
Pharmacogenomics: A Step forward Precision Medicine in Childhood Asthma

 , , ,
, , , 
Abstract
:1. Introduction
2. Assessing Response to Treatment in Childhood Asthma: The Contribution of Pharmacogenomics
2.1. Short-Acting β Agonists
2.2. Long-Acting β Agonists
2.3. Inhaled Corticosteroids
2.4. Inhaled Corticosteroids + Long-Acting β Agonists
2.5. Leukotriene Modifiers
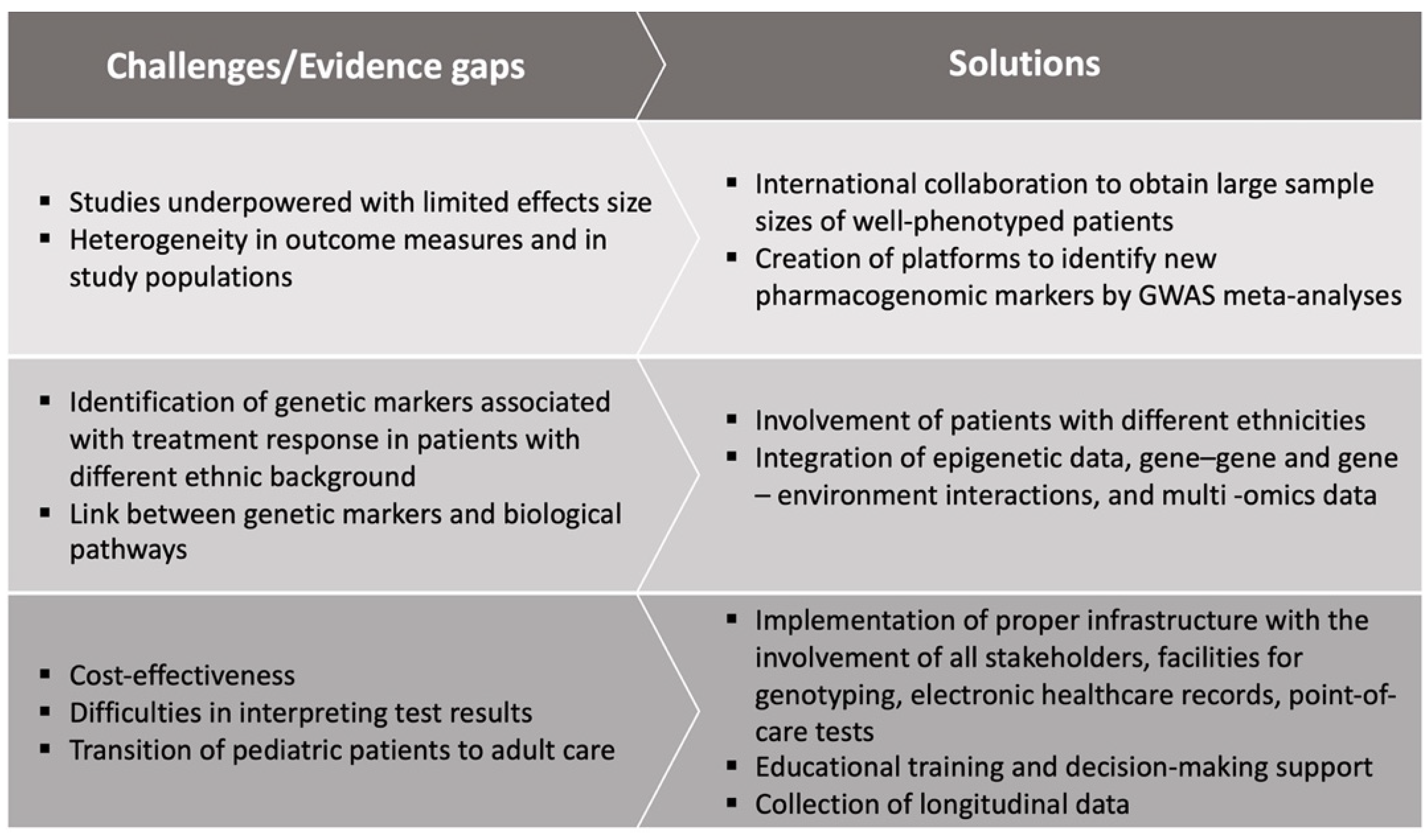
3. Application of Pharmacogenomics in Childhood Asthma Practice: Challenges and Evidence Gaps
4. Future Research Perspectives
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Ferrante, G.; La Grutta, S. The Burden of Pediatric Asthma. Front. Pediatr. 2018, 6, 186. [Google Scholar] [CrossRef] [Green Version]
- Chung, K.F. Asthma phenotyping: A necessity for improved therapeutic precision and new targeted therapies. J. Intern. Med. 2015, 279, 192–204. [Google Scholar] [CrossRef] [PubMed]
- Sottile, G.; Ferrante, G.; Torregrossa, M.; Cibella, F.; Cilluffo, G.; Fasola, S.; Alessandro, R.; Seidita, G.; Viegi, G.; La Grutta, S. An association analysis to identify genetic variants linked to asthma and rhino-conjunctivitis in a cohort of Sicilian children. Ital. J. Pediatr. 2019, 45, 16. [Google Scholar] [CrossRef] [PubMed]
- Global Initiative for Asthma (GINA). Global Strategy for Asthma Management and Prevention. 2018. Available online: https://ginasthma.org/ (accessed on 23 January 2022).
- Licari, A.; Brambilla, I.; Marseglia, A.; De Filippo, M.; Paganelli, V.; Marseglia, G.L. Difficult vs. Severe Asthma: Definition and Limits of Asthma Control in the Pediatric Population. Front. Pediatr. 2018, 6, 170. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kersten, E.T.; Koppelman, G.H. Pharmacogenetics of asthma: Toward precision medicine. Curr. Opin. Pulm. Med. 2017, 23, 12–20. [Google Scholar] [CrossRef] [Green Version]
- Ortega, V.E.; Meyers, D.A. Pharmacogenetics: Implications of race and ethnicity on defining genetic profiles for personalized medicine. J. Allergy Clin. Immunol. 2014, 133, 16–26. [Google Scholar] [CrossRef] [Green Version]
- Solazzo, G.; Ferrante, G.; La Grutta, S. DNA Methylation in Nasal Epithelium: Strengths and Limitations of an Emergent Biomarker for Childhood Asthma. Front. Pediatr. 2020, 8, 256. [Google Scholar] [CrossRef] [PubMed]
- Seyhan, A.A.; Carini, C. Are innovation and new technologies in precision medicine paving a new era in patients centric care? J. Transl. Med. 2019, 17, 114. [Google Scholar] [CrossRef] [Green Version]
- Collins, F.S.; Varmus, H. A New Initiative on Precision Medicine. N. Engl. J. Med. 2015, 372, 793–795. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ferrante, G.; Rossi, R.; Cilluffo, G.; Di Silvestre, D.; Brambilla, A.; De Palma, A.; Villa, C.; Malizia, V.; Gagliardo, R.; Torrente, Y.; et al. Shotgun Proteomics of Isolated Urinary Extracellular Vesicles for Investigating Respiratory Impedance in Healthy Preschoolers. Molecules 2021, 26, 1258. [Google Scholar] [CrossRef]
- What Is Pharmacogenomics? Available online: https://ghr.nlm.nih.gov/primer/genomicresearch/pharmacogenomics (accessed on 23 January 2022).
- McLeod, H.L.; E Evans, W. Pharmacogenomics: Unlocking the Human Genome for Better Drug Therapy. Annu. Rev. Pharmacol. Toxicol. 2001, 41, 101–121. [Google Scholar] [CrossRef] [PubMed]
- Mooney, S.D. Progress towards the integration of pharmacogenomics in practice. Hum. Genet. 2015, 134, 459–465. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cilluffo, G.; Fasola, S.; Ferrante, G.; Malizia, V.; Montalbano, L.; La Grutta, S. Machine Learning: An Overview and Applications in Pharmacogenetics. Genes 2021, 12, 1511. [Google Scholar] [CrossRef]
- Fasola, S.; Montalbano, L.; Cilluffo, G.; Cuer, B.; Malizia, V.; Ferrante, G.; Annesi-Maesano, I.; La Grutta, S. A Critical Review of Statistical Methods for Twin Studies Relating Exposure to Early Life Health Conditions. Int. J. Environ. Res. Public Health 2021, 18, 12696. [Google Scholar] [CrossRef] [PubMed]
- Maagdenberg, H.; Vijverberg, S.; Bierings, M.B.; Carleton, B.; Arets, H.G.M.; De Boer, A.; Der Zee, A.H.M.-V. Pharmacogenomics in Pediatric Patients: Towards Personalized Medicine. Pediatr. Drugs 2016, 18, 251–260. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mak, A.C.Y.; White, M.J.; Eckalbar, W.L.; Szpiech, Z.A.; Oh, S.S.; Pino-Yanes, M.; Hu, D.; Goddard, P.; Huntsman, S.; Galanter, J.; et al. Whole-Genome Sequencing of Pharmacogenetic Drug Response in Racially Diverse Children with Asthma. Am. J. Respir. Crit. Care Med. 2018, 197, 1552–1564. [Google Scholar] [CrossRef] [PubMed]
- Spear, M.L.; Hu, D.; Pino-Yanes, M.; Huntsman, S.; Eng, C.; Levin, A.M.; Ortega, V.E.; White, M.J.; McGarry, M.E.; Thakur, N.; et al. A Genome-Wide Association and Admixture Mapping Study of Bronchodilator Drug Response in African Ameri-cans with Asthma. Pharm. J. 2019, 19, 249–259. [Google Scholar]
- Fishe, J.N.; Labilloy, G.; Higley, R.; Casey, D.; Ginn, A.; Baskovich, B.; Blake, K.V. Single Nucleotide Polymorphisms (SNPs) in PRKG1 & SPATA13-AS1 are associated with bronchodilator response: A pilot study during acute asthma exacerbations in African American children. Pharmacogenetics Genom. 2021, 31, 146–154. [Google Scholar] [CrossRef]
- Scaparrotta, A.; Franzago, M.; Marcovecchio, M.L.; Di Pillo, S.; Chiarelli, F.; Mohn, A.; Stuppia, L. Role of THRB, ARG1, and ADRB2 Genetic Variants on Bronchodilators Response in Asthmatic Children. J. Aerosol Med. Pulm. Drug Deliv. 2019, 32, 164–173. [Google Scholar] [CrossRef]
- Slob, E.M.A.; Richards, L.B.; Vijverberg, S.J.H.; Longo, C.; Koppelman, G.H.; Pijnenburg, M.W.H.; Bel, E.H.D.; Neerincx, A.H.; Herrera Luis, E.; Perez-Garcia, J.; et al. Genome-wide association studies of exacerbations in children using long-acting beta2-agonists. Pediatr. Allergy Immunol. 2021, 32, 1197–1207. [Google Scholar]
- Slob, E.M.A.; Vijverberg, S.J.H.; Palmer, C.; Zazuli, Z.; Farzan, N.; Oliveri, N.M.B.; Pijnenburg, M.W.; Koppelman, G.H.; Der Zee, A.H.M.-V. Pharmacogenetics of inhaled long-acting beta2-agonists in asthma: A systematic review. Pediatr. Allergy Immunol. 2018, 29, 705–714. [Google Scholar] [CrossRef] [PubMed]
- Farzan, N.; Vijverberg, S.; Arets, H.G.; Raaijmakers, J.A.M.; Der Zee, A.H.M.-V. Pharmacogenomics of inhaled corticosteroids and leukotriene modifiers: A systematic review. Clin. Exp. Allergy 2016, 47, 271–293. [Google Scholar] [CrossRef]
- Huang, J.; Hu, X.; Zheng, X.; Kuang, J.; Liu, C.; Wang, X.; Tang, Y. Effects of STIP1 and GLCCI1 polymorphisms on the risk of childhood asthma and inhaled corticosteroid response in Chinese asthmatic children. BMC Pulm. Med. 2020, 20, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Farzan, N.; Vijverberg, S.J.; Hernandez-Pacheco, N.; Bel, E.H.D.; Berce, V.; Bønnelykke, K.; Bisgaard, H.; Burchard, E.G.; Canino, G.; Celedón, J.C.; et al. 17q21 variant increases the risk of exacerbations in asthmatic children despite inhaled corticosteroids use. Allergy 2018, 73, 2083–2088. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wan, Z.; Tang, Y.; Song, Q.; Zhang, J.; Xie, W.; He, Y.; Huang, R.; Zheng, X.; Liu, C.; Liu, J. Gene polymorphisms in VEGFA and COL2A1 are associated with response to inhaled corticosteroids in children with asthma. Pharmacogenomics 2019, 20, 947–955. [Google Scholar] [CrossRef]
- Hernandez-Pacheco, N.; Farzan, N.; Francis, B.; Karimi, L.; Repnik, K.; Vijverberg, S.J.; Soares, P.; Schieck, M.; Gorenjak, M.; Forno, E.; et al. Genome-wide association study of inhaled corticosteroid response in admixed children with asthma. Clin. Exp. Allergy 2019, 49, 789–798. [Google Scholar] [CrossRef] [Green Version]
- Hernandez-Pacheco, N.; Gorenjak, M.; Li, J.; Repnik, K.; Vijverberg, S.J.; Berce, V.; Jorgensen, A.; Karimi, L.; Schieck, M.; Samedy-Bates, L.-A.; et al. Identification of ROBO2 as a Potential Locus Associated with Inhaled Corticosteroid Response in Childhood Asthma. J. Pers. Med. 2021, 11, 733. [Google Scholar] [CrossRef] [PubMed]
- Dahlin, A.; Sordillo, J.E.; McGeachie, M.; Kelly, R.S.; Tantisira, K.G.; Lutz, S.M.; Lasky-Su, J.; Wu, A.C. Genome-wide in-teraction study reveals age-dependent determinants of responsiveness to inhaled corticosteroids in individuals with asthma. PLoS ONE 2020, 15, e0229241. [Google Scholar] [CrossRef]
- Hernandez-Pacheco, N.; Vijverberg, S.J.; Herrera-Luis, E.; Li, J.; Sio, Y.Y.; Granell, R.; Corrales, A.; Maroteau, C.; Lethem, R.; Perez-Garcia, J.; et al. Genome-wide association study of asthma exacerbations despite inhaled corticosteroid use. Eur. Respir. J. 2020, 57, 2003388. [Google Scholar] [CrossRef] [PubMed]
- Ortega, V.E.; Daya, M.; Szefler, S.J.; Bleecker, E.R.; Chinchilli, V.M.; Phipatanakul, W.; Mauger, D.; Martinez, F.D.; Herre-ra-Luis, E.; Pino-Yanes, M.; et al. NHLBI AsthmaNet. Pharmacogenetic studies of long-acting β agonist and inhaled corticosteroid responsiveness in randomised controlled trials of individuals of African descent with asthma. Lancet Child Adolesc. Health 2021, 5, 862–872. [Google Scholar] [CrossRef]
- Maroteau, C.; Espuela-Ortiz, A.; Herrera-Luis, E.; Srinivasan, S.; Carr, F.; Tavendale, R.; Wilson, K.; Hernandez-Pacheco, N.; Chalmers, J.D.; Turner, S.; et al. LTA4H rs2660845 association with montelukast response in early and late-onset asthma. PLoS ONE 2021, 16, e0257396. [Google Scholar] [CrossRef] [PubMed]
- Lemanske, R.F., Jr.; Mauger, D.T.; Sorkness, C.A.; Jackson, D.J.; Boehmer, S.J.; Martinez, F.D.; Strunk, R.C.; Szefler, S.J.; Zeiger, R.S.; Bacharier, L.B.; et al. Step-up therapy for children with uncontrolled asthma receiving inhaled corticosteroids. N. Engl. J. Med. 2010, 362, 975–985. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wechsler, M.E.; Castro, M.; Lehman, E.; Chinchilli, V.M.; Sutherland, E.R.; Denlinger, L.; Lazarus, S.C.; Peters, S.P.; Israel, E. Impact of Race on Asthma Treatment Failures in the Asthma Clinical Research Network. Am. J. Respir. Crit. Care Med. 2011, 184, 1247–1253. [Google Scholar] [CrossRef]
- Malka, J.; Mauger, D.T.; Covar, R.; Rabinovitch, N.; Lemanske, R.F., Jr.; Spahn, J.D.; Strunk, R.C.; Zeiger, R.S.; Morgan, W.J.; Szefler, S.J. Eczema and race as combined determinants for differential response to step-up asthma therapy. J. Allergy Clin. Immunol. 2014, 134, 483–485. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cohn, I.; Manshaei, R.; Liston, E.; Okello, J.B.A.; Khan, R.; Curtis, M.R.; Krupski, A.J.; Jobling, R.K.; Kalbfleisch, K.; Paton, T.A.; et al. Assessment of the Implementation of Pharmacogenomic Testing in a Pediatric Tertiary Care Setting. JAMA Netw. Open 2021, 4, e2110446. [Google Scholar] [CrossRef]
- van der Wouden, C.H.; on behalf of the Ubiquitous-Pharmacogenomics Consortium; Swen, J.J.; Samwald, M.; Mitropoulou, C.; Schwab, M.; Guchelaar, H.-J. A brighter future for the implementation of pharmacogenomic testing. Eur. J. Hum. Genet. 2016, 24, 1658–1660. [Google Scholar] [CrossRef] [Green Version]
- Rahawi, S.; Naik, H.; Blake, K.V.; Obeng, A.O.; Wasserman, R.M.; Seki, Y.; Funanage, V.L.; Oishi, K.; Scott, S.A. Knowledge and attitudes on pharmacogenetics among pediatricians. J. Hum. Genet. 2020, 65, 437–444. [Google Scholar] [CrossRef] [Green Version]
- Tonk, E.C.M.; Gurwitz, D.; Der Zee, A.-H.M.-V.; Janssens, A.C.J.W. Assessment of pharmacogenetic tests: Presenting measures of clinical validity and potential population impact in association studies. Pharmacogenomics J. 2016, 17, 386–392. [Google Scholar] [CrossRef] [PubMed]
- Slob, E.M.A.; Vijverberg, S.J.H.; Pijnenburg, M.W.; Koppelman, G.H.; Maitland-van der Zee, A.H. What do we need to transfer pharmacogenetics findings into the clinic? Pharmacogenomics 2018, 19, 589–592. [Google Scholar] [CrossRef]
- Fishe, J.N.; Higley, R.K.; Casey, D.; Hogans, L.; Wylie, T.W.; Hendry, P.L.; Henson, M.; Bertrand, A.; Blake, K.V. Methods and implementation of a pediatric asthma pharmacogenomic study in the emergency department setting. Pharmacogenetics Genom. 2020, 30, 201–207. [Google Scholar] [CrossRef] [PubMed]
- Trust, C.F. Life-Saving Drugs. 2020. Available online: https://www.cysticfibrosis.org.uk/the-work-we-do/campaigning-hard/life-saving-drugs (accessed on 13 February 2022).
- Farzan, N.; Vijverberg, S.J.; Andiappan, A.K.; Arianto, L.; Berce, V.; Blanca-López, N.; Bisgaard, H.; Bønnelykke, K.; Burchard, E.G.; Campo, P.; et al. Rationale and design of the multiethnic Pharmacogenomics in Childhood Asthma consortium. Pharmacogenomics 2017, 18, 931–943. [Google Scholar] [CrossRef] [PubMed]
- Parry, C.M.; Seddon, G.; Rogers, N.; Sinha, I.P.; Bracken, L.; King, C.; Peak, M.; Hawcutt, D.B. Pharmacogenomics and asthma treatment: Acceptability to children, families and healthcare professionals. Arch. Dis. Child. 2022, 107, 394–399. [Google Scholar] [CrossRef] [PubMed]
- Vijverberg, S.; Farzan, N.; Slob, E.M.A.; Neerincx, A.H.; Der Zee, A.H.M.-V. Treatment response heterogeneity in asthma: The role of genetic variation. Expert Rev. Respir. Med. 2017, 12, 55–65. [Google Scholar] [CrossRef] [Green Version]
- Feero, W.G.; Guttmacher, A.E. Genomics, personalized medicine, and pediatrics. Acad. Pediatr. 2014, 14, 14–22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ober, C. Asthma Genetics in the Post-GWAS Era. Ann. Am. Thorac. Soc. 2016, 13, S85–S90. [Google Scholar] [CrossRef]
- Bush, W.; Oetjens, M.T.; Crawford, D. Unravelling the human genome–phenome relationship using phenome-wide association studies. Nat. Rev. Genet. 2016, 17, 129–145. [Google Scholar] [CrossRef]
- Diogo, D.; Tian, C.; Franklin, C.S.; Kinnunen, M.; March, M.; Spencer, C.C.A.; Vangjeli, C.; Weale, M.; Mattsson, H.; Kilpeläinen, E.; et al. Phenome-wide association studies across large population cohorts support drug target validation. Nat. Commun. 2018, 9, 4285. [Google Scholar] [CrossRef] [Green Version]
- Denny, J.C.; Bastarache, L.; Roden, D.M. Phenome-Wide Association Studies as a Tool to Advance Precision Medicine. Annu. Rev. Genom. Hum. Genet. 2016, 17, 353–373. [Google Scholar] [CrossRef] [Green Version]
- Chen, S.; Tao, A. The Pharmacogenomics of Asthma Beyond its Endotypes. Curr. Drug Metab. 2018, 19, 1206–1212. [Google Scholar] [CrossRef]
- van der Schee, M.P.; Palmay, R.; Cowan, J.O.; Taylor, D.R. Predicting steroid responsiveness in patients with asthma using exhaled breath profiling. Clin. Exp. Allergy 2013, 43, 1217–1225. [Google Scholar] [CrossRef] [PubMed]
- Wysocki, K.; Conley, Y.; Wenzel, S. Epigenome Variation in Severe Asthma. Biol. Res. Nurs. 2014, 17, 263–269. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brinkman, P.; Van De Pol, M.A.; Gerritsen, M.G.; Bos, L.; Dekker, T.; Smids, B.S.; Sinha, A.; Majoor, C.; Sneeboer, M.M.; Knobel, H.H.; et al. Exhaled breath profiles in the monitoring of loss of control and clinical recovery in asthma. Clin. Exp. Allergy 2017, 47, 1159–1169. [Google Scholar] [CrossRef] [PubMed]
- BBMRI-ERIC®. Available online: https://www.bbmri-eric.eu/ (accessed on 22 February 2022).
- ELIXIR. Available online: https://elixir-europe.org/ (accessed on 22 February 2022).
- Chanfreau-Coffinier, C. Clinical Implications of Pharmacogenomic Testing in the Real World-Insights From a Pediatric Pro-gram. JAMA Netw. Open. 2021, 4, e2110467. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Author, Year | Study Design | Study Population | Aim | Results | Comments |
|---|---|---|---|---|---|
| Short-acting β agonists | |||||
| Mak, A.C.Y.; et al. Am J Respir Crit Care Med. 2018 [18] | WGS study | 1441 minority children with asthma from three ethnic groups (483 Puerto Ricans, 483 Mexicans, 475 African-Americans) | To identify genetic association with BDR | rs17834628 (OR: 1.67, 95% CI: 1.29–2.16, p = 1.18 × 10−8) and rs35661809 (OR: 1.59, 95% CI: 1.20–2.10, p = 3.33 × 10−8), including genome-wide significant (p < 3.53 × 10−7) and suggestive (p < 7.06 × 10−6) three specific-population loci (1p13.2 and 11p14.1 in Mexicans and 19p13.2 in African-Americans) and two shared-population loci (4q13.3 and 8q22.1) near genes DNAH5, NFKB1, PLCB1, ADAMTS3 and COX18 significantly associated with BDR | Population-specific and shared genetic variants were associated with BDR in three different ethnic populations of children with asthma |
| Spear M.L.; et al. JAMA Pharmacogenomics J. 2019 [19] | GWAS | 949 African American minority children with asthma | To identify genetic association with BDR | rs73650726 on chromosome 9q21 (p = 7.69 × 10−9) and three DNA variants within the intron of PRKG1 significantly associated with BDR (rs7903366, rs7070958, and rs7081864, p ≤ 5 × 10−8) | Population-specific and shared DNA variants contribute to differences in BDR in minority children with asthma |
| Fishe, J.N.; et al. Pharmacogenet Genomics. 2021 [20] | Prospective pilot study | 53 African American children with asthma | To identify genetic association with BDR during an acute asthma attack | rs912142 associated with decreased risk of low BDR (OR: 0.20; 95% CI: 0.02–0.92); rs7081864 and rs7903366 associated with decreased risk of high BDR (OR: 0.097; 95% CI: 0.009–0.62) | Genetic variants provide information regarding a child’s potential response to emergency asthma exacerbation treatment |
| Scaparrotta, A.; et al. J Aerosol Med Pulm Drug Deliv. 2019 [21] | Preliminary observational prospective study | 100 children with persistent asthma | To verify the association of genetic variants of ADRB2, THRB and ARG1 with BDR | Arg/Gly or Gly/Gly rs1042713 significantly associated with a worse BDR (post-BD FEV1: 108.68–15.62% in Arg/Arg vs. 101.86–14.03% in Arg/Gly or Gly/Gly patients, p = 0.02). No significant association for the other three examined DNA variants | Arg16Gly in ADRB2 gene is associated with a worse response to SABA in children with persistent asthma |
| Long-acting β agonists | |||||
| Slob, E.M.A.; et al. Pediatr Allergy Immunol. 2021 [22] | Meta-analysis of GWAS | 1425 children and young adults with asthma | To identify genetic association with exacerbations | Eight genetic variants suggestively (p threshold ≤5 × 10−6) associated with exacerbations despite LABA use; two DNA variants near loci TBX3 and EPHA7 identified. | Pharmacogenetic markers can determine whether children experience exacerbations despite LABA use |
| Slob, E.M.A.; et al. Pediatr Allergy Immunol. 2018 [23] | Systematic review of pharmacogenetic studies in patients with asthma treated with LABA | 6051 children with asthma | To identify genetic variants associated with LABA response | The ADRB2 rs1042713 variant was significantly associated with response to LABA; increased risk of exacerbations found in children carrying one or two A alleles (OR: 1.52, 95% CI: 1.17–1.99) | ADRB2 rs1042713 variant is associated with response to LABA in children |
| Inhaled corticosteroids | |||||
| Farzan, N.; et al. Clin Exp Allergy J. 2017 [24] | Systematic review of pharmacogenomics and pharmacogenetics of ICS in patients with asthma | Children and adolescents from 29 candidate gene studies and 4 GWAS | To identify genetic variants associated with ICS response | The FCER2 rs28364072 variant associated with asthma symptoms, poor lung function, the largest effect reported with the risk of exacerbations (hazard ratio: 3.95; 95% CI: 1.64–9.51) | A lack of replication of genetic variants is associated with poor ICS response. Most consistent findings found for the FCER2 gene |
| Huang, J.; et al. BMC Pulm. Med. 2020 [25] | Observational prospective study | 263 children with asthma | To determine the associations between GLCCI1 genetic variants and ICS response | GLCCI1 rs37969 minor genotypes (TT/GT) associated with less improvement in airway hyper-responsiveness (p = 0.028); significant associations between genetic variants rs37969, rs37972 and rs37973 minor genotypes and less improvement in pulmonary function (p = 0.036, p = 0.010 and p = 0.003, respectively) | GLCCI1 rs37969 minor genotypes is associated with less improvement in airway hyper-responsiveness. GLCCI1 rs37969, rs37972 and rs37973 genetic variants are associated with pulmonary function in children with asthma after ICS treatment. |
| Farzan, N.; Allergy. 2018 [26] | Observational study | 4000 asthmatic children/young adults treated with ICS | To study the association between genetic variant 17q21 rs7216389 and asthma exacerbations despite ICS use | 17q21 rs7216389 associated with an increased risk of oral corticosteroids use (summary OR per increase in variant allele: 1.19, 95% CI: 1.04–1.36, p = 0.01) and asthma-related hospitalizations/emergency visits (summary OR per increase in risk allele: 1.32, 95% CI: 1.17–1.49, p < 0.0001) | 17q21 is associated with an increased risk of exacerbations in children/young adults treated with ICS |
| Wan, Z.; et al. Pharmacogenomics. 2019 [27] | Observational prospective study | 128 children with mild-to-moderate asthma | To investigate the involvement of genetic variants in VEGFA, TBX21 and COL2A1 in the response to ICS | Change in FEV1 after ICS treatment in VEGFA rs3025039 minor homozygotes (TT) and heterozygotes (CT) smaller than that in major homozygotes (CC) (p = 0.040), and associated with changes in FEV1/FVC ratio (p = 0.016). Children with the minor homozygous (TT) and heterozygous (GT) genotypes at COL2A1 rs3809324 had less improvement in FEV1 than those with the major homozygous (GG) genotype (p = 0.048) | VEGFA and COL2A1 variants are associated with the response to ICS in asthmatic children |
| Hernandez-Pacheco, N.; et al. Clin Exp Allergy J. 2019 [28] | Meta-analysis of GWAS | 1347 Hispanics/Latinos and African-American children with asthma on ICS treatment | To identify genetic variants associated with asthma attacks in children on ICS treatment, and to validate previous GWAS findings | DNA variant rs5995653 in the intergenic region of APOBEC3B and APOBEC3C replicated in Europeans (p = 7.52 × 10−3) and associated with change in FEV1 (p = 4.91 × 10−3). DNA variant rs62081416 near L3MBTL4-ARHGAP28 associated with ICS response in African-admixed children (OR: 2.44, 95% CI: 1.63–3.65, p = 1.57 × 10−5) | APOBEC3B and APOBEC3C genes are associated with ICS response in asthmatic children. The association of the L3MBTL4-ARHGAP28 genomic region previously described in a GWAS of ICS response in subjects of European descent was validated in admixed children |
| Hernandez-Pacheco, N.; et al. J Pers Med. 2021 [29] | GWAS | 166 asthma patients, including children and young adults | To identify novel genetic variants involved in ICS response in patients with asthma | The DNA variant rs1166980 from the ROBO2 gene associated with change in FEV1 (OR: 7.01, 95% CI: 3.29–14.93, p = 4.61 × 10−7) | ROBO2 is a potential novel locus for ICS response in Europeans |
| Dahlin, A.; Plos One. 2020 [30] | GWIS | 1321 patients with asthma, including children and adults | To identify genetic variants associated with response to ICS | The top-ranked age-by-genotype association found for the DNA variant rs34631960 in THSD4, which could be protective against exacerbations risk in younger patients taking ICS, or may predict an increased risk of poor ICS response in older patients | Age-specific genetic mechanisms may regulate response to ICS |
| Hernandez-Pacheco, N.; et al. Eur Respir J. 2021 [31] | GWAS | 2681 children with asthma of European descent on ICS treatment | To identify genetic variants associated with asthma exacerbations | Ten genetic variants associated with asthma exacerbations (p ≤ 5 × 10−6). One variant at the CACNA2D3-WNT5A locus replicated in Europeans (rs67026078; p = 0.010), but not in non-European populations. | The intergenic region of CACNA2D3 and WNT5A could be a novel locus for asthma exacerbations despite ICS treatment in European children |
| Inhaled corticosteroids + Long-acting β agonists | |||||
| Ortega, V.E.; et al. Lancet Child Adolesc Health. 2021 [32] | Ancestry-based pharmacogenetic studies of children, adolescents and adults from the Best African Response to Drug trials | 249 children and 267 adolescents and adults of African descent | To understand the pharmacogenetic mechanisms regulating therapeutic responsiveness to ICS + LABA | In children, a locus for quintupling ICS vs. adding a LABA identified close to RNFT2 and NOS1 (rs73399224, OR: 0.7, 95% CI: 0.07–0.42, p = 8.4 × 10−5) | Including ancestral diversity is crucial in the identification of reliable precision medicine profiles of drug response in asthmatic patients |
| Leukotriene modifiers | |||||
| Farzan, N.; et al. Clin Exp Allergy J. 2017 [24] | Systematic review of pharmacogenomics and pharmacogenetics of LTMs in patients with asthma | Children and adolescents from 24 candidate gene studies and 2 GWAS | To identify genetic variants associated with LTMs response | No consistent findings for candidate gene studies of LTMs. | A lack of replication of genetic variants is associated with poor LTMs response |
| Maroteau, C.; Plos One. 2021 [33] | Meta-analysis of seven cohort studies | 3594 patients with asthma treated with montelukast for at least 6 months (2514 late-onset: >18 years, and 1080 early-onset: ≤18 years) from seven cohorts | To investigate the role of the LTA4H genetic variant rs2660845 and the age of asthma onset in response to montelukast | Increased risk of exacerbation under montelukast treatment in European individuals with early-onset carrying at least one copy of rs2660845 (OR: 2.92, 95% CI: 1.04–8.18, p = 0.0412) | Genetic variation in LTA4H, together with the age of asthma onset, may contribute to variability in montelukast response |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ferrante, G.; Fasola, S.; Malizia, V.; Licari, A.; Cilluffo, G.; Piacentini, G.; La Grutta, S. Pharmacogenomics: A Step forward Precision Medicine in Childhood Asthma. Genes 2022, 13, 599. https://doi.org/10.3390/genes13040599
Ferrante G, Fasola S, Malizia V, Licari A, Cilluffo G, Piacentini G, La Grutta S. Pharmacogenomics: A Step forward Precision Medicine in Childhood Asthma. Genes. 2022; 13(4):599. https://doi.org/10.3390/genes13040599
Chicago/Turabian StyleFerrante, Giuliana, Salvatore Fasola, Velia Malizia, Amelia Licari, Giovanna Cilluffo, Giorgio Piacentini, and Stefania La Grutta. 2022. "Pharmacogenomics: A Step forward Precision Medicine in Childhood Asthma" Genes 13, no. 4: 599. https://doi.org/10.3390/genes13040599
APA StyleFerrante, G., Fasola, S., Malizia, V., Licari, A., Cilluffo, G., Piacentini, G., & La Grutta, S. (2022). Pharmacogenomics: A Step forward Precision Medicine in Childhood Asthma. Genes, 13(4), 599. https://doi.org/10.3390/genes13040599