Fourier-Transform Infrared Spectroscopy of Skeletal Muscle Tissue: Expanding Biomarkers in Primary Mitochondrial Myopathies


 ,
,  ,
,  ,
,  , ,
, ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Participants
2.2. Muscle Biopsy Collection and Fourier-Transform Infrared Measurements
2.3. Statistical Analyses
3. Results
4. Discussion
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Gorman, G.S.; Schaefer, A.M.; Ng, Y.; Gomez, N.; Blakely, E.L.; Alston, C.L.; Feeney, C.; Horvath, R.; Yu-Wai-Man, P.; Chinnery, P.F.; et al. Prevalence of nuclear and mitochondrial DNA mutations related to adult mitochondrial disease. Ann. Neurol. 2015, 77, 753–759. [Google Scholar] [CrossRef] [Green Version]
- Lightowlers, R.N.; Taylor, R.W.; Turnbull, D.M. Mutations causing mitochondrial disease: What is new and what challenges remain? Science 2015, 349, 1494–1499. [Google Scholar] [CrossRef]
- Schon, K.R.; Ratnaike, T.; van den Ameele, J.; Horvath, R.; Chinnery, P.F. Mitochondrial Diseases: A Diagnostic Revolution. Trends Genet. 2020, 36, 702–717. [Google Scholar] [CrossRef] [PubMed]
- Gorman, G.S.; Chinnery, P.F.; Di Mauro, S.; Hirano, M.; Koga, Y.; McFarland, R.; Suomalainen, A.; Thorburn, D.R.; Zeviani, M.; Turnbull, D.M. Mitochondrial diseases. Nat. Rev. Dis. Primers 2016, 2, 16080. [Google Scholar] [CrossRef] [PubMed]
- Mancuso, M.; McFarland, R.; Klopstock, T.; Hirano, M. Consortium on Trial Readiness in Mitochondrial Myopathies. International Workshop: Outcome measures and clinical trial readiness in primary mitochondrial myopathies in children and adults. Consensus recommendations. 16-18 November 2016, Rome, Italy. Neuromuscul. Disord. 2017, 27, 1126–1137. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Primiano, A.; Persichilli, S.; Gambaro, G.; Ferraro, P.M.; D’Addessi, A.; Cocci, A.; Schiattarella, A.; Zuppi, C.; Gervasoni, J. FTIR analysis of urinary stones: A helpful tool for clinician comparison with the chemical spot test. Dis. Markers 2014, 2014, 176165. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Romanò, S.; Di Giacinto, F.; Primiano, A.; Mazzini, A.; Panzetta, C.; Papi, M.; Di Gaspare, A.; Ortolani, M.; Gervasoni, J.; De Spirito, M.; et al. Fourier Transform Infrared Spectroscopy as a useful tool for the automated classification of cancer cell-derived exosomes obtained under different culture conditions. Anal. Chim. Acta 2020, 1140, 219–227. [Google Scholar] [CrossRef] [PubMed]
- Sjoström, M.; Wold, S.; Söderström, S. PLS discriminant plots. In Pattern Recognition in Practice II; Gelsema, E.S., Kanal, L.N., Eds.; Elsevier: Amsterdam, The Netherlands, 1986; pp. 461–470. [Google Scholar]
- Cocchi, M.; Biancolillo, A.; Marini, F. Chapter Ten—Chemometric Methods for Classification and Feature Selection. In Comprehensive Analytical Chemistry; Jaumot, J., Bedia, C., Tauler, R., Eds.; Elsevier: Oxford, UK, 2018; pp. 265–299. [Google Scholar]
- Fisher, R.A. The use of multiple measurements in taxonomic problems. Ann. Eugen. 1936, 7, 179–188. [Google Scholar] [CrossRef]
- Wold, S.; Sjöström, M.; Eriksson, L. PLS-regression: A basic tool of chemometrics. Chemom. Intell. Lab. Syst. 2001, 58, 109–130. [Google Scholar] [CrossRef]
- Roger, J.M.; Palagos, B.; Bertrand, D.; Fernandez-Ahumada, E. CovSel: Variable selection for highly multivariate and multi-response calibration: Application to IR spectroscopy. Chemom. Intell. Lab. Syst. 2011, 106, 216–223. [Google Scholar] [CrossRef] [Green Version]
- Smit, S.; van Breemen, M.J.; Hoefsloot, H.C.J.; Smilde, A.K.; Aerts, J.M.F.G.; de Koster, C.G. Assessing the statistical validity of proteomics based biomarkers. Anal. Chim. Acta 2007, 592, 210–217. [Google Scholar] [CrossRef] [PubMed]
- Szymańska, E.; Saccenti, E.; Smilde, A.K.; Westerhuis, J.A. Double-check: Validation of diagnostic statistics for PLS-DA models in metabolomics studies. Metabolomics 2012, 8 (Suppl. 1), 3–16. [Google Scholar]
- Holt, I.J.; Harding, A.E.; Morgan-Hughes, J.A. Deletions of muscle mitochondrial DNA in patients with mitochondrial myopathies. Nature 1988, 331, 717–719. [Google Scholar] [CrossRef] [PubMed]
- Zeviani, M.; Moraes, C.T.; DiMauro, S.; Nakase, H.; Bonilla, E.; Schon, E.A.; Rowland, L.P. Deletions of mitochondrial DNA in Kearns-Sayre syndrome. Neurology 1988, 38, 1339–1346. [Google Scholar] [CrossRef] [PubMed]
- Moraes, C.T.; DiMauro, S.; Zeviani, M.; Lombes, A.; Shanske, S.; Miranda, A.F.; Nakase, H.; Bonilla, E.; Werneck, L.C.; Servidei, S.; et al. Mitochondrial DNA deletions in progressive external ophthalmoplegia and Kearns-Sayre syndrome. N. Engl. J. Med. 1989, 320, 1293–1299. [Google Scholar] [CrossRef] [PubMed]
- Zeviani, M.; Servidei, S.; Gellera, C.; Bertini, E.; DiMauro, S.; DiDonato, S. An autosomal dominant disorder with multiple deletions of mitochondrial DNA starting at the D-loop region. Nature 1989, 339, 309–311. [Google Scholar] [CrossRef] [PubMed]
- Parikh, S.; Goldstein, A.; Karaa, A.; Koenig, M.K.; Anselm, I.; Brunel-Guitton, C.; Christodoulou, J.; Cohen, B.H.; Dimmock, D.; Enns, G.M.; et al. Patient care standards for primary mitochondrial disease: A consensus statement from the Mitochondrial Medicine Society. Genet. Med. 2017, 19, 1380. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Vries, M.C.; Brown, D.A.; Allen, M.E.; Bindoff, L.; Gorman, G.S.; Karaa, A.; Keshavan, N.; Lamperti, C.; McFarland, R.; Ng, Y.S.; et al. Safety of drug use in patients with a primary mitochondrial disease: An international Delphi-based consensus. J. Inherit. Metab. Dis. 2020, 43, 800–818. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Primiano, G.; Servidei, S. A severe linezolid-induced rhabdomyolysis and lactic acidosis in Leigh syndrome. J. Inherit. Metab. Dis. 2020. [Google Scholar] [CrossRef] [PubMed]
- Orsucci, D.; Angelini, C.; Bertini, E.; Carelli, V.; Comi, G.P.; Federico, A.; Minetti, C.; Moggio, M.; Mongini, T.; Santorelli, F.M.; et al. Revisiting mitochondrial ocular myopathies: A study from the Italian Network. J. Neurol. 2017, 264, 1777–1784. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
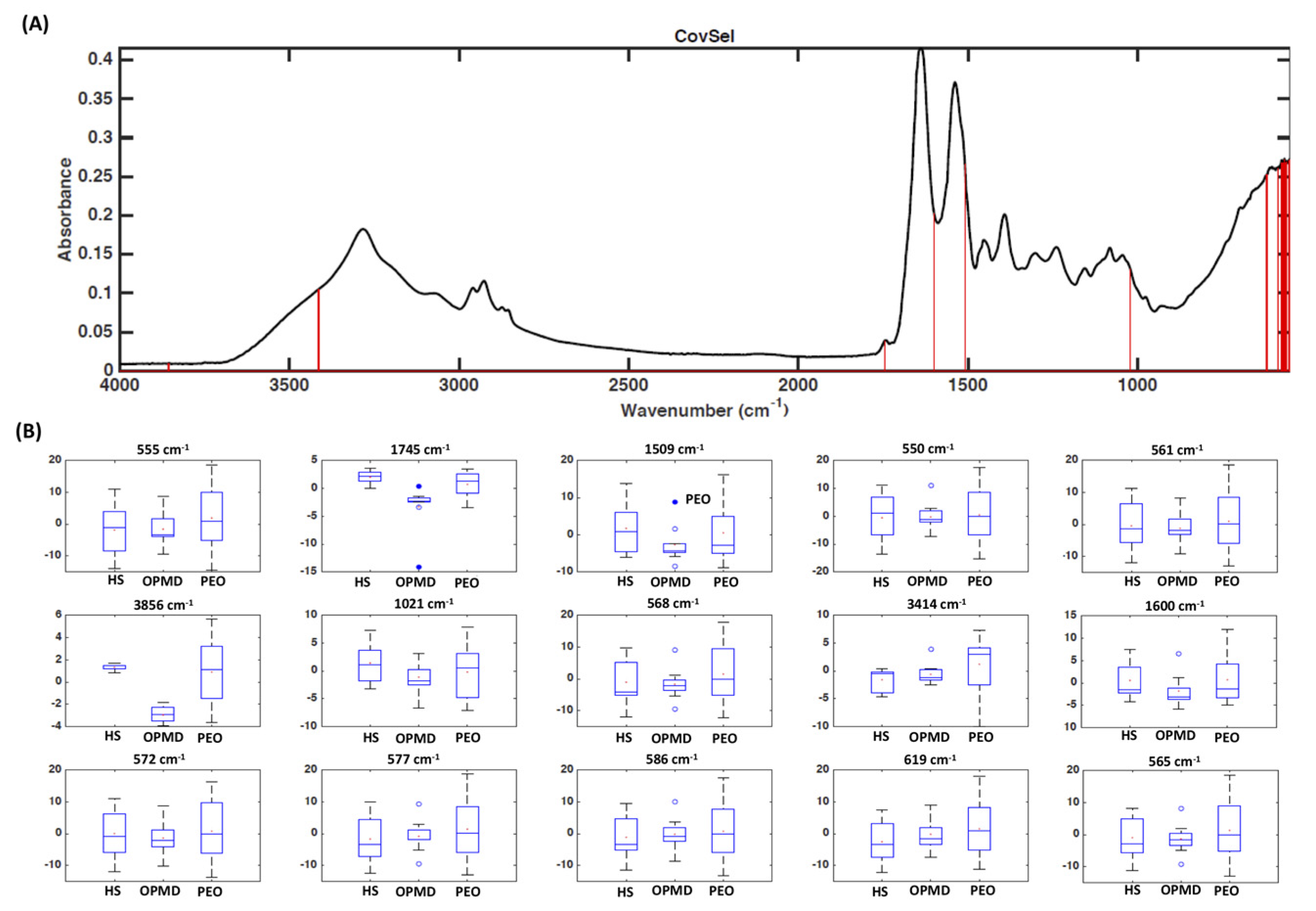
| Spectral Region (cm−1) | Biomolecular Peak Assignments |
|---|---|
| 3000–2800 | Symmetric and asymmetric C-H stretching vibrations of lipids |
| 1745–1725 | Symmetric C=O stretching vibration of lipids |
| 1700–1600 | Amide I region of proteins carrying information on secondary structure |
| 1600–1500 | Amide II region of proteins |
| 1200–900 | Symmetric and asymmetric PO3− stretching vibration and symmetric CO-O-C stretching vibration of nucleic acids and carbohydrates |
| Participants | Sex | Age at Biopsy (Years) | Phenotype | Genotype |
|---|---|---|---|---|
| 1 | M | 27 | PEO | c.2864A>G [p.Y955C] POLG |
| 2 | F | 64 | PEO | c.2864A>G [p.Y955C] POLG |
| 3 | F | 47 | PEO | c.1943C>G [P648R]/c.2243G>C [p.W748S] POLG |
| 4 | F | 52 | PEO | c.926G>A [p.R309H]/c.1760C>T [p.P587L] POLG |
| 5 | F | 61 | PEO | c.3293A>G [p.1098N>S] POLG |
| 6 | M | 44 | PEO | c.2864A>G [p.Y955C] POLG |
| 7 | F | 39 | PEO | c.2864A>G [p.Y955C] POLG |
| 8 | F | 35 | PEO | c.2864A>G [p.Y955C] POLG |
| 9 | M | 14 | PEO | single mtDNA deletion |
| 10 | F | 31 | PEO | single mtDNA deletion |
| 11 | F | 31 | PEO | single mtDNA deletion |
| 12 | F | 62 | PEO | single mtDNA deletion |
| 13 | M | 54 | PEO | single mtDNA deletion |
| 14 | M | 13 | PEO | single mtDNA deletion |
| 15 | M | 11 | PEO | single mtDNA deletion |
| 16 | F | 23 | PEO | single mtDNA deletion |
| 17 | M | 62 | OPMD | PABPN1 (GCN)13/Ala13 |
| 18 | F | 55 | OPMD | PABPN1 (GCN)13/Ala13 |
| 19 | M | 56 | OPMD | PABPN1 (GCN)15/Ala15 |
| 20 | M | 54 | OPMD | PABPN1 (GCN)15/Ala15 |
| 21 | M | 62 | OPMD | PABPN1 (GCN)15/Ala15 |
| 22 | F | 61 | OPMD | PABPN1 (GCN)13/Ala13 |
| 23 | F | 71 | OPMD | PABPN1 (GCN)12/Ala12 |
| 24 | F | 80 | OPMD | PABPN1 (GCN)11/Ala11 |
| 25 | M | 59 | OPMD | PABPN1 (GCN)13/Ala13 |
| Class | Sensitivity | Specificity | Accuracy | Average Classification Error |
|---|---|---|---|---|
| PEO | 85.7 ± 7.2% | 94.7 ± 3.7% | 90.1 ± 4.2% | 8.7 ± 3.8% |
| OPMD | 96.4 ± 5.2% | 95.7 ± 4.0% | ||
| Controls | 91.7 ± 6.9% | 94.7 ± 2.6% |
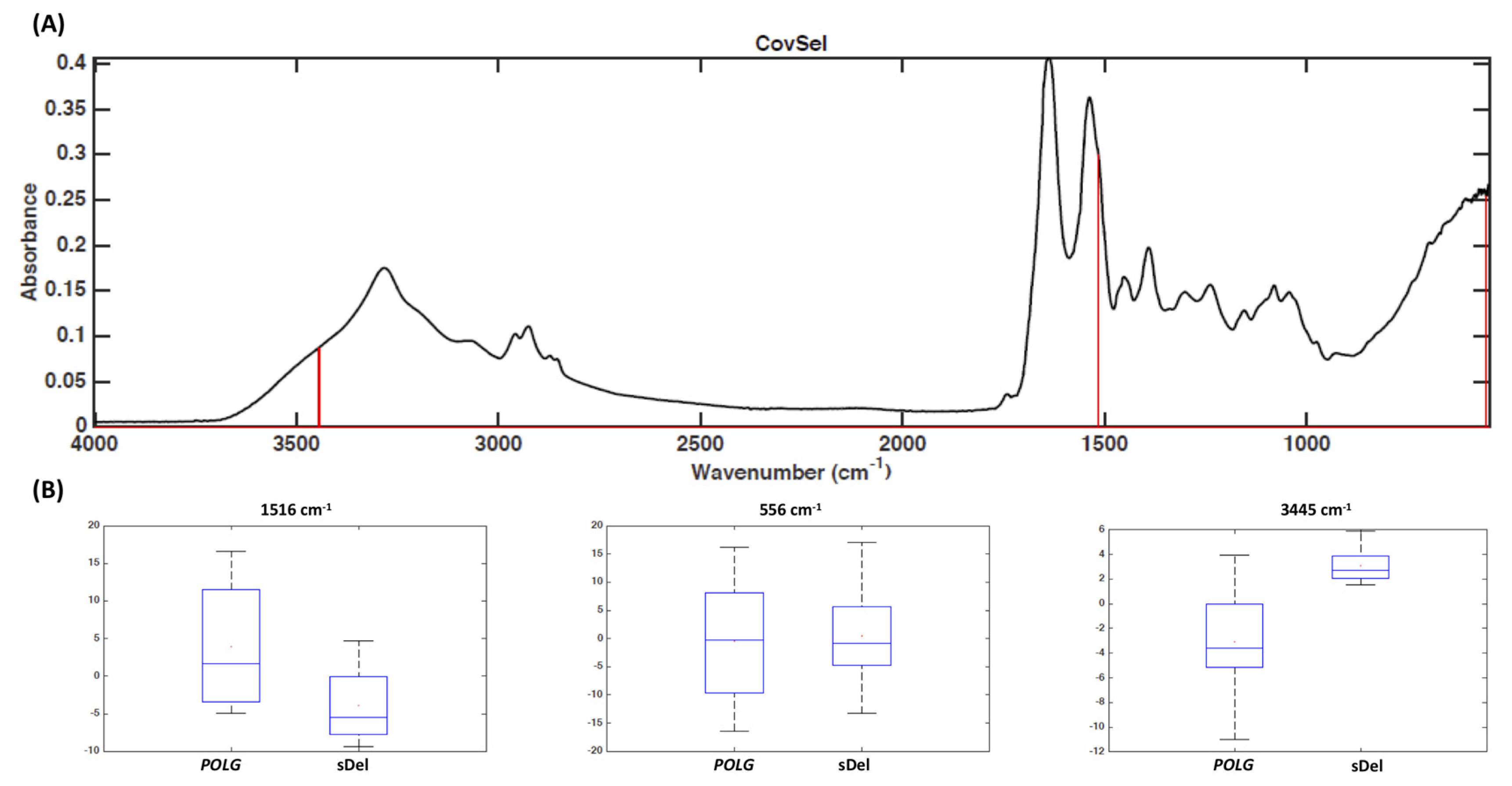
| Class | Sensitivity | Specificity | Accuracy | Average Classification Error |
|---|---|---|---|---|
| Single mtDNA deletion | 100.0 ± 0.0% | 99.0 ± 3.4% | 99.5 ± 1.7% | 0.5 ± 1.7% |
| POLG mutations | 99.0 ± 3.4% | 100.0 ± 0.0% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gervasoni, J.; Primiano, A.; Marini, F.; Sabino, A.; Biancolillo, A.; Calvani, R.; Picca, A.; Marzetti, E.; Persichilli, S.; Urbani, A.; et al. Fourier-Transform Infrared Spectroscopy of Skeletal Muscle Tissue: Expanding Biomarkers in Primary Mitochondrial Myopathies. Genes 2020, 11, 1522. https://doi.org/10.3390/genes11121522
Gervasoni J, Primiano A, Marini F, Sabino A, Biancolillo A, Calvani R, Picca A, Marzetti E, Persichilli S, Urbani A, et al. Fourier-Transform Infrared Spectroscopy of Skeletal Muscle Tissue: Expanding Biomarkers in Primary Mitochondrial Myopathies. Genes. 2020; 11(12):1522. https://doi.org/10.3390/genes11121522
Chicago/Turabian StyleGervasoni, Jacopo, Aniello Primiano, Federico Marini, Andrea Sabino, Alessandra Biancolillo, Riccardo Calvani, Anna Picca, Emanuele Marzetti, Silvia Persichilli, Andrea Urbani, and et al. 2020. "Fourier-Transform Infrared Spectroscopy of Skeletal Muscle Tissue: Expanding Biomarkers in Primary Mitochondrial Myopathies" Genes 11, no. 12: 1522. https://doi.org/10.3390/genes11121522
APA StyleGervasoni, J., Primiano, A., Marini, F., Sabino, A., Biancolillo, A., Calvani, R., Picca, A., Marzetti, E., Persichilli, S., Urbani, A., Servidei, S., & Primiano, G. (2020). Fourier-Transform Infrared Spectroscopy of Skeletal Muscle Tissue: Expanding Biomarkers in Primary Mitochondrial Myopathies. Genes, 11(12), 1522. https://doi.org/10.3390/genes11121522