
The Seroprevalence and Seropositivity of SARS-CoV-2 among Healthcare Workers during the Third Pandemic Wave

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Hospital Settings
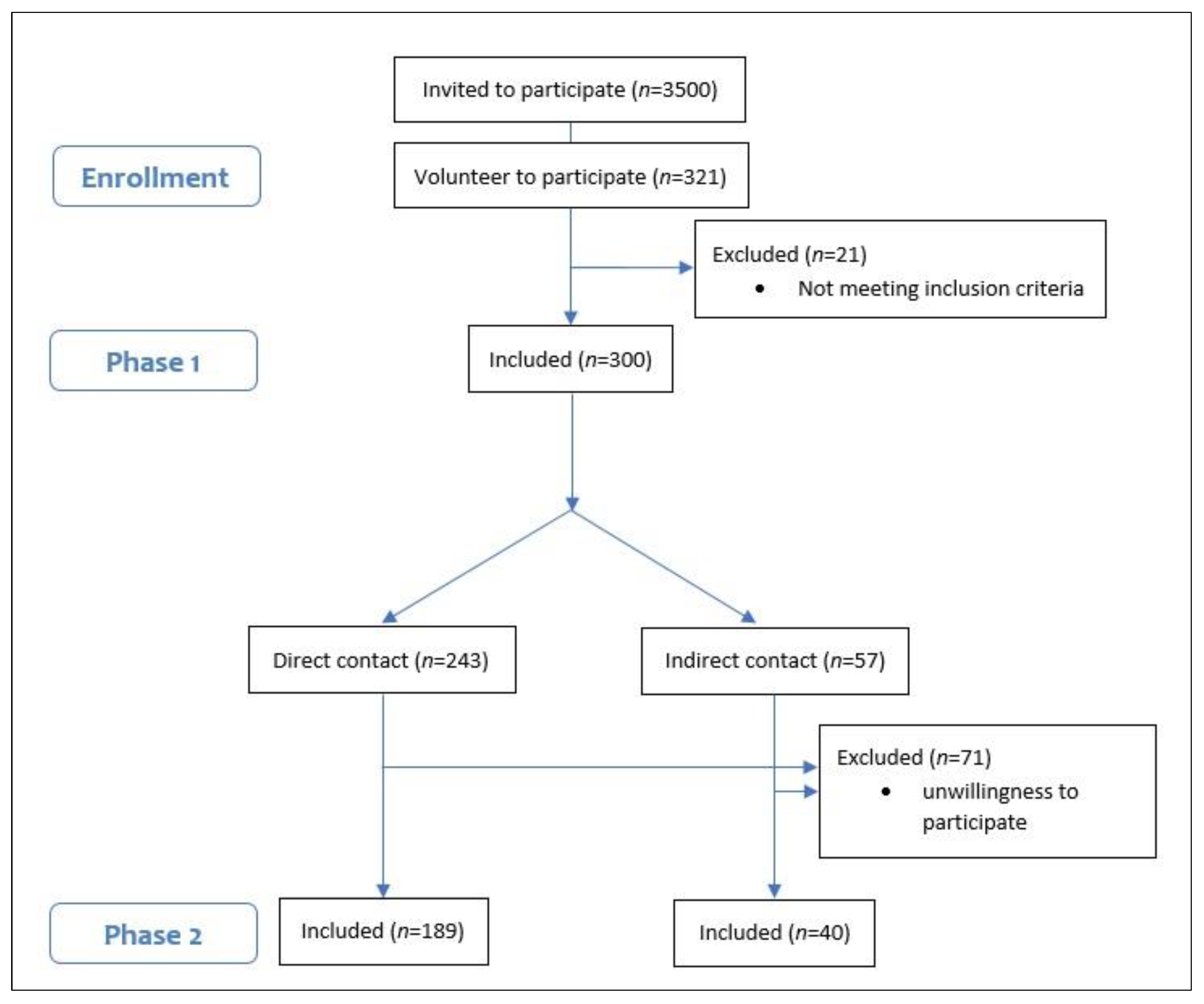
2.2. Study Design and Participants
2.3. Serologic Assay and Measures
2.4. Statistical Analysis
3. Results
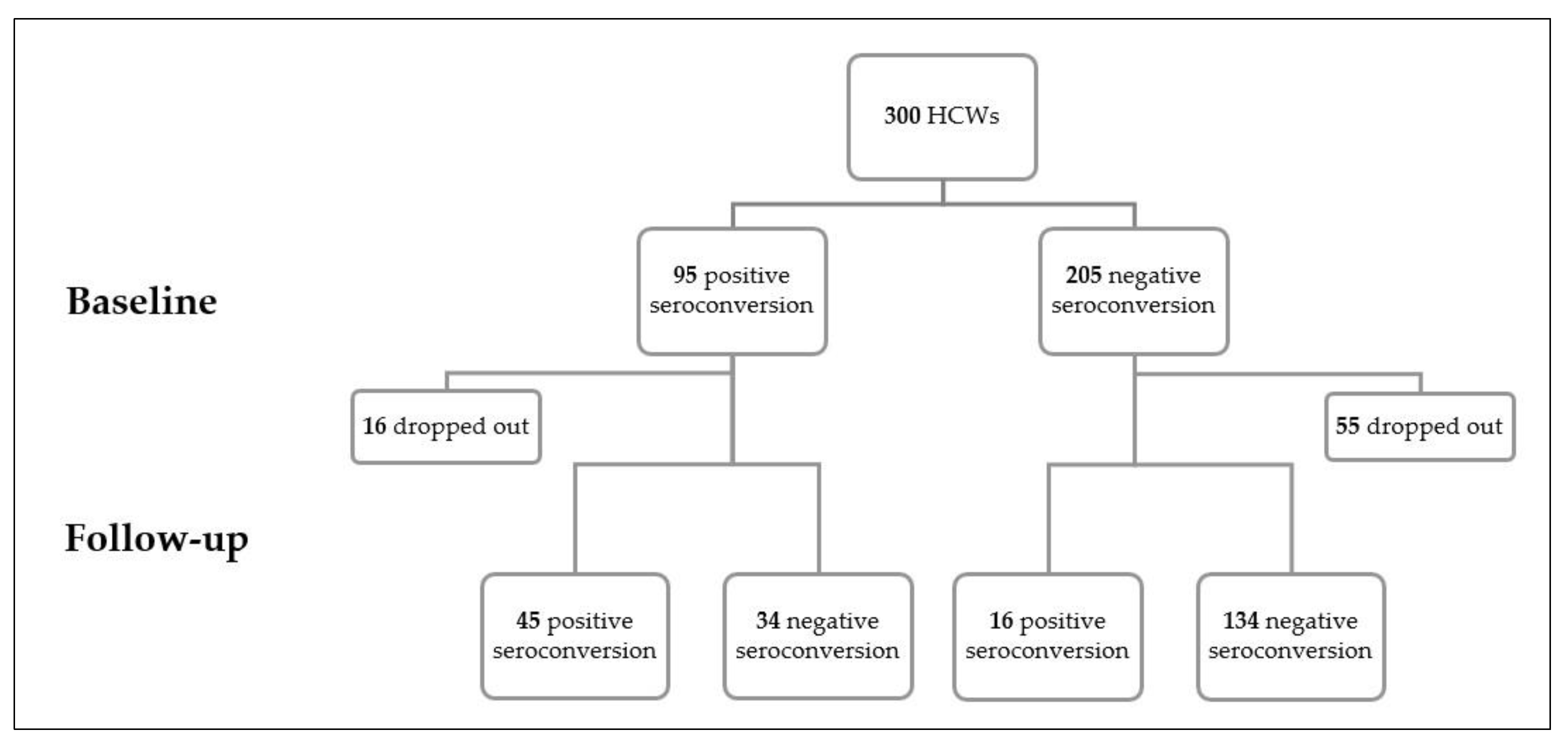
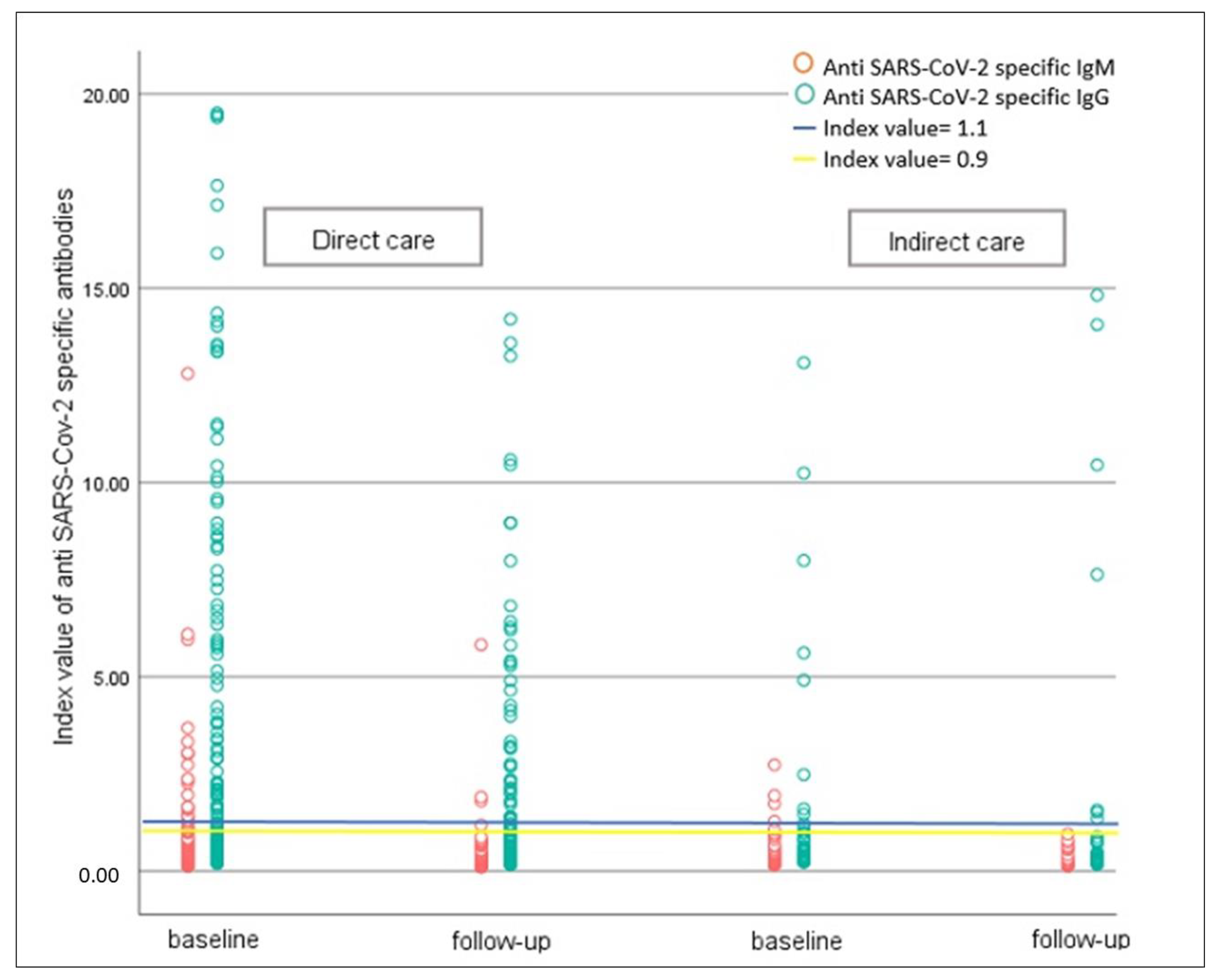
3.1. Serologic Findings and Seroconversion Rate
3.2. Symptoms Based on Seroconversion
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- WHO Coronavirus (COVID-19) Dashboard. Available online: https://covid19.who.int/ (accessed on 10 April 2022).
- Miller, T.E.; Beltran, W.F.G.; Bard, A.Z.; Gogakos, T.; Anahtar, M.N.; Astudillo, M.G.; Yang, D.; Thierauf, J.; Fisch, A.S.; Mahowald, G.K.; et al. Clinical sensitivity and interpretation of PCR and serological COVID-19 diagnostics for patients presenting to the hospital. FASEB J. 2020, 34, 13877–13884. [Google Scholar] [CrossRef] [PubMed]
- Arons, M.M.; Hatfield, K.M.; Reddy, S.C.; Kimball, A.; James, A.; Jacobs, J.R.; Taylor, J.; Spicer, K.; Bardossy, A.C.; Oakley, L.P.; et al. Presymptomatic SARS-CoV-2 infections and transmission in a skilled nursing facility. N. Engl. J. Med. 2020, 382, 2081–2090. [Google Scholar] [CrossRef] [PubMed]
- Oran, A.D.P.; Topol, E.J. Prevalence of Asymptomatic SARS-CoV-2 Infection: A Narrative Review. Ann. Intern. Med. 2020, 173, 362–367. [Google Scholar] [CrossRef] [PubMed]
- Maine, G.N.; Lao, K.M.; Krishnan, S.M.; Afolayan-Oloye, O.; Fatemi, S.; Kumar, S.; VanHorn, L.; Hurand, A.; Sykes, E.; Sun, Q. Longitudinal characterization of the IgM and IgG humoral response in symptomatic COVID-19 patients using the Abbott Architect. J. Clin. Virol. 2020, 133, 104663. [Google Scholar] [CrossRef]
- Xiao, T.; Wang, Y.; Yuan, J.; Ye, H.; Wei, L.; Liao, X.; Wang, H.; Qian, S.; Wang, Z.; Liu, L.; et al. Early viral clearance and antibody kinetics of COVID-19 among asymptomatic carriers. Front. Med. 2021, 8, 595773. [Google Scholar] [CrossRef]
- Racine, R.; Winslow, G.M. IgM in microbial infections: Taken for granted? Immunol. Lett. 2009, 125, 79–85. [Google Scholar] [CrossRef] [Green Version]
- Toulis, P. Estimation of COVID-19 prevalence from serology tests: A partial identification approach. J. Econom. 2021, 220, 193–213. [Google Scholar] [CrossRef]
- Sotgiu, G.; Barassi, A.; Miozzo, M.; Saderi, L.; Piana, A.; Orfeo, N.; Colosio, C.; Felisati, G.; Davì, M.; Gerli, A.G.; et al. SARS-CoV-2 specific serological pattern in healthcare workers of an Italian COVID-19 forefront hospital. BMC Pulm. Med. 2020, 20, 1–6. [Google Scholar] [CrossRef]
- Ng, K.; Poon, B.H.; Puar, T.H.K.; Quah, J.L.S.; Loh, W.J.; Wong, Y.J.; Tan, T.Y.; Raghuram, J. COVID-19 and the risk to health care workers: A case report. Ann. Intern. Med. 2020, 172, 766–767. [Google Scholar] [CrossRef] [Green Version]
- Lai, X.; Wang, M.; Qin, C.; Tan, L.; Ran, L.; Chen, D.; Zhang, H.; Shang, K.; Xia, C.; Wang, S.; et al. Coronavirus disease 2019 (COVID-2019) infection among health care workers and implications for prevention measures in a tertiary hospital in Wuhan, China. JAMA Netw. Open 2020, 3, e209666. [Google Scholar] [CrossRef]
- Nguyen, L.H.; Drew, D.A.; Graham, M.S.; Joshi, A.D.; Guo, C.-G.; Ma, W.; Mehta, R.S.; Warner, E.T.; Sikavi, D.R.; Lo, C.-H.; et al. Risk of COVID-19 among front-line health-care workers and the general community: A prospective cohort study. Lancet Public Health 2020, 5, e475–e483. [Google Scholar] [CrossRef] [PubMed]
- Korth, J.; Wilde, B.; Dolff, S.; Anastasiou, O.E.; Krawczyk, A.; Jahn, M.; Cordes, S.; Ross, B.; Esser, S.; Lindemann, M.; et al. SARS-CoV-2-specific antibody detection in healthcare workers in Germany with direct contact to COVID-19 patients. J. Clin. Virol. 2020, 128, 104437. [Google Scholar] [CrossRef] [PubMed]
- Mansour, M.; Leven, E.; Muellers, K.; Stone, K.; Mendu, D.R.; AJJogim, W. Prevalence of SARS-CoV-2 antibodies among healthcare workers at a tertiary academic hospital in New York City. J. Gen. Intern. Med. 2020, 35, 2485–2486. [Google Scholar] [CrossRef] [PubMed]
- Nikolai, L.A.; Meyer, C.G.; Kremsner, P.G.; Velavan, T.P. Asymptomatic SARS Coronavirus 2 infection: Invisible yet invincible. Int. J. Infect. Dis. 2020, 100, 112–116. [Google Scholar] [CrossRef] [PubMed]
- Krejcie, R.V.; Morgan, D.W. Determining sample size for research activities. Educ. Psychol. Meas. 1970, 30, 607–610. [Google Scholar] [CrossRef]
- Pishtaz Teb Diagnostics SARS-CoV-2 IgG ELISA kits. Available online: http://pishtazteb.com/en/sars-cov-2-igg-elisa-kit/ (accessed on 19 September 2020).
- Pishtaz Teb Diagnostics SARS-CoV-2 IgM ELISA kits. Available online: https://pishtazteb.com/en/sars-cov-2-igm-elisa-kit/ (accessed on 19 September 2020).
- Fonseca, M.H.; Silva, M.F.; Pinto, A.C.; de Melo, A.C.; de Oliveira, F.D.; Araújo, F.M.; de Andrade, L.O. Persistently positive SARS-CoV-2-specific IgM during 1-year follow-up. J. Med. Virol. 2022, 94, 4037. [Google Scholar] [CrossRef]
- Waxman, J.G.; Makov-Assif, M.; Reis, B.Y.; Netzer, D.; Balicer, R.D.; Dagan, N.; Barda, N. Comparing COVID-19-related hospitalization rates among individuals with infection-induced and vaccine-induced immunity in Israel. Nat. Commun. 2022, 13, 2202. [Google Scholar] [CrossRef]
- Carazo, S.; Skowronski, D.M.; Brisson, M.; Sauvageau, C.; Brousseau, N.; Gilca, R.; Ouakki, M.; Barkati, S.; Fafard, J.; Talbot, D.; et al. Estimated Protection of Prior SARS-CoV-2 Infection Against Reinfection with the Omicron Variant Among Messenger RNA–Vaccinated and Nonvaccinated Individuals in Quebec, Canada. JAMA Netw Open. 2022, 5, e2236670. [Google Scholar] [CrossRef]
- Houlihan, C.F.; Vora, N.; Byrne, T.; Lewer, D.; Kelly, G.; Heaney, J.; Gandhi, S.; Spyer, M.; Beale, R.; Cherepanov, P.; et al. Pandemic peak SARS-CoV-2 infection and seroconversion rates in London frontline health-care workers. Lancet 2020, 396, e6–e7. [Google Scholar] [CrossRef]
- Rashid-Abdi, M.; Krifors, A.; Sälléber, A.; Eriksson, J.; Månsson, E. Low rate of COVID-19 seroconversion in health-care workers at a Department of Infectious Diseases in Sweden during the later phase of the first wave; a prospective longitudinal seroepidemiological study. Infect. Dis. 2021, 53, 169–175. [Google Scholar] [CrossRef]
- Poustchi, H.; Darvishian, M.; Mohammadi, Z.; Shayanrad, A.; Delavari, A.; Bahadorimonfared, A.; Eslami, S.; Javanmard, S.H.; Shakiba, E.; Somi, M.H.; et al. SARS-CoV-2 antibody seroprevalence in the general population and high-risk occupational groups across 18 cities in Iran: A population-based cross-sectional study. Lancet Infect. Dis. 2021, 21, 473–481. [Google Scholar] [CrossRef]
- Kubina, R.; Dziedzic, A. Molecular and serological tests for COVID-19. A comparative review of SARS-CoV-2 coronavirus laboratory and point-of-care diagnostics. Diagnostics 2020, 10, 434. [Google Scholar] [CrossRef] [PubMed]
- Long, Q.-X.; Tang, X.-J.; Shi, Q.-L.; Li, Q.; Deng, H.-J.; Yuan, J.; Hu, J.-L.; Xu, W.; Zhang, Y.; Lv, F.-J.; et al. Clinical and immunological assessment of asymptomatic SARS-CoV-2 infections. Nat. Med. 2020, 26, 1200–1204. [Google Scholar] [CrossRef] [PubMed]
- Roy, S. COVID-19 reinfection: Myth or truth? SN Compr. Clin. Med. 2020, 2, 710–713. [Google Scholar] [CrossRef] [PubMed]
- Falahi, S.; Kenarkoohi, A. COVID-19 reinfection: Prolonged shedding or true reinfection? New Microbes New Infect. 2020, 38, 100812. [Google Scholar] [CrossRef] [PubMed]
- Kellam, P.; Barclay, W. The dynamics of humoral immune responses following SARS-CoV-2 infection and the potential for reinfection. J. Gen. Virol. 2020, 101, 791–797. [Google Scholar] [CrossRef]
- Al-Naemi, M.H.B.; Hassanen, W.S.; El Nahrawi, S.F.M.; Rashad, R.A. Life span of COVID-19 antibodies following infection in a sample worker population in Qatar. J. Emerg. Med. Trauma Acute Care 2021, 2021, 5. [Google Scholar] [CrossRef]
- Ye, G.; Pan, Z.; Pan, Y.; Deng, Q.; Chen, L.; Li, J.; Li, Y.; Wang, X. Clinical characteristics of severe acute respiratory syndrome coronavirus 2 reactivation. J. Infect. 2020, 80, e14–e17. [Google Scholar] [CrossRef]
- Yu, X.; Yang, R. COVID-19 transmission through asymptomatic carriers is a challenge to containment. Influenza Other Respir. Viruses 2020, 14, 474–475. [Google Scholar] [CrossRef] [Green Version]
- Fakhim, H.; Nasri, E.; Aboutalebian, S.; Gholipour, S.; Nikaeen, M.; Vaezi, A.; Mousavi, S.; Faramarzi, S.; Farhang, A.; Javanmard, S.H.; et al. Asymptomatic carriers of coronavirus disease 2019 among healthcare workers in Isfahan, Iran. Future Virol. 2021, 16, 93–98. [Google Scholar] [CrossRef]
- Steensels, D.; Oris, E.; Coninx, L.; Nuyens, D.; Delforge, M.-L.; Vermeersch, P.; Heylen, L. Hospital-wide SARS-CoV-2 antibody screening in 3056 staff in a tertiary center in Belgium. JAMA 2020, 324, 195–197. [Google Scholar] [CrossRef] [PubMed]
- Rudberg, A.-S.; Havervall, S.; Månberg, A.; Falk, A.J.; Aguilera, K.; Ng, H.; Gabrielsson, L.; Salomonsson, A.-C.; Hanke, L.; Murrell, B.; et al. SARS-CoV-2 exposure, symptoms and seroprevalence in healthcare workers in Sweden. Nat. Commun. 2020, 11, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Sims, M.D.; Maine, G.N.; Childers, K.L.; Podolsky, R.H.; Voss, D.R.; Berkiw-Scenna, N.; Oh, J.; E Heinrich, K.; Keil, H.; Kennedy, R.H.; et al. Coronavirus Disease 2019 (COVID-19) seropositivity and asymptomatic Rates in healthcare workers are associated with job function and masking. Clin. Infect. Dis. 2021, 73 (Suppl. 2), S154–S162. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Total | Contact with COVID-19 Patients | p-Value | ||
|---|---|---|---|---|
| Direct (n = 243) | Indirect (n = 57) | |||
| Age (mean ± SD) | 38.5 ± 9.15 | 38.2 ± 9.03 | 40.0 ± 9.60 | 0.19 * |
| Gender | 0.1 | |||
| Female | 202 (67.3) | 168 (69.1) | 34 (59.6) | |
| Male | 98 (32.7) | 75 (30.9) | 23 (40.4) | |
| Occupation | <0.001 | |||
| Doctor/Resident/Medical student | 32 (10.7) | 32 (13.2) | 0 | |
| Nurse | 211 (70.3) | 211 (68.8) | 0 | |
| Others | 57 (19.0) | 0 | 57 (100) | |
| Ward | 0.01 | |||
| Emergency room | 29 (9.7) | 21 (8.6) | 8 (14.0) | |
| ICU | 158 (52.7) | 138 (56.8) | 20 (35.1) | |
| Others | 113 (37.7) | 84 (34.6) | 29 (50.9) | |
| Education level | <0.001 | |||
| High school and less | 68 (22.7) | 43 (17.7) | 25 (43.9) | |
| Bachelor | 198 (66.0) | 167 (68.7) | 31 (54.4) | |
| MD and more | 34 (11.3) | 33 (13.6) | 1 (1.8) | |
| Educating about IPC | 0.1 | |||
| Yes | 260 (86.7) | 214 (88.1) | 46 (80.7) | |
| No | 40 (13.3) | 29 (11.9) | 11 (19.3) | |
| IPC guidelines compliance | 0.03 | |||
| Yes | 208 (69.3) | 162 (66.7) | 46 (80.7) | |
| No | 92 (30.7) | 81 (33.3) | 11 (19.3) | |
| Comorbidities | ||||
| CVD | 13 (4.3) | 10 (4.1) | 3 (5.3) | 0.4 |
| Cancer | 9 (3.0) | 8 (3.3) | 1 (1.8) | 0.4 |
| Respiratory diseases | 2 (0.7) | 1 (0.4) | 1 (1.8) | 0.3 |
| DM | 12 (4.0) | 9 (3.7) | 3 (5.3) | 0.7 |
| Any previous diseases | 64 (21.3) | 51 (21.0) | 13 (22.8) | 0.7 |
| BMI ≥ 25 | 130 (45.5) | 104 (44.4) | 26 (50.0) | 0.4 |
| Whole Sample | Contact with COVID-19 Patients | p-Value | |||
|---|---|---|---|---|---|
| Direct (n = 243) | Indirect (n = 57) | ||||
| Baseline | Seroconversion n (%) | 0.1 * | |||
| Yes | 95 (31.7) | 82 (33.7) | 13 (22.8) | ||
| No | 205 (68.3) | 161 (66.3) | 44 (77.2) | ||
| Anti SARS-CoV-2 IgM | 0.37 (0.34–0.41) | 0.38 (0.35–0.42) | 0.37 (0.31–0.43) | 0.83 ** | |
| Anti SARS-CoV-2 IgG | 0.77 (0.67–0.89) | 0.89 (0.71–0.99) | 0.54 (0.41–0.70) | 0.02 ** | |
| Follow-up | Seroconversion n (%) | 0.2 * | |||
| Yes | 61 (26.6) | 53 (28.0) | 8 (20.0) | ||
| No | 168 (73.4) | 136 (72.0) | 32 (80.0) | ||
| Anti SARS-CoV-2 IgM | 0.23 (0.21–0.24) | 0.22 (0.21–0.24) | 0.24 (0.20–0.28) | 0.95 ** | |
| Anti SARS-CoV-2 IgG | 0.56 (0.48–0.65) | 0.58 (0.49–0.68) | 0.49 (0.34–0.72) | 0.32 ** | |
| Total (n = 122) | Seroconversion | p-Value | ||
|---|---|---|---|---|
| Positive (n = 69) | Negative (n = 53) | |||
| Fever (≥38) | 63 (51.6) | 41 (59.4) | 22 (41.5) | 0.05 |
| Sore throat | 68 (55.7) | 40 (58.0) | 28 (52.8) | 0.5 |
| Cough | 71 (58.2) | 42 (60.9) | 29 (54.7) | 0.4 |
| Rhinorrhea | 55 (45.1) | 34 (49.3) | 21 (39.6) | 0.2 |
| Dyspnea | 58 (47.5) | 35 (50.7) | 23 (43.4) | 0.4 |
| Chills | 81 (66.4) | 51 (73.9) | 30 (56.6) | 0.04 |
| Nausea/vomiting | 48 (39.3) | 34 (49.3) | 14 (26.4) | 0.01 |
| Diarrhea | 40 (32.8) | 24 (34.8) | 16 (30.2) | 0.5 |
| Loss of appetite | 65 (53.3) | 41 (60.3) | 24 (45.3) | 0.1 |
| Anosmia or ageusia | 60 (49.2) | 43 (62.3) | 17 (32.1) | 0.001 |
| Skin rash | 15 (12.3) | 8 (11.6) | 7 (13.2) | 0.7 |
| Conjunctivitis | 13 (10.7) | 6 (8.7) | 7 (13.2) | 0.5 |
| Body/joint pain | 100 (82.0) | 57 (82.6) | 43 (81.1) | 0.8 |
| Fatigue | 106 (86.9) | 61 (88.4) | 45 (84.9) | 0.5 |
| Headache | 93 (76.2) | 52 (75.4) | 41 (77.4) | 0.7 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vaezi, A.; Fakhim, H.; Abbasi, S.; Masoudi, S.; Rizi, M.H.; Haghjooy Javanmard, S. The Seroprevalence and Seropositivity of SARS-CoV-2 among Healthcare Workers during the Third Pandemic Wave. Antibodies 2023, 12, 2. https://doi.org/10.3390/antib12010002
Vaezi A, Fakhim H, Abbasi S, Masoudi S, Rizi MH, Haghjooy Javanmard S. The Seroprevalence and Seropositivity of SARS-CoV-2 among Healthcare Workers during the Third Pandemic Wave. Antibodies. 2023; 12(1):2. https://doi.org/10.3390/antib12010002
Chicago/Turabian StyleVaezi, Atefeh, Hamed Fakhim, Saeed Abbasi, Soraya Masoudi, Mahnaz Hosseini Rizi, and Shaghayegh Haghjooy Javanmard. 2023. "The Seroprevalence and Seropositivity of SARS-CoV-2 among Healthcare Workers during the Third Pandemic Wave" Antibodies 12, no. 1: 2. https://doi.org/10.3390/antib12010002
APA StyleVaezi, A., Fakhim, H., Abbasi, S., Masoudi, S., Rizi, M. H., & Haghjooy Javanmard, S. (2023). The Seroprevalence and Seropositivity of SARS-CoV-2 among Healthcare Workers during the Third Pandemic Wave. Antibodies, 12(1), 2. https://doi.org/10.3390/antib12010002