
Exploring Health Impacts of Occupational Exposure to Carbon Monoxide in the Labour Community of Hattar Industrial Estate

 ,
, 
Abstract
:
1. Introduction
2. Materials and Methods
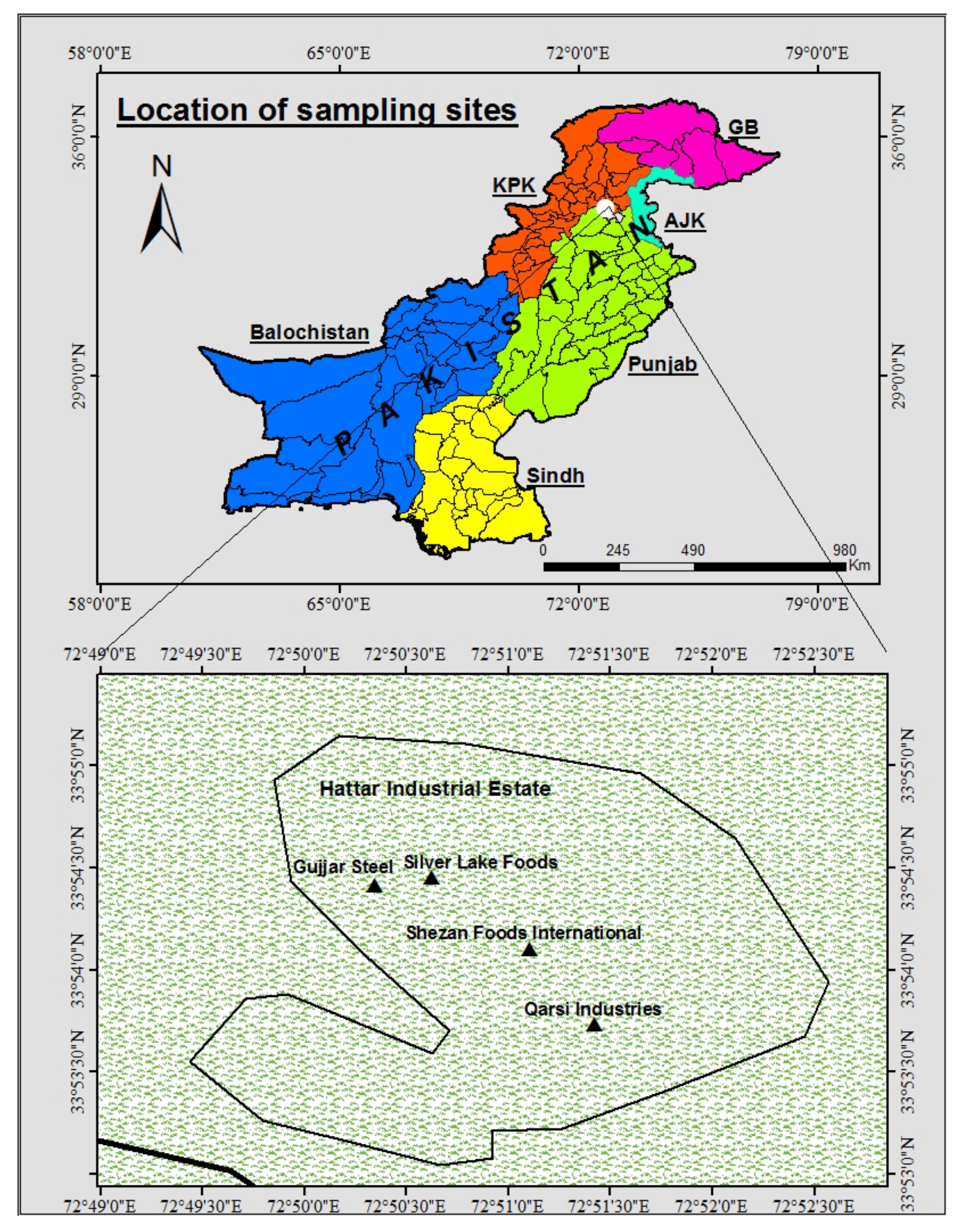
2.1. The Study Area
2.2. Sampling Sites
2.3. Control Sites
2.4. Carbon Monoxide Saturation in the Hemoglobin (SpCO) of Respondents
2.5. Comparision of Observed and Standard Concentration of Carbon Monoxide
2.6. Statistical Package for the Social Sciences (SPSS)
2.7. Statistical Modelling Equation for Attributable Risk (AP)
3. Results
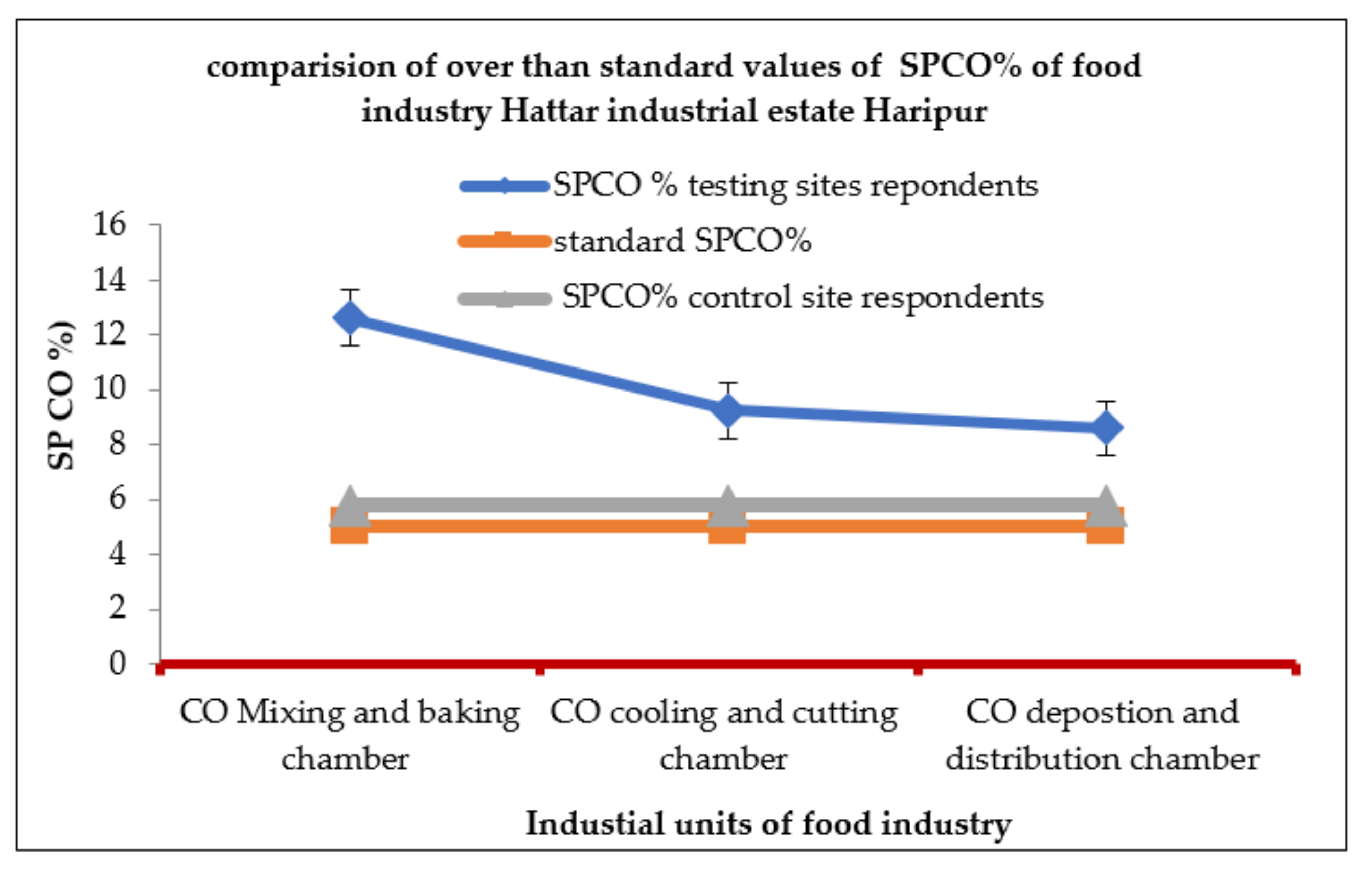
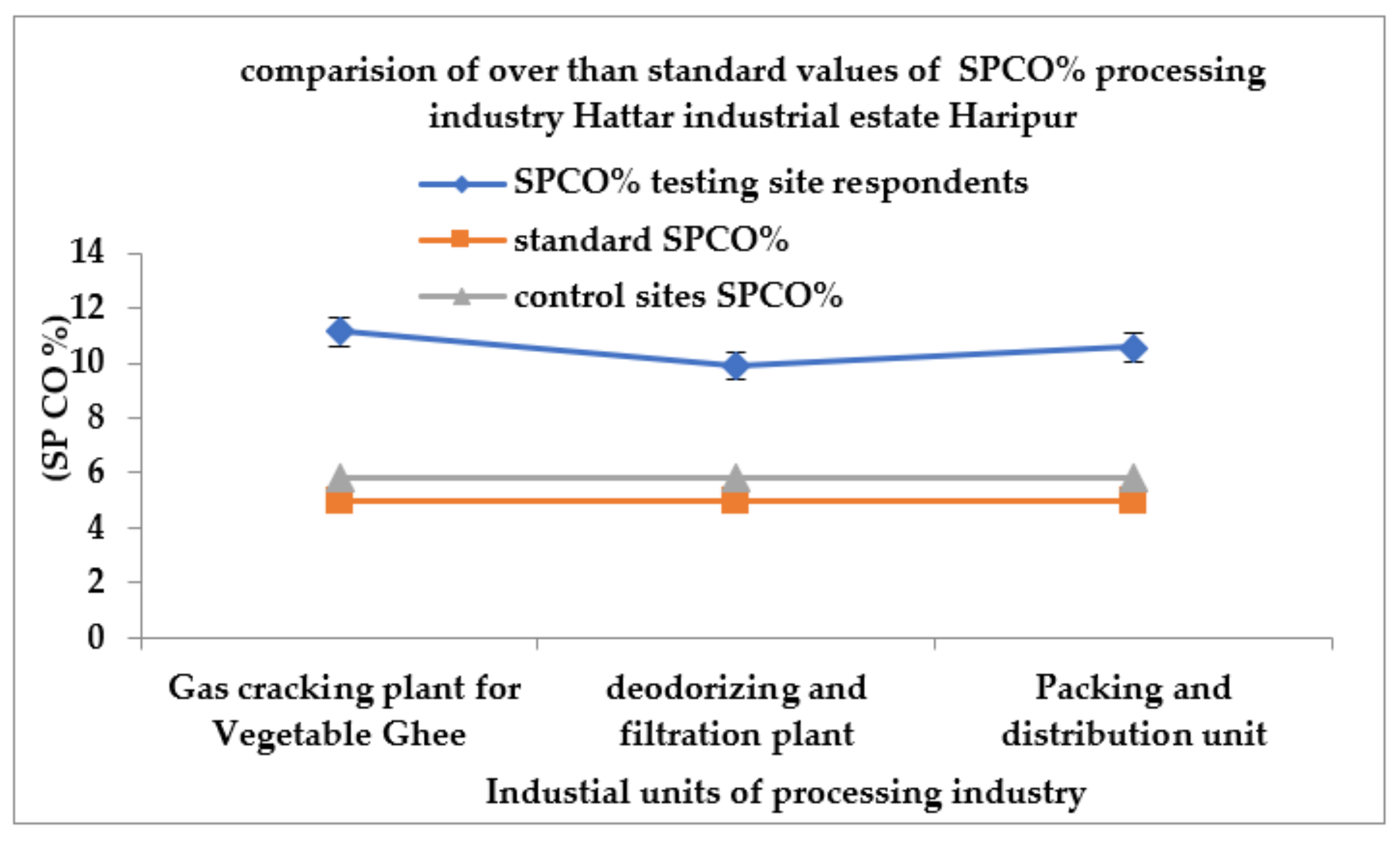
3.1. Comparision of Observed and Standard Concentrations of Carbon Monoxide
3.1.1. Food Industry
3.1.2. Processing Industry
3.1.3. Steel Industry
3.2. Comparision of SPCO% among Respondents from the Food, Processing and Steel Industries
3.3. Statistical Package for the Social Sciences (SPSS)
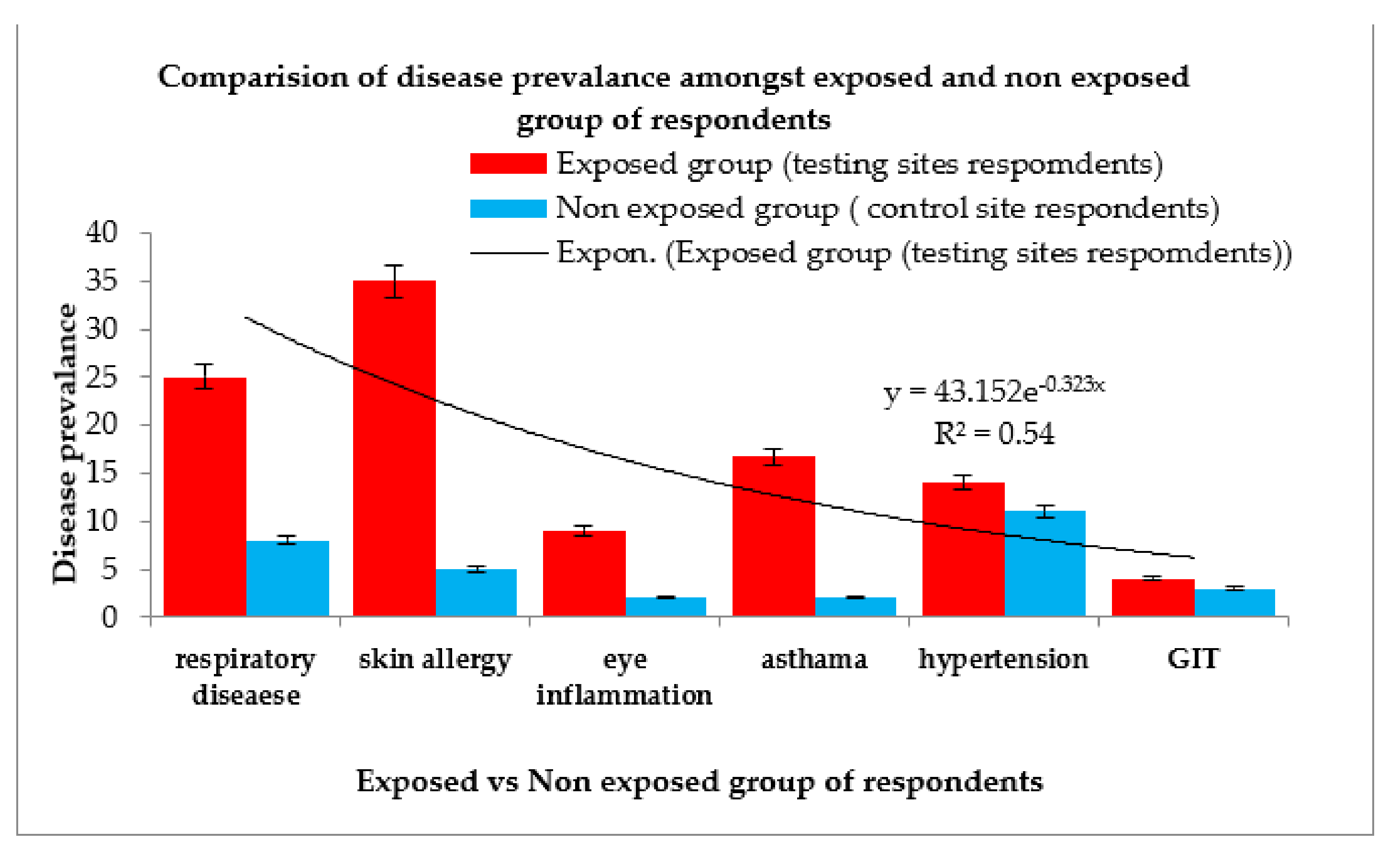
3.4. Statistical Model Validation of the Perfusion Index (%CO)
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| (ppm) | parts per million |
| The Food and Drug Administration | FDA- |
| Carboxyhemoglobin by pulse oximeter | (SPCO®) |
| Standard laboratory blood measurement | (COHb) |
| Cardiovascular disease | CV |
| Perfusion index ratio | (PI) |
| GIT | Gastrointestinal tract |
| Ppb | Parts per billion |
| CO | Carbon monoxide |
| PM | Particulate matter |
| O3 | Ozone |
| NO2 | Nitrogen dioxide |
| SO2 | Sulfur dioxide |
References
- Fidaev, D.T.; Khunarov, A.M.; Kuchkarova, N.X. Air pollution and its consequences for human health. J. Educ. Res. 2021, 2, 2. [Google Scholar]
- Bala, G.P.; Rajnoveanu, R.M.; Tudorache, E.; Motișan, R.; Oancea, C. Air pollution exposure—The (in) visible risk factor for respiratory diseases. Environ. Sci. Pollut. Res. 2019, 26, 12280–12287. [Google Scholar]
- Dias, C.; Marques, M.; Santos, V.; Tavares, A.S. Spectrophotometric determination of carboxyhaemoglobin in a sample of automobile mechanics occupationally exposed to carbon monoxide. Res. Netw. Health 2018, 1, 1–7. [Google Scholar]
- Oliverio, S.; Varlet, V.; Zeka, A.; Leonardi, G. PI-3-9 The burden of carbon monoxide exposure on public health: Evaluating the role of carboxyhaemoglobin (cohb) as a biomarker and exploring new approaches for quantification. Occup. Environ. Med. 2018, 75, 31–39. [Google Scholar]
- Hoy, R.F.; Glass, D.C.; Dimitriadis, C.; Hansen, J.; Hore-Lacy, F.; Sim, M.R. Identification of early-stage silicosis through health screening of stone benchtop industry workers in Victoria, Australia. Occup. Environ. Med. 2021, 78, 296–302. [Google Scholar] [CrossRef] [PubMed]
- Kantor, D.B.; Petty, C.R.; Phipatanakul, W.; Gaffin, J.M. Transcutaneous CO-oximetry differentiates asthma exacerbation and convalescence in children. J. Allergy Clin. Immunol. 2018, 142, 676–678. [Google Scholar] [CrossRef] [Green Version]
- Chen, L.; Li, J.; Pang, X.; Shi, K.; Chen, J.; Wang, J.; Xu, M. Impact of COVID-19 Lockdown on Air Pollutants in a Coastal area of the Yangtze River Delta: China. Measured by Low-Cost Sensor Package. Atmosphere 2021, 12, 345. [Google Scholar] [CrossRef]
- Acharya, S.P.; Purpura, A.; Kao, L.; House, D. RIncidence and risk factors for carbon monoxide poisoning in an emergency department in Nepal. Toxicol. Commun. 2022, 6, 13–19. [Google Scholar] [CrossRef]
- Martinasek, M.P.; Calvanese, A.V.; Lipski, B.K.A. Naturalistic Study of Carbon Monoxide, Heart Rate, Oxygen Saturation, and Perfusion Index in Hookah Lounge Patrons. Respir. Care 2021, 66, 269–274. [Google Scholar] [CrossRef]
- Bahng, Y.; Baek, K.; Park, J.T.; Choi, W.J.; Kwak, K. Carbon Monoxide Poisoning and Developing Ischemic Heart Disease: A Nationwide Population-Based Nested Case-Control Study. Toxics 2021, 9, 239. [Google Scholar] [CrossRef]
- Diaz-Canestro, C.; Pentz, B.; Sehgal, A.; Montero, D. Sex Differences in Orthostatic Tolerance Are Mainly Explained by Blood Volume and Oxygen Carrying Capacity. Crit. Care Explor. 2022, 9, 1. [Google Scholar] [CrossRef] [PubMed]
- Cloyd, T.; Davidson, C.; LoVecchio, F. Carbon Monoxide Exposure: Evaluation and Management. Emerg. Med. Rep. 2021, 42, 24. [Google Scholar]
- Zaouter, C.; Zavorsky, G.S. The measurement of carboxyhemoglobin and methemoglobin using a non-invasive pulse CO-oximeter. Respir. Physiol. Neurobiol. 2012, 182, 88–92. [Google Scholar] [CrossRef]
- World Health Organization. WHO Global Air Quality Guidelines: Particulate Matter (PM2.5 and PM10), Ozone, Nitrogen Dioxide, Sulfur Dioxide and Carbon Monoxide 2021; WHO: Geneva, Switzerland, 2021. [Google Scholar]
- Townsend, C.L.; Maynard, R.L. Effects on health of prolonged exposure to low Concentrations of carbon monoxide. Occup. Environ. Med. 2021, 59, 708–711. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mukhopadhyay, S.; Hirsch, A.; Etienne, S.; Melnikova, N.; Wu, J.; Sircar, K.; Orr, M. Surveillance of carbon monoxide-related incidents—Implications for prevention of related illnesses and injuries, 2005–2014. Am. J. Emerg. Med. 2018, 36, 1837–1844. [Google Scholar] [CrossRef] [PubMed]
- Raub, J.A.; Mathieu-Nolf, M.; Hampson, N.B.; Thom, S.R. Carbon monoxide poisoning—A public health perspective. J. Toxicol. 2000, 145, 1–14. [Google Scholar] [CrossRef]
- Quarmby, S.; Georgina, S.; Megan, M. Air Quality Strategies and Technologies: A Rapid Review of the International Evidence. Sustainability 2019, 11, 2757. [Google Scholar] [CrossRef] [Green Version]
- Bourdrel, T.; Annesi-Maesano, I.; Alahmad, B.; Maesano, C.N.; Bind, M.A. The impact of outdoor air pollution on COVID-19: A review of evidence from in vitro, animal, and human studies. Eur. Respir. Rev. 2021, 30, 200242. [Google Scholar] [CrossRef]
- Nilsson, L.J.; Bauer, F.; Åhman, M.; Andersson, F.N.; Bataille, C.; de la Rue du Can, S.; Vogl, V. An industrial policy framework for transforming energy and emissions intensive industries towards zero emissions. Clim. Policy 2021, 21, 1053–1065. [Google Scholar] [CrossRef]
- Andersson, K.; Busch Paulsson, E. Accuracy Validation of Pulse Oximeters Used at Hospitals: A Cross-Sectional Study performed in Stockholm; School of Technology and Health, Royal Institute of Technology: Stockholm, Sweden, 2017. [Google Scholar]
- Masimo Corp. Masimo SET Rad 57 Pulse CO-Oximeter. 510(k) Summary of the Safety and Efficacy. Available online: http://www.accessdata.fda.gov/scripts/cdrh/cfdocs/cfPMN/pmn.cfm (accessed on 10 August 2010).
- Verweij, B.G.F.; Rood, P.P.M.; Schuit, S.C.E.; Bouwhuis, M.G. Waterpipe smoking: Not as innocent as it may seem. Neth. J. Med. 2019, 77, 156–159. [Google Scholar]
- Yildiz, L.A.; Gultekingil, A.; Kesici, S.; Bayrakci, B.; Teksam, O. Predictors of severe clinical course in children with carbon monoxide poisoning. Pediatr. Emerg. Care 2021, 37, 308–311. [Google Scholar]
- Marvel, S.W.; House, J.S.; Wheeler, M.; Song, K.; Zhou, Y.H.; Wright, F.A.; Reif, D.M. The COVID-19 Pandemic Vulnerability Index (PVI) Dashboard: Monitoring county-level vulnerability using visualization, statistical modeling, and machine learning. Environ. Health Perspect. 2021, 129, 017701. [Google Scholar] [CrossRef] [PubMed]
- Okagbue, H.I.; Oguntunde, P.E.; Obasi, E.C.; Akhmetshin, E. MTrends and usage pattern of SPSS and Minitab Software in Scientific research. J. Phys. Conf. Ser. 2021, 1734, 012017. [Google Scholar] [CrossRef]
- Faustini, A.; Davoli, M. Attributable Risk to Assess the Health Impact of Air Pollution: Advances, Controversies, State of the Art and Future Needs. Int. J. Environ. Res. 2020, 17, 4512. [Google Scholar] [CrossRef]
- Kim, D.; Chen, Z.; Zhou, L.F.; Huang, S.X. Air pollutants and early origins of respiratory diseases. Chronic Dis. 2018, 4, 75–94. [Google Scholar] [CrossRef] [PubMed]
- Simonsen, C.; Magnusdottir, S.O.; Andreasen, J.J.; Wimmer, R.; Rasmussen Kjærgaard, B.S.B.; Maltesen, R.G. Metabolic changes during carbon monoxide poisoning, An experimental study. J. Cell. Mol. Med. 2021, 11, 5191–5201. [Google Scholar] [CrossRef] [PubMed]
- Gokhale, S.G.; Daggubati, V.S. Spectrometry of cord blood and maternal blood for Hb-F and Hb-A and novel technology for non-invasive measurement of hemoglobin in mother and baby. J. Matern. Fetal Neonatal. Med. 2021, 35, 1–4. [Google Scholar] [CrossRef]
- Maisel, W.H.; Lewis, R.J. Noninvasive measurement of carboxyhemoglobin: How accurate is accurate enough. Ann. Emerg. Med. 2010, 56, 389–391. [Google Scholar] [CrossRef]
- Liu, Z.; Meng, H.; Huang, J.; Kwangwari, P.; Ma, K.; Xiao, B.; Li, L. Acute carbon monoxide poisoning with low saturation of carboxyhaemoglobin: A forensic retrospective study in Shanghai, China. Sci. Rep. 2021, 11, 18554. [Google Scholar] [CrossRef]
- Rose, J.J.; Wang, L.; Xu, Q.; McTiernan, C.F.; Shiva, S.; Tejero, J.; Gladwin, M.T. Carbon monoxide poisoning: Pathogenesis, management, and future directions of therapy. Am. J. Respir. Crit. 2017, 195, 596–606. [Google Scholar] [CrossRef]
- Aoshima, K.; Yamaoka, H.; Nakamura, S.; Nojima, T.; Naito, H.; Nakao, A. Right hemiplegia following acute carbon monoxide poisoning. Cureus 2021, 7, 7759–16738. [Google Scholar] [CrossRef]
- Wang, H.; Hao, S.C.S.; Chang, K.C.; Hung, M.; Yang, C.C.; Liao, S.C. Quantifying the Effects of Climate Factors on Carbon Monoxide Poisoning: A Retrospective Study in Taiwan. Front. Public Health 2021, 14, 1537. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Lu, Q.; Jia, J.; Xiang, D.; Xi, Y. Multicenter retrospective analysis of the risk factors for delayed neurological sequelae after acute carbon monoxide poisoning. Am. J. Emerg. Med. 2021, 46, 165–169. [Google Scholar] [CrossRef] [PubMed]
- Carrol, R.; Prentice, C.R. Community vulnerability and mobility: What matters most in spatio-temporal modeling of the COVID-19 pandemic? Soc. Sci. Med. 2021, 287, 114395. [Google Scholar] [CrossRef] [PubMed]
- Yarragunta, Y.; Srivastava, S.; Mitra, D.; Chandola, H.C. Source apportionment of carbon monoxide over India: A quantitative analysis using mozart-4. Environ. Sci. Pollut. Res. 2021, 28, 8722–8742. [Google Scholar] [CrossRef] [PubMed]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| SpCO% Interpretation (Carboxyheamoglobin) | |
|---|---|
| 0–5% | Normal in non-smokers |
| 5–10% | Normal in smokers For non-smokers, treat with high-flow O2 if available |
| 10–15% | (In any patient) treat with high-flow O2 if available |
| >15% | High-flow O2 × 30 min, then reassess |
| >30%, or unconscious or pregnant | Consider immediate transport to closest hyperbaric treatment facility |
| Formula Used | ||
|---|---|---|
| Respiratory Diseases | Dermatosis | Eye Ittitation |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jadoon, S.; Nawazish, S.; Mahmood, Q.; Rafique, A.; Sohail, S.; Zaidi, A. Exploring Health Impacts of Occupational Exposure to Carbon Monoxide in the Labour Community of Hattar Industrial Estate. Atmosphere 2022, 13, 406. https://doi.org/10.3390/atmos13030406
Jadoon S, Nawazish S, Mahmood Q, Rafique A, Sohail S, Zaidi A. Exploring Health Impacts of Occupational Exposure to Carbon Monoxide in the Labour Community of Hattar Industrial Estate. Atmosphere. 2022; 13(3):406. https://doi.org/10.3390/atmos13030406
Chicago/Turabian StyleJadoon, Suneela, Shamyla Nawazish, Qaisar Mahmood, Asif Rafique, Summar Sohail, and Asma Zaidi. 2022. "Exploring Health Impacts of Occupational Exposure to Carbon Monoxide in the Labour Community of Hattar Industrial Estate" Atmosphere 13, no. 3: 406. https://doi.org/10.3390/atmos13030406
APA StyleJadoon, S., Nawazish, S., Mahmood, Q., Rafique, A., Sohail, S., & Zaidi, A. (2022). Exploring Health Impacts of Occupational Exposure to Carbon Monoxide in the Labour Community of Hattar Industrial Estate. Atmosphere, 13(3), 406. https://doi.org/10.3390/atmos13030406