
Radiogenomic Features of GIMAP Family Genes in Clear Cell Renal Cell Carcinoma: An Observational Study on CT Images

 ,
,  ,
,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. The Cancer Genome Atlas
2.2. ccRCC Patients
2.3. Imaging Features
2.4. Imaging Analyses
2.5. Statistical Analyses
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kuo, M.D.; Jamshidi, N. Behind the numbers: Decoding molecular phenotypes with radiogenomics-guiding principles and technical considerations. Radiology 2014, 270, 320–325. [Google Scholar] [CrossRef] [PubMed]
- Lander, E.S.; Linton, L.M.; Birren, B.; Nusbaum, C.; Zody, M.C.; Baldwin, J.; Devon, K.; Dewar, K.; Doyle, M.; FitzHugh, W.; et al. Initial sequencing and analysis of the human genome. Nature 2001, 409, 860–921. [Google Scholar] [PubMed]
- The Cancer Genome Atlas Research Network. Comprehensive molecular characterization of clear cell renal cell carcinoma. Nature 2012, 499, 43–49. [Google Scholar]
- Karlo, C.A.; Di Paolo, P.L.; Chaim, J.; Hakimi, A.A.; Ostrovnaya, I.; Russo, P.; Hricak, H.; Motzer, R.; Hsieh, J.J.; Akin, O. Radiogenomics of clear cell renal cell carcinoma: Associations between CT imaging features and mutations. Radiology 2014, 270, 464–471. [Google Scholar] [CrossRef]
- Shinagare, A.B.; Vikram, R.; Jaffe, C.; Akin, O.; Kirby, J.; Huang, E.; Freymann, J.; Sainani, N.I.; Sadow, C.A.; Bathala, T.K.; et al. Radiogenomics of clear cell renal cell carcinoma: Preliminary findings of The Cancer Genome Atlas-Renal Cell Carcinoma (TCGA-RCC) Imaging Research Group. Abdom. Imaging 2015, 40, 1684–1692. [Google Scholar] [CrossRef]
- Alessandrino, F.; Krajewski, K.M.; Shinagare, A.B. Update on radiogenomics of clear cell renal cell carcinoma. Eur. Urol. Focus 2016, 2, 572–573. [Google Scholar] [CrossRef]
- Pinker, K.; Shitano, F.; Sala, E.; Do, R.K.; Young, R.J.; Wibmer, A.G.; Hricak, H.; Sutton, E.J.; Morris, E.A. Background, current role, and potential applications of radiogenomics. J. Magn. Reson. Imaging 2018, 47, 604–620. [Google Scholar] [CrossRef]
- Gerlinger, M.; Rowan, A.J.; Horswell, S.; Math, M.; Larkin, J.; Endesfelder, D.; Gronroos, E.; Martinez, P.; Matthews, N.; Stewart, A.; et al. Intratumor heterogeneity and branched evolution revealed by multiregion sequencing. N. Engl. J. Med. 2012, 366, 883–892, Erratum in: N. Engl. J. Med. 2012, 367, 976. [Google Scholar] [CrossRef]
- Kreso, A.; O’Brien, C.A.; van Galen, P.; Gan, O.I.; Notta, F.; Brown, A.M.; Ng, K.; Ma, J.; Wienholds, E.; Dunant, C.; et al. Variable clonal repopulation dynamics influence chemotherapy response in colorectal cancer. Science 2013, 339, 543–548. [Google Scholar] [CrossRef]
- Greco, F.; Mallio, C.A. Relationship between visceral adipose tissue and genetic mutations (VHL and KDM5C) in clear cell renal cell carcinoma. Radiol. Med. 2021, 126, 645–651. [Google Scholar] [CrossRef]
- Greco, F.; Tafuri, A.; Grasso, R.F.; Beomonte Zobel, B.; Mallio, C.A. Clinicopathological and Body Composition Analysis of VHL and TTN Gene Mutations in Clear Cell Renal Cell Carcinoma: An Exploratory Study. Appl. Sci. 2022, 12, 9502. [Google Scholar] [CrossRef]
- Pagès, F.; Kirilovsky, A.; Mlecnik, B.; Asslaber, M.; Tosolini, M.; Bindea, G.; Lagorce, C.; Wind, P.; Marliot, F.; Bruneval, P.; et al. In situ cytotoxic and memory T cells predict outcome in patients with early-stage colorectal cancer. J. Clin. Oncol. 2009, 27, 5944–5951. [Google Scholar] [CrossRef]
- Gajewski, T.F.; Schreiber, H.; Fu, Y.X. Innate and adaptive immune cells in the tumor microenvironment. Nat. Immunol. 2013, 14, 1014–1022. [Google Scholar] [CrossRef]
- Tumeh, P.C.; Harview, C.L.; Yearley, J.H.; Shintaku, I.P.; Taylor, E.J.; Robert, L.; Chmielowski, B.; Spasic, M.; Henry, G.; Ciobanu, V.; et al. PD-1 blockade induces responses by inhibiting adaptive immune resistance. Nature 2014, 515, 568–571. [Google Scholar] [CrossRef]
- Krucken, J.; Schroetel, R.M.; Muller, I.U.; Saidani, N.; Marinovski, P.; Benten, W.P.; Stamm, O.; Wunderlich, F. Comparative analysis of the human gimap gene cluster encoding a novel GTPase family. Gene 2004, 341, 291–304. [Google Scholar] [CrossRef] [PubMed]
- Zenz, T.; Roessner, A.; Thomas, A.; Frohling, S.; Dohner, H.; Calabretta, B.; Dahéron, L. hIan5: The human ortholog to the rat Ian4/Iddm1/lyp is a new member of the Ian family that is overexpressed in B-cell lymphoid malignancies. Genes Immun. 2004, 5, 109–116. [Google Scholar] [CrossRef] [PubMed]
- Datta, P.; Webb, L.M.; Avdo, I.; Pascall, J.; Butcher, G.W. Survival of mature T cells in the periphery is intrinsically dependent on GIMAP1 in mice. Eur. J. Immunol. 2017, 47, 84–93. [Google Scholar] [CrossRef] [PubMed]
- Webb, L.M.; Datta, P.; Bell, S.E.; Kitamura, D.; Turner, M.; Butcher, G.W. GIMAP1 Is Essential for the Survival of Naive and Activated B Cells In Vivo. J. Immunol. 2016, 196, 207–216. [Google Scholar] [CrossRef] [PubMed]
- Limoges, M.A.; Cloutier, M.; Nandi, M.; Ilangumaran, S.; Ramanathan, S. The GIMAP Family Proteins: An Incomplete Puzzle. Front. Immunol. 2021, 12, 679739. [Google Scholar] [CrossRef]
- Schnell, S.; Demolliere, C.; van den Berk, P.; Jacobs, H. Gimap4 accelerates T-cell death. Blood 2006, 108, 591–599. [Google Scholar] [CrossRef] [PubMed]
- Ho, C.H.; Tsai, S.F. Functional and biochemical characterization of a T cell-associated anti-apoptotic protein, GIMAP6. J. Biol. Chem. 2017, 292, 9305–9319. [Google Scholar] [CrossRef] [PubMed]
- CIP TCGA Radiology Initiative—The Cancer Imaging Archive (TCIA) Public Access—Cancer Imaging Archive Wiki. Available online: https://wiki.cancerimagingarchive.net/display/Public/CIP+TCGA+Radiology+Initiative;jsessionid=92ACC1CC632A2219F9A6F965E2325B68 (accessed on 1 November 2019).
- Greco, F.; Panunzio, A.; Tafuri, A.; Bernetti, C.; Pagliarulo, V.; Beomonte Zobel, B.; Scardapane, A.; Mallio, C.A. CT-Based Radiogenomics of P4HA3 Expression in Clear Cell Renal Cell Carcinoma. Acad. Radiol. 2023, S1076-6332(23)00351-3. [Google Scholar] [CrossRef] [PubMed]
- Chevrier, S.; Levine, J.H.; Zanotelli, V.R.T.; Silina, K.; Schulz, D.; Bacac, M.; Ries, C.H.; Ailles, L.; Jewett, M.A.S.; Moch, H.; et al. An Immune Atlas of Clear Cell Renal Cell Carcinoma. Cell 2017, 169, 736–749.e18. [Google Scholar] [CrossRef] [PubMed]
- Barnes, M.J.; Aksoylar, H.; Krebs, P.; Bourdeau, T.; Arnold, C.N.; Xia, Y.; Khovananth, K.; Engel, I.; Sovath, S.; Lampe, K.; et al. Loss of T cell and B cell quiescence precedes the onset of microbial flora-dependent wasting disease and intestinal inflammation in Gimap5-deficient mice. J. Immunol. 2010, 184, 3743–3754. [Google Scholar] [CrossRef]
- Schulteis, R.D.; Chu, H.; Dai, X.; Chen, Y.; Edwards, B.; Haribhai, D.; Williams, C.B.; Malarkannan, S.; Hessner, M.J.; Glisic-Milosavljevic, S.; et al. Impaired survival of peripheral T cells, disrupted 365 NK/NKT cell development, and liver failure in mice lacking Gimap5. Blood 2008, 112, 4905–4914. [Google Scholar] [CrossRef]
- Varn, F.S.; Wang, Y.; Mullins, D.W.; Fiering, S.; Cheng, C. Systematic Pan-Cancer Analysis Reveals Immune Cell Interactions in the Tumor Microenvironment. Cancer Res. 2017, 77, 1271–1282. [Google Scholar] [CrossRef]
- Noessner, E.; Brech, D.; Mendler, A.N.; Masouris, I.; Schlenker, R.; Prinz, P.U. Intratumoral alterations of dendritic-cell differentiation and CD8(+) T-cell anergy are immune escape mechanisms of clear cell renal cell carcinoma. Oncoimmunology 2012, 1, 1451–1453. [Google Scholar] [CrossRef]
- Giraldo, N.A.; Becht, E.; Vano, Y.; Petitprez, F.; Lacroix, L.; Validire, P.; Sanchez-Salas, R.; Ingels, A.; Oudard, S.; Moatti, A.; et al. Tumor-Infiltrating and Peripheral Blood T-cell Immunophenotypes Predict Early Relapse in Localized Clear Cell Renal Cell Carcinoma. Clin. Cancer Res. 2017, 23, 4416–4428. [Google Scholar] [CrossRef]
- Giraldo, N.A.; Becht, E.; Pagès, F.; Skliris, G.; Verkarre, V.; Vano, Y.; Mejean, A.; Saint-Aubert, N.; Lacroix, L.; Natario, I.; et al. Orchestration and Prognostic Significance of Immune Checkpoints in the Microenvironment of Primary and Metastatic Renal Cell Cancer. Clin. Cancer Res. 2015, 21, 3031–3040. [Google Scholar] [CrossRef]
- Dungan, L.S.; McGuinness, N.C.; Boon, L.; Lynch, M.A.; Mills, K.H. Innate IFN-γ promotes development of experimental autoimmune encephalomyelitis: A role for NK cells and M1 macrophages. Eur. J. Immunol. 2014, 44, 2903–2917. [Google Scholar] [CrossRef]
- Deng, S.; Zhang, Z.; Lu, X.; Zhou, Q.; Xia, S.; Li, M. Systemic analyses of expression patterns and clinical features for GIMAPs family members in lung adenocarcinoma. Aging 2020, 12, 20413–20431. [Google Scholar] [CrossRef] [PubMed]
- Meng, Z.; Ren, D.; Zhang, K.; Zhao, J.; Jin, X.; Wu, H. Using ESTIMATE algorithm to establish an 8-mRNA signature prognosis prediction system and identify immunocyte infiltration-related genes in Pancreatic adenocarcinoma. Aging 2020, 12, 5048–5070. [Google Scholar] [CrossRef] [PubMed]
- Brugarolas, J. Molecular genetics of clear-cell renal cell carcinoma. J. Clin. Oncol. 2014, 32, 1968–1976. [Google Scholar] [CrossRef] [PubMed]
- Motzer, R.J.; Rini, B.I.; McDermott, D.F.; Redman, B.G.; Kuzel, T.M.; Harrison, M.R.; Vaishampayan, U.N.; Drabkin, H.A.; George, S.; Logan, T.F. Nivolumab for Metastatic Renal Cell Carcinoma: Results of a Randomized Phase II Trial. J. Clin. Oncol. 2015, 33, 1430–1437. [Google Scholar] [CrossRef] [PubMed]
- Farolfi, A.; Schepisi, G.; Conteduca, V.; Burgio, S.L.; Lolli, C.; De Giorgi, U. Pharmacokinetics, pharmacodynamics and clinical 458 efficacy of nivolumab in the treatment of metastatic renal cell carcinoma. Expert Opin. Drug Metab. Toxicol. 2016, 12, 1089–1096. [Google Scholar] [CrossRef] [PubMed]
- Xu, W.; Atkins, M.B.; McDermott, D.F. Checkpoint inhibitor immunotherapy in kidney cancer. Nat. Rev. Urol. 2020, 17, 137–150. [Google Scholar] [CrossRef]
- Şenbabaoğlu, Y.; Gejman, R.S.; Winer, A.G.; Liu, M.; Van Allen, E.M.; de Velasco, G.; Miao, D.; Ostrovnaya, I.; Drill, E.; Luna, A.; et al. Tumor immune microenvironment characterization in clear cell renal cell carcinoma identifies prognostic and immunotherapeutically relevant messenger RNA signatures. Genome Biol. 2016, 17, 231, Erratum in: Genome Biol. 2017, 18, 46. [Google Scholar] [CrossRef]
- Snyder, A.; Makarov, V.; Merghoub, T.; Yuan, J.; Zaretsky, J.M.; Desrichard, A.; Walsh, L.A.; Postow, M.A.; Wong, P.; Ho, T.S.; et al. Genetic basis for clinical response to CTLA-4 blockade in melanoma. N. Engl. J. Med. 2014, 371, 2189–2199, Erratum in: N. Engl. J. Med. 2018, 379, 2185. [Google Scholar] [CrossRef]
- Rizvi, N.A.; Hellmann, M.D.; Snyder, A.; Kvistborg, P.; Makarov, V.; Havel, J.J.; Lee, W.; Yuan, J.; Wong, P.; Ho, T.S.; et al. Cancer immunology. Mutational landscape determines sensitivity to PD-1 blockade in non-small cell lung cancer. Science 2015, 348, 124–128. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| GIMAPs | Localization | Activity in Human |
|---|---|---|
| GIMAP 1 [17,18,19] | Golgi apparatus | Maintenance of T cells proliferation and mature B cells function |
| GIMAP 2 [19] | Lipid droplets | Not known |
| GIMAP 3 [19] | Endoplasmic reticulum | Not known |
| GIMAP 4 [19,20] | Cytosolic | May promote T cells apoptosis |
| GIMAP 5 [19] | Lysosomes and vesicles | Deficiency determines: T cells and natural killer cells defects and replicative senescence in T cells |
| GIMAP 6 [19,21] | Autophagosomes | Leads Jurkat T cells more susceptible to apoptosis inducers |
| GIMAP 7 [19] | Cytosolic | Not known |
| GIMAP 8 [19] | Not known | Not known |
| Characteristic | Overall n = 193 a | GIMAP Family Genes Expression | p-Value b,c,d | |
|---|---|---|---|---|
| No n = 141 (73.1%) a | Yes n = 52 (26.9%) a | |||
| Clinical-pathological features | ||||
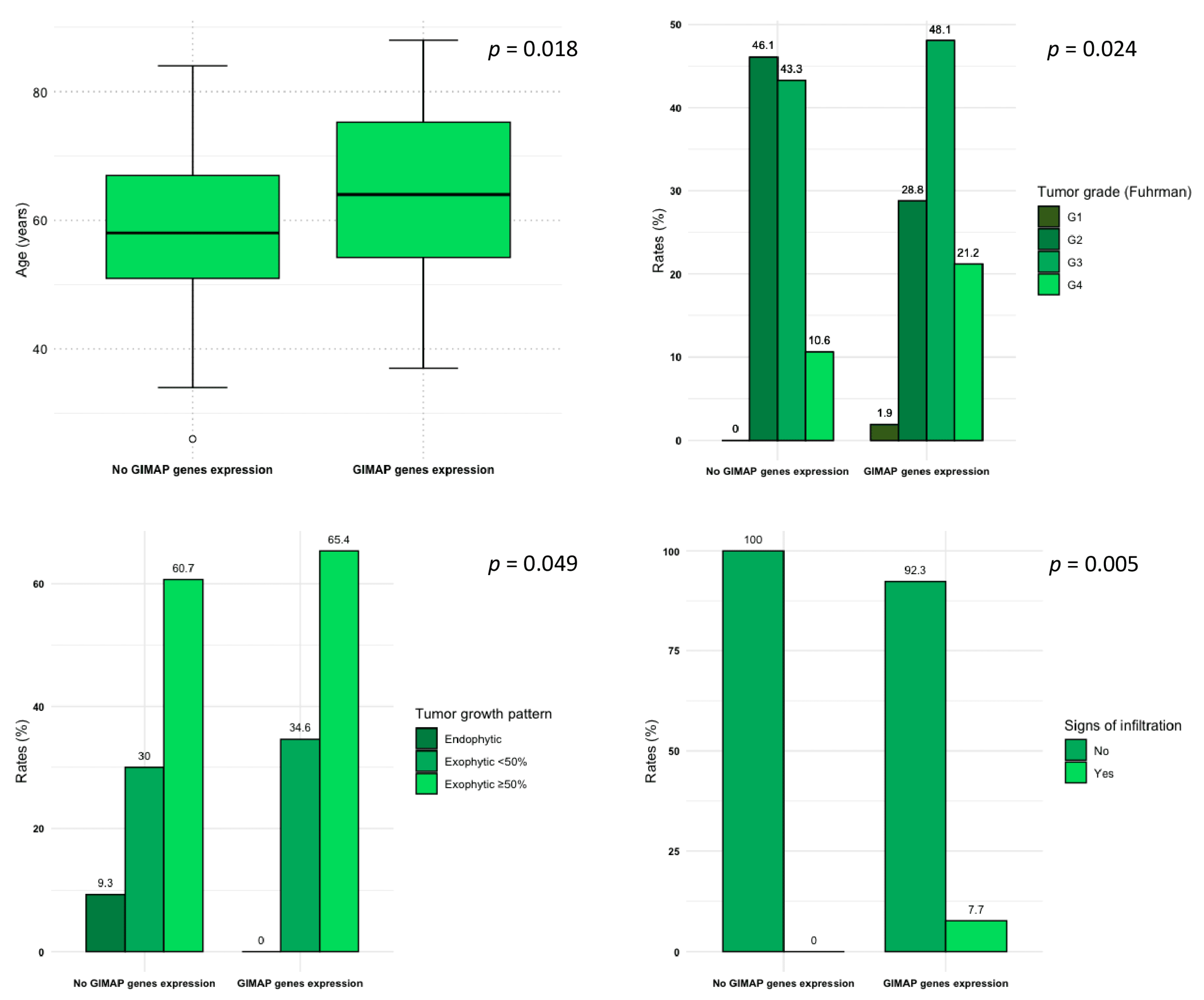
| Age (years) | 59 (51, 70) | 58 (51, 67) | 64 (54, 75) | 0.018 b |
| Sex (males) | 131 (67.9%) | 93 (66.0%) | 38 (73.1%) | 0.3 d |
| Primary tumor size (mm) | 52 (38, 78) | 52 (37, 78) | 55 (43, 71) | 0.4 b |
| Tumor grade (Fuhrman) G1 G2 G3 G4 | 1 (0.5%) 80 (41.5%) 86 (44.6%) 26 (13.4%) | 0 (0%) 65 (46.1%) 61 (43.3%) 15 (10.6%) | 1 (1.9%) 15 (28.8%) 25 (48.1%) 11 (21.2%) | 0.024 c |
| Tumor stage Stage I Stage II Stage III Stage IV | 105 (54.7%) 18 (9.3%) 46 (24.0%) 23 (12.0%) | 78 (55.7%) 15 (10.7%) 34 (24.3%) 13 (9.3%) | 27 (51.9%) 3 (5.8%) 12 (23.1%) 10 (19.2%) | 0.3 c |
| CT-based features | ||||
| Collateral vascular supply | 103 (54.8%) | 78 (57.4%) | 25 (48.1%) | 0.3 d |
| Tumor margins Ill-defined Well-defined | 64 (33.3%) 128 (66.7%) | 45 (32.1%) 95 (67.9%) | 19 (36.5%) 33 (63.5%) | 0.6 d |
| Tumor composition Solid Cystic | 176 (92.1%) 15 (7.9) | 129 (92.1%) 11 (7.9%) | 47 (92.2%) 4 (7.8%) | 0.9 c |
| Tumor necrosis 0% 1–33% 34–66% > 66% | 12 (6.2%) 115 (59.9%) 45 (23.4%) 20 (10.5%) | 9 (6.4%) 82 (58.6%) 34 (24.3%) 15 (10.7%) | 3 (5.8%) 33 (63.5%) 11 (21.2%) 5 (9.5%) | 0.9 c |
| Tumor growth pattern Endophytic Exophytic < 50% Exophytic ≥ 50% | 13 (6.8%) 60 (31.3%) 119 (61.9%) | 13 (9.3%) 42 (30.0%) 85 (60.7%) | 0 (0%) 18 (34.6%) 34 (65.4%) | 0.049 c |
| Calcifications | 34 (17.8%) | 22 (15.8%) | 12 (23.1%) | 0.2 d |
| Signs of infiltration | 4 (2.1%) | 0 (0.0%) | 4 (7.7%) | 0.005 c |
| Hydronephrosis | 6 (3.1%) | 3 (2.1%) | 3 (5.8%) | 0.3 c |
| Thrombosis or infiltration of renal artery | 4 (2.1%) | 3 (2.2%) | 1 (1.9%) | 0.9 c |
| Thrombosis or infiltration of renal vein | 12 (6.3%) | 9 (6.4%) | 3 (5.8%) | 0.9 c |
| Collecting system invasion | 58 (30.2%) | 41 (29.3%) | 17 (32.7%) | 0.6 d |
| Perinephric stranding | 88 (70.4%) | 64 (71.9%) | 24 (66.7%) | 0.6 d |
| Gerota’s fascia thickening | 59 (47.6%) | 43 (48.9%) | 16 (44.4%) | 0.7 d |
| Intralesional hemorrhage | 4 (2.1%) | 4 (2.9%) | 2 (3.8%) | 0.3 c |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Greco, F.; Panunzio, A.; Tafuri, A.; Bernetti, C.; Pagliarulo, V.; Beomonte Zobel, B.; Scardapane, A.; Mallio, C.A. Radiogenomic Features of GIMAP Family Genes in Clear Cell Renal Cell Carcinoma: An Observational Study on CT Images. Genes 2023, 14, 1832. https://doi.org/10.3390/genes14101832
Greco F, Panunzio A, Tafuri A, Bernetti C, Pagliarulo V, Beomonte Zobel B, Scardapane A, Mallio CA. Radiogenomic Features of GIMAP Family Genes in Clear Cell Renal Cell Carcinoma: An Observational Study on CT Images. Genes. 2023; 14(10):1832. https://doi.org/10.3390/genes14101832
Chicago/Turabian StyleGreco, Federico, Andrea Panunzio, Alessandro Tafuri, Caterina Bernetti, Vincenzo Pagliarulo, Bruno Beomonte Zobel, Arnaldo Scardapane, and Carlo Augusto Mallio. 2023. "Radiogenomic Features of GIMAP Family Genes in Clear Cell Renal Cell Carcinoma: An Observational Study on CT Images" Genes 14, no. 10: 1832. https://doi.org/10.3390/genes14101832
APA StyleGreco, F., Panunzio, A., Tafuri, A., Bernetti, C., Pagliarulo, V., Beomonte Zobel, B., Scardapane, A., & Mallio, C. A. (2023). Radiogenomic Features of GIMAP Family Genes in Clear Cell Renal Cell Carcinoma: An Observational Study on CT Images. Genes, 14(10), 1832. https://doi.org/10.3390/genes14101832