FFPE | CD34: (Rb, MC), Abcam PAS: Sigma-Aldrich | CD34−/PAS+ channels with a lining of tumor cells on the external wall | No ECs on the inner wall |
| Study | End-Point | Adjusted Analysis | Adjusted Factors | Results Interpretation |
|---|---|---|---|---|
| [26] | DFS | - | - | VM correlates significantly with poor survival |
| [22] | OS | HR = 2.117, p = 0.003 | VM, recurrence, TNM stage, radiotherapy | VM is related to pTNM stage, LNM. VM adversely predicted OS and DFS |
| 95% CI = 1.286–3.425 | ||||
| DFS | - | |||
| [28] | DFS | HR = 2.57, p = 0.003 | VM, recurrence, radiation | VM was an adverse prognosticator for DFS and MFS by univariate survival analyses. VM is independent prognostic factor for only DFS |
| 95% CI = 1.388–4.757 | ||||
| MFS | - | |||
| LRFS | - | |||
| [23] | OS | HR = 0.458, p = 0.04 95% CI = 0.217–0.9681 | Gender, age, site, gross morphology, size, DIF, LNM, serosa infiltration, pTNM, VM, HIF-1a, E-cad | VM was significantly correlated with LNM, infiltration, pTNM staging, and 5-year OS of ESCC patients.VM is independent risk factors of patients with ESCC |
| [24] | OS | HR = 0.369, p = 0.001 | pTNM, DIF, TIN expression, VM | VM indicates poor OS and DFS. VM is significant independent prognostic predictors in ESCC |
| 95% CI = 0.207–0.658) | ||||
| DFS | - | |||
| [25] | OS | HR = 1.674, p = 0.010 95% CI = 1.131–2.476 | LGR5, VM, TNM, LNM | VM was positively related to tumor size, grades, LNM, TNM stages, and inversely with patients OS |
| [27] | PFS | - | - | VM formation was associated with a poor prognosis in NPC patients |
| Study | No. of Cases | Age Range (Years) | Age Median (Years) | Hazard Ratio (95% CI) | Relative Weight (%) |
|---|---|---|---|---|---|
| ALL STUDIES | |||||
| [23] | 160 | 32–87 | - | 0.46 (0.22–0.97) | 11.81 |
| [22] | 203 | 32–77 | 66 | 0.47 (0.29–0.77) | 26.55 |
| [25] | 190 | 26–86 | 61 | 0.60 (0.40–0.89 | 41.81 |
| [24] | 117 | 46–80 | 63 | 0.37 (0.21–0.66) | 19.82 |
| Pooled overall estimate | 0.50 (0.38–0.64) | 100 | |||
| Heterogeneity measures | I-squared = 0.0% (p = 0.575); Tau-squared = 0.00 | ||||
| Subgroup Analyses of the Association between VM and OS in HNSCC and ESCC Studies | |||||
| HNSCC STUDIES | |||||
| [22] | 203 | 32–77 | 66 | 0.47 (0.29–0.77) | 38.84 |
| [25] | 190 | 26–86 | 61 | 0.60 (0.40–0.89 | 61.16 |
| Pooled overall estimate | 0.55 (0.40–0.74) | 100 | |||
| Heterogeneity measures | I-squared = 0.0% (p = 0.449); Tau-squared = 0.00 | ||||
| ESCC STUDIES | |||||
| [23] | 160 | 32–87 | - | 0.46 (0.22–0.97) | 37.33 |
| [24] | 117 | 46–80 | 63 | 0.37 (0.21–0.66) | 62.67 |
| Pooled overall estimate | 0.40 (0.26–0.63) | 100 | |||
| Heterogeneity measures | I-squared = 0.0% (p = 0.649); Tau-squared = 0.00 | ||||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hujanen, R.; Almahmoudi, R.; Karinen, S.; Nwaru, B.I.; Salo, T.; Salem, A. Vasculogenic Mimicry: A Promising Prognosticator in Head and Neck Squamous Cell Carcinoma and Esophageal Cancer? A Systematic Review and Meta-Analysis. Cells 2020, 9, 507. https://doi.org/10.3390/cells9020507
Hujanen R, Almahmoudi R, Karinen S, Nwaru BI, Salo T, Salem A. Vasculogenic Mimicry: A Promising Prognosticator in Head and Neck Squamous Cell Carcinoma and Esophageal Cancer? A Systematic Review and Meta-Analysis. Cells. 2020; 9(2):507. https://doi.org/10.3390/cells9020507
Chicago/Turabian StyleHujanen, Roosa, Rabeia Almahmoudi, Sini Karinen, Bright I. Nwaru, Tuula Salo, and Abdelhakim Salem. 2020. "Vasculogenic Mimicry: A Promising Prognosticator in Head and Neck Squamous Cell Carcinoma and Esophageal Cancer? A Systematic Review and Meta-Analysis" Cells 9, no. 2: 507. https://doi.org/10.3390/cells9020507
APA StyleHujanen, R., Almahmoudi, R., Karinen, S., Nwaru, B. I., Salo, T., & Salem, A. (2020). Vasculogenic Mimicry: A Promising Prognosticator in Head and Neck Squamous Cell Carcinoma and Esophageal Cancer? A Systematic Review and Meta-Analysis. Cells, 9(2), 507. https://doi.org/10.3390/cells9020507