
Rett-like Phenotypes in HNRNPH2-Related Neurodevelopmental Disorder

Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Rett, A. On a Unusual Brain Atrophy Syndrome in Hyperammonemia in Childhood. Wien. Med. Wochenschr. 1966, 116, 723–726. [Google Scholar] [PubMed]
- Hagberg, B.; Aicardi, J.; Dias, K.; Ramos, O. A Progressive Syndrome of Autism, Dementia, Ataxia, and Loss of Purposeful Hand Use in Girls: Rett’s Syndrome: Report of 35 CASES. Ann. Neurol. 1983, 14, 471–479. [Google Scholar] [CrossRef] [PubMed]
- Amir, R.E.; Van den Veyver, I.B.; Wan, M.; Tran, C.Q.; Francke, U.; Zoghbi, H.Y. Rett Syndrome Is Caused by Mutations in x-Linked MECP2, ENCODING Methyl-CpG-Binding Protein 2. Nat. Genet. 1999, 23, 185–188. [Google Scholar] [CrossRef] [PubMed]
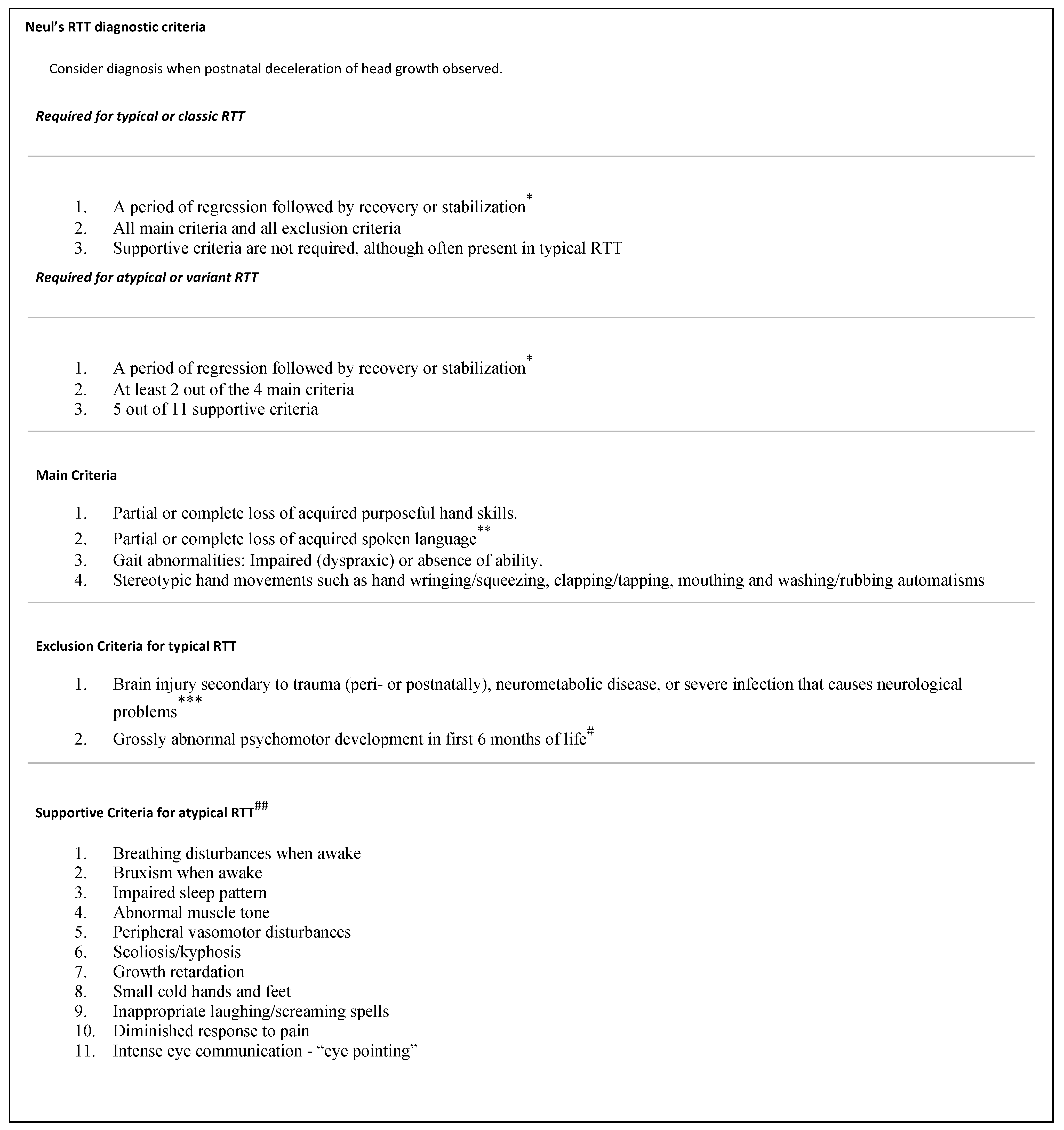
- Neul, J.L.; Kaufmann, W.E.; Glaze, D.G.; Christodoulou, J.; Clarke, A.J.; Bahi-Buisson, N.; Leonard, H.; Bailey, M.E.S.; Schanen, N.C.; Zappella, M.; et al. Rett Syndrome: Revised Diagnostic Criteria and Nomenclature. Ann. Neurol. 2010, 68, 944–950. [Google Scholar] [CrossRef]
- Haas, R.H. The History and Challenge of Rett Syndrome. J. Child Neurol. 1988, 3, S3–S5. [Google Scholar] [CrossRef]
- Huang, K.W.; Lubicky, T.J.; Hammerberg, J.P. Scoliosis in Rett Syndrome. Orthop. Rev. 1994, 23, 931–937. [Google Scholar]
- Neul, J.L.; Fang, P.; Barrish, J.; Lane, J.; Caeg, E.B.; Smith, E.O.; Zoghbi, H.; Percy, A.; Glaze, D.G. Specific Mutations IN Methyl-CpG-Binding Protein 2 Confer Different Severity in Rett Syndrome. Neurology 2008, 70, 1313–1321. [Google Scholar] [CrossRef]
- Percy, A.K.; Lane, J.B.; Childers, J.; Skinner, S.; Annese, F.; Barrish, J.; Caeg, E.; Glaze, D.G.; MacLeod, P. Rett Syndrome: North American Database. J. Child Neurol. 2007, 22, 1338–1341. [Google Scholar] [CrossRef]
- Watson, P. Angelman Syndrome Phenotype Associated with Mutations in MECP2, a Gene Encoding a Methyl Cpg Binding Protein. J. Med. Genet. 2001, 38, 224–228. [Google Scholar] [CrossRef]
- Huppke, P.; Maier, E.M.; Warnke, A.; Brendel, C.; Laccone, F.; Gärtner, J. Very Mild Cases of Rett Syndrome with Skewed X Inactivation. J. Med. Genet. 2006, 43, 814–816. [Google Scholar] [CrossRef]
- Carney, R.M.; Wolpert, C.M.; Ravan, S.A.; Shahbazian, M.; Ashley-Koch, A.; Cuccaro, M.L.; Vance, J.M.; Pericak-Vance, M.A. Identification of mecp2 Mutations in a Series of Females with Autistic Disorder. Pediatr. Neurol. 2003, 28, 205–211. [Google Scholar] [CrossRef] [PubMed]
- Collins, A.L.; Levenson, J.M.; Vilaythong, A.P.; Richman, R.; Armstrong, D.L.; Noebels, J.L.; Sweatt, J.D.; Zoghbi, H.Y. Mild Overexpression of mecp2 Causes a Progressive Neurological Disorder in Mice. Hum. Mol. Genet. 2004, 13, 2679–2689. [Google Scholar] [CrossRef] [PubMed]
- Bahi-Buisson, T.; Bienvenu, N. CDKL5-Related Disorders: From Clinical Description to Molecular Genetics. Mol. Sindonology 2012, 2, 137–152. [Google Scholar] [CrossRef]
- Neul, J.L. The Relationship of Rett Syndrome and Mecp2 Disorders to Autism. Dialogues Clin. Neurosci. 2012, 14, 253–262. [Google Scholar] [CrossRef] [PubMed]
- Florian, C.; Bahi-Buisson, N.; Bienvenu, T. Foxg1-Related Disorders: From Clinical Description to Molecular Genetics. Mol. Syndromol. 2011, 2, 153–163. [Google Scholar] [CrossRef]
- Bain, J.M.; Cho, M.T.; Telegrafi, A.; Wilson, A.; Brooks, S.; Botti, C.; Gowans, G.; Autullo, L.A.; Krishnamurthy, V.; Willing, M.C.; et al. Variants in HNRNPH2 on the X Chromosome Are Associated with a Neurodevelopmental Disorder in Females. Am. J. Hum. Genet. 2016, 99, 728–734. [Google Scholar] [CrossRef]
- Bain, J.M.; Thornburg, O.; Pan, C.; Rome-Martin, D.; Boyle, L.; Fan, X.; Devinsky, O.; Frye, R.; Hamp, S.; Keator, C.G.; et al. Detailed Clinical and Psychological Phenotype of the X-Linked HNRNPH2-Related Neurodevelopmental Disorder. Neurol. Genet. 2021, 7, 1–13. [Google Scholar] [CrossRef]
- NIH. HNRNPH2 Heterogeneous Nuclear Ribonucleoprotein H2 [Homo Sapiens (Human)]. In National Center for Biotechnology Information; U.S. National Library of Medicine: Bethesda, MD, USA, 2023. Available online: https://www.ncbi.nlm.nih.gov/gene/3188 (accessed on 31 August 2022).
- Madhok, S.; Bain, J. HNRNPH2-Related Neurodevelopmental Disorder; NCBI: Bethesda, MD, USA, 2022. Available online: https://www.ncbi.nlm.nih.gov/books/NBK584018/ (accessed on 31 August 2022).
- Peron, A.; Novara, F.; La Briola, F.; Merati, E.; Giannusa, E.; Segalini, E.; Anniballi, G.; Vignoli, A.; Ciccone, R.; Canevini, M.P. Missense Variants in the ARG206 Residue of HNRNPH2: Further Evidence of Causality and Expansion of the Phenotype. Am. J. Med. Genet. Part A 2020, 182, 823–828. [Google Scholar] [CrossRef]
- Salazar, R.; Beenders, S.; LaMarca, N.M.; Thornburg, O.; Rubin-Thompson, L.; Snow, A.; Goldman, S.; Chung, W.K.; Bain, J.M.; Rachel, S. Cross-Sectional, Quantitative Analysis of Motor Function in Females with HNRNPH2-Related Disorder. Res. Dev. Disabil. 2021, 119, 104110. [Google Scholar] [CrossRef]
- Kreienkamp, H.J.; Wagner, M.; Weigand, H.; McConkie-Rossell, A.; McDonald, M.; Keren, B.; Mignot, C.; Gauthier, J.; Soucy, J.F.; Michaud, J.L.; et al. Variant-Specific Effects Define the Phenotypic Spectrum of HNRNPH2-Associated Neurodevelopmental Disorders in Males. Hum. Genet. 2022, 141, 257–272. [Google Scholar] [CrossRef]
- Jong Kim, S. Sensory Dysfunction. In Sensory Dysfunction—An Overview; Elsevier: Amsterdam, The Netherlands, 2010; Available online: https://www.sciencedirect.com/topics/medicine-and-dentistry/sensory-dysfunction (accessed on 31 August 2022).
- D’Souza, A.D. Seizures. Rett Syndrome News. 30 April 2019. Available online: https://rettsyndromenews.com/seizures/ (accessed on 31 August 2022).
- Bozzi, Y.; Casarosa, S.; Caleo, M. Epilepsy as a Neurodevelopmental Disorder. Front. Psychiatry 2012, 3, 19. [Google Scholar] [CrossRef] [PubMed]
- Operto, F.F.; Mazza, R.; Pastorino, G.M.G.; Verrotti, A.; Coppola, G. Epilepsy and Genetic in Rett Syndrome: A Review. Brain Behav. 2019, 9, e01250. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Average age of Individuals (years) | 14.4 |
| Sex of patients | 23 females, 3 males |
| Total genotypes represented | 7 |
| Most common genotypes | p.Arg206Trp |
| Ethnicities represented | 3 |
| Ethnicities reported | Caucasian (n = 23), Hispanic (n = 2), East Asian (n = 1) |
| Phenotypes (Neul’s Major Criteria Bolded) | Proportions of Individuals with Phenotypes |
|---|---|
| Partial or complete purposeful loss of hand skills | 1/26 (4%) |
| Partial or complete loss of acquired spoken language | 5/26 (19%) |
| Gait abnormalities | 21/26 (81%) |
| Hand stereotypies | 18/26 (69%) |
| Breathing abnormalities | 5/26 (19%) |
| Bruxism while awake | 12/26 (46%) |
| Impaired sleeping patterns | 6 /25 (24%) |
| Impaired muscle tone (hypo/hypertonia) | 25/26 (96%) |
| Small, cold hands/feet | 13/26 (50%) |
| Vasomotor disturbances | 8 /26 (31%) |
| Scoliosis or kyphosis | 10/26 (38%) |
| Growth Retardation | 9 /25 (36%) |
| Inappropriate laughing/screaming spells | 15/26 (58%) |
| Diminished response to pain | 13/24 (54%) |
| “Eye pointing” | 6/26 (23%) |
| 4 main criteria | 0 |
| 3 main criteria, 5 or more supportive criteria | 4/26 (15%) |
| 3 main criteria, less than 5 supportive criteria | 1/26 (4%) |
| 2 main criteria, 5 or more supportive criteria | 8/26 (31%) |
| 2 main criteria, less than 5 supportive criteria | 5/26 (19%) |
| 1 main criteria, 5 or more supportive criteria | 2/26 (8%) |
| 1 main criteria, less than 5 supportive criteria | 2/26 (8%) |
| No main criteria, 5 or more supportive criteria | 0 |
| No main criteria, less than 5 supportive criteria | 4/26 (15%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gonzalez, J.N.; Goldman, S.; Carter, M.T.; Bain, J.M. Rett-like Phenotypes in HNRNPH2-Related Neurodevelopmental Disorder. Genes 2023, 14, 1154. https://doi.org/10.3390/genes14061154
Gonzalez JN, Goldman S, Carter MT, Bain JM. Rett-like Phenotypes in HNRNPH2-Related Neurodevelopmental Disorder. Genes. 2023; 14(6):1154. https://doi.org/10.3390/genes14061154
Chicago/Turabian StyleGonzalez, Joseph Nicho, Sylvie Goldman, Melissa T. Carter, and Jennifer M. Bain. 2023. "Rett-like Phenotypes in HNRNPH2-Related Neurodevelopmental Disorder" Genes 14, no. 6: 1154. https://doi.org/10.3390/genes14061154
APA StyleGonzalez, J. N., Goldman, S., Carter, M. T., & Bain, J. M. (2023). Rett-like Phenotypes in HNRNPH2-Related Neurodevelopmental Disorder. Genes, 14(6), 1154. https://doi.org/10.3390/genes14061154