Autism in Fragile X Syndrome; A Functional MRI Study of Facial Emotion-Processing


Abstract
:1. Introduction
2. Materials and Methods
2.1. Participant Recuritment
2.2. Imaging Procedure
2.3. Imaging Sequences
2.4. Image Processing and Analysis
2.4.1. Preprocessing of fMRI Data
2.4.2. Statistical Analysis of fMRI Data
2.5. Measure of Cognitive Ability
2.6. Measure of Autistic Traits
3. Results
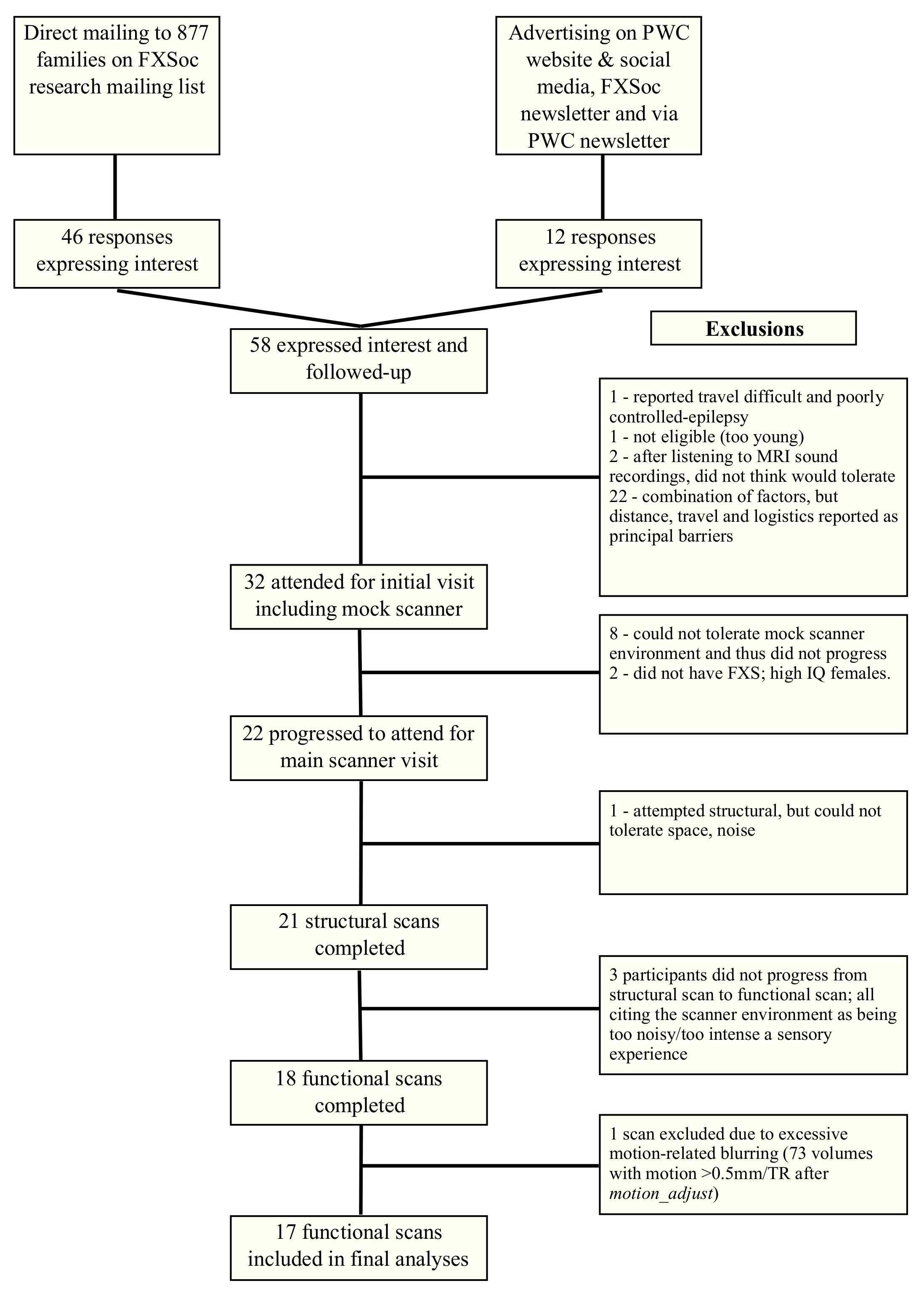
3.1. Feasibility of Functional Imaging in Fragile X Syndrome
3.2. Investigating the Role of Autism in Mediating Facial Emotion Processing
3.2.1. Between-Group Analyses
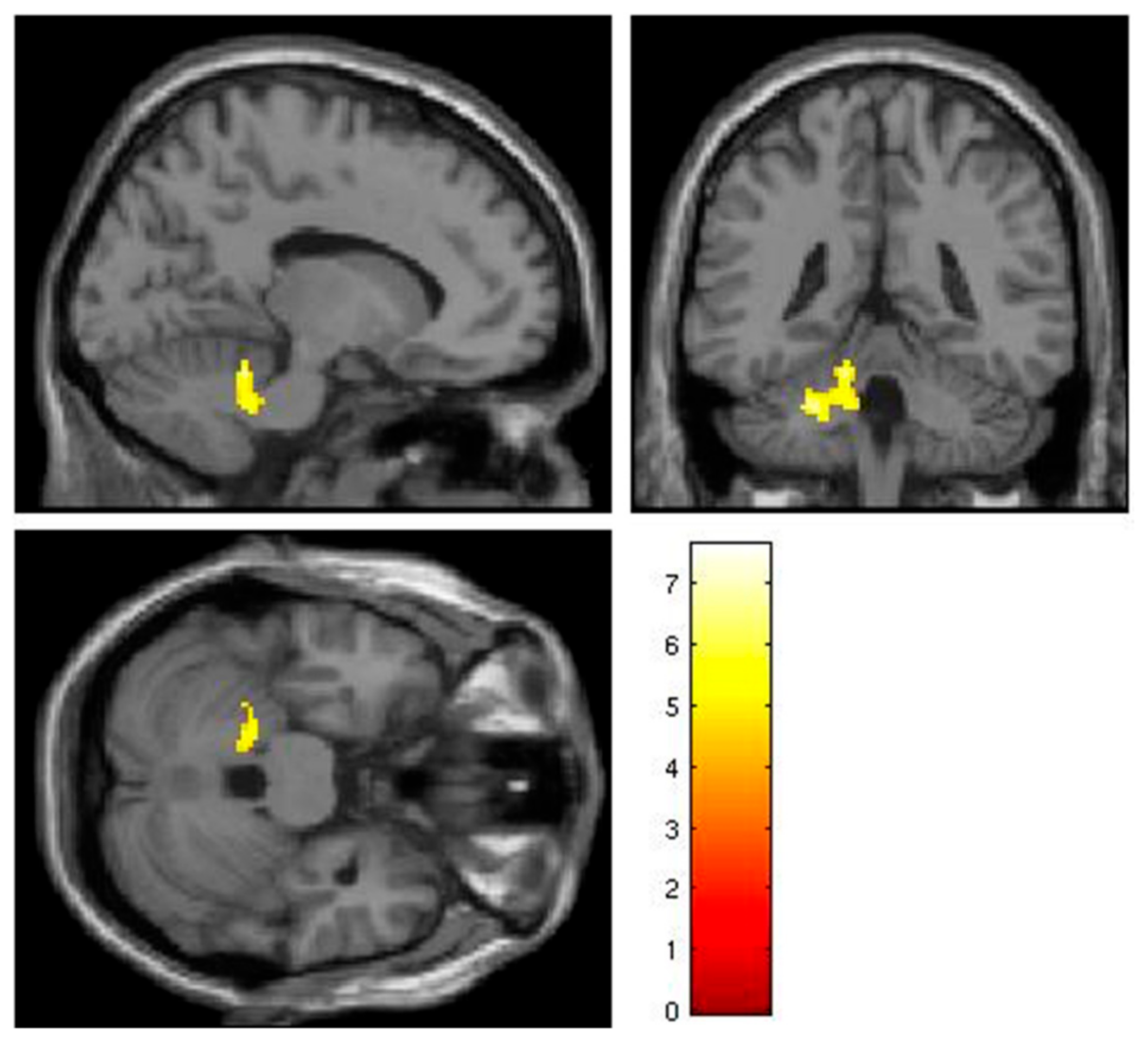
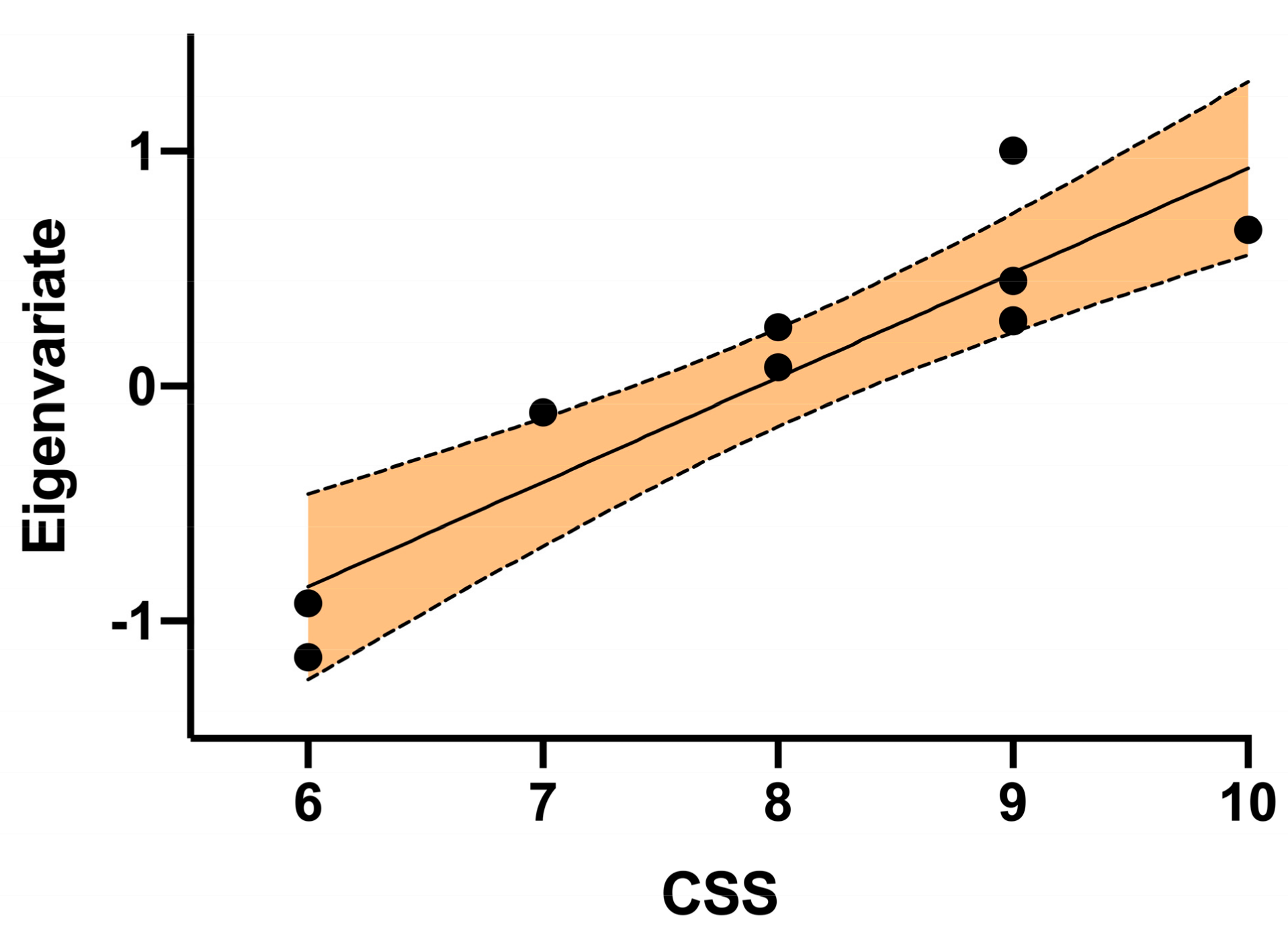
3.2.2. Correlation between ADOS Calibrated Severity Score and Response to Fearful and Neutral Faces
4. Discussion
4.1. Limitations
4.1.1. Participants
4.1.2. Measures
4.1.3. fMRI Paradigm and Acquisition
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A
Appendix B

References
- Crawford, D.C.; Meadows, K.L.; Newman, J.L.; Taft, L.F.; Pettay, D.L.; Gold, L.B.; Hersey, S.J.; Hinkle, E.F.; Stanfield, M.L.; Holmgreen, P.; et al. Prevalence and phenotype consequence of FRAXA and FRAXE alleles in a large, ethnically diverse, special education-needs population. Am. J. Hum. Genet. 1999, 64, 495–507. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brown, W.T.; Friedman, E.; Jenkins, E.C.; Brooks, J.; Wisniewski, K.; Raguthu, S.; French, J.H. Association of fragile X syndrome with autism. Lancet 1982, 1, 100. [Google Scholar] [CrossRef]
- Meryash, D.L.; Szymanski, L.S.; Gerald, P.S. Infantile autism associated with the fragile-X syndrome. J. Autism Dev. Disord. 1982, 12, 295–301. [Google Scholar] [CrossRef] [PubMed]
- Levitas, A.; Hagerman, R.J.; Braden, M.; Rimland, B.; McBogg, P.; Matus, I. Autism and the fragile X syndrome. J. Dev. Behav. Pediatr. 1983, 4, 151–158. [Google Scholar] [CrossRef]
- Fryns, J.P. The fragile X syndrome. A study of 83 families. Clin. Genet. 1984, 26, 497–528. [Google Scholar] [CrossRef] [PubMed]
- Hagerman, R.J.; Jackson, A.W., III; Levitas, A.; Rimland, B.; Braden, M. An analysis of autism in fifty males with the fragile X syndrome. Am. J. Med. Genet. 1986, 23, 359–374. [Google Scholar] [CrossRef]
- Borghgraef, M.; Fryns, J.P.; Dielkens, A.; Pyck, K.; Van den Berghe, H. Fragile (X) syndrome: A study of the psychological profile in 23 prepubertal patients. Clin. Genet. 1987, 32, 179–186. [Google Scholar] [CrossRef] [PubMed]
- Brown, W.T.; Jenkins, E.C.; Cohen, I.L.; Fisch, G.S.; Wolf-Schein, E.G.; Gross, A.; Waterhouse, L.; Fein, D.; Mason-Brothers, A.; Ritvo, E.; et al. Fragile X and autism: A multicenter survey. Am. J. Med. Genet. 1986, 23, 341–352. [Google Scholar] [CrossRef]
- Goldfine, P.E.; McPherson, P.M.; Heath, G.A.; Hardesty, V.A.; Beauregard, L.J.; Gordon, B. Association of fragile X syndrome with autism. Am. J. Psychiatry 1985, 142, 108–110. [Google Scholar] [CrossRef] [PubMed]
- Mcgillivray, B.C.; Herbst, D.S.; Dill, F.J.; Sandercock, H.J.; Tischler, B. Infantile-Autism—An Occasional Manifestation of Fragile-(X) Mental-Retardation. Am. J. Med. Genet. 1986, 23, 353–358. [Google Scholar] [CrossRef]
- Pueschel, S.M.; Herman, R.; Groden, G. Screening-Children with Autism for Fragile-X Syndrome and Phenylketonuria. J. Autism Dev. Disord. 1985, 15, 335–338. [Google Scholar] [CrossRef] [PubMed]
- Wahlstrom, J.; Gillberg, C.; Gustavson, K.H.; Holmgren, G. Infantile autism and the fragile X. A Swedish multicenter study. Am. J. Med. Genet. 1986, 23, 403–408. [Google Scholar] [CrossRef]
- Watson, M.S.; Leckman, J.F.; Annex, B.; Breg, W.R.; Boles, D.; Volkmar, F.R.; Cohen, D.J.; Carter, C. Fragile X in a survey of 75 autistic males. N. Engl. J. Med. 1984, 310, 1462. [Google Scholar] [CrossRef] [PubMed]
- Roesser, J. Diagnostic Yield of Genetic Testing in Children Diagnosed With Autism Spectrum Disorders at a Regional Referral Center. Clin. Pediatr. 2011, 50, 834–843. [Google Scholar] [CrossRef] [PubMed]
- Shen, Y.P.; Dies, K.A.; Holm, I.A.; Bridgemohan, C.; Sobeih, M.M.; Caronna, E.B.; Miller, K.J.; Frazier, J.A.; Silverstein, I.; Picker, J.; et al. Clinical Genetic Testing for Patients With Autism Spectrum Disorders. Pediatrics 2010, 125, E727–E735. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McGrew, S.G.; Peters, B.R.; Crittendon, J.A.; Veenstra-VanderWeele, J. Diagnostic Yield of Chromosomal Microarray Analysis in an Autism Primary Care Practice: Which Guidelines to Implement? J. Autism Dev. Disord. 2012, 42, 1582–1591. [Google Scholar] [CrossRef]
- Cornish, K.; Turk, J.; Levitas, A. Fragile X Syndrome and Autism: Common Developmental Pathways? Curr. Pediatr. Rev. 2007, 3, 61–68. [Google Scholar] [CrossRef] [Green Version]
- Abbeduto, L.; McDuffie, A.; Thurman, A.J. The fragile X syndrome-autism comorbidity: What do we really know? Front. Genet. 2014, 5, 355. [Google Scholar] [CrossRef] [Green Version]
- Hall, S.S.; Lightbody, A.A.; Hirt, M.; Rezvani, A.; Reiss, A.L. Autism in fragile X syndrome: A category mistake? J. Am. Acad. Child Adolesc. Psychiatry 2010, 49, 921–933. [Google Scholar] [CrossRef] [Green Version]
- Kanner, L. Infantile Autism and the Schizophrenias. In Schizophrenia: The First Ten Dean Award Lectures; Dean, S.R., Ed.; MSS Information Corporation: New York, NY, USA, 1973; pp. 95–104. [Google Scholar]
- Harms, M.B.; Martin, A.; Wallace, G.L. Facial emotion recognition in autism spectrum disorders: A review of behavioral and neuroimaging studies. Neuropsychol. Rev. 2010, 20, 290–322. [Google Scholar] [CrossRef]
- Clark, T.F.; Winkielman, P.; McIntosh, D.N. Autism and the extraction of emotion from briefly presented facial expressions: Stumbling at the first step of empathy. Emotion 2008, 8, 803–809. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Teunisse, J.P.; de Gelder, B. Impaired categorical perception of facial expressions in high-functioning adolescents with autism. Child Neuropsychol. 2001, 7, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Leppanen, J.M.; Nelson, C.A. The development and neural bases of facial emotion recognition. Adv. Child Dev. Behav. 2006, 34, 207–246. [Google Scholar] [PubMed]
- Philip, R.C.; Dauvermann, M.R.; Whalley, H.C.; Baynham, K.; Lawrie, S.M.; Stanfield, A.C. A systematic review and meta-analysis of the fMRI investigation of autism spectrum disorders. Neurosci. Biobehav. Rev. 2012, 36, 901–942. [Google Scholar] [CrossRef] [PubMed]
- Di Martino, A.; Ross, K.; Uddin, L.Q.; Sklar, A.B.; Castellanos, F.X.; Milham, M.P. Functional brain correlates of social and nonsocial processes in autism spectrum disorders: An activation likelihood estimation meta-analysis. Biol. Psychiatry 2009, 65, 63–74. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pierce, K.; Muller, R.A.; Ambrose, J.; Allen, G.; Courchesne, E. Face processing occurs outside the fusiform ‘face area’ in autism: Evidence from functional MRI. Brain 2001, 124, 2059–2073. [Google Scholar] [CrossRef]
- Pelphrey, K.A.; Morris, J.P.; McCarthy, G.; Labar, K.S. Perception of dynamic changes in facial affect and identity in autism. Soc. Cogn. Affect. Neurosci. 2007, 2, 140–149. [Google Scholar] [CrossRef]
- Humphreys, K.; Hasson, U.; Avidan, G.; Minshew, N.; Behrmann, M. Cortical patterns of category-selective activation for faces, places and objects in adults with autism. Autism Res. 2008, 1, 52–63. [Google Scholar] [CrossRef] [Green Version]
- Scherf, K.S.; Luna, B.; Minshew, N.; Behrmann, M. Location, Location, Location: Alterations in the Functional Topography of Face-but not Object- or Place-Related Cortex in Adolescents with Autism. Front. Hum. Neurosci. 2010, 4, 26. [Google Scholar] [CrossRef] [Green Version]
- Perlman, S.B.; Hudac, C.M.; Pegors, T.; Minshew, N.J.; Pelphrey, K.A. Experimental manipulation of face-evoked activity in the fusiform gyrus of individuals with autism. Soc. Neurosci. 2011, 6, 22–30. [Google Scholar] [CrossRef]
- Hadjikhani, N.; Joseph, R.M.; Snyder, J.; Tager-Flusberg, H. Abnormal activation of the social brain during face perception in autism. Hum. Brain Mapp. 2007, 28, 441–449. [Google Scholar] [CrossRef] [PubMed]
- Ashwin, C.; Baron-Cohen, S.; Wheelwright, S.; O’Riordan, M.; Bullmore, E.T. Differential activation of the amygdala and the ‘social brain’ during fearful face-processing in Asperger Syndrome. Neuropsychologia 2007, 45, 2–14. [Google Scholar] [CrossRef] [PubMed]
- Bruno, J.L.; Garrett, A.S.; Quintin, E.M.; Mazaika, P.K.; Reiss, A.L. Aberrant Face and Gaze Habituation in Fragile X Syndrome. Am. J. Psychiatry 2014, 171, 1099–1106. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dalton, K.M.; Holsen, L.; Abbeduto, L.; Davidson, R.J. Brain Function and Gaze Fixation During Facial-Emotion Processing in Fragile X and Autism. Autism Res. 2008, 1, 231–239. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Garrett, A.S.; Menon, V.; MacKenzie, K.; Reiss, A.L. Here’s looking at you, kid: Neural systems underlying face and gaze processing in fragile X syndrome. Arch. Gen. Psychiatry 2004, 61, 281–288. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hagan, C.C.; Hoeft, F.; Mackey, A.; Mobbs, D.; Reiss, A.L. Aberrant Neural Function During Emotion Attribution in Female Subjects With Fragile X Syndrome. J. Am. Acad. Child Adolesc. Psychiatry 2008, 47, 1443–1454. [Google Scholar] [CrossRef] [Green Version]
- Holsen, L.M.; Dalton, K.M.; Johnstone, T.; Davidson, R.J. Prefrontal social cognition network dysfunction underlying face encoding and social anxiety in fragile X syndrome. Neuroimage 2008, 43, 592–604. [Google Scholar] [CrossRef] [Green Version]
- Kim, S.Y.; Burris, J.; Bassal, F.; Koldewyn, K.; Chattarji, S.; Tassone, F.; Hessl, D.; Rivera, S.M. Fear-Specific Amygdala Function in Children and Adolescents on the Fragile X Spectrum: A Dosage Response of the FMR1 Gene. Cereb. Cortex 2014, 24, 600–613. [Google Scholar] [CrossRef] [Green Version]
- Watson, C.; Hoeft, F.; Garrett, A.S.; Hall, S.S.; Reiss, A.L. Aberrant Brain Activation During Gaze Processing in Boys With Fragile X Syndrome. Arch. Gen. Psychiatry 2008, 65, 1315–1323. [Google Scholar] [CrossRef] [Green Version]
- Hall, S.S.; Walter, E.; Sherman, E.; Hoeft, F.; Reiss, A.L. The neural basis of auditory temporal discrimination in girls with fragile X syndrome. J. Neurodev. Disord. 2009, 1, 91–99. [Google Scholar] [CrossRef] [Green Version]
- Cornish, K.; Swainson, R.; Cunnington, R.; Wilding, J.; Morris, P.; Jackson, G. Do women with fragile X syndrome have problems in switching attention: Preliminary findings from ERP and fMRI. Brain Cognit. 2004, 54, 235–239. [Google Scholar] [CrossRef] [PubMed]
- Greicius, M.D.; Boyett-Anderson, J.M.; Menon, V.; Reiss, A.L. Reduced basal forebrain and hippocampal activation during memory encoding in girls with fragile X syndrome. Neuroreport 2004, 15, 1579–1583. [Google Scholar] [CrossRef] [PubMed]
- Hoeft, F.; Hernandez, A.; Parthasarathy, S.; Watson, C.L.; Hall, S.S.; Reiss, A.L. Fronto-striatal dysfunction and potential compensatory mechanisms in male adolescents with fragile X syndrome. Hum. Brain Mapp. 2007, 28, 543–554. [Google Scholar] [CrossRef] [PubMed]
- Klabunde, M.; Saggar, M.; Hustyi, K.M.; Kelley, R.G.; Reiss, A.L.; Hall, S.S. Examining the neural correlates of emergent equivalence relations in fragile X syndrome. Psychiatry Res. Neuroimaging 2015, 233, 373–379. [Google Scholar] [CrossRef] [Green Version]
- Kwon, H.; Menon, V.; Eliez, S.; Warsofsky, I.S.; White, C.D.; Dyer-Friedman, J.; Taylor, A.K.; Glover, G.H.; Reiss, A.L. Functional neuroanatomy of visuospatial working memory in fragile X syndrome: Relation to behavioral and molecular measures. Am. J. Psychiatry 2001, 158, 1040–1051. [Google Scholar] [CrossRef]
- Menon, V.; Leroux, J.; White, C.D.; Reiss, A.L. Frontostriatal deficits in fragile X syndrome: Relation to FMR1 gene expression. Proc. Natl. Acad. Sci. USA 2004, 101, 3615–3620. [Google Scholar] [CrossRef] [Green Version]
- Rivera, S.M.; Menon, V.; White, C.D.; Glaser, B.; Reiss, A.L. Functional brain activation during arithmetic processing in females with fragile X Syndrome is related to FMRI protein expression. Hum. Brain Mapp. 2002, 16, 206–218. [Google Scholar] [CrossRef]
- Tamm, L.; Menon, V.; Johnston, C.K.; Hessl, D.R.; Reiss, A.L. fMRI study of cognitive interference processing in females with fragile X syndrome. J. Cogn. Neurosci. 2002, 14, 160–171. [Google Scholar] [CrossRef]
- Hall, S.S.; Jiang, H.; Reiss, A.L.; Greicius, M.D. Identifying large-scale brain networks in fragile X syndrome. JAMA Psychiatry 2013, 70, 1215–1223. [Google Scholar] [CrossRef] [Green Version]
- Isanova, E.; Petrovskiy, E.; Savelov, A.; Yudkin, D.; Tulupov, A. Resting-state fMRI study of patients with fragile X syndrome. J. Phys. Conf. Ser. 2017, 886. [Google Scholar] [CrossRef] [Green Version]
- Hagerman, P.J.; Randol, J.; Kim, K.; Espinal, G.; Hessl, D.; Schneider, A.; Protic, D.; Aydin, Y.; Hagerman, R. Relationship between Fragile X protein (FMRP) and IQ using a quantitative FRET—Based method for determining FMRP levels. In Proceedings of the 19th International Workshop on Fragile X and Other Neurodevelopmental Disorders, Sorrento, Italy, 18–21 September 2019. [Google Scholar]
- Ekman, P.; Friesen, W.V. Pictures of Facial Affect; Consulting Psychologists Press: Palo Alto, CA, USA, 1976. [Google Scholar]
- Mazaika, P. ArtRepair; Version 5b3; Center for Interdisciplinary Brain Science Research; Stanford University: Stanford, CA, USA, 2015. [Google Scholar]
- Mazaika, P.; Hoeft, F.; Glover, G.; Reiss, A. Methods and Software for fMRI Analysis for Clinical Subjects. Neuroimage 2009, 47, S58. [Google Scholar] [CrossRef]
- Kaufman, A.S.; Kaufman, N.L. Kaufman Brief Intelligence Test, 2nd ed.; Pearson Clinical Assessment: San Antonio, TX, USA, 2004. [Google Scholar]
- Lord, C.; Rutter, M.; DiLavore, P.C.; Risi, S.; Gotham, K.; Bishop, S. Autism Diagnostic Observation Schedule, 2nd ed.; Western Psychological Services: Torrance, CA, USA, 2012. [Google Scholar]
- Hus, V.; Lord, C. The autism diagnostic observation schedule, module 4: Revised algorithm and standardized severity scores. J. Autism Dev. Disord. 2014, 44, 1996–2012. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Critchley, H.D.; Daly, E.M.; Bullmore, E.T.; Williams, S.C.; Van Amelsvoort, T.; Robertson, D.M.; Rowe, A.; Phillips, M.; McAlonan, G.; Howlin, P.; et al. The functional neuroanatomy of social behaviour: Changes in cerebral blood flow when people with autistic disorder process facial expressions. Brain 2000, 123, 2203–2212. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Deeley, Q.; Daly, E.M.; Surguladze, S.; Page, L.; Toal, F.; Robertson, D.; Curran, S.; Giampietro, V.; Seal, M.; Brammer, M.J.; et al. An event related functional magnetic resonance imaging study of facial emotion processing in Asperger syndrome. Biol. Psychiatry 2007, 62, 207–217. [Google Scholar] [CrossRef] [PubMed]
- Grezes, J.; Wicker, B.; Berthoz, S.; de Gelder, B. A failure to grasp the affective meaning of actions in autism spectrum disorder subjects. Neuropsychologia 2009, 47, 1816–1825. [Google Scholar] [CrossRef] [PubMed]
- Herrington, J.D.; Baron-Cohen, S.; Wheelwright, S.J.; Singh, K.D.; Bullmore, E.T.; Brammer, M.; Williams, S.C.R. The role of MT+/V5 during biological motion perception in Asperger Syndrome: An fMRI study. Res. Autism Spectr. Disord. 2007, 1, 14–27. [Google Scholar] [CrossRef]
- Van Overwalle, F.; Baetens, K.; Marien, P.; Vandekerckhove, M. Social cognition and the cerebellum: A meta-analysis of over 350 fMRI studies. Neuroimage 2014, 86, 554–572. [Google Scholar] [CrossRef]
- Mazaika, P. Motion Correction and Despike Functions; Stanford University: Stanford, CA, USA, 2009. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Autism Group | Non-Autism Group | |
|---|---|---|
| N | 10 | 7 |
| Male: female | 8:2 | 5:2 |
| Age | 18 (6.2) | 27 (11.7) |
| Full-scale IQ | 59 (8.9) | 63 (14.2) |
| Verbal IQ | 69 (11.9) | 71 (14.2) |
| Performance IQ | 58 (11.1) | 60 (14.4) |
| ADOS Total | 15 (10–20) | 2 (0–5) |
| ADOS CSS | 8 (6–10) | 2 (1–2) |
| Cluster | pFWE-corr | kE | Z≡ | x | y | z |
|---|---|---|---|---|---|---|
| Left superior temporal gyrus | 0.001 | 570 | 4.45 | −64 | −30 | 22 |
| Cluster | pFWE-corr | kE | Z≡ | x | y | z |
|---|---|---|---|---|---|---|
| Left cerebellum, anterior lobe, lobules IV/V | 0.029 | 198 | 4.01 | −24 | −42 | −34 |
| Cluster | pFWE-corr | kE | Z≡ | x | y | z |
|---|---|---|---|---|---|---|
| Left cerebellum, anterior lobe, lobules IV/V | 0.006 | 27 | 3.70 | −20 | −38 | −30 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
McKechanie, A.G.; Campbell, S.; Eley, S.E.A.; Stanfield, A.C. Autism in Fragile X Syndrome; A Functional MRI Study of Facial Emotion-Processing. Genes 2019, 10, 1052. https://doi.org/10.3390/genes10121052
McKechanie AG, Campbell S, Eley SEA, Stanfield AC. Autism in Fragile X Syndrome; A Functional MRI Study of Facial Emotion-Processing. Genes. 2019; 10(12):1052. https://doi.org/10.3390/genes10121052
Chicago/Turabian StyleMcKechanie, Andrew G., Sonya Campbell, Sarah E. A. Eley, and Andrew C. Stanfield. 2019. "Autism in Fragile X Syndrome; A Functional MRI Study of Facial Emotion-Processing" Genes 10, no. 12: 1052. https://doi.org/10.3390/genes10121052
APA StyleMcKechanie, A. G., Campbell, S., Eley, S. E. A., & Stanfield, A. C. (2019). Autism in Fragile X Syndrome; A Functional MRI Study of Facial Emotion-Processing. Genes, 10(12), 1052. https://doi.org/10.3390/genes10121052