Making Administrative Systems Adaptive to Emerging Climate Change-Related Health Effects: Case of Estonia



Abstract
:1. Introduction
1.1. Climate Change Adaptation of Health Systems
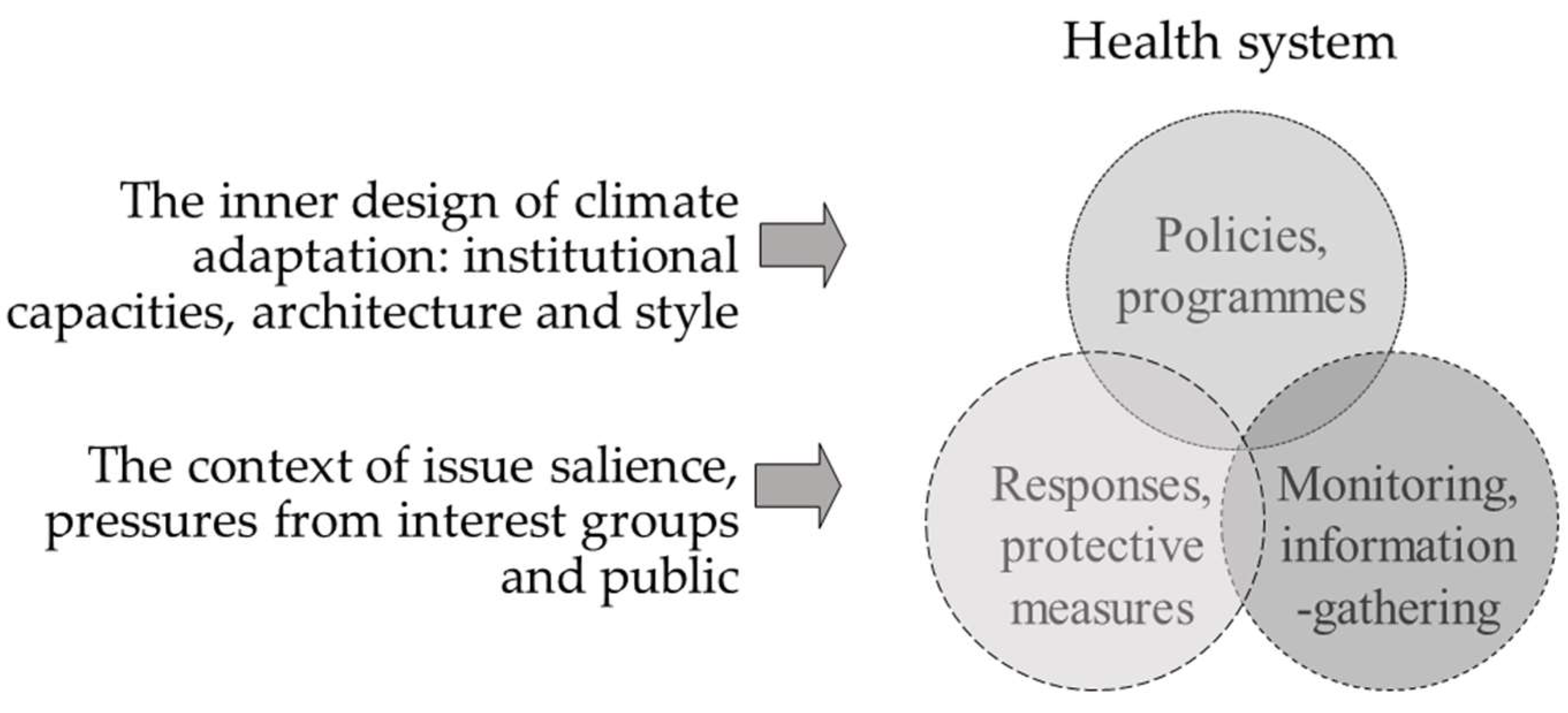
1.2. Factors Influencing Adaptation of Policy Programmes, Monitoring Systems, and Response Measures
2. Methods
3. Results
3.1. Adapting Health Systems to Climate Change
3.1.1. Planning Responses to Climate Change-Related Health Risks
3.1.2. Gathering Information and Monitoring the Situation
3.1.3. Protective Measures and Responses
3.2. Explanations for the Current Situation with Respect to Health Adaptation
3.2.1. The Inner Functioning of the State Apparatus Influences the Adaptation Activities
3.2.2. Adaptation Activities Influenced by the External Pressure Factors of the State Apparatus
3.2.3. International Pressures
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Appendix A
- Expert on social work (4 March 2015)
- Local government official (10 March 2015)
- Tartu City Government official (17 March 2015)
- Environmental health scientist (20 April 2015)
- Official from the ministry of the Interior (29 April 2015)
- Climate expert (29 April 2015)
- Environmental health specialist, Ministry of Social Affairs (4 May 2015)
- Official from the Estonian Environmental Research Centre (4 May 2015)
- Family physician (member of the managing board, Association of Family Physicians) (7 May 2015)
- Health Board official (7 May 2015)
- Public health specialist (8 May 2015)
- Official from the Ministry of the Environment (21 May 2015)
- Representative of a hospital (member of managing board) (4 June 2015)
- City medical officer (12 June 2015)
- Representative of volunteer rescue service providers (16 June 2015)
- Representative of Rescue Board (Lääne päästekeskus) (18 June 2015)
- Official from the Health System Development Department, Ministry of Social Affairs (19 June 2015)
- Chief specialist from the Environmental Health Research Centre, Health Board (27 May 2015)
- Official from the Health Board’s medical bureau (25 May 2015)
- Official from Pärnu City Government (26 August 2015)
- Official from Government Office (27 August 2015)
Appendix B
- What do you think about the climate change and its health effects?
- ○
- Health risks in the world/Estonia
- ○
- Future trends
- How would you assess health systems functioning to cope with CC effects on health?
- ○
- Sufficiency of regulations, programmes
- ○
- Monitoring and information gathering (prognoses, risk analyses)
- ○
- Protective responses, prevention
- What could be the key drivers/impediments on (a) tailoring programmes, measures, and (b) their implementation for CC health adaptation, (c) gathering information? Assess the role of ...
- ○
- yourself as an expert; public salience, NGOs, private companies, scientific groups, international organisations
- ○
- state officials, their competences and resources, regulatory style (and size), architecture (dispersion of responsibilities).
Appendix C

{kind=link}
| 1 | Personal Exposure | No Exposure | Extreme Exposure | ||||
| Please rate on a scale of 1–5 your exposure to extreme weather events | 1 | 2 | 3 | 4 | 5 | ||
| 2 | Personal worry | No exposure | Extreme exposure | ||||
| In general, how worried are you about the health risks posed to you and your family by your residential environment? | 1 | 2 | 3 | 4 | 5 | ||
| 3 | Belief in need for measures | No exposure | Extreme exposure | ||||
| Measures against climate change related risks are urgently needed | 1 | 2 | 3 | 4 | 5 | ||
| 4 | Belief in institutional efficiency | No exposure | Extreme exposure | ||||
| I trust that the authorities will take care of the healthfulness of my living environment | 1 | 2 | 3 | 4 | 5 | ||
Appendix D
| Low Demand, n (%) | High Demand, n (%) | Chi2 | p Value | |
|---|---|---|---|---|
| Gender | 3.11 | 0.08 | ||
| Male | 320 (72.7) | 120 (27.3) | ||
| Female | 377 (67.6) | 301 (32.4) | ||
| Age | 2.47 | 0.29 | ||
| Age, 20–34 | 110 (67.9) | 52 (32.1) | ||
| Age, 35–54 | 211 (69.2) | 94 (30.8) | ||
| Age, 55–75 | 109 (62.3) | 66 (37.7) | ||
| Education | 0.03 | 0.98 | ||
| primary | 23 (65.7) | 12 (34.3) | ||
| secondary | 262 (67.2) | 128 (32.8) | ||
| higher | 143 (66.8) | 71 (33.2) | ||
| Home language | 13.86 | 0.00 | ||
| Estonian | 496 (73.6) | 178 (26.4) | ||
| Russian or other | 201 (62.0) | 123 (38.0) | ||
| Place of residence | 9.93 | 0.00 | ||
| Urban | 473 (66.9) | 234 (33.1) | ||
| Rural | 224 (77) | 67 (23) | ||
| Self-rated health status | 8.69 | 0.12 | ||
| Very good | 52 (71.2) | 21 (28.8) | ||
| Good | 299 (72.7) | 112 (27.3) | ||
| Average | 277 (67.6) | 133 (32.4) | ||
| Bad | 59 (69.4) | 26 (30.6) | ||
| Very bad | 6 (75.0) | 2 (25.0) |
References
- Sellers, S.; Ebi, K.L. Climate change and health under the shared socioeconomic pathway framework. Int. J. Environ. Res. Public Health 2017, 15, 3. [Google Scholar] [CrossRef] [PubMed]
- Watts, N.; Adger, W.N.; Agnolucci, P.; Blackstock, J.; Byass, P.; Cai, W.; Chaytor, S.; Colbourn, T.; Collins, M.; Cooper, A.; et al. Health and climate change: Policy responses to protect public health. Lancet 2015, 386, 1861–1914. [Google Scholar] [CrossRef]
- Smith, K.R.; Woodward, A.; Campbell-Lendrum, D.; Chadee, D.D.; Honda, Y.; Liu, Q.; Olwoch, J.; Revich, B.; Sauerborn, R. Human health: Impacts, adaptation, and co-benefits. In Climate Change 2014: Impacts, Adaptation, and Vulnerability. Part A: Global and Sectoral Aspects. Contribution of Working Group II to the Fifth Assessment Report of the Intergovernmental Panel on Climate Change; Field, C.B., Barros, V.R., Dokken, D.J., Mach, K.J., Mastrandrea, M.D., Bilir, T.E., Chatterjee, M., Ebi, K.L., Estrada, Y.O., Genova, R.C., et al., Eds.; Cambridge University Press: Cambridge, UK, 2014; pp. 709–754. [Google Scholar]
- Jordan, A.; Huitema, D. Innovations in climate policy: The politics of invention, diffusion, and evaluation. Environ. Politics 2014, 23, 715–734. [Google Scholar] [CrossRef]
- Austin, S.E.; Biesbroek, R.; Berrang-Ford, L.; Ford, J.D.; Parker, S.; Fleury, M.D. Public health adaptation to climate change in oecd countries. Int. J. Environ. Res. Public Health 2016, 13, 889. [Google Scholar] [CrossRef] [PubMed]
- Hess, J.J.; McDowell, J.Z.; Luber, G. Integrating climate change adaptation into public health practice: Using adaptive management to increase adaptive capacity and build resilience. Environ. Health Perspect. 2012, 120, 171–179. [Google Scholar] [CrossRef] [PubMed]
- Bowen, K.J.; Ebi, K.L. Governing the health risks of climate change: Towards multi-sector responses. Curr. Opin. Environ. Sustain. 2015, 12, 80–85. [Google Scholar] [CrossRef]
- Amundsen, H.; Berglund, F.; Westskog, H. Overcoming barriers to climate change adaptation—A question of multilevel governance? Environ. Plan. C Gov. Policy 2010, 28, 276–289. [Google Scholar] [CrossRef]
- Austin, S.E.; Ford, J.D.; Berrang-Ford, L.; Araos, M.; Parker, S.; Fleury, M.D. Public health adaptation to climate change in canadian jurisdictions. Int. J. Environ. Res. Public Health 2015, 12, 623–651. [Google Scholar] [CrossRef] [PubMed]
- Roose, A. Climate changes—How to adapt? Publ. Inst. Geogr. Univ. Tartu 2015, 112, 6–19. [Google Scholar]
- Rothstein, H.; Demeritt, D.; Paul, R.; Beaussier, A.-L.; Wesseling, M.; Howard, M.; de Haan, M.; Borraz, O.; Huber, M.; Bouder, F. Varieties of risk regulation in europe: Coordination, complementarity and occupational safety in capitalist welfare states. Socio-Econom. Rev. 2017, mwx029. [Google Scholar] [CrossRef]
- Hood, C.; Rothstein, H.; Baldwin, R. The Government of Risk: Understanding Risk Regulation Regimes; Oxford University Press: New York, NY, USA, 2001. [Google Scholar]
- World Health Organization. Operational Framework for Building Climate Resilient Health Systems; World Health Organization: Geneva, Switzerland, 2015. [Google Scholar]
- Kieny, M.P.; Bekedam, H.; Dovlo, D.; Fitzgerald, J.; Habicht, J.; Harrison, G.; Kluge, H.; Lin, V.; Menabde, N.; Mirza, Z.; et al. Strengthening health systems for universal health coverage and sustainable development. Bull. World Health Organ. 2017, 95, 537–539. [Google Scholar] [CrossRef] [PubMed]
- Commission of the European Communities. White Paper–Adapting to Climate Change: Towards a European Framework for Action; COM: Brussels, Belgium, 2009. [Google Scholar]
- Hildén, M. Evaluation, assessment, and policy innovation: Exploring the links in relation to emissions trading. Environ. Politics 2014, 23, 839–859. [Google Scholar] [CrossRef]
- Hildén, M.; Jordan, A.; Rayner, T. Climate policy innovation: Developing an evaluation perspective. Environ. Politics 2014, 23, 884–905. [Google Scholar] [CrossRef]
- Orru, K.; Rothstein, H. Not ‘dead letters’, just ‘blind eyes’: The europeanisation of drinking water risk regulation in estonia and lithuania. Environ. Plan. A Econ. Space 2015, 47, 356–372. [Google Scholar] [CrossRef] [Green Version]
- Vihalemm, T.; Keller, M.; Kiisel, M. From Intervention to Social Change: A Guide to Reshaping Everyday Practices; Ashgate: Surrey, UK, 2015. [Google Scholar]
- Knaggård, Å. What do policy-makers do with scientific uncertainty? The incremental character of swedish climate change policy-making. Policy Stud. 2014, 35, 22–39. [Google Scholar] [CrossRef]
- Howlett, M. Why are policy innovations rare and so often negative? Blame avoidance and problem denial in climate change policy-making. Glob. Environ. Chang. 2014, 29, 395–403. [Google Scholar] [CrossRef]
- Gupta, J.; Termeer, C.; Klostermann, J.; Meijerink, S.; van den Brink, M.; Jong, P.; Nooteboom, S.; Bergsma, E. The adaptive capacity wheel: A method to assess the inherent characteristics of institutions to enable the adaptive capacity of society. Environ. Sci. Policy 2010, 13, 459–471. [Google Scholar] [CrossRef] [Green Version]
- Massey, D.; Chaboyer, W.; Aitken, L. Nurses’ perceptions of accessing a medical emergency team: A qualitative study. Aust. Crit. Care Off. J. Confed. Aust. Crit. Care Nurses 2014, 27, 133–138. [Google Scholar] [CrossRef] [PubMed]
- Rauken, T.; Mydske, P.K.; Winsvold, M. Mainstreaming climate change adaptation at the local level. Local Environ. 2015, 20, 408–423. [Google Scholar] [CrossRef]
- Reckien, D.; Salvia, M.; Heidrich, O.; Church, J.M.; Pietrapertosa, F.; De Gregorio-Hurtado, S.; D’Alonzo, V.; Foley, A.; Simoes, S.G.; Krkoška Lorencová, E.; et al. How are cities planning to respond to climate change? Assessment of local climate plans from 885 cities in the eu-28. J. Clean. Product. 2018, 191, 207–219. [Google Scholar] [CrossRef]
- Gupta, S.; Harnisch, J.; Barua, D.C.; Chingambo, L.; Frankel, P.; Vazquez, R.J.G.; Gomez-Echeverri, L.; Haites, E.; Huang, Y.; Kopp, R.; et al. Cross-cutting investment and finance issues. In IPCC Working Group III AR5.; Cambridge University Press: Cambridge, UK, 2014. [Google Scholar]
- Bowen, K.J.; Ebi, K.; Friel, S.; McMichael, A.J. A multi-layered governance framework for incorporating social science insights into adapting to the health impacts of climate change. Glob. Health Action 2013, 6, 21820. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tosun, J.; Lang, A. Policy integration: Mapping the different concepts. Policy Stud. 2017, 38, 553–570. [Google Scholar] [CrossRef]
- Ollila, E. Health in all policies: From rhetoric to action. Scand. J. Public Health 2011, 39, 11–18. [Google Scholar] [CrossRef] [PubMed]
- May, P.J.; Jochim, A.E.; Sapotichne, J. Constructing homeland security: An anemic policy regime. Policy Stud. J. 2011, 39, 285–307. [Google Scholar] [CrossRef]
- Spence, A.; Venables, D.; Pidgeon, N.; Poortinga, W.; Demski, C. Public Perceptions of Climate Change and Energy Futures in Britain; Technical Report; School of Psychology: Cardiff, UK, 2010. [Google Scholar]
- Kingdon, J.W. Agendas, Alternatives, and Public Policies; Longman: Boston, MA, USA, 2011. [Google Scholar]
- Portier, C.; Thigpen Tart, K.; Carter, S.; Dilworth, C.; Grambsch, A.; Gohlke, J.; Hess, J.; Howard, S.; Luber, G.; Lutz, J.; et al. A Human Health Perspective on Climate Change: A Report Outlining the Research Needs on the Human Health Effects of Climate Change; Environmental Health Perspectives/National Institute of Environmental Health Science: Durham, NC, USA, 2010.
- Wardekker, J.A.; de Jong, A.; van Bree, L.; Turkenburg, W.C.; van der Sluijs, J.P. Health risks of climate change: An assessment of uncertainties and its implications for adaptation policies. Environ. Health 2012, 11, 67. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Braun, M. Eu climate norms in east-central europe. JCMS J. Common Mark. Stud. 2014, 52, 445–460. [Google Scholar] [CrossRef]
- Biesenbender, S.; Tosun, J. Domestic politics and the diffusion of international policy innovations: How does accommodation happen? Glob. Environ. Chang. 2014, 29, 424–433. [Google Scholar] [CrossRef]
- Skjærseth, J.B.; Wettestad, J. Is eu enlargement bad for environmental policy? Confronting gloomy expectations with evidence. Int. Environ. Agreem. Politics Law Econ. 2007, 7, 263–280. [Google Scholar] [CrossRef]
- Felix, C.; Marcus, H.; James, R.; Kacper, S. Challenging the european climate debate: Can universal climate justice and economics be reconciled with particularistic politics? Glob. Policy 2014, 5, 6–14. [Google Scholar]
- Tompkins, E.L.; Amundsen, H. Perceptions of the effectiveness of the united nations framework convention on climate change in advancing national action on climate change. Environ. Sci. Policy 2008, 11, 1–13. [Google Scholar] [CrossRef]
- World Bank. Rural Population. Indicators. Available online: https://data.worldbank.org/indicator/SP.RUR.TOTL.ZS (accessed on 24 May 2018).
- Reile, R.; Helakorpi, S.; Klumbiene, J.; Tekkel, M.; Leinsalu, M. The recent economic recession and self-rated health in estonia, lithuania and finland: A comparative cross-sectional study in 2004–2010. J. Epidemiol. Community Health 2014, 68, 1072–1079. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Global Health Observatory Data Repository. Life Expectancy. Available online: http://apps.who.int/gho/data/view.main.SDG2016LEXv?lang=en (accessed on 24 May 2018).
- Ministry of Environment. Proposal for Compiling Action Plan for Coping with Climate Change Till 2030; Ministry of Environment: Tallinn, Estonia, 2015. [Google Scholar]
- Orru, K.; Hendrikson, R.; Nordlund, A.; Nutt, N.; Veeber, T.; Orru, H. Keskkonnatervis: Arusaamine Riskidest ja Motivatsioon Tervisemõjude Vähendamiseks. Keskkonnatervise Uuringute Keskus; Health Board: Tallinn, Estonia, 2015.
- Orru, H.; Lanki, T.; Forsberg, B.; Saava, A.; Åström, D.O.; Indermitte, E.; Orru, K.; Åström, K.; Rekker, K.; Tillmann, K.; et al. Tervis. In Kliimamuutuste Mõjude Hindamine ja Kohanemismeetmete Väljatöötamine Planeeringute, Maakasutuse, Inimtervise ja Päästevõimekuse Teemas (kati); Roose, A., Ed.; Tartu Ülikool: Tartu, Estonia, 2015; pp. 162–252. [Google Scholar]
- Giorgi, F.; Torma, C. Climate Variability and Change Over Europe. In Connections to Pollen Concentrations; ICTP: Trieste, Italy, 2015. [Google Scholar]
- Hamaoui-Laguel, L.; Vautard, R.; Liu, L.; Solmon, F.; Viovy, N.; Khvorostyanov, D.; Essl, F.; Chuine, I.; Colette, A.; Semenov, M.A.; et al. . Effects of climate change and seed dispersal on airborne ragweed pollen loads in europe. Nat. Clim. Chang. 2015, 5, 766. [Google Scholar] [CrossRef]
- Semenza, J.C.; Suk, J.E.; Estevez, V.; Ebi, K.L.; Lindgren, E. Mapping climate change vulnerabilities to infectious diseases in europe. Environ. Health Perspect. 2012, 120, 385–392. [Google Scholar] [CrossRef] [PubMed]
- Mölter, T.; Schindler, D.; Albrecht, A.; Kohnle, U. Review on the projections of future storminess over the north atlantic european region. Atmosphere 2016, 7, 60. [Google Scholar] [CrossRef]
- Ministry of Social Affairs. Action Plan of National Health Plan 2009–2020; Ministry of Social Affairs: Tallinn, Estonia, 2008. [Google Scholar]
- Ministry of Environment. Estonian Environmental Strategy Until 2030; Ministry of Environment: Tallinn, Estonia, 2007. [Google Scholar]
- Ministry of Environment. Estonian Environmental Action Plan 2007–2013; Ministry of Environment: Tallinn, Estonia, 2007. [Google Scholar]
- Estonian State Weather Service. Sõnastik. Available online: http://www.ilmateenistus.ee/ilmatarkus/sonastik/#hiromb (accessed on 6 June 2018).
- Estonian State Weather Service. Sunshine. Available online: https://www.ilmateenistus.ee/kliima/climate-maps/sunshine/?lang=en (accessed on 6 June 2018).
- Estonian State Weather Service. High-Resolution Operational Model for the Baltic Sea, Hiromb; Estonian State Weather Service: Tallinn, Estonia, 2016. [Google Scholar]
- Air Quality Management System. Seirevõrgustik. Available online: http://airviro.klab.ee/ (accessed on 8 June 2018).
- Ministry of Interior. Emergency act. In RT I, 2009, 39, 262; Ministry of Interior: Tallinn, Estonia, 2009. [Google Scholar]
- Ministry of Interior. Development Plan for Interior Security 2015–2020; Ministry of Interior: Tallinn, Estonia, 2015.
- Ministry of Social Affairs. Public health act. In RT I, 1995, 57, 978; Ministry of Social Affairs: Tallinn, Estonia, 1995. [Google Scholar]
- Health Board. Centre for Environmental Health Studies. Available online: http://www.terviseamet.ee/keskkonnatervis/keskkonnatervise-uuringute-keskus.html (accessed on 6 June 2018).
- Ministry of Interior. The List of Emergencies According to Which a Risk Analysis and Solution Plan Will Be Composed and the Identification of the Institutions Responsible for Risk Analysis and Emergency; Ministry of Interior: Tallinn, Estonia, 2013.
- Ministry of Interior. Plan. for Solving Emergencies Due to Storm; Ministry of Interior: Tallinn, Estonia, 2013.
- Ministry of Interior. Plan. for Solving Emergencies Due to Flooding in Densely Populated Areas; Ministry of Interior: Tallinn, Estonia, 2013.
- Ministry of Interior. Risk Analysis for Emergency Situations in 2013; Ministry of Interior: Tallinn, Estonia, 2013.
- Ministry of Social Affairs. Development Plan for the Primary Care in 2009–2015; Ministry of Social Affairs: Tallinn, Estonia, 2009.
- Health Board. Risk Analysis for Emergency Situation Related to Epidemics; Health Board: Tallinn, Estonia, 2013.
- Ministry of Interior. Law on changing the law on emergency situations. In RT I, 2017, 1; Ministry of Interior: Tallinn, Estonia, 2017. [Google Scholar]
- European Commission. Special Eurobarometer 459. Report. Climate Change; TNS Opinion & Social: Brussels, Belgium, 2017. [Google Scholar]
- Ministry of Environment. Report on Assessment of the Flood Risks; Ministry of Environment: Tallinn, Estonia, 2011. [Google Scholar]
- Ministry of Environment. Climate Change Adaption Development Plan Until 2030; Ministry of Environment: Tallinn, Estonia, 2017. [Google Scholar]
- Uustal, T. Development Plan for Adapting to the Climate Change in 2030; Proposal; Estonian Environmental Research Centre: Tallinn, Estonia, 2016. [Google Scholar]
- Bulkeley, H.; Jordan, A. Transnational environmental governance: New findings and emerging research agendas. Environ. Plan. C Gov. Policy 2012, 30, 556–570. [Google Scholar] [CrossRef]
- Brouwer, S.; Rayner, T.; Huitema, D. Mainstreaming climate policy: The case of climate adaptation and the implementation of eu water policy. Environ. Plan. C Gov. Policy 2013, 31, 134–153. [Google Scholar] [CrossRef]
- Bouwer, L.M.; Aerts, J.C. Financing climate change adaptation. Disasters 2006, 30, 49–63. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Andrew, J.; Andrea, L. Environmental policy integration: A state of the art review. Environ.Policy Gov. 2010, 20, 147–158. [Google Scholar]
- Peters, B.G. Pursuing Horizontal Management: The Politics of Public Sector Coordination; University Press of Kansas: Laurence, KS, USA, 2015. [Google Scholar]
- Pidgeon, N.; Kasperson, R.E.; Slovic, P. The Social Amplification of Risk; Cambridge University Press: Cambridge, UK, 2003. [Google Scholar]
- Dietz, T.; Stern, P.C. Public Participation in Environmental Assessment and Decision Making; National Academies Press: Washington, DC, USA, 2008. [Google Scholar]
- Shwom, R.; Bidwell, D.; Dan, A.; Dietz, T. Understanding u.S. Public support for domestic climate change policies. Glob. Environ. Chang. 2010, 20, 472–482. [Google Scholar] [CrossRef]
- Shum, R.Y. Effects of economic recession and local weather on climate change attitudes. Clim. Policy 2012, 12, 38–49. [Google Scholar] [CrossRef]
- Scruggs, L.; Benegal, S. Declining public concern about climate change: Can we blame the great recession? Glob. Environ. Chang. 2012, 22, 505–515. [Google Scholar] [CrossRef]
- Milfont, T.L. The interplay between knowledge, perceived efficacy, and concern about global warming and climate change: A one-year longitudinal study. Risk Anal. Off. Publ. Soc. Risk Anal. 2012, 32, 1003–1020. [Google Scholar] [CrossRef] [PubMed]
- Kellstedt, P.M.; Zahran, S.; Vedlitz, A. Personal efficacy, the information environment, and attitudes toward global warming and climate change in the united states. Risk Anal. Off. Publ. Soc. Risk Anal. 2008, 28, 113–126. [Google Scholar] [CrossRef] [PubMed]
- Demski, C.; Capstick, S.; Pidgeon, N.; Sposato, R.G.; Spence, A. Experience of extreme weather affects climate change mitigation and adaptation responses. Clim. Chang. 2017, 140, 149–164. [Google Scholar] [CrossRef]
- Reser, J.P.; Bradley, G.L.; Ellul, M.C. Encountering climate change: ‘Seeing’ is more than ‘believing’. Wiley Interdiscip. Rev. Clim. Chang. 2014, 5, 521–537. [Google Scholar] [CrossRef]
- McDonald, R.I.; Chai, H.Y.; Newell, B.R. Personal experience and the ‘psychological distance’ of climate change: An integrative review. J. Environ. Psychol. 2015, 44, 109–118. [Google Scholar] [CrossRef]
- Barriopedro, D.; Fischer, E.M.; Luterbacher, J.; Trigo, R.M.; Garcia-Herrera, R. The hot summer of 2010: Redrawing the temperature record map of europe. Science 2011, 332, 220–224. [Google Scholar] [CrossRef] [PubMed]
- Anders, I.; Stagl, J.; Auer, I.; Pavlik, D. Climate change in central and eastern europe. In Managing Protected Areas in Central and Eastern Europe under Climate Change; Ranow, S., Neubert, M., Eds.; Springer: Dordrecht, The Netherlands, 2014; pp. 17–30. [Google Scholar]
- Orru, H.; Ebi, K.L.; Forsberg, B. The interplay of climate change and air pollution on health. Curr. Environ. Health Rep. 2017, 4, 504–513. [Google Scholar] [CrossRef] [PubMed]
- Macias, T. Environmental risk perception among race and ethnic groups in the united states. Ethnicities 2015, 16, 111–129. [Google Scholar] [CrossRef]

| Key Institutions | Policies and Programmes | Monitoring and Information-Gathering | Responses and Protective Measures | Addressing Climate Change? |
|---|---|---|---|---|
| Ministry of Social Affairs, Health Board, National Institute for Health Development | National Health Plan 2020 | Health Board: monitoring and prevention of infectious diseases, vector transmitted diseases, including cyanotoxins in bathing water | Health Board: Information on web on prevention of infectious diseases, vector transmitted diseases. | No |
| Ministry of Environment, Weather Service | Environmental Strategy 2030 | Weather Service [53,54,55]: European forecast model HIRLAM, Weather Alert System Meteoalarm, Baltic Sea forecast models HIROMB; UV radiation; pollen content for allergens | Weather Service: forecasts and warnings on web: Estonian Weather Service, Air Quality Management System [56]. | Included in environment monitoring |
| Ministry of Interior | Emergency Act [57], Internal Security Development Plan 2015–2020 | Rescue Board in collaboration with Health Board conducts risk analysis for emergency situations including floods, extensive forest fires, extremely cold and warm weather | Emergency plans for large-scale forest or landscape fires; storms and floods in densely populated areas; epidemics. Instructions on behaviour during emergencies on Crisis web | Included in rescue capacity |
| Base Model | Sig. | Exp(B) |
|---|---|---|
| Gender, man (ref woman) | 0.79 | 0.96 (0.68–1.34) |
| Age, 20–34 (ref 55–75) | 0.19 | 0.73 (0.46–1.17) |
| Age, 35–54 (ref 55–75) | 0.10 | 0.71 (0.48–1.06) |
| Education, primary (ref higher) | 0.84 | 1.08 (0.50–2.33) |
| Education, secondary (ref higher) | 0.57 | 0.90 (0.62–1.30) |
| Home language, Estonian (ref Russian or other) | 0.01 | 0.61 (0.43–0.86) |
| Self-rated health status | 0.71 | 0.96 (0.79–1.18) |
| Social and psychological factors * | ||
| Belief in state institutions taking care of the healthfulness of living environment | 0.52 | 0.94 (0.79–1.18) |
| Worry about health effects from environment on personal and family health | ||
| Low (ref high worry) | 0.01 | 0.57 (0.37–0.88) |
| Medium (ref high worry) | 0.01 | 0.58 (0.38–0.88) |
| Exposure to extreme weather events | 0.01 | 1.24 (1.06–1.45) |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Orru, K.; Tillmann, M.; Ebi, K.L.; Orru, H. Making Administrative Systems Adaptive to Emerging Climate Change-Related Health Effects: Case of Estonia. Atmosphere 2018, 9, 221. https://doi.org/10.3390/atmos9060221
Orru K, Tillmann M, Ebi KL, Orru H. Making Administrative Systems Adaptive to Emerging Climate Change-Related Health Effects: Case of Estonia. Atmosphere. 2018; 9(6):221. https://doi.org/10.3390/atmos9060221
Chicago/Turabian StyleOrru, Kati, Mari Tillmann, Kristie L. Ebi, and Hans Orru. 2018. "Making Administrative Systems Adaptive to Emerging Climate Change-Related Health Effects: Case of Estonia" Atmosphere 9, no. 6: 221. https://doi.org/10.3390/atmos9060221
APA StyleOrru, K., Tillmann, M., Ebi, K. L., & Orru, H. (2018). Making Administrative Systems Adaptive to Emerging Climate Change-Related Health Effects: Case of Estonia. Atmosphere, 9(6), 221. https://doi.org/10.3390/atmos9060221