3. Results
The results of the present study, part of a PhD dissertation [
69], can be grouped into five subsections:
Mean values of physical parameters;
Mean values of airtightness of the samples;
Mean values of occupants’ votes;
Mean values of occupants’ clothing insulation; or
Mean values of occupants’ symptoms and related health effects.
These values were analyzed according to seasons (winter, W, and midseasons, MS) and windows’ and doors’ operation (open windows, OW, closed windows, CW, open door, OD). In this way, 26 classrooms (55% of the case studies) had the windows closed during the measurement period, with 23 of these during the winter session, and 21 had the windows open (45% of the case studies), with 11 of them during the winter period. No intervention by the researchers was made to modify classroom-state, allowing us to gather operational actual conditions.
3.1. Mean Values of Physical Parameters
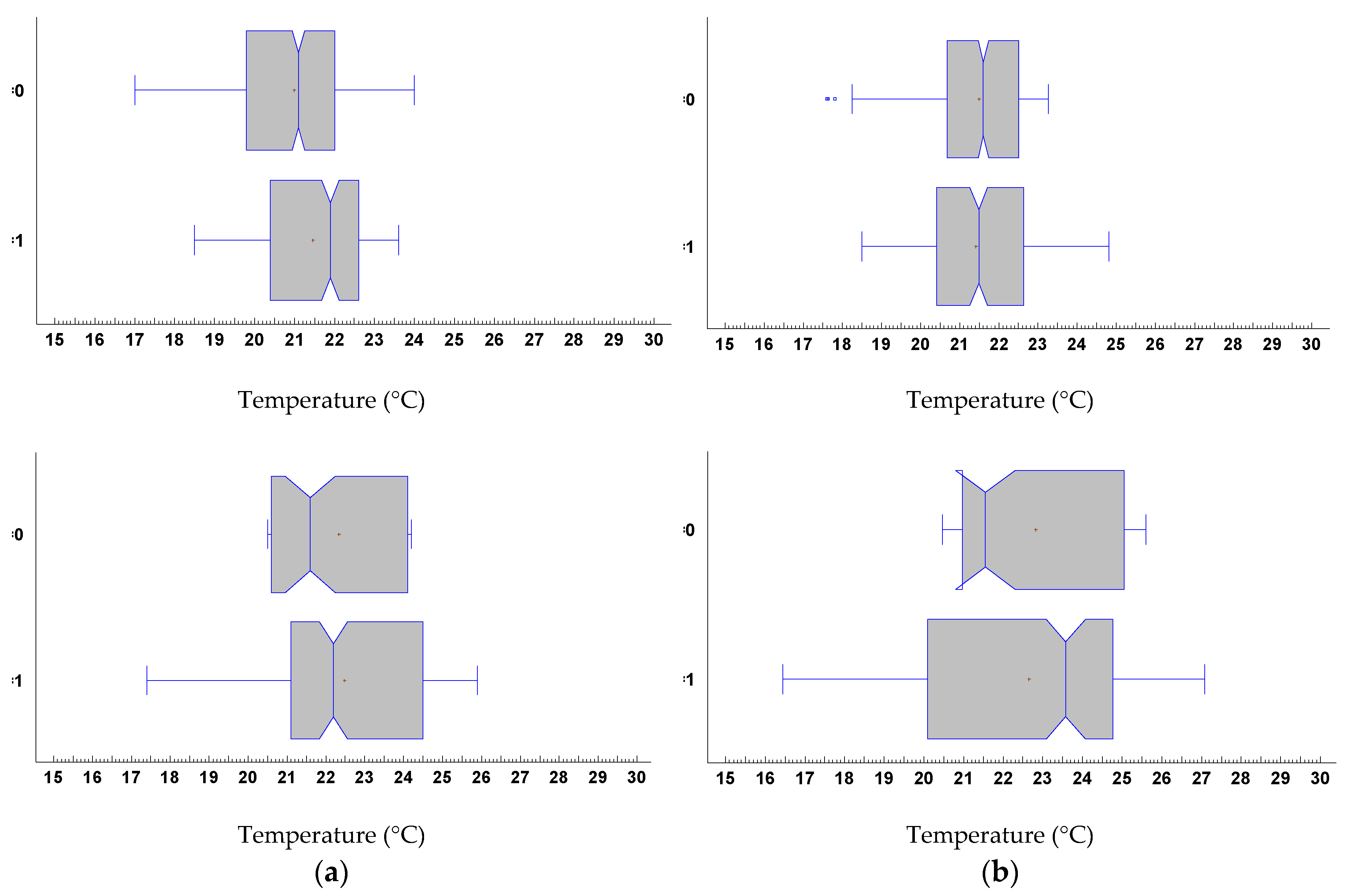
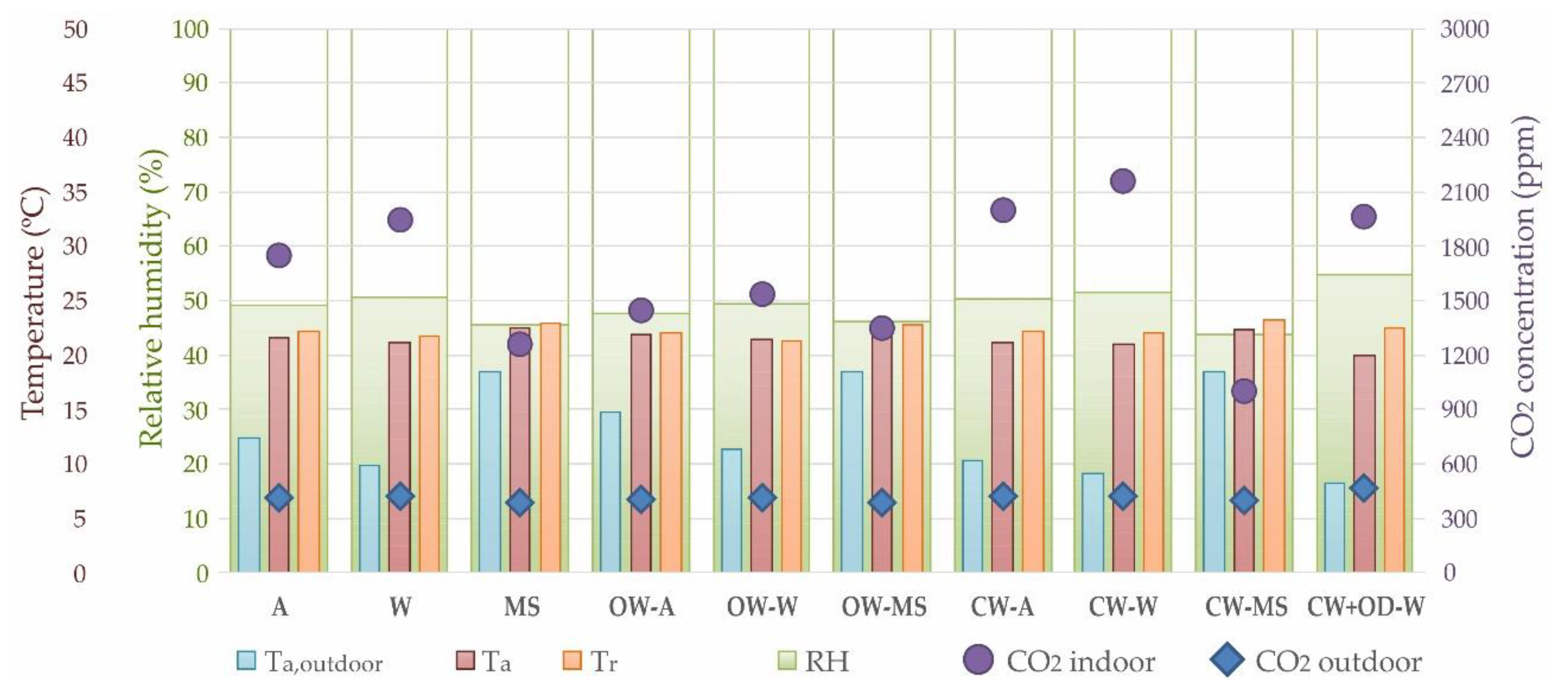
The measured interior air temperature (Ta) ranged between 17.8 and 22.7 °C during winter season (
Table 5), with the lowest mean temperature values obtained for the case studies with closed windows, especially when inner doors were open, with values of 20 °C. It can be related with the outdoor conditions, given that the lowest outdoor temperature values (Ta, outdoor) were measured for classrooms with closed windows and open inner doors. In addition, 8 of the case studies had the windows open during winter, which can mean that there was a bad regulation of the heating system and the heat excess had to be dissipated, or that the students considered that they had to ventilate the classroom due to a poor environment perception. Indoor air temperature in midseasons was oscillating around 22.4 °C, without a direct relation with window operation. Although winter time temperature expectations range between near 20–22 °C to 20.4–22.6 °C if windows are open (central quartile lower and upper values), this band nearly doubles in middle season, when temperatures from 20.6 to 24 °C may be expected (21.1 to 24.5 °C if windows are open). A quartile distribution plot for indoor thermal parameters, air temperature, and operative temperature is proposed in
Figure 4. It is noteworthy to highlight that there was a statistical significance between seasons in a windows-state with independent behavior aspect that was verified through test of comparison of samples, F-test for the variance and a K-S (Kolmogórov-Smirnov) for the distributions of probability with
p-values under 0.05 in all the cases.
Although average values of mean radiant temperature (
) were within the recommended operating temperature ranges for classrooms according to ISO 7730 standard [
23] (22.0 ± 2.0 °C for category B), there was a high dispersion of figures with a standard deviation (SD) between 1.7 °C in winter with closed windows and 3.7 °C in midseasons with open windows, which was due to the operation of HW radiator system, especially when windows were open, with
values of 27.2–28.0 °C with radiators on and values of 17.5–19.0 °C when radiators were turned off. This caused operative temperature to swing usually between 20 and 25 (central quartiles) during middle season, with typical values of 20.6 to 22.5 °C during winter, with a very similar band of 20.4 to 22.6 °C if windows were open, highlighting the effect of surface thermal control performed by the radiator heating system.
Relative humidity (RH) in winter was always over 40%, with a maximum value of 64% in the case of one of the classrooms with windows closed and inner doors opened. In midseasons, relative humidity was lower but with a higher oscillation, with a minimum value of 29%.
Air velocity (V
a) values were oscillating under 0.05 m/s, both in winter and midseasons, only exceeding the recommended design limit for comfort category B established by the ISO 7730 standard [
23] of 0.16 m/s in one of the case studies with open windows, with a value of 0.18 m/s. In the case of closed windows, air velocity was always under 0.09 m/s. This showed poor air movement and limited air displacement potential.
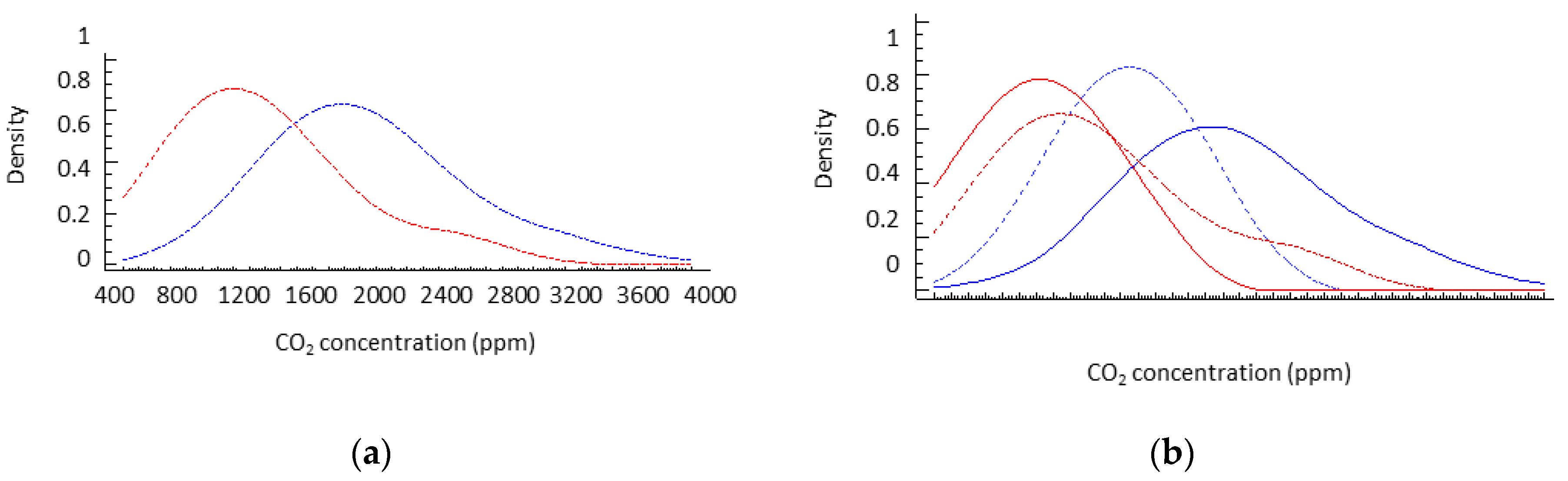
Measurements of the CO
2 concentration usually show figures well above typical thresholds (
Figure 5). The World Health Organization (WHO) recommends a limit for healthy indoor spaces of 1000 ppm [
70]. In this way, the probability distribution derived from the measures showed that more than 92% of the distribution for closed windows was above this limit, while this only decreased to 88% of the time when windows were open. In addition, 47.5% of classrooms with windows closed exceeded the 2000 ppm threshold. The greatest relative effect of window operation was seen in the winter, when CO
2 concentration can be decreased by 25%, comparing median values. However, figures were above desirable levels, indicating the lack of capacity of the window operation to solve a suitable ventilation. In general, during the intermediate season, the operation of the windows did not provide a significant improvement of indoor air quality, which may be related to the lack of thermal differential between indoor and outdoor air, limiting the air exchange due to the absence of a thermodynamic effect (
Figure 6).
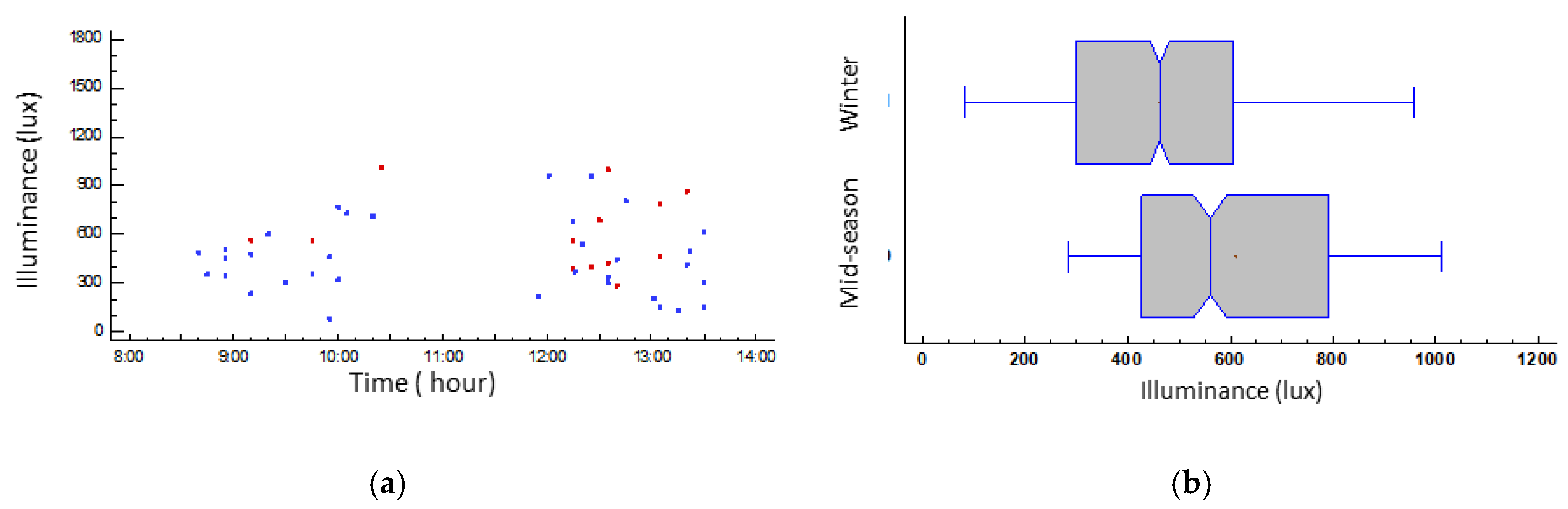
The median room mean illuminance (E) in the case studies oscillated between 461 and 560 lx (both cases with a SD of 222) according to the season, with an average lighting uniformity (U
o) of 0.48. However, although there seemed to be a greater illumination associated with the half-season period, it was not possible to rule out, without further measurements, the fact of being biased by the activities in execution during the measurements. The high SD was due both to the use of the projector and the solar protection devices (as low as 15 lx) and the lack of use of a solar protection device with direct solar radiation (figures as high as 1710 lx) (
Figure 7). The homogeneity of the lighting solutions in almost all buildings generated visual fields with very similar characteristics, mainly dominated by the behavior of their electric lighting. The correlated color temperature was similar in all cases, varying from 3500 to 5500 K; hence, it can be considered that both the amount of light and hue did not affect the thermal perception of the participants, as exposed by Bellia et al. [
71] and Acosta et al. [
72].
3.2. Mean Values of Airtightness of the Samples
The values of airtightness of the classrooms under study with a difference of pressure between indoor and outdoor of 50 Pa (n50 range) varied from 2.6 h–1 to 10 h–1, with an average value of n50 of 6.97 h–1 and a SD of 2.06 h–1.
3.3. Mean Values of Occupants’ Votes
The mean thermal sensation vote (TSV) of the students in both seasons was “slightly warm”, with a value of +0.32 on the ASHRAE scale in winter and +0.38 in midseasons, having a SD of between 0.93 and 0.83, respectively. This can be identified as a common situation among poorly ventilated and crowded spaces. Even with open windows the actual air-removal capacity looked very limited as previously evaluated (
Table 6). These thermal perceptions were higher (+0.10 points) when windows were open, highlighting an excess of heat release of the heating system due to inefficient regulation and the wish of the users of dissipation. In this case, the occupants’ thermal preference vote (TPV) expressed was softer and closer to neutrality than the TSV, not fitting at all with the perceived thermal sensations (R² = −0.47, moderate correlation), as showed by Teli et al. [
14,
53].
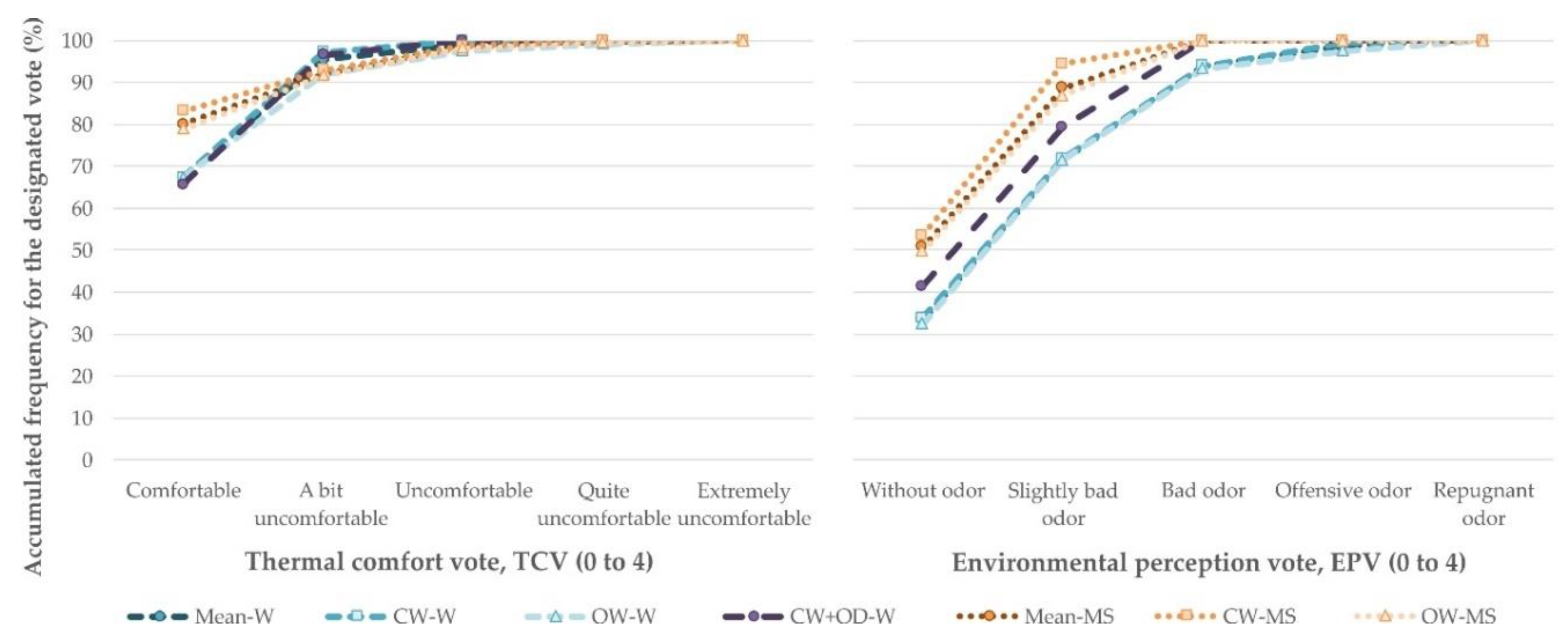
The average thermal environment rejection percentage (PD
acc) expressed by students, based on a scale from 1 (acceptance) to 0 (rejection), was low and homogeneous in both seasons, with a mean value of 0.81 in winter conditions and 0.85 for midseasons. In addition, thermal acceptance was, in general, slightly better in classrooms with closed windows in both seasons, but in the case of closed windows and open doors. The thermal comfort vote (TCV) allowed us to qualify this acceptance-rejection PD
acc index, given that less than 70% of students found “comfortable” the thermal environment in winter conditions compared to more than 80% in midseasons. This percentage increased to 96% for students with “comfortable” or “a bit uncomfortable” votes in winter conditions, but without reaching 92% in midseasons. By contrast, the number of users who, accepting a slight discomfort, considered the acceptable environment was superior in winter than in midseason, where the feeling of discomfort was slightly more marked, can be seen in
Figure 8.
The mean environmental perception vote (EPV) showed during winter a 1.03 value (slightly bad odor), with low differences regarding windows’ operation (less than 0.03 points); in midseasons, EPV was more favorable (0.61), with more than 0.10 points of difference regarding windows’ operation.
Figure 8 also shows the accumulated distribution of the EPV, in which less than 35% of students voted “without odor” in winter, while more than 50% voted it during midseasons. In addition, almost 30% of students perceived a slight odor or worse in winter in comparison to the midseasons, with 10%. Finally, around 7% of students voted “bad odor” or worse in winter, while there were no votes in this way during midseasons.
During the winter there is a more evident feeling of a poorly ventilated (not healthy) environment, in line with the measured CO2 values acting as a token of the indoor ambient renovation state. The operation of windows produced little to no effect on the improvement of the environmental quality, especially during the winter. Although it was found that the opening of windows in this period generated noticeable dilution of the interior atmosphere, it was still insufficient to guarantee pleasant environments.
During midseason, although the ventilation mechanism was less effective (by means of a lack of thermal differential), the capability of diluting the indoor environment to threshold levels was perceived by the users as somewhat better. The assessment of these user perception-thresholds was a key aspect of research, since it will allow the design of more adequate and well-accepted spaces.
3.4. Mean Values of Occupants’ Clothing Insulation
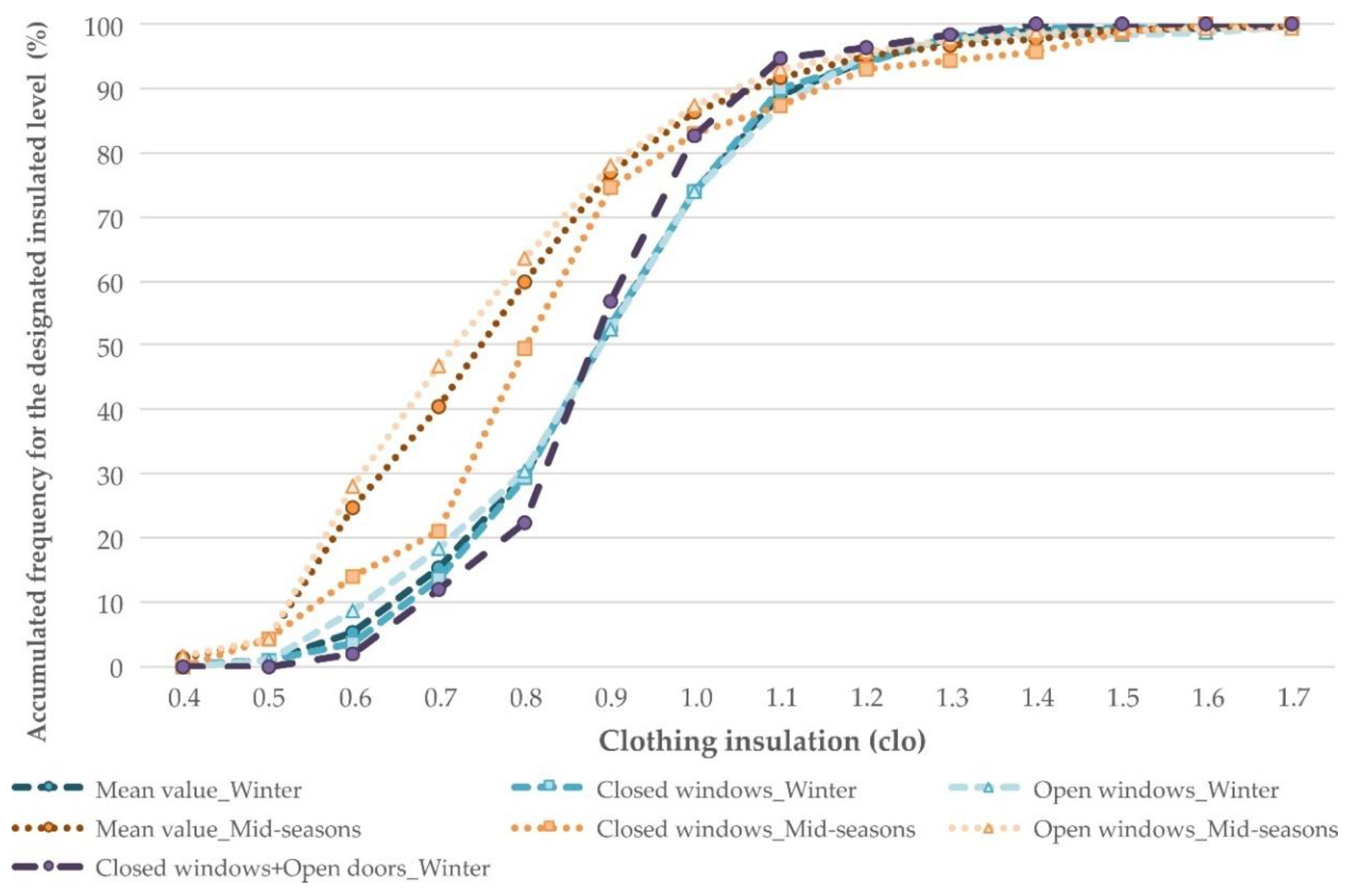
The occupants’ clothing insulation (I
cl) showed two models of response linked to the season, as it can be seen in
Table 7. Clothing distribution in winter was homogeneous, with a mean value of 0.90 clo and a SD of 0.19, common both for open and closed windows, and a minor divergence of 5% around 0.6–0.7 clo values related to windows’ operation, showed in
Figure 9. It should also be noted that the biggest slope of the insulation distribution was during winter with closed windows and inner doors open, which highlighted the smaller variation in clothing insulation of this group of case studies.
In midseasons, the clothing insulation was lower and variable, with a SD of 0.23 and an asymmetrical distribution. There was a divergence of up to 25% in the frequency of the lowest levels of clothing insulation during midseasons regarding the windows’ operation, coinciding both frequencies around the value of 0.90 clo (75–80% of the accumulated frequency).
3.5. Symptoms and Related Health Effects
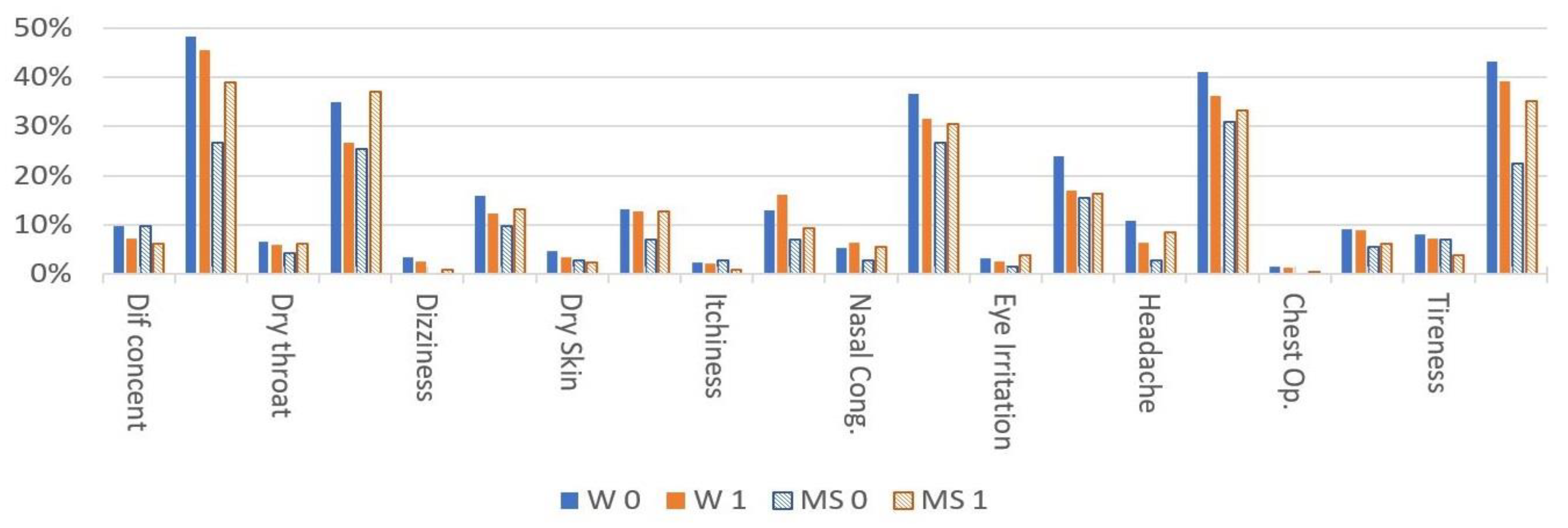
The most commonly reported severe symptoms were headache and concentration difficulty (around 10%), followed by tiredness and a dry throat (under 10%), with a greater prevalence during wintertime and closed windows’ operation. The action of the windows (
Figure 10) was relatively weak, indicating the limited actual ventilation capacity of these spaces with only the opening of windows (reductions were around 25% less, in general). However, the perception of mild symptoms was very common in the classrooms, with tiredness, headache, and difficulty in concentration presenting a prevalence in the range of 40% to 50% for closed operation and slightly lower when windows were open (decreasing around 10–15 %), as shown
Table 8.
This situation changed in midseason, where the symptom report was lower, even for the situation of closed windows. However, unlike winter, symptomatic perception increased when the windows were open for both perceptions, severe and mild, especially for dry throat, itchiness, nasal congestion, and headache, which are symptoms that can be linked to the penetration of external species (in many cases aerobiological such as pollen [
73,
74,
75]).
Aiming to evaluate the overall impact of the different perceptions of symptoms, while assuming the variability component of the subjective responses and different individual sensitivity to the environments, unlike the evaluation of physical parameters, users were asked to assess the intensity of the perception of discomfort on a scale of 0 to 1 (0 none and 1 maximum intensity). Although this was not a standardized parameter (it may vary between different users) it had a great potential to represent the importance that each user assigned to the nuisance and, therefore, to assess the actual perception of the indoor conditions. Similar subjective ratings in conjunction with objective environmental measures were used in relevant studies, such as [
76,
77,
78,
79]. An overall indicator was collected through the addition of the specific scores or valuations generated by the users of each symptom or condition. This represented a global assessment of perceived impact, with a fundamentally qualitative character, since there was no univocal relationship but strong enough to highlight health discomfort ant to categorize best and worse indoor environments. The main values from the different classrooms are grouped by seasons and windows’ situation in
Table 9. This table contains the statistical summary for the data samples. Of particular interest are standardized bias and standardized kurtosis since, in all the cases (except the kurtosis of MS_1) these statistics were outside the range of −2 to +2 standard deviation, thus indicating significant deviations from normal.
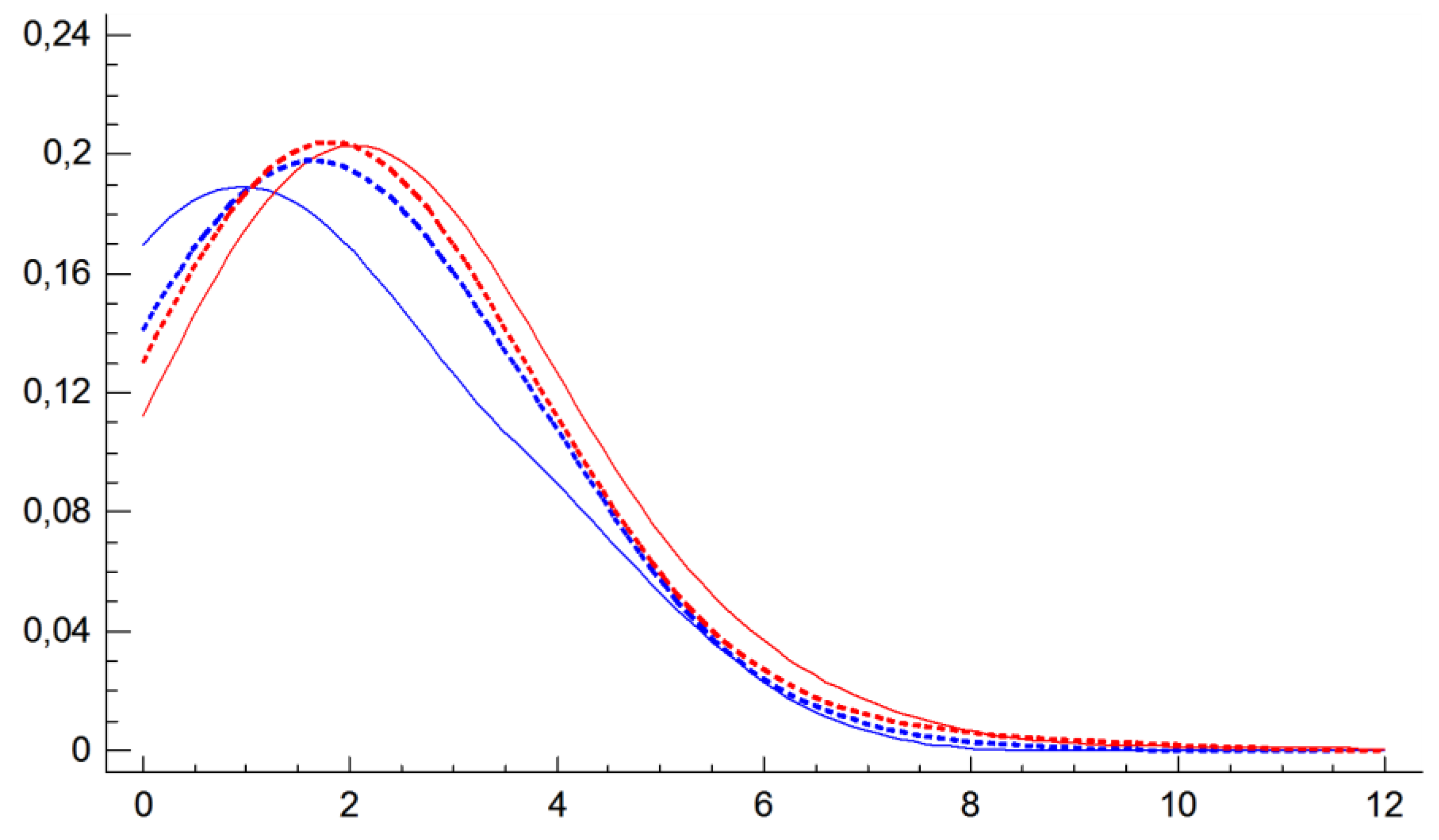
The distribution of symptoms’ samples for each scenario (
Figure 11) was asymmetrical, not normal (Shapiro–Wilk test with
p-value less than 0.05 in all cases, so it can be ruled out with 95% confidence) with bias. Median values located between 1.4 as the lower impact case in half a season (closed windows) up to 2.10 for winter (also with closed windows). Although values concentrated around 2.00, there was a significant dispersion, reaching values of up to 11, which meant a maximum vote in practically all the symptoms. (This specific case must be understood as outlier). This highlighted that even in the best scenario analyzed, there was a significant perception of ambient-related symptoms and problems by the users. By contrast, there was also a non-negligible presence of users that did not reflect any discomfort or effects, especially in the midseason scenario with closed windows, with percentiles that stood at 39%, compared to lower values in the other states, where this group went from 6.1% to 16.4% (W0 to MS1). In this way, the low level of difference in the distribution according to windows’ operation can also show that the ventilation airflow through windows was not enough to guarantee a noticeable reduction of the students’ symptoms, although it can modify slightly the physical parameters of the interior environment. This aspect was of singular importance, since it indicated that the mere control of the usual environmental values did not guarantee satisfaction with the interior environment, at least with regard to the absence of bothersome symptoms. In the case of midseason, symptoms described with open windows can be due to the higher level of external aerobiological particles entering into the classrooms, such as pollen. That is why the appropriate ventilation to provide a perceptive reduction of the symptomatology should be done by means of fans with filter system.
The probabilistic distributions of individual related symptoms’ scores for the different scenarios showed some similarity in the global pattern response and central values, mainly for open windows, except for the MS_0 (closed windows). A set nonparametric contrast through K–S test (Kolmogorov–Smirnov for the global parameter) was developed to evaluate the pertinence to a common distribution. In all four cases, comparisons for accumulated distances of the samples showed statistically significant differences at 95% significance between the distributions (with all the cases with a p-value < 0.05 and DN values over Dcrit.0.05), with DN around 0.122 to 0.148 for the samples with closest distribution (windows open winter vs. middle season and winter open vs. closed windows) and the greater DN value 0.380 for the furthest. So it can be established that there were different distributions for all the cases
3.6. Airtightness
The average value of the infiltration rate at 50 Pa (n
50) was 6.97 h
−1, with a standard deviation of 2.06 h
−1. Models with the lowest n
50 values were those in the C3 climate zone, where the lowest average temperature values are recorded in the winter. The values of n
50 ranged from 10 h
−1 (maximum) to 2.6 h
−1 (minimum), both recorded in the B4 climate zone (
Table 10).
4. Discussion
This section is focused on the analysis of the relationships between the symptoms described by occupants and the rest of the parameters under study (physical, building operation, and votes).
4.1. Relationship between Physical Parameters and Classroom Operation
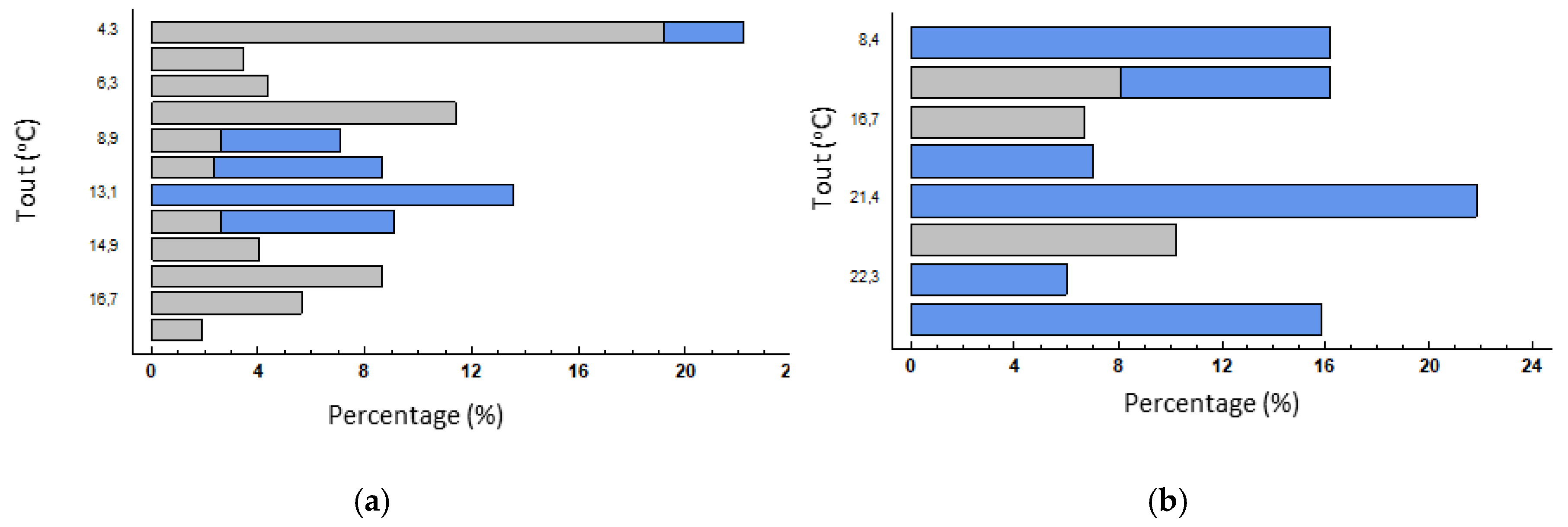
It could be assumed that manual opening of windows in naturally ventilated buildings should depend on outdoor conditions, as this is the main element of control. However, it was observed that, despite the fact that in midseason windows remain open longer than in winter, no clear linear trend can be observed. In winter, the need for ventilation or indoor air changes is considered more important than the need to control the entry of outdoor cold air. Analysis by categories of the opening of windows (
Figure 12) showed this occurs mostly in mid temperatures, although it was also observed in cooler conditions when necessary. Furthermore, no progressive growth was observed with the increased temperature, as could be expected. In midseason, it is more common to open windows, although there was no clear correlation with temperature, some of which was similar to winter, where more windows are opened in comparison.
It could be deduced that users are psychologically or culturally conditioned to some extent as to how and when they open windows. Although it would be preferable for the classroom windows to remain open, the act of opening was seen as a reaction to poorer indoor air quality, which was more noticeable for the same thermal conditions in spring. It, therefore, appears that there is an adaptation process.
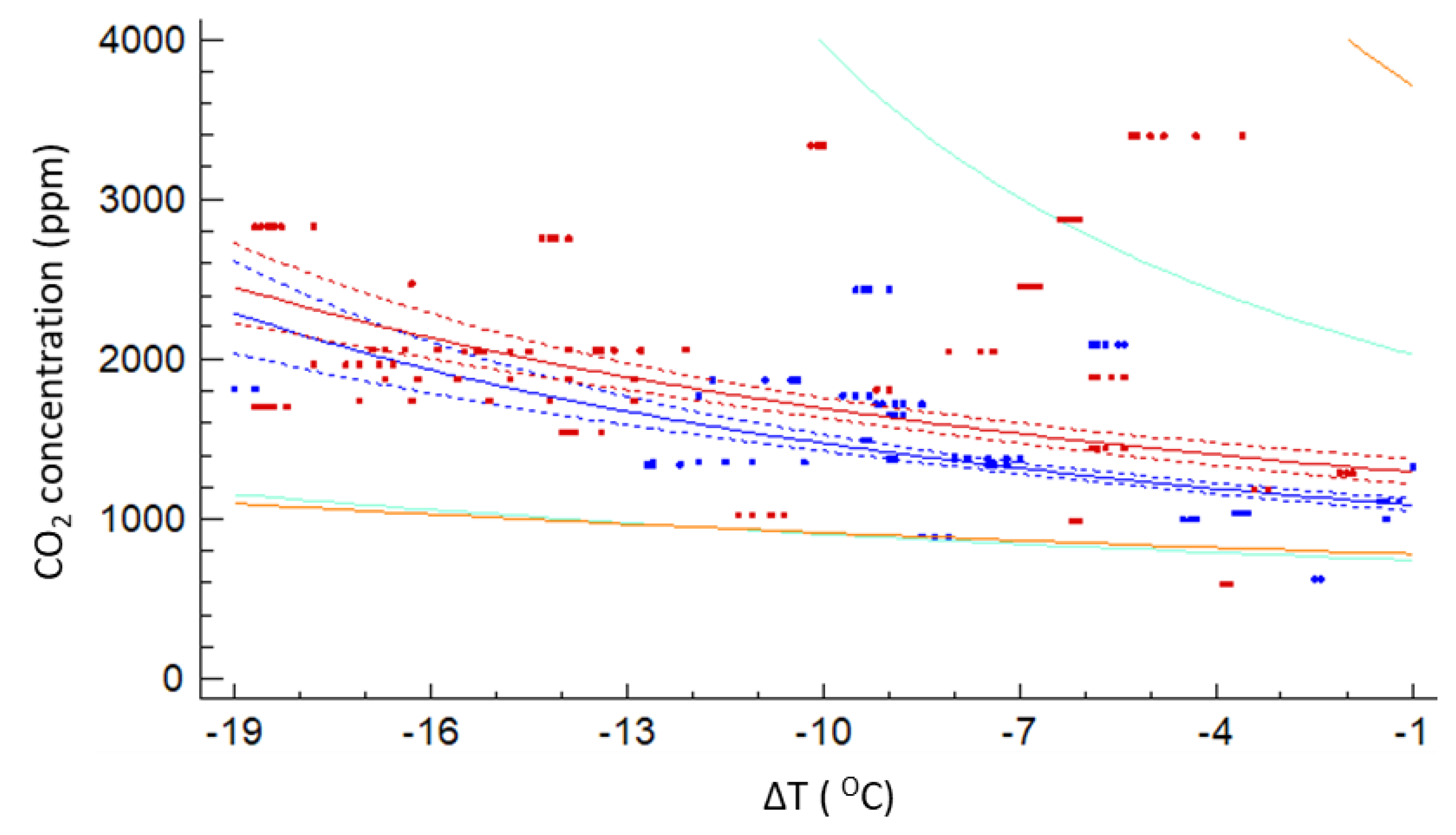
As it can be seen in
Figure 13, although there was statistical significance between the CO
2 concentration and the outdoor-indoor air temperature differential (
p-value < 0.05), the correlation was somehow weak and more clear in winter time (R
2 = 0.249) than in midseason (R
2 = 0.145), with a better fit to a y-reciprocal relation. However, the predictive mathematical model lacked enough accuracy to be of utility to forecast actual situations. Besides the wide dispersion on values, there was a trend in the worsening of the indoor environment as DT increased, as can be usually expected, due to the lack of a controlled ventilation system.
Is noteworthy to highlight that moderate DT winter and midseason trends were very similar, which matched with the foreseen windows’ operation patterns, when most of the apertures occurred around cold-mild external temperatures.
4.2. Relationship between Physical Parameters and Symptoms Described
Some symptoms were more predominant when outdoor temperature was lower, although no clear linear relationship could be established. These symptoms were more frequent in winter when the thermal differential is at its highest, usually linked to a lack of ventilation at the time, as supported by the high CO2 indices as a general air quality indicator.
Although the symptoms often appeared to be more evident when the windows were open, this should be seen as a consequence, not a cause, as user perception of the symptoms was generally clearer when opening the windows. This is interesting to note, as it could be due to a situation which exceeded the perception threshold. In the winter, it is more common to observe symptoms such as difficulty concentrating, dry throat, and tiredness. These are very closely linked to poor hygrothermal control, even with windows open, where temperature and relative humidity are far more important, especially with open windows, as well as increased indoor CO2 linked to poor ventilation. In contrast, itchiness and chest tightness were barely noticeable.
The situation changed in midseason and symptoms, such as difficulty concentrating, tiredness, and nasal congestion, were less widely reported. However, symptoms less connected with the absence of hygrothermal regulation increased, while there was a greater presence of symptoms that may be linked to outdoor exposure.
When both lighting parameters, illuminance (E) and illuminance uniformity (Uo), were analyzed and referred to symptomatology, no clear correlation was obtained, as other previous studies showed for educational buildings [
80]. This may be because illuminance values in the classrooms under study were generally over 350–400 lx with a uniformity of 0.40–0.50, so they were values good enough to not influence students at a symptomatic level.
The infiltration rate (n50) and the symptoms related by occupants showed a very tenuous connection, with some weak trends in the case of tiredness, as well as difficulty on concentrating, dry throat, and headache. Given that the airtightness of the classrooms was, in general, adequate or even good, with an average value of 6.97 h−1 with a maximum value of 10 h−1, its influence can be moderate due to its low impact on air renewal. It also indicates that other variables, like time spent inside the classroom or windows’ and doors’ operation, can have more importance than the airtightness of the room.
There was no clear linear correlation between the students’ clothing insulation and the symptoms described during measurements. The possibility of freely varying the level of clothing insulation by the students, according to their individual thermal needs, may be a factor that influenced this lack of relationship between clothing and symptomatology, besides psychological factors linked to clothing.
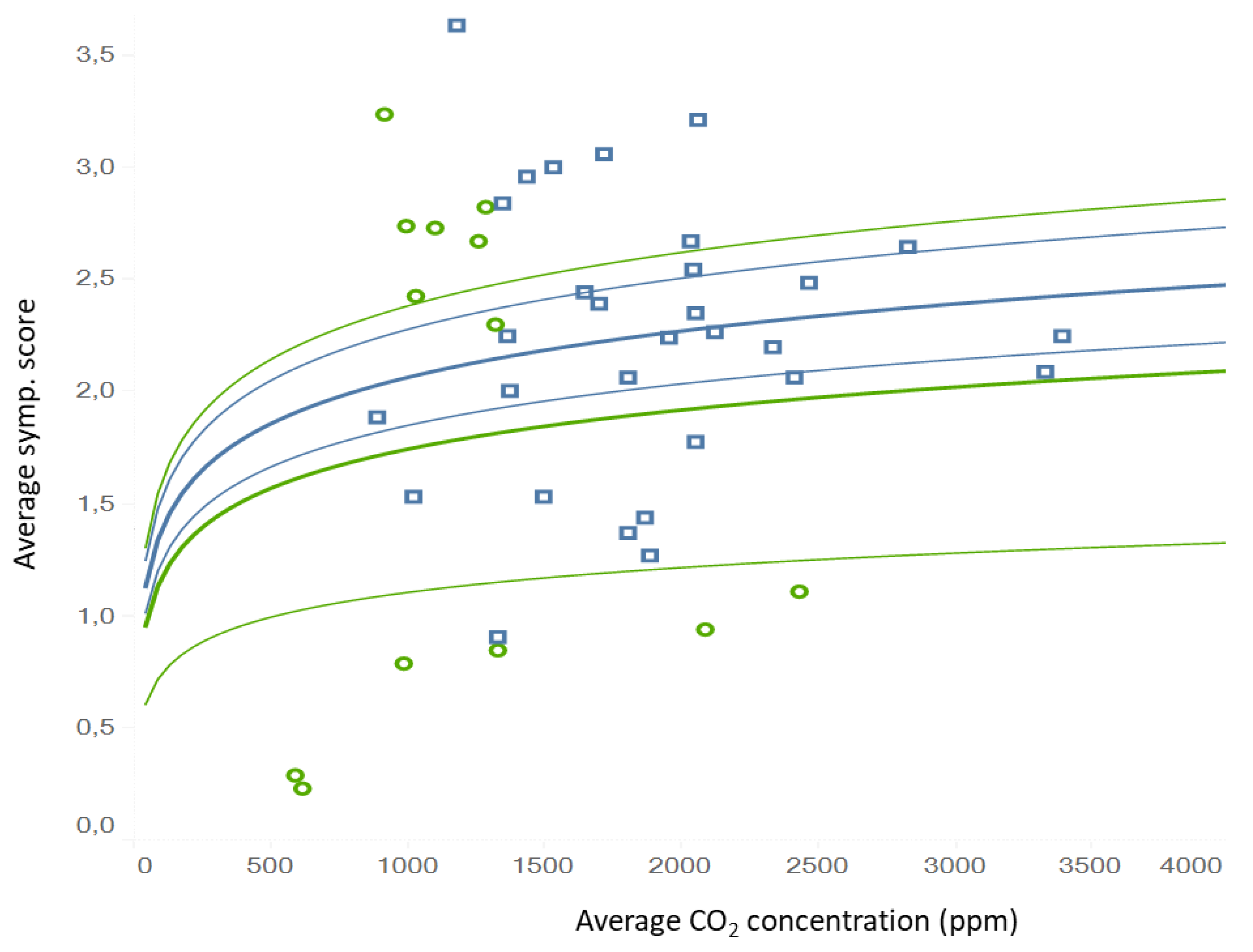
When symptomatology was assessed as global, there were some trends that could be identified. If CO
2 was assumed as an overall indicator of indoor air renovation (not as a contaminant itself), the worsening of indoor environment linked with the increase of symptoms related. It can be approximated to a logarithmic regression relation (
Figure 14), although a wide spread of values must be assumed. Different patterns for winter and midseason were described due to adaptation of users and the influence of outdoor species. Although this model presents some uncertainty for its use as a prediction tool, it does have the capacity to act as a qualitative indicator.
A linear trend model was calculated for the average symptom score and given a record of the average indoor CO2 (logarithmic fit). The model was statistically significant at p < 0.05, having a high correlation coefficient (R2 = 0.8833) and a mean square error (MSE) of 0.6160.
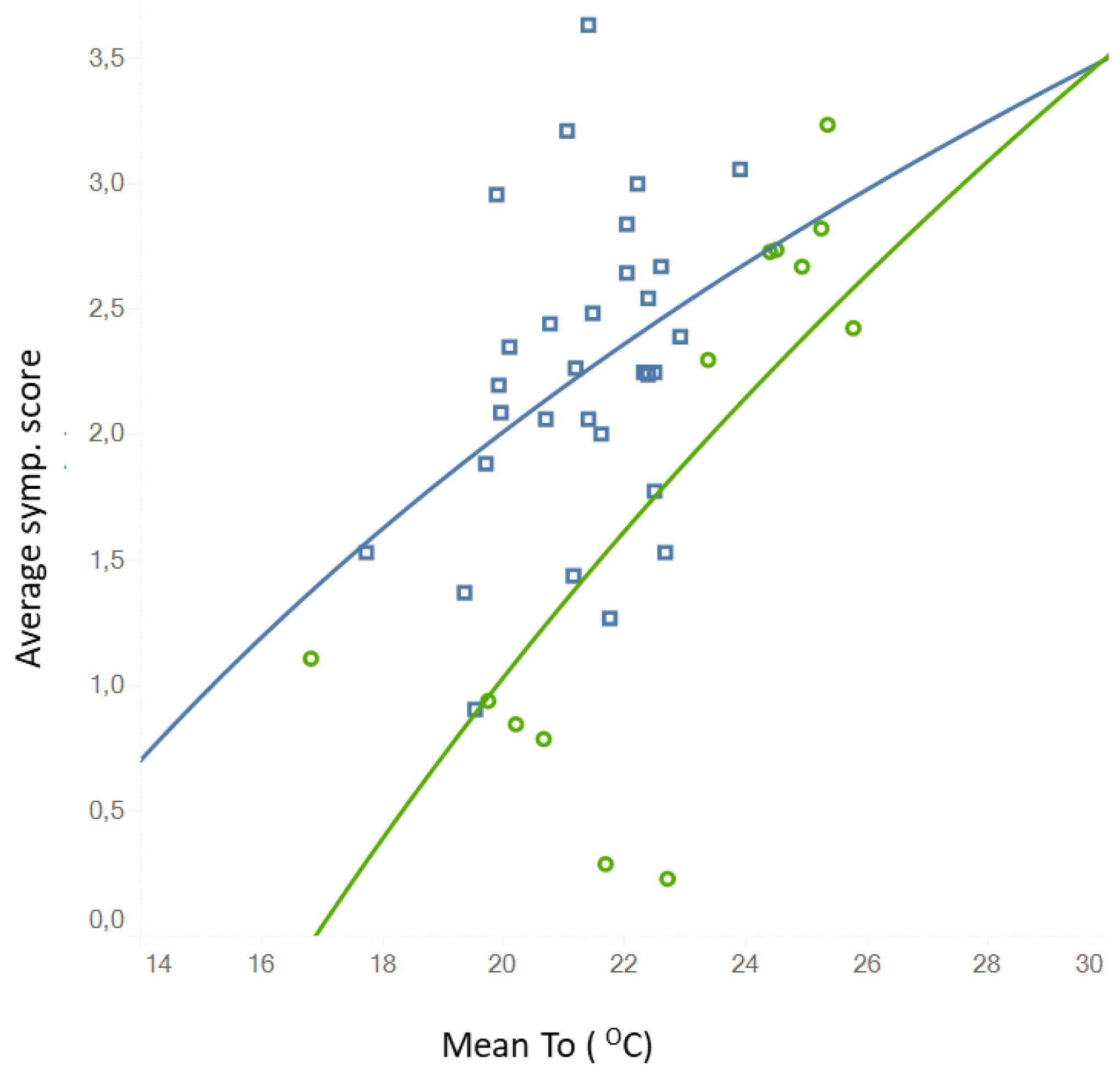
A somewhat weaker linear relationship (logarithmic fit also) was seen (R² = 0.509 for midseason and R² = 0.143 for winter) but with statistical signification (
p-value < 0.05 in both cases) and an error of MSE 0.425. Although dispersion was high, it was also a useful qualitative trend indicator, and was found between the overall perception of symptoms and the indoor operative temperature (
Figure 15). In this case, it can be established that the symptoms tended to be more frequent when indoor temperatures increased, also with specific patterns for winter and middle season.
5. Conclusions
A wide study sample of 47 naturally ventilated multipurpose classrooms of the most representative climate zones of southern Spain was characterized and analyzed through field measurements and surveys distributions, in order to contrast environmental sensation votes, perception, and indoor-related symptoms described by 977 students during lessons with physical and environmental parameters, as well as operational scenarios.
The main operational case to be analyzed, according to votes and symptoms, was the windows’ operation. In this sense, the 61% of the case studies during winter season had the windows open, which can be related both to a bad regulation of the heating system (the slight heat excess had to be dissipated) as well as to a poor indoor environment perception. In this way, the case studies with open windows in winter had a higher mean indoor air temperature value (21.5 °C versus 21.0 °C) and higher standard deviation of the mean radiant temperature (2.6 °C versus 1.6 °C). The mean thermal perception of students in winter season with open windows reinforced this slight heat excess, given that it was in a comfort range but 0.15 points warmer than in the case of closed windows, also expressing a thermal preference of thermal neutrality-mild cold (−0.06 on the ASHRAE scale) with open windows in contrast to the preference for a warmer environment when the windows were closed (+0.13). The thermal assessment of the environment through the thermal comfort vote (TCV) also had a poorer value with open windows (−0.44 versus −0.35 from 0 to −4), also showing a higher deviation in the votes (0.75 versus 0.54) and a somewhat higher linear correlation with CO2 concentration. Therefore, the architectural design should take into account to guarantee the air quality of the venue, as well as a comfortable heating system, in order to lead students to not open the windows uncontrollably, which produces, as explained above, a noticeable energy consumption and distorts interior comfort control.
The operation of windows during winter helps to decrease the mean value of CO2 concentration, with 1537 ppm versus 2164 ppm with windows closed; but, in most of cases, this decrease was insufficient both to be within the standard recommendations for healthy environments and to reach threshold values of perceptions of the users. Given that the mean CO2 concentration level was still high even when windows were open, the mean environmental perception of the students (EPV) was not strongly influenced by the opening of windows, with almost 30% of students expressing a certain level of annoying odor in both cases, but also having a moderate correlation between poor environment perception and CO2 concentration just when windows were closed. Therefore, it can be stated that there was not a high correlation between the CO2 value and the students’ perceptions, mainly due to the olfactory adaptation phenomenon, irrespective of the need to provide a suitable air quality for healthiness purpose. In this way, when symptoms reported were added to this analysis, they presented a not-direct relationship with EPV, with the higher complaint values when windows were open. This odor perception was also somehow related with tiredness, difficulty on concentrating, eye irritation, headache, and dry throat.
In midseasons, windows’ operation led to a greater variation of indoor thermal values, both air and radiant, also maintaining in general CO2 levels over the WHO recommendations (mean vale of 1537 ppm). In addition, students’ TSVs were higher with open windows, close to the thermal comfort limit by warmth. Furthermore, the odor perception (EPV) was also poorer (0.63 value versus 0.52) when windows were open in midseasons, reinforcing the finding that windows alone are not able to provide an adequate renewal capacity for the indoor environment.
The study of the symptoms reported during measurements showed that they were largely expressed by students, both for windows open and closed, particularly in the case of difficulty of concentrating (52%), headache and tiredness (46%), followed by dry throat and nasal congestion (39%), which also were the symptoms most frequently combined with the other symptoms. According to the studied scenario, without a mechanically controlled ventilation system, complaints were more often found during winter, especially when windows were closed. In midseason conditions, symptoms were somewhat less common, but students expressed more acute symptomatology when windows were open, especially for dry throat, itchiness, nasal congestion, and headache, which are symptoms that can be related to hypersensitivity to external agents such as allergies and other respiratory conditions. This conclusion states the clear need to provide a ventilation system with a suitable filtering.
Regarding the relationship with indoor temperature, it can also be established that the symptoms tended to be more frequent when indoor temperatures increased, also with specific patterns for winter and middle season, also related to the occupants’ thermal perceptions.
Other operation factors, like illuminance and illuminance uniformity, as well as students’ clothing insulation, were analyzed referred to this symptomatology, but no clear correlation was obtained. In the case of lighting parameters, almost all the classrooms under study were generally over 350–400 lx with a uniformity of 0.40–0.50, so they were values good enough to not influence students at a symptomatic level. The correlated color temperature was similar in all cases, varying from 3500 to 5500 K; hence, it can be considered that both the amount of light and hue did not affect the thermal perception of the participants. On the other hand, students had the possibility of freely varying the level of clothing insulation, according to their individual thermal needs, so its impact on symptomatology was diminished.
In conclusion, the findings of this study show that effectively controlled ventilation systems are needed to assure an actual indoor ambient renovation and clean air supply. The special sensibility to external species make it advisable to incorporate filtering and cleaning systems for outdoor air beyond the impact on investment costs and energy use that this may entail. In addition, the study of symptomatology suggests that CO2 indicator should be complemented by other pollutants’ measurements to assure a proper interpretation of data, given that they could not be correctly identified exclusively using this single CO2 control parameter. As explained above, CO2 levels have a fuzzy influence in the students’ symptomatology; hence, the air quality should be complementarily assessed through other parameters, such as particle or VOCs’ levels.
The following points can be established as key aspects:
The use of CO2 as a standalone indicator of environmental quality, especially for the management of ventilation systems or driving the windows’ opening, may be insufficient and can derivate in situations of increased user discomfort, alongside thermal-ambient disturbance. Although there was evidence that there is a relationship with the indoor CO2 levels growing (assumed as general index) and the increase in reported global symptoms, this was not a direct link and tended to be asymptotic from certain threshold levels (around 2000 ppm).
In most cases, natural ventilation systems are not able to solve properly the removal of pollutants, generating situations with high rates of complaints even when windows are open, although they can mitigate the situations during indoor peak situations (such as produced in winter season). In many cases, windows’ opening can be counterproductive, given that, although the classic indicators of the indoor environment valuation improve, the perception of the users was negative or, at least, worse than in situations with closed windows.
Assuming that indoor ambient is a complex and multifactor model, in the current state of the art of school buildings, the use of natural ventilation by itself (with the typical configuration of classrooms and enclosures of the buildings in the region) does not guarantee adequate control of the indoor environment, against popular assumption in the area, both by users and administrators. This aspect, although it was previously included in the text, has been emphasized.
This fact may be related to the need to review the classic indicators and parameters commonly used in the environmental management of these spaces. This research found situations of discomfort even within the ranges generally assumed as comfortable by the standards and design guides. Thus, it is necessary to develop complementary indicators based on the perception and the probability of developing symptoms that allow contributing to the correct valorization of the indoor environments from the users’ points of view.
In this way, this analysis should also be complemented with corresponding measurements and surveys distributions in classrooms with mechanical ventilation systems in order to develop a comparison of results with adequate CO2 levels, so further research on this field is required.

 ,
, 



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}














