
The Thermal Environment of Housing and Its Implications for the Health of Older People in South Australia: A Mixed-Methods Study

 ,
,  , , , , ,
, , , , , 

Abstract
:1. Introduction
2. Materials and Methods
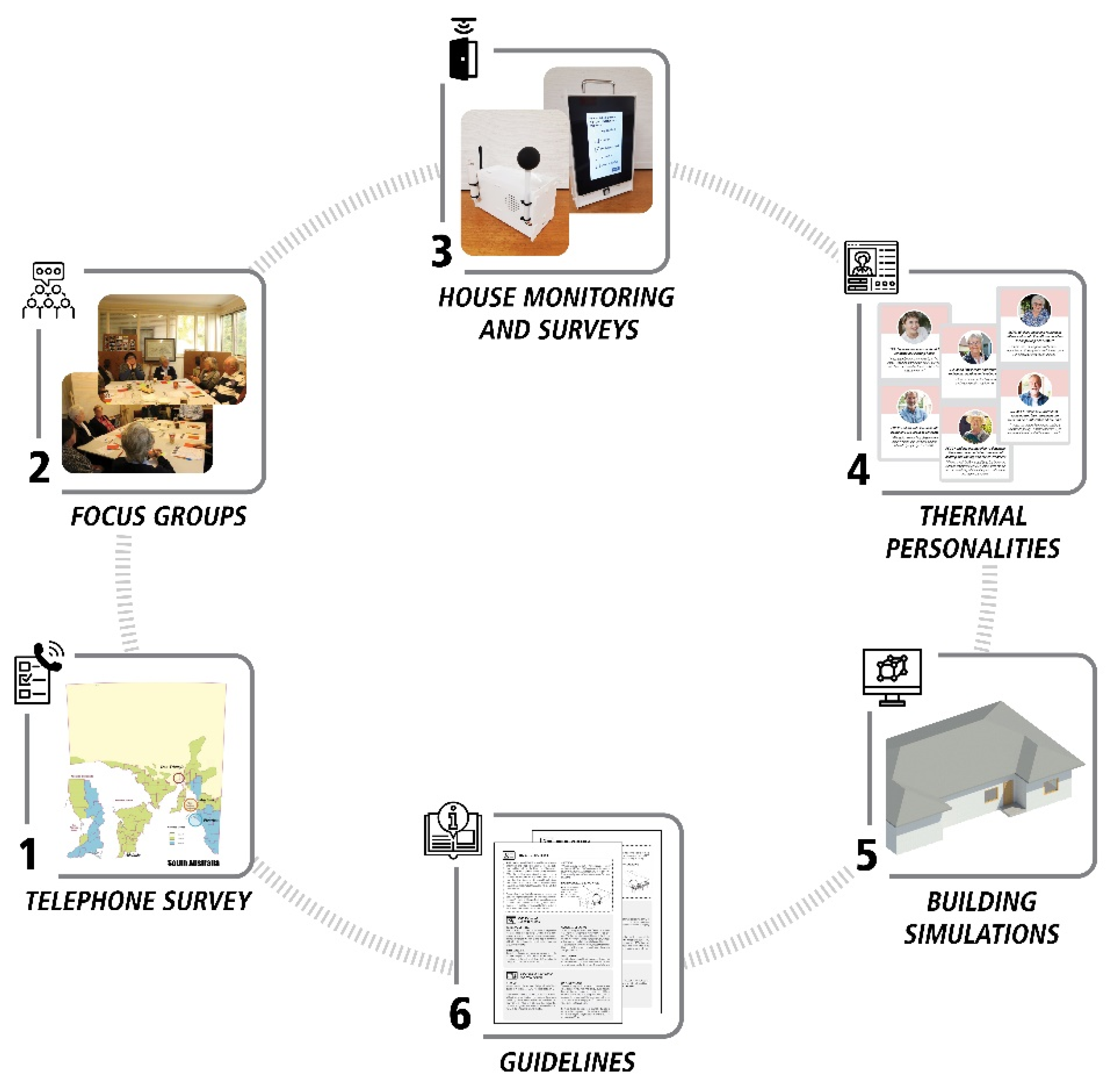
2.1. Initial Research
2.1.1. Telephone Survey
2.1.2. Focus Groups
2.1.3. Home Monitoring and Occupant Surveys
2.1.4. Thermal Personalities and Building Performance Simulations
2.2. Effects of the Thermal Environment on Health and Wellbeing
3. Results
3.1. Telephone Survey
3.2. Focus Groups
3.3. Home Monitoring and Occupant Surveys
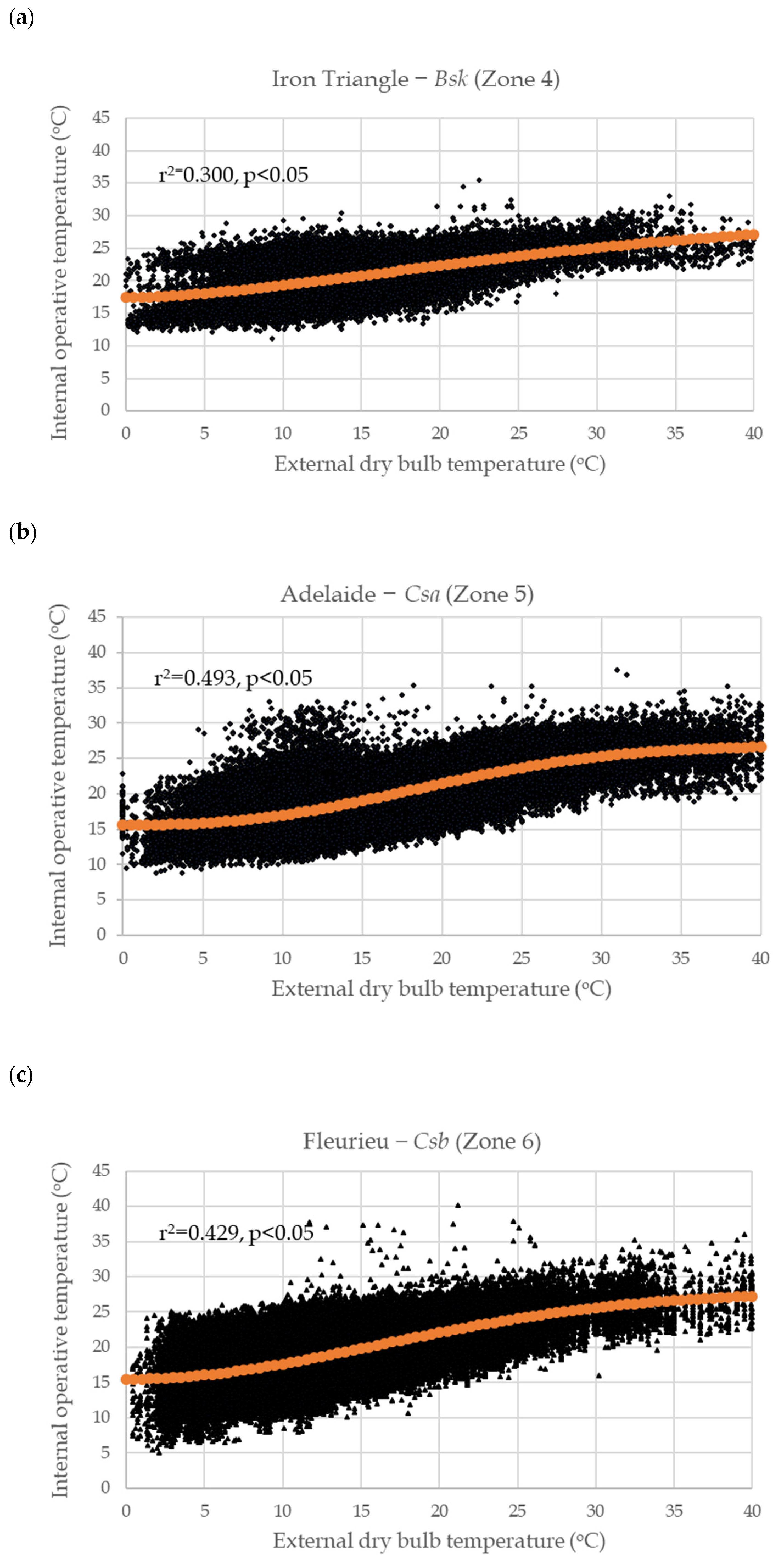
3.3.1. Analysis of Outdoor and Indoor Temperatures and Use of Heating/Cooling
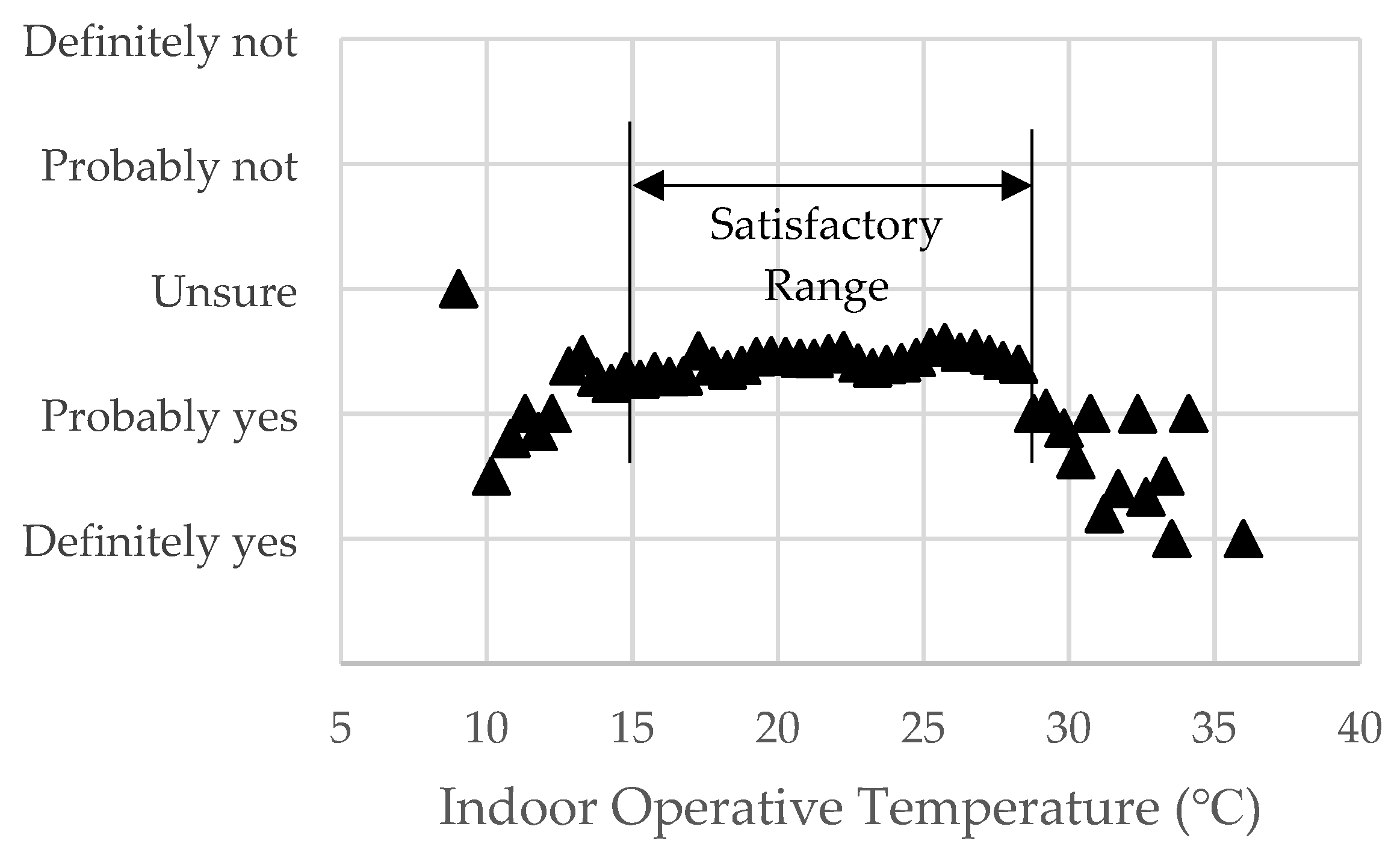
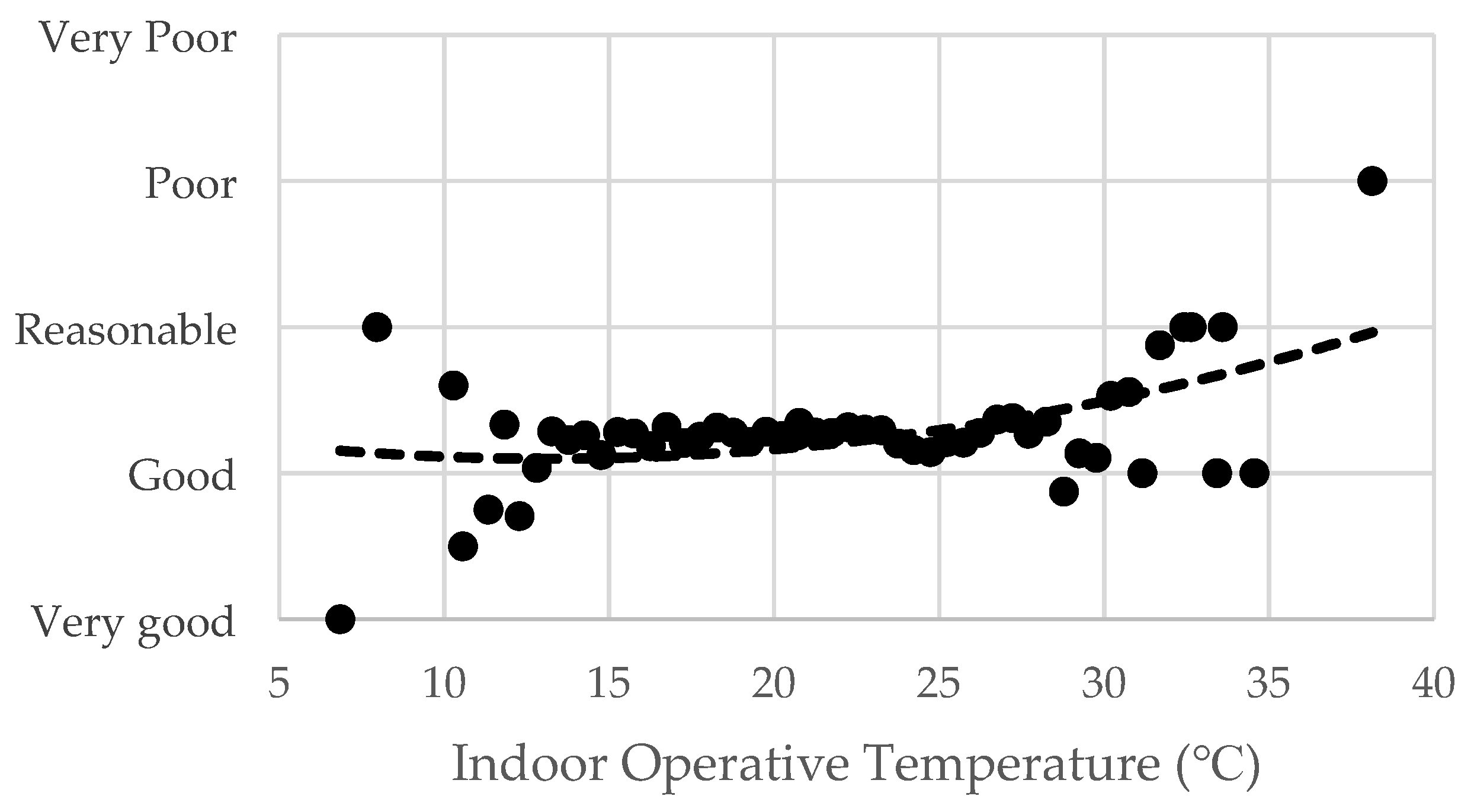
3.3.2. Health and Wellbeing
3.3.3. Temperature Humidity Health Index
3.3.4. Occupant Behaviours
4. Discussion
4.1. Thermal Environment, Behaviour and Health
4.1.1. Cold Indoor Conditions
4.1.2. Hot Indoor Conditions
4.2. Optimal Temperatures for Human Health and Thermal Comfort
4.3. The Way Forward
4.4. Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Dahlgren, G.; Whitehead, M. Policies and Strategies to Promote Social Equity in Health; Institute for Future Studies: Stockholm, Sweden, 1991. [Google Scholar]
- Howden-Chapman, P. Housing standards: A glossary of housing and health. J. Epidemiol. Community Health 2004, 3, 162–168. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kenney, W.L.; Munce, T.A. Invited review: Aging and human temperature regulation. J. Appl. Physiol. 2003, 95, 2598–2603. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, J. Who is sensitive to extremes of temperature? A case-only analysis. Epidemiology 2005, 16, 67–72. [Google Scholar] [CrossRef] [PubMed]
- Hansen, A.; Bi, P.; Pisaniello, D.; Nitschke, M.; Tucker, G.; Newbury, J.; Kitson, A.; Dal Grande, E.; Avery, J.; Zhang, Y.; et al. Heat-health behaviours of older people in two Australian states. Australas J. Ageing 2015, 34, E19–E25. [Google Scholar] [CrossRef] [PubMed]
- van Hoof, J.; Bennetts, H.; Hansen, A.; Kazak, J.K.; Soebarto, V. The living environment and thermal behaviours of older South Australians: A multi-focus group study. Int. J. Environ. Res. Public Health 2019, 16, 935. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nitschke, M.; Hansen, A.; Bi, P.; Pisaniello, D.; Newbury, J.; Kitson, A.; Tucker, G.; Avery, J.; Dal Grande, E. Risk factors, health effects and behaviour in older people during extreme heat: A survey in South Australia. Int. J. Environ. Res. Public Health 2013, 10, 6721–6733. [Google Scholar] [CrossRef] [Green Version]
- Gasparrini, A.; Guo, Y.; Hashizume, M.; Lavigne, E.; Zanobetti, A.; Schwartz, J.; Tobias, A.; Tong, S.; Rocklov, J.; Forsberg, B.; et al. Mortality risk attributable to high and low ambient temperature: A multicountry observational study. Lancet 2015, 386, 369–375. [Google Scholar] [CrossRef]
- Bennett, C.M.; Dear, K.B.; McMichael, A.J. Shifts in the seasonal distribution of deaths in Australia, 1968–2007. Int. J. Biometeorol. 2014, 58, 835–842. [Google Scholar] [CrossRef]
- Barnett, A.G.; Dobson, A.J.; McElduff, P.; Salomaa, V.; Kuulasmaa, K.; Sans, S. Cold periods and coronary events: An analysis of populations worldwide. J. Epidemiol. Community Health 2005, 59, 551–557. [Google Scholar] [CrossRef] [Green Version]
- Hajat, S.; Kovats, R.S.; Lachowycz, K. Heat-related and cold-related deaths in England and Wales: Who is at risk? Occup. Environ. Med. 2007, 64, 93–100. [Google Scholar] [CrossRef] [Green Version]
- Costello, A.; Abbas, M.; Allen, A.; Ball, S.; Bell, S.; Bellamy, R.; Friel, S.; Groce, N.; Johnson, A.; Kett, M.; et al. Managing the health effects of climate change: Lancet and University College London Institute for Global Health Commission. Lancet 2009, 373, 1693–1733. [Google Scholar] [CrossRef]
- Astrom, D.O.; Forsberg, B.; Rocklov, J. Heat wave impact on morbidity and mortality in the elderly population: A review of recent studies. Maturitas 2011, 69, 99–105. [Google Scholar] [CrossRef] [PubMed]
- McMichael, A.J.; Wilkinson, P.; Kovats, R.S.; Pattenden, S.; Hajat, S.; Armstrong, B.; Vajanapoom, N.; Niciu, E.M.; Mahomed, H.; Kingkeow, C.; et al. International study of temperature, heat and urban mortality: The ’ISOTHURM’ project. Int. J. Epidemiol. 2008, 37, 1121–1131. [Google Scholar] [CrossRef] [Green Version]
- Bi, P.; Williams, S.; Loughnan, M.; Lloyd, G.; Hansen, A.; Kjellstrom, T.; Dear, K.; Saniotis, A. The effects of extreme heat on human mortality and morbidity in Australia: Implications for Public Health. Asia Pac. J. Public Health 2011, 23, 27S–36S. [Google Scholar]
- Diaz, J.; Garcia, R.; Lopez, C.; Linares, C.; Tobias, A.; Prieto, L. Mortality impact of extreme winter temperatures. Int. J. Biometeorol. 2005, 49, 179–183. [Google Scholar] [CrossRef]
- Medina-Ramon, M.; Schwartz, J. Temperature, temperature extremes, and mortality: A study of acclimatization and effect modification in 50 United States Cities. Occup. Environ. Med. 2007, 64, 827–833. [Google Scholar] [CrossRef] [Green Version]
- Basu, R.; Samet, J.M. Relation between elevated ambient temperature and mortality: A review of the epidemiologic evidence. Epidemiol. Rev. 2002, 24, 190–202. [Google Scholar] [CrossRef] [PubMed]
- de Vries, R.; Blane, D. Fuel poverty and the health of older people: The role of local climate. J. Public Health 2013, 35, 361–366. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Howden-Chapman, P.; Viggers, H.; Chapman, R.; O’Sullivan, K.; Barnard, L.T.; Lloyd, B. Tackling cold housing and fuel poverty in New Zealand: A review of policies, research, and health impacts. Energy Policy 2012, 49, 134–142. [Google Scholar] [CrossRef]
- Hansen, A.; Bi, P.; Nitschke, M.; Pisaniello, D.; Newbury, J.; Kitson, A. Perceptions of heat-susceptibility in older persons: Barriers to adaptation. Int. J. Environ. Res. Public Health 2011, 8, 4714–4728. [Google Scholar] [CrossRef] [PubMed]
- Nitschke, M.; Krackowizer, A.; Hansen, A.L.; Bi, P.; Tucker, G.R. Heat health messages: A randomized controlled trial of a preventative messages tool in the older population of South Australia. Int. J. Environ. Res. Public Health 2017, 14, 992. [Google Scholar] [CrossRef] [Green Version]
- van Loenhout, J.A.; le Grand, A.; Duijm, F.; Greven, F.; Vink, N.M.; Hoek, G.; Zuurbier, M. The effect of high indoor temperatures on self-perceived health of elderly persons. Environ. Res. 2016, 146, 27–34. [Google Scholar] [CrossRef]
- Loughnan, M.; Carroll, M.; Tapper, N.J. The relationship between housing and heat wave resilience in older people. Int. J. Biometeorol. 2015, 59, 1291–1298. [Google Scholar] [CrossRef]
- Naughton, M.P.; Henderson, A.; Mirabelli, M.C.; Kaiser, R.; Wilhelm, J.L.; Kieszak, S.M.; Rubin, C.H.; McGeehin, M.A. Heat-related mortality during a 1999 heat wave in Chicago. Am. J. Prev. Med. 2002, 22, 221–227. [Google Scholar] [CrossRef]
- Kenny, G.P.; Flouris, A.D.; Yagouti, A.; Notley, S.R. Towards establishing evidence-based guidelines on maximum indoor temperatures during hot weather in temperate continental climates. Temperature 2019, 6, 11–36. [Google Scholar] [CrossRef] [PubMed]
- van Hoof, J.; Schellen, L.; Soebarto, V.; Wong, J.K.W.; Kazak, J.K. Ten questions concerning thermal comfort and ageing. Build. Environ. 2017, 120, 123–133. [Google Scholar] [CrossRef]
- Bennetts, H.; Martins, L.A.; van Hoof, J.; Soebarto, V. Thermal personalities of older people in South Australia: A personas-based approach to develop thermal comfort guidelines. Int. J. Environ. Res. Public Health 2020, 17, 8402. [Google Scholar] [CrossRef]
- Soebarto, V.; Bennetts, H.; Hansen, A.; Zuo, J.; Williamson, T.; Pisaniello, D.; van Hoof, J.; Visvanathan, R. Living environment, heating-cooling behaviours and well-being: Survey of older South Australians. Build. Environ. 2019, 157, 215–226. [Google Scholar] [CrossRef]
- Australian Bureau of Statistics National. State and Territory Population. Available online: https://www.abs.gov.au/statistics/people/population/national-state-and-territory-population/jun-2020 (accessed on 24 March 2021).
- Stern, H.; de Hoedt, G.; Ernst, J. Objective classification of Australian climates. Aust. Meteorol. Mag. 2000, 49, 87–96. [Google Scholar]
- Australian Building Codes Board Climate Zone Map Australia. Available online: https://www.abcb.gov.au/resource/map/climate-zone-map-australia (accessed on 27 October 2021).
- EuroQol Research Foundation. EQ-5D-5L User Guide. 2019. Available online: https://euroqol.org/publications/user-guides (accessed on 5 May 2021).
- IBM Corp IBM SPSS Statistics for Windows, Version 25.0. Available online: https://www.ibm.com/products/spss-statistics (accessed on 27 October 2021).
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psych. 2006, 3, 77–101. [Google Scholar] [CrossRef] [Green Version]
- Soebarto, V.; Williamson, T.; Bennetts, H.; Arakawa Martins, L.; Pisaniello, D.; Hansen, A.; Visvanathan, R.; Carre, A. Development of an integrated data acquisition system for thermal comfort. In Proceedings of the Windsor 2020 Resilient Comfort Conference, Windsor, UK, 16–19 April 2020; Roaf, S., Nicol, F., Finlayson, W., Eds.; Silesian University of Technology: Gliwice, Poland, 2020; pp. 155–170. [Google Scholar]
- Tanita Corporation Innerscan Dual RD-953 Instruction Manual. Available online: https://tanita.eu/media/wysiwyg/manuals/home-use-body-composition-monitors/rd-953-instruction-manual-en.pdf (accessed on 27 October 2021).
- Völgyi, E.; Tylavsky, F.A.; Lyytikäinen, A.; Suominen, H.; Alén, M.; Cheng, S. Assessing body composition with DXA and bioimpedance: Effects of obesity, physical activity, and age. Obesity 2008, 16, 700–705. [Google Scholar] [CrossRef] [PubMed]
- Arakawa Martins, L.; Williamson, T.; Bennetts, H.; Zuo, J.; Visvanathan, R.; Hansen, A.; Pisaniello, D.; van Hoof, J.; Soebarto, V. Individualising thermal comfort models for older people: The effects of personal characteristics on comfort and wellbeing. In Proceedings of the Windsor 2020 Resilient Comfort Conference, Windsor, UK, 16–19 April 2020; Roaf, S., Nicol, F., Finlayson, W., Eds.; Silesian University of Technology: Gliwice, Poland, 2020; pp. 187–199. [Google Scholar]
- Soebarto, V.; Williamson, T.; Carre, A.; Arakawa Martins, L. Understanding indoor environmental conditions and occupant’s responses in houses of older people. IOP Conf. Ser. Mater. Sci. Eng. 2019, 609, 042096. [Google Scholar] [CrossRef] [Green Version]
- De Dear, R. Ping-pong globe thermometers for mean radiant temperatures. H V Eng. 1988, 60, 10–11. [Google Scholar]
- d’Ambrosio Alfano, F.R.; Dell’isola, M.; Ficco, G.; Palella, B.I.; Riccio, G. On the measurement of the mean radiant temperature by means of globes: An experimental investigation under black enclosure conditions. Build. Environ. 2021, 193, 107655. [Google Scholar] [CrossRef]
- ASHRAE. Thermal Environmental Conditions for Human Occupancy; American Society of Heating, Refrigerating and Air Conditioning Engineers, Inc.: Atlanta, GA, USA, 2020. [Google Scholar]
- Adlin, T.; Pruitt, J. The Essential Persona Lifecycle Your Guide to Building and Using Personas, 1st ed.; Morgan Kaufmann: Burlington, MA, USA, 2010. [Google Scholar]
- Arakawa Martins, L.; Soebarto, V.; Williamson, T.; Pisaniello, D.; Bennetts, H. The use of building performance simulation and personas for the development of thermal comfort guidelines for older people in South Australia. J. Build. Perform. Simul. 2021; in press. [Google Scholar] [CrossRef]
- Williamson, T.; Soebarto, V.; Bennetts, H.; Arakawa Martins, L.; Pisaniello, D. Thermal comfort, well-being and health of older residents in South Australia. In Proceedings of the Windsor 2020 Resilient Comfort Conference, Windsor, UK, 16–19 April 2020; Roaf, S., Nicol, F., Finlayson, W., Eds.; Silesian University of Technology: Gliwice, Poland, 2020; pp. 171–186. [Google Scholar]
- United Nations Department of Economic and Social Affairs Sustainable Development. Available online: https://sdgs.un.org/goals (accessed on 24 March 2021).
- Curriero, F.C.; Heiner, K.S.; Samet, J.M.; Zeger, S.L.; Strug, L.; Patz, J.A. Temperature and mortality in 11 cities of the eastern United States. Am. J. Epidemiol. 2002, 155, 80–87. [Google Scholar] [CrossRef]
- World Health Organization. WHO Housing and Health Guidelines; World Health Organization: Geneva, Switzerland, 2018. [Google Scholar]
- Fyfe, C.; Telfar, L.; Barnard; Howden-Chapman, P.; Douwes, J. Association between home insulation and hospital admission rates: Retrospective cohort study using linked data from a national intervention programme. BMJ 2020, 371, m4571. [Google Scholar] [CrossRef]
- Bright, F.M.; Winskog, C.; Walker, M.; Byard, R.W. A comparison of hypothermic deaths in South Australia and Sweden. J. Forensic. Sci. 2014, 59, 983–985. [Google Scholar] [CrossRef]
- Hansen, A.; Soebarto, V. The epidemiology of health and mortality at extremes. In Proceedings of the 1st International Conference on Comfort at the Extremes: Energy, Economy and Climate, Dubai, United Arab Emirates, 10–11 April 2019; Roaf, S., Finlayson, W., Eds.; Ecohouse Initiave Ltd.: Dubai, United Arab Emirates, 2019; pp. 10–22. [Google Scholar]
- Byard, R.W.; Bright, F.M. Lethal hypothermia—A sometimes elusive diagnosis. Forensic Sci. Med. Pathol. 2018, 14, 421–423. [Google Scholar] [CrossRef] [Green Version]
- Bright, F.; Gilbert, J.D.; Winskog, C.; Byard, R.W. Additional risk factors for lethal hypothermia. J. Forensic Leg. Med. 2013, 20, 595–597. [Google Scholar] [CrossRef] [PubMed]
- Hwang, R.L.; Chen, C.P. Field study on behaviors and adaptation of elderly people and their thermal comfort requirements in residential environments. Indoor Air 2010, 20, 235–245. [Google Scholar] [CrossRef]
- Davis, R.E.; McGregor, G.R.; Enfield, K.B. Humidity: A review and primer on atmospheric moisture and human health. Environ. Res. 2016, 144, 106–116. [Google Scholar] [CrossRef] [Green Version]
- Han, L.; Ran, J.; Chan, K.H.; Mak, Y.W.; Suen, L.; Cowling, B.J.; Yang, L. Indoor environmental factors and acute respiratory illness in a prospective cohort of community-dwelling older adults. J. Infect. Dis. 2020, 222, 967–978. [Google Scholar] [CrossRef]
- Varghese, B.M.; Beaty, B.; Bi, P.; Nairn, J. Heatwave-Health Vulnerability in Adelaide: Analysis of Mortality and Morbidity Outcomes. Available online: https://ehp.niehs.nih.gov/doi/abs/10.1289/isee.2020.virtual.P-0399 (accessed on 27 October 2021).
- Williams, S.; Nitschke, M.; Sullivan, T.; Tucker, G.R.; Weinstein, P.; Pisaniello, D.L.; Parton, K.A.; Bi, P. Heat and health in Adelaide, South Australia: Assessment of heat thresholds and temperature relationships. Sci. Total Environ. 2012, 414, 126–133. [Google Scholar] [CrossRef] [PubMed]
- Guergova, S.; Dufour, A. Thermal sensitivity in the elderly: A review. Ageing Res. Rev. 2011, 10, 80–92. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization UN Decade of Healthy Ageing. Available online: https://www.who.int/initiatives/decade-of-healthy-ageing (accessed on 24 March 2021).
- Soebarto, V.; Bennetts, H.; Arakawa Martins, L.; van Hoof, J.; Visvanathan, R.; Hansen, A.; Pisaniello, D.; Williamson, T.; Zuo, J. Thermal Comfort at Home: A Guide for Older South Australians; The University of Adelaide: Adelaide, Australia, 2021; ISBN 978-0-646-85165-5. [Google Scholar] [CrossRef]
- Australian Government Bureau of Meteorology South Australia in Summer 2018–2019: Record Warm Days and Drier than Average. Available online: http://www.bom.gov.au/climate/current/season/sa/archive/201902.summary.shtml (accessed on 24 March 2021).
- Ziersch, A.M.; Baum, F.; Ngurah Darmawan, I.G.; Kavanagh, A.M.; Bentley, R.J. Social capital and health in rural and urban communities in South Australia. ANZ J. Public Health. 2009, 33, 7–16. [Google Scholar] [CrossRef] [PubMed]
- Australian Bureau of Statistics National Health Survey: First Results 2014–2015. Available online: https://www.abs.gov.au/AUSSTATS/[email protected]/DetailsPage/4364.0.55.0012014-15?OpenDocument (accessed on 27 October 2021).
- Hansen, A.; Bi, P.; Nitschke, M.; Ryan, P.; Pisaniello, D.; Tucker, G. The effect of heat waves on mental health in a temperate Australian city. Environ. Health Perspect. 2008, 116, 1369–1375. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Y.; Nitschke, M.; Krackowizer, A.; Dear, K.; Pisaniello, D.; Weinstein, P.; Tucker, G.; Shakib, S.; Bi, P. Risk factors of direct heat-related hospital admissions during the 2009 heatwave in Adelaide, Australia: A matched case-control study. BMJ Open 2016, 6, e010666. [Google Scholar] [CrossRef] [Green Version]
- van Hoof, J.; Kort, H.S.M.; Hensen, J.L.M.; Duijnstee, M.S.H.; Rutten, P.G.S. Thermal comfort and the integrated design of homes for older people with dementia. Build. Environ. 2010, 45, 358–370. [Google Scholar] [CrossRef] [Green Version]
- Vandentorren, S.; Bretin, P.; Zeghnoun, A.; Mandereau-Bruno, L.; Croisier, A.; Cochet, C.; Riberon, J.; Siberan, I.; Declercq, B.; Ledrans, M. August 2003 heat wave in France: Risk factors for death of elderly people living at home. Eur. J. Public Health 2006, 16, 583–591. [Google Scholar] [CrossRef] [Green Version]
- Cincinelli, A.; Martellini, T. Indoor air quality and health. Int. J. Environ. Res. Public Health 2017, 14, 1286. [Google Scholar] [CrossRef] [PubMed] [Green Version]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Iron Triangle Bsk (Zone 4) | Adelaide Csa (Zone 5) | Fleurieu Csb (Zone 6) | Total | |||
|---|---|---|---|---|---|---|---|
| Males | Females | Males | Females | Males | Females | ||
| Survey | 15 | 25 | 35 | 55 | 48 | 72 | 250 |
| Focus groups | 0 | 7 | 5 | 22 | 3 | 12 | 49 |
| Home monitoring | 2 | 3 | 10 | 23 | 11 | 22 | 71 |
| TOTAL | 17 | 35 | 50 | 100 | 62 | 106 | 370 1 |
| Metric and Time | Iron Triangle | Adelaide | Fleurieu |
|---|---|---|---|
| Bsk (Zone 4) | Csa (Zone 5) | Csb (Zone 6) | |
| Throughout monitoring period: | |||
| Outdoor 1 | |||
| Max daily temperature (°C) | 41.1 | 47.4 | 40.5 |
| Min daily temperature (°C) | −0.6 | −1.7 | 0.0 |
| Indoor 2 | |||
| Ave max operative temperature (°C) | 32.7 | 31.9 | 32.7 |
| Ave min operative temperature (°C) | 12.8 | 12.0 | 11.0 |
| Mean SD operative temperature (°C) | 3.25 | 3.27 | 3.11 |
| At the time votes were recorded 3 | |||
| Max indoor (outdoor) hourly temp. (°C) | 28.9 (40) | 38.1 (46.8) | 33.4 (40.5) |
| Min indoor (outdoor) hourly temp. (°C) | 12.6 (4.2) | 11.8 (2.4) | 6.8 (4.8) |
| Ave indoor (outdoor) RH (%) | 52 (54) | 56 (57) | 57 (63) |
| AC usage (% of time) | 8.7 | 8.3 | 9.7 |
| Heating usage (% of time) | 22.4 | 19.8 | 15.8 |
| Location (Climate Zone) | A | B | K | n |
|---|---|---|---|---|
| Iron Triangle (Bsk, Zone 4) | 17.409 | 12.339 | 0.00421 | 1.60 |
| Adelaide (Csa, Zone 5) | 15.621 | 11.181 | 0.00044 | 2.48 |
| Fleurieu (Csb, Zone 6) | 15.470 | 12.394 | 0.00199 | 1.98 |
| All 3 climate zones | 15.844 | 11.665 | 0.000813 | 2.28 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hansen, A.; Williamson, T.; Pisaniello, D.; Bennetts, H.; van Hoof, J.; Arakawa Martins, L.; Visvanathan, R.; Zuo, J.; Soebarto, V. The Thermal Environment of Housing and Its Implications for the Health of Older People in South Australia: A Mixed-Methods Study. Atmosphere 2022, 13, 96. https://doi.org/10.3390/atmos13010096
Hansen A, Williamson T, Pisaniello D, Bennetts H, van Hoof J, Arakawa Martins L, Visvanathan R, Zuo J, Soebarto V. The Thermal Environment of Housing and Its Implications for the Health of Older People in South Australia: A Mixed-Methods Study. Atmosphere. 2022; 13(1):96. https://doi.org/10.3390/atmos13010096
Chicago/Turabian StyleHansen, Alana, Terence Williamson, Dino Pisaniello, Helen Bennetts, Joost van Hoof, Larissa Arakawa Martins, Renuka Visvanathan, Jian Zuo, and Veronica Soebarto. 2022. "The Thermal Environment of Housing and Its Implications for the Health of Older People in South Australia: A Mixed-Methods Study" Atmosphere 13, no. 1: 96. https://doi.org/10.3390/atmos13010096
APA StyleHansen, A., Williamson, T., Pisaniello, D., Bennetts, H., van Hoof, J., Arakawa Martins, L., Visvanathan, R., Zuo, J., & Soebarto, V. (2022). The Thermal Environment of Housing and Its Implications for the Health of Older People in South Australia: A Mixed-Methods Study. Atmosphere, 13(1), 96. https://doi.org/10.3390/atmos13010096