
Effects of Speleotherapy on Aerobiota: A Case Study from the Sežana Hospital Cave, Slovenia


Abstract
:1. Introduction
2. Materials and Methods
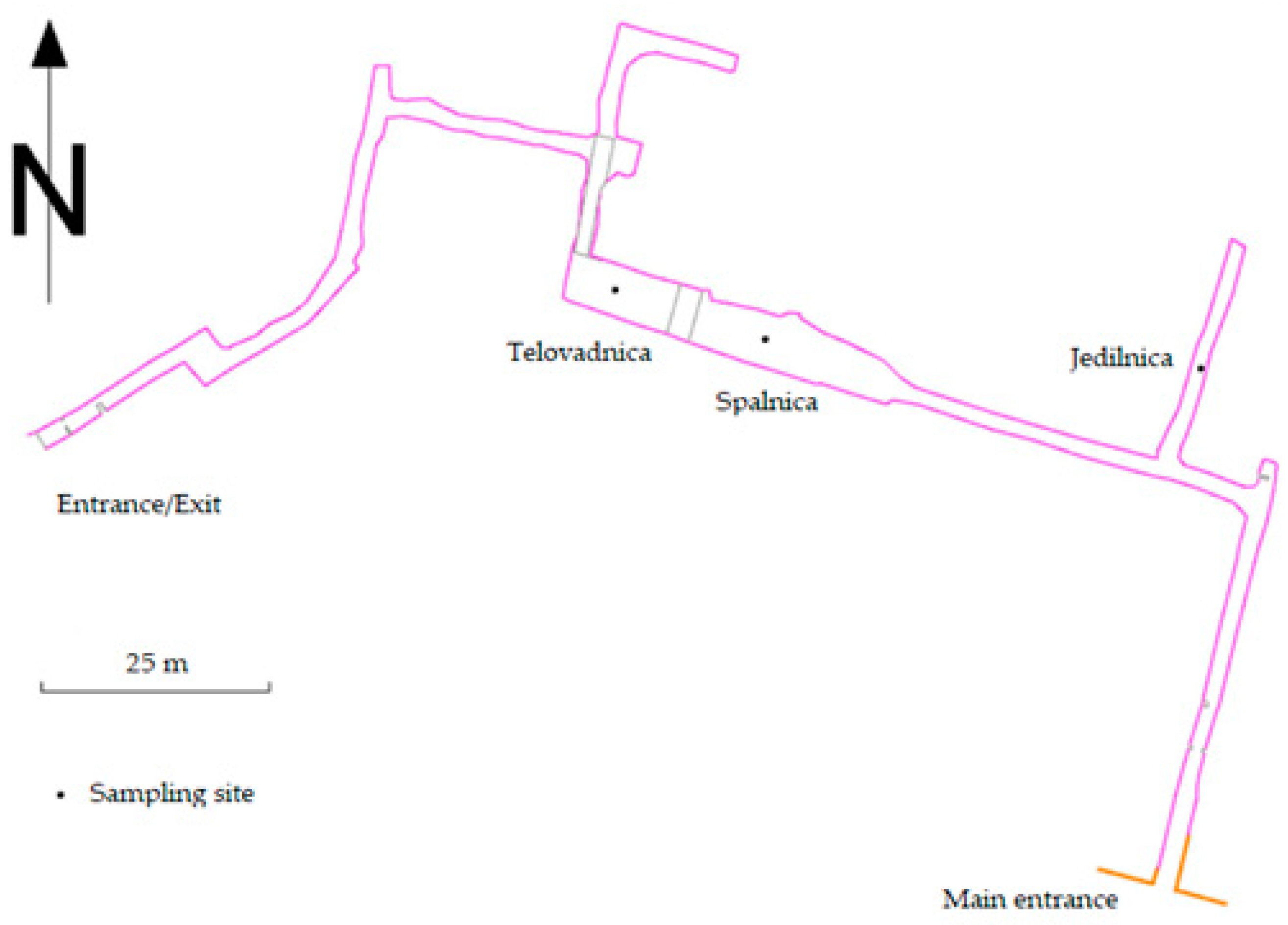
2.1. Sampling Sites
2.2. Air Sampling and Measurement of Environmental Parameters
2.3. Microbial Cultivation
2.3.1. Microbial Cultivation after Sampling with the Impactor
2.3.2. Microbial Cultivation after Sampling with the Impinger
2.4. Microbial Identification
2.5. Statistical Analysis
3. Results
3.1. Environmental Parameters
3.2. Quantification and Identification of Culturable Airborne Microorganisms
3.3. Identification of Culturable Airborne Microorganisms
3.4. Microbial Indicators of Cave Anthropization
3.5. Outdoor Air
4. Discussion
4.1. Environmental Parameters
4.2. Culturable Airborne Microorganisms and Speleotherapeutic Activities
4.3. Comparison of Air Sampling Methods
4.4. Cave Anthropization
4.5. MALDI-TOF MS Identification Success Rate
4.6. Culturable Microorganisms and Potential Indicators of Human Impact
4.7. Pathogenic Microorganisms in Cave Aerobiota
4.8. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Labaki, W.W.; Han, M.K. Chronic Respiratory Diseases: A Global View. Lancet Respir. Med. 2020, 8, 531–533. [Google Scholar] [CrossRef] [PubMed]
- Clemente-Suárez, V.J.; Mielgo-Ayuso, J.; Ramos-Campo, D.J.; Beltran-Velasco, A.I.; Martínez-Guardado, I.; Navarro Jimenez, E.; Redondo-Flórez, L.; Yáñez-Sepúlveda, R.; Tornero-Aguilera, J.F. Basis of Preventive and Non-Pharmacological Interventions in Asthma. Front. Public Health 2023, 11, 1172391. [Google Scholar] [CrossRef] [PubMed]
- Linneberg, A.; Dam Petersen, K.; Hahn-Pedersen, J.; Hammerby, E.; Serup-Hansen, N.; Boxall, N. Burden of Allergic Respiratory Disease: A Systematic Review. Clin. Mol. Allergy 2016, 14, 12. [Google Scholar] [CrossRef] [PubMed]
- Miravitlles, M.; Vogelmeier, C.; Roche, N.; Halpin, D.; Cardoso, J.; Chuchalin, A.G.; Kankaanranta, H.; Sandström, T.; Śliwiński, P.; Zatloukal, J. A Review of National Guidelines for Management of COPD in Europe. Eur. Respir. J. 2016, 47, 625–637. [Google Scholar] [CrossRef] [PubMed]
- López-Campos, J.L.; Ruiz-Ramos, M.; Soriano, J.B. Mortality Trends in Chronic Obstructive Pulmonary Disease in Europe, 1994–2010: A Joinpoint Regression Analysis. Lancet Respir. Med. 2014, 2, 54–62. [Google Scholar] [CrossRef] [PubMed]
- ur Rehman, A.; Hassali, M.A.A.; Abbas, S.; Ali, I.A.B.H.; Harun, S.N.; Muneswarao, J.; Hussain, R. Pharmacological and Non-Pharmacological Management of COPD; Limitations and Future Prospects: A Review of Current Literature. J. Public Health 2020, 28, 357–366. [Google Scholar] [CrossRef]
- Tong, S.; Yin, Y.; Bao, Y. Climatotherapy for Asthma: Research Progress and Prospect. Environ. Res. 2022, 214, 113988. [Google Scholar] [CrossRef] [PubMed]
- Lăzărescu, H.; Simionca, I.; Hoteteu, M.; Mirescu, L. Speleotherapy–Modern Bio-Medical Perspectives. J. Med. Life 2014, 7, 76. [Google Scholar]
- Kim, K.-H.; Kabir, E.; Jahan, S.A. Airborne Bioaerosols and Their Impact on Human Health. J. Environ. Sci. 2018, 67, 23–35. [Google Scholar] [CrossRef]
- GSJ, S.; Ramakodi, M.P.; TVBPS, R. Review of Bioaerosols from Different Sources and Their Health Impacts. Environ. Monit. Assess. 2023, 195, 1321. [Google Scholar]
- D’Amato, G.; Vitale, C.; Sanduzzi, A.; Molino, A.; Vatrella, A.; D’Amato, M. Allergenic Pollen and Pollen Allergy in Europe. In Allergy and Allergen Immunotherapy; Apple Academic Press: Palm Bay, FL, USA, 2017; pp. 287–306. [Google Scholar]
- Horvath, T. Speleotherapy: A Special Kind of Climatotherapy, Its Role in Respiratory Rehabilitation. Int. Rehabil. Med. 1986, 8, 90–92. [Google Scholar] [CrossRef]
- Puryshev, E.A. The Efficacy of Speleotherapy in Atopic Dermatitis in Children. Vopr. Kurortol. Fizioter. I Lech. Fiz. Kult. 1994, 4, 34–35. [Google Scholar]
- Munteanu, C.; Munteanu, D.; Simionca, I.; Hoteteu, M. Morphological and Electrophoretic Data about Heterogeneous Primary Skin Cells Cultures Obtained from Normal and Ovalbumin-Challenged Wistar Rats after Treatment by Speleotherapy in the Cacica and Dej Romanian Salt Mines. Balneo-Res. J. 2010, 1. Available online: https://bioclima.ro/J14.pdf (accessed on 8 March 2024). [CrossRef]
- Freidl, J.; Huber, D.; Braunschmid, H.; Romodow, C.; Pichler, C.; Weisböck-Erdheim, R.; Mayr, M.; Hartl, A. Winter Exercise and Speleotherapy for Allergy and Asthma: A Randomized Controlled Clinical Trial. J. Clin. Med. 2020, 9, 3311. [Google Scholar] [CrossRef] [PubMed]
- Munteanu, C. SPELEOTHERAPY-Scientific Relevance in the Last Five Years (2013–2017)–A Systematic Review. Balneo Res. J. 2017, 8, 252–254. [Google Scholar] [CrossRef]
- Eslaminejad, A.; Taghavi, K.; Zohal, M.; Kialashaki, M.; Fakharian, A. Speleotherapy as an Effective Treatment of Chronic Obstructive Pulmonary Disease. J. Respir. Med. Lung Dis. 2017, 2, 1029. [Google Scholar]
- Wasik, A.A.; Tuuminen, T. Salt Therapy as a Complementary Method for the Treatment of Respiratory Tract Diseases, With a Focus on Mold-Related Illness. Altern. Ther. Health Med. 2021, 27, 233. [Google Scholar]
- Beamon, S.P.; Falkenbach, A.; Fainburg, G.; Linde, K.; Group, C.A. Speleotherapy for Asthma. Cochrane Database Syst. Rev. 1996, 2019. [Google Scholar] [CrossRef]
- Hubelova, D.; Ulmann, V.; Mikuska, P.; Licbinsky, R.; Alexa, L.; Modra, H.; Gersl, M.; Babak, V.; Weston, R.T.; Pavlik, I. Nontuberculous Mycobacteria Prevalence in Aerosol and Spiders’ Webs in Karst Caves: Low Risk for Speleotherapy. Microorganisms 2021, 9, 2573. [Google Scholar] [CrossRef]
- Mętel, S.; Kostrzon, M.; Adamiak, J.; Gattner, H.; Kościelecka, D.; Sosulska, A.; Szczygieł, E.; Golec, J. The Influence of Speleotherapy Combined with Pulmonary Rehabilitation on Functional Fitness in Older Adults–Preliminary Report. Ther. Adv. Respir. Dis. 2020, 14, 1753466620926952. [Google Scholar] [CrossRef]
- Kertész, Z.; Borbély-Kiss, I.; Hunyadi, I. Study of Aerosols Collected in a Speleotherapeutic Cave Situated below Budapest, Hungary. Nucl. Instrum. Methods Phys. Res. Sect. B Beam Interact. Mater. At. 1999, 150, 384–391. [Google Scholar] [CrossRef]
- Cristofori, A.; Cristofolini, F.; Gottardini, E. Rare Occurrence of Airborne Bioparticles in a Speleotherapy Site: The Case Study of the Sant’Aloisio Disused Siderite Mine (Brescia, Italy). Aerobiologia 2020, 36, 125–130. [Google Scholar] [CrossRef]
- Iqbal, M.A.; Siddiqua, S.A.; Faruk, M.O.; Islam, A.R.M.T.; Salam, M.A. Systematic Review and Meta-Analysis of the Potential Threats to Respiratory Health from Microbial Bioaerosol Exposures. Environ. Pollut. 2023, 341, 122972. [Google Scholar] [CrossRef]
- Fraczek, K.; Górny, R.L. Microbial Air Quality at Szczawnica Sanatorium, Poland. Ann. Agric. Environ. Med. 2011, 18, 63–71. [Google Scholar]
- Bercea, S.; Năstase-Bucur, R.; Mirea, I.C.; Măntoiu, D.Ş.; Kenesz, M.; Petculescu, A.; Baricz, A.; Andrei, A.-Ş.; Banciu, H.L.; Papp, B. Novel Approach to Microbiological Air Monitoring in Show Caves. Aerobiologia 2018, 34, 445–468. [Google Scholar] [CrossRef]
- Tomazin, R.; Simčič, S.; Stopinšek, S.; Kopitar, A.N.; Kukec, A.; Matos, T.; Mulec, J. Effects of Anthropogenic Disturbance and Seasonal Variation on Aerobiota in Highly Visited Show Caves in Slovenia. Microorganisms 2023, 11, 2381. [Google Scholar] [CrossRef]
- Del Rosal, Y.; Liñán, C.; Hernández-Mariné, M. The Conservation of the Nerja Cave: Preserving Anthropogenic Impact in a Tourist Cave. In The Conservation of Subterranean Cultural Heritage; CRC Press/Balkema: Leide, Germany, 2014; pp. 193–206. [Google Scholar]
- Škerlj, A. Oblikovanje Speleoterapevtskega Parka Pri Bolnišnici Sežana/Designing a Speleotherapy Park by Sežana Hospital. Master’s Thesis, Biotechnical Faculty, University of Ljubljana, Ljubljana, Slovenia, 2015. [Google Scholar]
- Mulec, J.; Skok, S.; Tomazin, R.; Letić, J.; Pliberšek, T.; Stopinšek, S.; Simčič, S. Long-Term Monitoring of Bioaerosols in an Environment without UV and Desiccation Stress, an Example from the Cave Postojnska Jama, Slovenia. Microorganisms 2023, 11, 809. [Google Scholar] [CrossRef]
- Walsh, T.J.; Hayden, R.T.; Larone, D.H. Larone’s Medically Important Fungi: A Guide to Identification; John Wiley & Sons: Hoboken, NJ, USA, 2018; ISBN 1-68367-296-8. [Google Scholar]
- Hoog, G.S. Atlas of Clinical Fungi: The Ultimate Benchtool for Diagnostics; Foundation Atlas of Clinical Fungi: Hilversum, The Netherlands, 2020; ISBN 94-93226-12-3. [Google Scholar]
- Wilson, M. The Human Microbiota in Health and Disease: An Ecological and Community-Based Approach; Garland Science: New York, NY, USA, 2018. [Google Scholar]
- Savini, V.; Catavitello, C.; Onofrillo, D.; Masciarelli, G.; Astolfi, D.; Balbinot, A.; Febbo, F.; D’Amario, C.; D’Antonio, D. What Do We Know about Candida Guilliermondii? A Voyage throughout Past and Current Literature about This Emerging Yeast. Mycoses 2011, 54, 434–441. [Google Scholar] [CrossRef] [PubMed]
- Murray, P.R.; Rosenthal, K.S.; Pfaller, M.A. Medical Microbiology E-Book; Elsevier Health Sciences: London, UK, 2020; ISBN 0-323-67450-X. [Google Scholar]
- Hansel, N.N.; McCormack, M.C.; Kim, V. The Effects of Air Pollution and Temperature on COPD. COPD J. Chronic Obstr. Pulm. Dis. 2016, 13, 372–379. [Google Scholar] [CrossRef]
- Shoraka, H.R.; Soodejani, M.T.; Abobakri, O.; Khanjani, N. The Relation between Ambient Temperature and Asthma Exacerbation in Children: A Systematic Review. J. Lung Health Dis. 2019, 3, 1–9. [Google Scholar] [CrossRef]
- Hayes Jr, D.; Collins, P.B.; Khosravi, M.; Lin, R.-L.; Lee, L.-Y. Bronchoconstriction Triggered by Breathing Hot Humid Air in Patients with Asthma: Role of Cholinergic Reflex. Am. J. Respir. Crit. Care Med. 2012, 185, 1190–1196. [Google Scholar] [CrossRef] [PubMed]
- Internationales Symposium für Speläotherapie 9, 1987; Trimmel, H. Akten Des 9. Internationalen Symposiums Für Speläotherapie: Bad Bleiberg (Kärnten), September 1987, Verb. Österr. Höhlenforscher. 1992.
- Constantin, S.; Mirea, I.C.; Petculescu, A.; Arghir, R.A.; Măntoiu, D.Ș.; Kenesz, M.; Robu, M.; Moldovan, O.T. Monitoring Human Impact in Show Caves. A Study of Four Romanian Caves. Sustainability 2021, 13, 1619. [Google Scholar] [CrossRef]
- Forbes, J. Air Temperature and Relative Humidity Study: Torgac Cave, New Mexico. J. Caves Karst Stud. 1998, 60, 27–32. [Google Scholar]
- Bodaghkhani, E.; Mahdavian, M.; MacLellan, C.; Farrell, A.; Asghari, S. Effects of Meteorological Factors on Hospitalizations in Adult Patients with Asthma: A Systematic Review. Can. Respir. J. 2019, 2019, 3435103. [Google Scholar] [CrossRef] [PubMed]
- Lunghi, E.; Manenti, R.; Ficetola, G.F. Cave Features, Seasonality and Subterranean Distribution of Non-Obligate Cave Dwellers. PeerJ 2017, 5, e3169. [Google Scholar] [CrossRef] [PubMed]
- Smetanová, I.; Holý, K.; Luhová, Ľ.; Csicsay, K.; Haviarová, D.; Kunáková, L. Seasonal Variation of Radon and CO2 in the Važecká Cave, Slovakia. Nukleonika 2020, 65, 153–157. [Google Scholar] [CrossRef]
- Prelovšek, M.; Šebela, S.; Turk, J. Carbon Dioxide in Postojna Cave (Slovenia): Spatial Distribution, Seasonal Dynamics and Evaluation of Plausible Sources and Sinks. Environ. Earth Sci. 2018, 77, 289. [Google Scholar] [CrossRef]
- Lang, M.; Faimon, J.; Pracný, P.; Kejíková, S. A Show Cave Management: Anthropogenic CO2 in Atmosphere of Výpustek Cave (Moravian Karst, Czech Republic). J. Nat. Conserv. 2017, 35, 40–52. [Google Scholar] [CrossRef]
- Lang, M.; Faimon, J.; Godissart, J.; Ek, C. Carbon Dioxide Seasonality in Dynamically Ventilated Caves: The Role of Advective Fluxes. Theor. Appl. Climatol. 2017, 129, 1355–1372. [Google Scholar] [CrossRef]
- Siani, R.; Stabl, G.; Gutjahr, C.; Schloter, M.; Radl, V. Acidovorax Pan-Genome Reveals Specific Functional Traits for Plant Beneficial and Pathogenic Plant-Associations. Microb. Genom. 2021, 7, 000666. [Google Scholar] [CrossRef]
- Cosseau, C.; Romano-Bertrand, S.; Duplan, H.; Lucas, O.; Ingrassia, I.; Pigasse, C.; Roques, C.; Jumas-Bilak, E. Proteobacteria from the Human Skin Microbiota: Species-Level Diversity and Hypotheses. One Health 2016, 2, 33–41. [Google Scholar] [CrossRef] [PubMed]
- Mulec, J.; Oarga-Mulec, A.; Šturm, S.; Tomazin, R.; Matos, T. Spacio-Temporal Distribution and Tourist Impact on Airborne Bacteria in a Cave (Škocjan Caves, Slovenia). Diversity 2017, 9, 28. [Google Scholar] [CrossRef]
- Lodge, J.P. Methods of Air Sampling and Analysis; Routledge: New York, NY, USA, 2017; ISBN 0-203-74740-2. [Google Scholar]
- Kabir, E.; Azzouz, A.; Raza, N.; Bhardwaj, S.K.; Kim, K.-H.; Tabatabaei, M.; Kukkar, D. Recent Advances in Monitoring, Sampling, and Sensing Techniques for Bioaerosols in the Atmosphere. ACS Sens. 2020, 5, 1254–1267. [Google Scholar] [CrossRef] [PubMed]
- IWC Authority. Linee Guida Sugli Standard Di Sicurezza e Di Igiene Del Lavoro Nel Reparto Operatorio; Istituto Superiore per la Prevenzione e la Sicurezza del Lavoro, Dipartimento Igiene del Lavoro (ISPESL): Rome, Italy, 2009. [Google Scholar]
- Sandle, T. EU GMP Annex 1: Manufacture of Sterile Medicinal Products; European Commission: Brussels, Belgium, 2022. [Google Scholar]
- Tomazin, R.; Matos, T. Mycological Methods for Routine Air Sampling and Interpretation of Results in Operating Theaters. Diagnostics 2024, 14, 288. [Google Scholar] [CrossRef]
- Pasquarella, C.; Vitali, P.; Saccani, E.; Manotti, P.; Boccuni, C.; Ugolotti, M.; Signorelli, C.; Mariotti, F.; Sansebastiano, G.E.; Albertini, R. Microbial Air Monitoring in Operating Theatres: Experience at the University Hospital of Parma. J. Hosp. Infect. 2012, 81, 50–57. [Google Scholar] [CrossRef] [PubMed]
- ISO 14698-1; Cleanrooms and Associated Controlled Environments–Biocontamination Control, Part 1: General Principles and Methods. ISO Standard. International Organization for Standardization: Geneva, Switzerland, 2003.
- Calin, M.R.; Simionca, I.G.; Radulescu, I. Natural Therapeutic Factors Assessment for the Use in Speleotherapeutic Purposes of the Cacica Saline Mine, Romania. Rom. Rep. Phys. 2021, 73, 801. [Google Scholar]
- Chinn, R.Y.; Sehulster, L. Guidelines for Environmental Infection Control in Health-Care Facilities: Recommendations of CDC and Healthcare Infection Control Practices Advisory Committee (HICPAC). Morb. Mortal Wkly. Rep. 2003, 52. Available online: https://www.cdc.gov/mmwr/preview/mmwrhtml/rr5210a1.htm?fbclid=IwAR2fLaoYktAcxp7Mu9ngotP1FfdrJBBWE9Gtg5nGOjhTDrMIft46un3iQtU (accessed on 8 March 2024).
- Fleischer, M.; Bober-Gheek, B.; Bortkiewicz, O.; Rusiecka-Ziólkowskaa, J. Microbiological Control of Airborne Contamination in Hospitals. Indoor Built Environ. 2006, 15, 53–56. [Google Scholar] [CrossRef]
- Bhatia, L.; Vishwakarma, R. Hospital Indoor Airborne Microflora in Private and Government-Owned Hospitals in Sagar City, India. World J. Med. Sci. 2010, 5, 65–70. [Google Scholar]
- Alonso, L.; Pommier, T.; Kaufmann, B.; Dubost, A.; Chapulliot, D.; Doré, J.; Douady, C.J.; Moënne-Loccoz, Y. Anthropization Level of Lascaux Cave Microbiome Shown by Regional-scale Comparisons of Pristine and Anthropized Caves. Mol. Ecol. 2019, 28, 3383–3394. [Google Scholar] [CrossRef]
- Biagioli, F.; Coleine, C.; Piano, E.; Nicolosi, G.; Poli, A.; Prigione, V.; Zanellati, A.; Varese, C.; Isaia, M.; Selbmann, L. Microbial Diversity and Proxy Species for Human Impact in Italian Karst Caves. Sci. Rep. 2023, 13, 689. [Google Scholar] [CrossRef] [PubMed]
- Mulec, J. Human Impact on Underground Cultural and Natural Heritage Sites, Biological Parameters of Monitoring and Remediation Actions for Insensitive Surfaces: Case of Slovenian Show Caves. J. Nat. Conserv. 2014, 22, 132–141. [Google Scholar] [CrossRef]
- Bontemps, Z.; Alonso, L.; Pommier, T.; Hugoni, M.; Moënne-Loccoz, Y. Microbial Ecology of Tourist Paleolithic Caves. Sci. Total Environ. 2022, 816, 151492. [Google Scholar] [CrossRef] [PubMed]
- Licbinsky, R.; Faimon, J.; Tanda, S.; Hegrova, J.; Goessler, W.; Uberhuberova, J. Changes in the Elemental Composition of Particulate Matter in a Speleotherapeutic Cave. Atmos. Pollut. Res. 2020, 11, 1142–1154. [Google Scholar] [CrossRef]
- Porca, E.; Jurado, V.; Martin-Sanchez, P.M.; Hermosin, B.; Bastian, F.; Alabouvette, C.; Saiz-Jimenez, C. Aerobiology: An Ecological Indicator for Early Detection and Control of Fungal Outbreaks in Caves. Ecol. Indic. 2011, 11, 1594–1598. [Google Scholar] [CrossRef]
- Ashfaq, M.Y.; Da’na, D.A.; Al-Ghouti, M.A. Application of MALDI-TOF MS for Identification of Environmental Bacteria: A Review. J. Environ. Manag. 2022, 305, 114359. [Google Scholar] [CrossRef] [PubMed]
- Rychert, J. Benefits and Limitations of MALDI-TOF Mass Spectrometry for the Identification of Microorganisms. J. Infect. Epidemiol. 2019, 2. [Google Scholar] [CrossRef]
- Mudgil, D.; Paul, D.; Baskar, S.; Baskar, R.; Shouche, Y.S. Cultivable Microbial Diversity in Speleothems Using MALDI-TOF Spectrometry and DNA Sequencing from Krem Soitan, Krem Lawbah, Krem Mawpun, Khasi Hills, Meghalaya, India. Arch. Microbiol. 2022, 204, 495. [Google Scholar] [CrossRef] [PubMed]
- Bielen, A.; Babić, I.; Vuk Surjan, M.; Kazazić, S.; Šimatović, A.; Lajtner, J.; Udiković-Kolić, N.; Mesić, Z.; Hudina, S. Comparison of MALDI-TOF Mass Spectrometry and 16S RDNA Sequencing for Identification of Environmental Bacteria: A Case Study of Cave Mussel-Associated Culturable Microorganisms. Environ. Sci. Pollut. Res. 2024, 31, 21752–21764. [Google Scholar] [CrossRef] [PubMed]
- Kato, N.N.; Arini, G.S.; Silva, R.R.; Bichuette, M.E.; Bitencourt, J.A.P.; Lopes, N.P. The World of Cave Microbiomes: Biodiversity, Ecological Interactions, Chemistry, and the Multi-Omics Integration. J. Braz. Chem. Soc. 2024, 35, e-20230148. [Google Scholar] [CrossRef]
- Jurado, V.; Laiz, L.; Rodriguez-Nava, V.; Boiron, P.; Hermosin, B.; Sanchez-Moral, S.; Saiz-Jimenez, C. Pathogenic and Opportunistic Microorganisms in Caves. Int. J. Speleol. 2010, 39, 2. [Google Scholar] [CrossRef]
- Adetutu, E.M.; Thorpe, K.; Shahsavari, E.; Bourne, S.; Cao, X.; Mazaheri Nezhad Fard, R.; Kirby, G.; Ball, A.S. Bacterial Community Survey of Sediments at Naracoorte Caves, Australia. Int. J. Speleol. 2012, 41, 2. [Google Scholar] [CrossRef]
- Ikner, L.A.; Toomey, R.S.; Nolan, G.; Neilson, J.W.; Pryor, B.M.; Maier, R.M. Culturable Microbial Diversity and the Impact of Tourism in Kartchner Caverns, Arizona. Microb. Ecol. 2007, 53, 30–42. [Google Scholar] [CrossRef]
- Martin-Sanchez, P.M.; Jurado, V.; Porca, E.; Bastian, F.; Lacanette, D.; Alabouvette, C.; Saiz-Jimenez, C. Airborne Microorganisms in Lascaux Cave (France). Int. J. Speleol. 2014, 43, 295–303. [Google Scholar] [CrossRef]
- Yasir, M. Analysis of Bacterial Communities and Characterization of Antimicrobial Strains from Cave Microbiota. Braz. J. Microbiol. 2018, 49, 248–257. [Google Scholar] [CrossRef]
- Dominguez-Moñino, I.; Jurado, V.; Rogerio-Candelera, M.A.; Hermosin, B.; Saiz-Jimenez, C. Airborne Bacteria in Show Caves from Southern Spain. Microb. Cell 2021, 8, 247. [Google Scholar] [CrossRef] [PubMed]
- Lavoie, K.H.; Northup, D.E. Bacteria as Indicators of Human Impact in Caves. In Proceedings of the 17th National Cave and Karst Management Symposium, Albany, NY, USA, 31 October–4 November 2005; The NCKMS Steering Committee: Albany, NY, USA, 2006; pp. 40–47. Available online: https://nckms.org/wp-content/uploads/2018/05/2005_lavoie-bacteria.pdf (accessed on 8 March 2024).
- Kloos, W.E.; Musselwhite, M.S. Distribution and Persistence of Staphylococcus and Micrococcus Species and Other Aerobic Bacteria on Human Skin. Appl. Microbiol. 1975, 30, 381–395. [Google Scholar] [CrossRef]
- Al Atrouni, A.; Joly-Guillou, M.-L.; Hamze, M.; Kempf, M. Reservoirs of Non-Baumannii Acinetobacter Species. Front. Microbiol. 2016, 7, 49. [Google Scholar] [CrossRef]
- Svec, P.; Devriese, L.A.; Sedlácek, I.; Baele, M.; Vancanneyt, M.; Haesebrouck, F.; Swings, J.; Doskar, J. Enterococcus Haemoperoxidus Sp. Nov. and Enterococcus Moraviensis Sp. Nov., Isolated from Water. Int. J. Syst. Evol. Microbiol. 2001, 51, 1567–1574. [Google Scholar] [CrossRef] [PubMed]
- Hong, H.A.; To, E.; Fakhry, S.; Baccigalupi, L.; Ricca, E.; Cutting, S.M. Defining the Natural Habitat of Bacillus Spore-Formers. Res. Microbiol. 2009, 160, 375–379. [Google Scholar] [CrossRef]
- Ropars, J.; Didiot, E.; de La Vega, R.C.R.; Bennetot, B.; Coton, M.; Poirier, E.; Coton, E.; Snirc, A.; Le Prieur, S.; Giraud, T. Domestication of the Emblematic White Cheese-Making Fungus Penicillium Camemberti and Its Diversification into Two Varieties. Curr. Biol. 2020, 30, 4441–4453.e4. [Google Scholar] [CrossRef] [PubMed]
- Yadav, A.N.; Verma, P.; Kumar, V.; Sangwan, P.; Mishra, S.; Panjiar, N.; Gupta, V.K.; Saxena, A.K. Biodiversity of the Genus Penicillium in Different Habitats. In New and Future Developments in Microbial Biotechnology and Bioengineering; Elsevier: Amsterdam, The Netherlands, 2018; pp. 3–18. [Google Scholar]
- Poli, A.; Zanellati, A.; Piano, E.; Biagioli, F.; Coleine, C.; Nicolosi, G.; Selbmann, L.; Isaia, M.; Prigione, V.; Varese, G.C. Cultivable Fungal Diversity in Two Karstic Caves in Italy: Under-Investigated Habitats as Source of Putative Novel Taxa. Sci. Rep. 2024, 14, 4164. [Google Scholar] [CrossRef] [PubMed]
- Shah, P. A Review of Salt Therapy as a Complementary Treatment for Enhancing Respiratory Wellness and Skin Ailment. Indian Pract. 2019, 72, 28–32. [Google Scholar]
- Faimon, J.; Ličbinský, R.; Lang, M.; Überhuberová, J.; Hebelka, J. Cave Microclimatology: Diurnal Variations in Aerosol Particle Concentrations. Theor. Appl. Climatol. 2019, 137, 2841–2852. [Google Scholar] [CrossRef]
- LEMKO, O.; LEMKO, I. Haloaerosoltherapy: Mechanisms of Curative Effect and Place in the Respiratory Rehabilitation. Balneo PRM Res. J. 2021, 12, 365–375. [Google Scholar] [CrossRef]
- Tanda, S.; Ličbinský, R.; Hegrová, J.; Faimon, J.; Goessler, W. Arsenic Speciation in Aerosols of a Respiratory Therapeutic Cave: A First Approach to Study Arsenicals in Ultrafine Particles. Sci. Total Environ. 2019, 651, 1839–1848. [Google Scholar] [CrossRef]
- Myszkowska, D.; Kostrzon, M.; Dyga, W.; Kędzierska, J.; Namysł, M.; Stanisz, A.; Zagórska, M.; Ziemianin, M.; Obtułowicz, K.; Czarnobilska, E. Bioaerosol of Salt Chambers in the ‘Wieliczka’Salt Mine, Poland. Aerobiologia 2019, 35, 297–311. [Google Scholar] [CrossRef]
- Ferri, S.; Crimi, C.; Campisi, R.; Cacopardo, G.; Paoletti, G.; Puggioni, F.; Crimi, N.; Heffler, E. Impact of Asthma on Bronchiectasis Severity and Risk of Exacerbations. J. Asthma 2022, 59, 469–475. [Google Scholar] [CrossRef]
- Viniol, C.; Vogelmeier, C.F. Exacerbations of COPD. Eur. Respir. Rev. 2018, 27, 170103. [Google Scholar] [CrossRef]
- Tiew, P.Y.; San Ko, F.W.; Pang, S.L.; Matta, S.A.; Sio, Y.Y.; Poh, M.E.; Lau, K.J.; Mac Aogáin, M.; Jaggi, T.K.; Ivan, F.X. Environmental Fungal Sensitisation Associates with Poorer Clinical Outcomes in COPD. Eur. Respir. J. 2020, 56, 2000418. [Google Scholar] [CrossRef]
- Tiwary, M.; Samarasinghe, A.E. Initiation and Pathogenesis of Severe Asthma with Fungal Sensitization. Cells 2021, 10, 913. [Google Scholar] [CrossRef] [PubMed]
- Kramer, C.D.; Genco, C.A. Microbiota, Immune Subversion, and Chronic Inflammation. Front. Immunol. 2017, 8, 255. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Ran, Z.; Wang, F.; Xin, C.; Xiong, B.; Song, Z. Role of Pulmonary Microorganisms in the Development of Chronic Obstructive Pulmonary Disease. Crit. Rev. Microbiol. 2021, 47, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Górny, R.L.; Frączek, K.; Ropek, D.R. Size Distribution of Microbial Aerosols in Overground and Subterranean Treatment Chambers at Health Resorts. J. Environ. Health Sci. Eng. 2020, 18, 1437–1450. [Google Scholar] [CrossRef] [PubMed]
- Murrison, L.B.; Brandt, E.B.; Myers, J.B.; Hershey, G.K.K. Environmental Exposures and Mechanisms in Allergy and Asthma Development. J. Clin. Investig. 2019, 129, 1504–1515. [Google Scholar] [CrossRef] [PubMed]
- Jusufovic, E. Molds as a Cause of Asthma and Exacerbations. J. Lung Pulm. Respir. Res. 2022, 9, 94–98. [Google Scholar] [CrossRef]
- Hammond, E.E.; McDonald, C.S.; Vestbo, J.; Denning, D.W. The Global Impact of Aspergillus Infection on COPD. BMC Pulm. Med. 2020, 20, 241. [Google Scholar] [CrossRef]
- Knutsen, A.P. Allergic Bronchopulmonary Aspergillosis in Asthma. Expert Rev. Clin. Immunol. 2017, 13, 11–14. [Google Scholar] [CrossRef]
- Knutsen, A.P. Allergic Aspects of Aspergillosis. Curr. Fungal Infect. Rep. 2013, 7, 334–344. [Google Scholar] [CrossRef]
- Kozlova, E.V.; Mazina, S.E. Biodiversity of Fungi in the Photic and Aphotic Zones of Montenegro Caves. Aerobiologia 2020, 36, 589–604. [Google Scholar] [CrossRef]
- Dominguez-Moñino, I.; Jurado, V.; Rogerio-Candelera, M.A.; Hermosin, B.; Saiz-Jimenez, C. Airborne Fungi in Show Caves from Southern Spain. Appl. Sci. 2021, 11, 5027. [Google Scholar] [CrossRef]
- Frączek, K.; Górny, R.L.; Ropek, D. Bioaerosols of Subterraneotherapy Chambers at Salt Mine Health Resort. Aerobiologia 2013, 29, 481–493. [Google Scholar] [CrossRef]
- Reboux, G.; Rocchi, S.; Vacheyrou, M.; Millon, L. Identifying Indoor Air Penicillium Species: A Challenge for Allergic Patients. J. Med. Microbiol. 2019, 68, 812–821. [Google Scholar] [CrossRef]
- Méheust, D.; Le Cann, P.; Reboux, G.; Millon, L.; Gangneux, J.-P. Indoor Fungal Contamination: Health Risks and Measurement Methods in Hospitals, Homes and Workplaces. Crit. Rev. Microbiol. 2014, 40, 248–260. [Google Scholar] [CrossRef] [PubMed]
- Hänninen, O.O. WHO Guidelines for Indoor Air Quality: Dampness and Mold. In Fundamentals of Mold Growth in Indoor Environments and Strategies for Healthy Living; Wageningen Academic: Wageningen, The Netherlands, 2011; pp. 277–302. [Google Scholar]
- Wanner, H.; Verhoeff, A.; Colombi, A.; Flannigan, B.; Gravesen, S.; Mouilleseaux, A.; Nevalainen, A.; Papadakis, J.; Seidel, K. Indoor Air Quality and Its Impact on Man: Report No. 12: Biological Particles in Indoor Environments; Brussels-Luxembourg: ECSC-EEC-EAEC; Publications Office of the European Union: Luxembourg, 1993. [Google Scholar]
- Wilkendorf, L.S.; Bowles, E.; Buil, J.B.; van der Lee, H.A.; Posteraro, B.; Sanguinetti, M.; Verweij, P.E. Update on Matrix-Assisted Laser Desorption Ionization–Time of Flight Mass Spectrometry Identification of Filamentous Fungi. J. Clin. Microbiol. 2020, 58. [Google Scholar] [CrossRef] [PubMed]
- Wang, P.; Sun, H.; Yang, W.; Fang, Y. Optical Methods for Label-Free Detection of Bacteria. Biosensors 2022, 12, 1171. [Google Scholar] [CrossRef] [PubMed]
- Eerola, E.; Lehtonen, O.-P. Optimal Data Processing Procedure for Automatic Bacterial Identification by Gas-Liquid Chromatography of Cellular Fatty Acids. J. Clin. Microbiol. 1988, 26, 1745–1753. [Google Scholar] [CrossRef]


{kind=link}
| Location | Before Therapeutic Activities | After Therapeutic Activities | |||||||
|---|---|---|---|---|---|---|---|---|---|
| T (°C) | CO2 (ppm) | RH (%) | Airflow (L/s) | T (°C) | CO2 (ppm) | RH (%) | Airflow (L/s) | ||
| Jedilnica | Mean | 15.0 | 1694.6 | 82.4 | 0.14 | 14.1 | 1528.3 | 93.7 | 0.20 |
| Minimum | 14.2 | 489.0 | 77.4 | 0.07 | 13.2 | 846.0 | 78.8 | 0.09 | |
| Maximum | 16.5 | 4757.9 | 84.6 | 0.21 | 16.2 | 2687.8 | 100.0 | 0.34 | |
| Standard deviation | 1.0 | 2048.4 | 3.4 | 0.06 | 1.4 | 810.1 | 10.1 | 0.10 | |
| Spalnica | Mean | 13.4 | 2112.8 | 93.3 | 0.17 | 13.8 | 1480.1 | 95.1 | 0.22 |
| Minimum | 13.0 | 457.3 | 90.6 | 0.09 | 13.1 | 939.0 | 88.7 | 0.00 | |
| Maximum | 14.1 | 6092.6 | 95.6 | 0.24 | 14.9 | 2121.6 | 100.0 | 0.52 | |
| Standard deviation | 0.5 | 2680.9 | 2.1 | 0.06 | 0.8 | 486.7 | 5.0 | 0.22 | |
| Telovadnica | Mean | 13.2 | 2219.8 | 96.9 | 0.16 | 13.4 | 1886.8 | 99.4 | 0.37 |
| Minimum | 12.8 | 508.0 | 93.4 | 0.01 | 13.0 | 1003.8 | 97.8 | 0.22 | |
| Maximum | 13.7 | 6160.7 | 99.4 | 0.41 | 13.9 | 2860.4 | 100.0 | 0.64 | |
| Standard deviation | 0.4 | 2673.7 | 2.5 | 0.18 | 0.4 | 792.6 | 1.1 | 0.19 | |
| SAS Duo Air Sampler | ||||||||
|---|---|---|---|---|---|---|---|---|
| Location | Date | Microbes—Before Patients (CFU/m3) | Microbes—After Patients (CFU/m3) | A/B Index—Microbial Load | No. of Microbial Species—Before Patients | No. of Microbial Species—After Patients | A/B Index—Species | No. of Patients and Staff |
| Jedilnica | 7 July 2020 | 102 | 354 | 3.5 | 10 | 10 | 1.1 | 15 |
| 27 November 2021 | 112 | 232 | 2.1 | 5 | 5 | 1.0 | 10 | |
| 2 June 2022 | 106 | 214 | 2.0 | 9 | 9 | 1.1 | 19 | |
| 10 January 2023 | 88 | 610 | 6.9 | 10 | 10 | 1.1 | 15 | |
| 10.2 * | 182.6 * | |||||||
| Spalnica | 7 July 2020 | 144 | 163 | 1.1 | 7 | 7 | 0.8 | 15 |
| 27 November 2021 | 143 | 185 | 1.3 | 4 | 4 | 1.3 | 10 | |
| 2 June 2022 | 64 | 218 | 3.4 | 7 | 7 | 0.6 | 19 | |
| 10 January 2023 | 54 | 138 | 2.6 | 8 | 8 | 1.1 | 15 | |
| 48.9 * | 33.9 * | |||||||
| Telovadnica | 7 July 2020 | 169 | 198 | 1.2 | 8 | 8 | 0.8 | 15 |
| 27 November 2021 | 202 | 148 | 0.7 | 3 | 3 | 0.6 | 10 | |
| 2 June 2022 | 152 | 190 | 1.3 | 11 | 11 | 1.4 | 19 | |
| 10 January 2023 | 96 | 650 | 6.8 | 7 | 7 | 0.9 | 15 | |
| 44.3 * | 236.7 * | |||||||
| Coriolis Air Sampler | ||||||||
|---|---|---|---|---|---|---|---|---|
| Microbes—Before Patients (CFU/m3) | Microbes—After Patients (CFU/m3) | A/B Index—Microbial Load | No. of Microbial Species—Before Patients | No. of Microbial Species—After Patients | A/B Index—Species | No. of Patients and Staff | ||
| Jedilnica | 7 July 2020 | 134 | 757 | 5.6 | 4 | 7 | 1.8 | 15 |
| 27 November 2021 | 50 | 3873 | 77.5 | 1 | 4 | 4.0 | 10 | |
| 2 June 2022 | 653 | 886 | 1.4 | 5 | 9 | 1.8 | 19 | |
| 10 January 2023 | 151 | 784 | 5.2 | 4 | 10 | 2.5 | 15 | |
| 274.2 * | 1533.0 * | |||||||
| Spalnica | 7 July 2020 | 217 | 518 | 2.4 | 5 | 3 | 0.6 | 15 |
| 27 November 2021 | 185 | 1820 | 9.8 | 3 | 4 | 1.3 | 10 | |
| 2 June 2022 | 818 | 435 | 0.5 | 8 | 7 | 0.9 | 19 | |
| 10 January 2023 | 304 | 951 | 3.1 | 8 | 5 | 0.6 | 15 | |
| 295.6 * | 634.4 * | |||||||
| Telovadnica | 7 July 2020 | 117 | 469 | 4.0 | 2 | 7 | 3.5 | 15 |
| 27 November 2021 | 2370 | 4558 | 1.9 | 2 | 4 | 2.0 | 10 | |
| 2 June 2022 | 501 | 301 | 0.6 | 5 | 5 | 1.0 | 19 | |
| 10 January 2023 | 317 | 934 | 2.9 | 5 | 6 | 1.2 | 15 | |
| 1041.0 * | 2012.9 * | |||||||
| Location | SAS Impactor (CFU/m3) | p | Coriolis Impinger (CFU/m3) | p | CO2 (ppm) | p | RH (%) | p | |
|---|---|---|---|---|---|---|---|---|---|
| Jedilnica | Before therapeutic activities | 104.0 | 0.068 | 142.5 | 0.068 | 765.8 | 0.715 | 83.8 | 0.068 |
| After therapeutic activities | 293.0 | 835.0 | 1289.7 | 97.9 | |||||
| Spalnica | Before therapaeutic activities | 103.5 | 0.068 | 260.5 | 0.273 | 950.60 | 0.715 | 93.5 | 0.465 |
| After therapeutic activities | 174.0 | 734.5 | 1429.9 | 95.9 | |||||
| Telovadnica | Before therapeutic activities | 160.5 | 0.465 | 409.0 | 0.144 | 1105.3 | 0.715 | 97.3 | 0.066 |
| Jedilnica | Spalnica | Telovadnica | Locations Combined | ||||||
|---|---|---|---|---|---|---|---|---|---|
| SAS | Coriolis | SAS | Coriolis | SAS | Coriolis | SAS | Coriolis | ||
| Non-identified microorganisms (CFU/m3) | Before patients | 412 | 550 | 514 | 622 | 472 | 751 | 1398 | 1923 |
| After patients | 288 | 2621 | 217 | 500 | 215 | 567 | 720 | 3688 | |
| All isolated microorganisms (CFU/m3) | Before patients | 850 | 1672 | 869 | 2041 | 953 | 3622 | 2672 | 7335 |
| After patients | 1410 | 6300 | 704 | 3743 | 1186 | 6262 | 3300 | 16,305 | |
| % of identified microorganisms | Before patients | 51.5 | 67.1 | 40.9 | 69.5 | 50.5 | 79.3 | 47.7 | 73.8 |
| After patients | 79.6 | 58.4 | 69.2 | 86.6 | 81.9 | 90.9 | 78.2 | 77.4 | |
| Microorganisms | Sampling Sites * | Risk Group (Country) | Human Microbiota |
|---|---|---|---|
| Bacteria | |||
| Aerococcus viridans | 1, 2 | 2 (BE, CH, DE) | skin, urinary tract |
| Corynebacterium amycolatum | 1 | 2 (CH, DE) | skin |
| Corynebacterium aurimucosum | 1, 3 | - | skin, vaginal mucosa |
| Kocuria marina | 1, 2 | - | skin |
| Kocuria palustris | 1, 2 | - | skin |
| Kocuria rhizophila | 2 | - | skin |
| Kocuria rosea | 1, 2, 3 | - | skin |
| Micrococcus luteus | 1, 2, 3 | 2 (BE, CH, DE, NIH) | skin |
| Rothia dentocariosa | 1 | - | oral mucosa |
| Staphylococcus capitis | 1, 2, 3 | - | skin, scalp |
| Staphylococcus cohnii | 1, 3 | - | skin |
| Staphylococcus epidermidis | 1, 2 | 2 (BE, CH, DE) | skin, nasopharynx |
| Staphylococcus haemolyticus | 2, 3 | 2 (CH, DE) | skin |
| Staphylococcus hominis | 1, 2, 3 | - | skin |
| Staphylococcus lugdunensis | 1, 2 | 2 (BE, CH, DE) | skin |
| Staphylococcus pettenkoferi | 1 | - | skin, urinary tract |
| Staphylococcus petrasii | 1 | - | skin |
| Staphylococcus saprophyticus | 2 | 2 (BE, CA, CH, DE) | skin |
| Staphylococcus schleiferi | 1 | 2 (BE, CH, DE) | skin |
| Staphylococcus warneri | 1, 2 | - | skin |
| Fungi | |||
| Cutaneotrichosporon dermatis | 2, 3 | - | skin |
| Meyerozyma guilliermondii | 1, 2, 3 | 2 (EU, UK) | skin, intestinal tract |
| Microbial Concentration (CFU/m3) | |||||
|---|---|---|---|---|---|
| Bacteria | 29 May 2020 | 7 July 2020 | 27 November 2021 | 2 June 2022 | 10 January 2023 |
| Arthrobacter parietis | NP | NP | 4 | NP | 2 |
| Bacillus pumilus | NP | NP | 4 | NP | 6 |
| Pantoea eucrina | NP | 2 | NP | NP | 4 |
| Paenarthrobacter ilicis | NP | NP | 4 | NP | NP |
| Fungi | NP | NP | NP | NP | NP |
| Aspergillus fumigatus * | 4 | 2 | 4 | 2 | 4 |
| Aspergillus flavus * | NP | 2 | NP | 2 | 4 |
| Aspergillus glaucus * | NP | NP | 8 | NP | 12 |
| Cladosporium * sp. | 20 | 20 | 28 | 26 | 24 |
| Penicillium brevicompactum * | 2 | 4 | 6 | 4 | 8 |
| Penicillium italicum * | 4 | 2 | 8 | 4 | 8 |
| Penicillium * sp. | 16 | 20 | 22 | 20 | 18 |
| Total microorganisms | 74 | 72 | 122 | 88 | 102 |
| Non-identified microorganisms | 28 | 20 | 26 | 30 | 12 |
| % of identified microorganisms | 62.2 | 72.2 | 78.7 | 65.9 | 88.2 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tomazin, R.; Kukec, A.; Švigelj, V.; Mulec, J.; Matos, T. Effects of Speleotherapy on Aerobiota: A Case Study from the Sežana Hospital Cave, Slovenia. Atmosphere 2024, 15, 518. https://doi.org/10.3390/atmos15050518
Tomazin R, Kukec A, Švigelj V, Mulec J, Matos T. Effects of Speleotherapy on Aerobiota: A Case Study from the Sežana Hospital Cave, Slovenia. Atmosphere. 2024; 15(5):518. https://doi.org/10.3390/atmos15050518
Chicago/Turabian StyleTomazin, Rok, Andreja Kukec, Viktor Švigelj, Janez Mulec, and Tadeja Matos. 2024. "Effects of Speleotherapy on Aerobiota: A Case Study from the Sežana Hospital Cave, Slovenia" Atmosphere 15, no. 5: 518. https://doi.org/10.3390/atmos15050518
APA StyleTomazin, R., Kukec, A., Švigelj, V., Mulec, J., & Matos, T. (2024). Effects of Speleotherapy on Aerobiota: A Case Study from the Sežana Hospital Cave, Slovenia. Atmosphere, 15(5), 518. https://doi.org/10.3390/atmos15050518