1. Introduction
Psoriasis is a common, complex, and incurable skin condition, affecting the physical, mental, and the social wellbeing of patients. It is characterized by epidermal hyperproliferation and poor differentiation of keratinocytes in the basal layer of the skin, resulting in the formation of pink, heavily scaled plaques on various sites of the body. Many other metabolic abnormalities have also been associated with psoriasis, including low thyroid function, colon problems, accelerated lipid peroxidation, and reduction in the total antioxidant activity [
1,
2]. In recent years, the focus of psoriatic research has been on the methylation cycle [
3], polyamine [
4,
5], folate, vitamin B
12 [
6,
7] and homocysteine levels [
6,
7,
8,
9]. Moreover, several studies have revealed an association between psoriasis and an increased risk of cardiovascular disease, diabetes, and atherosclerosis [
10,
11], highlighting the role of methionine metabolism in the pathogenesis of psoriasis. However, the exact etiology of this association remains unclear.
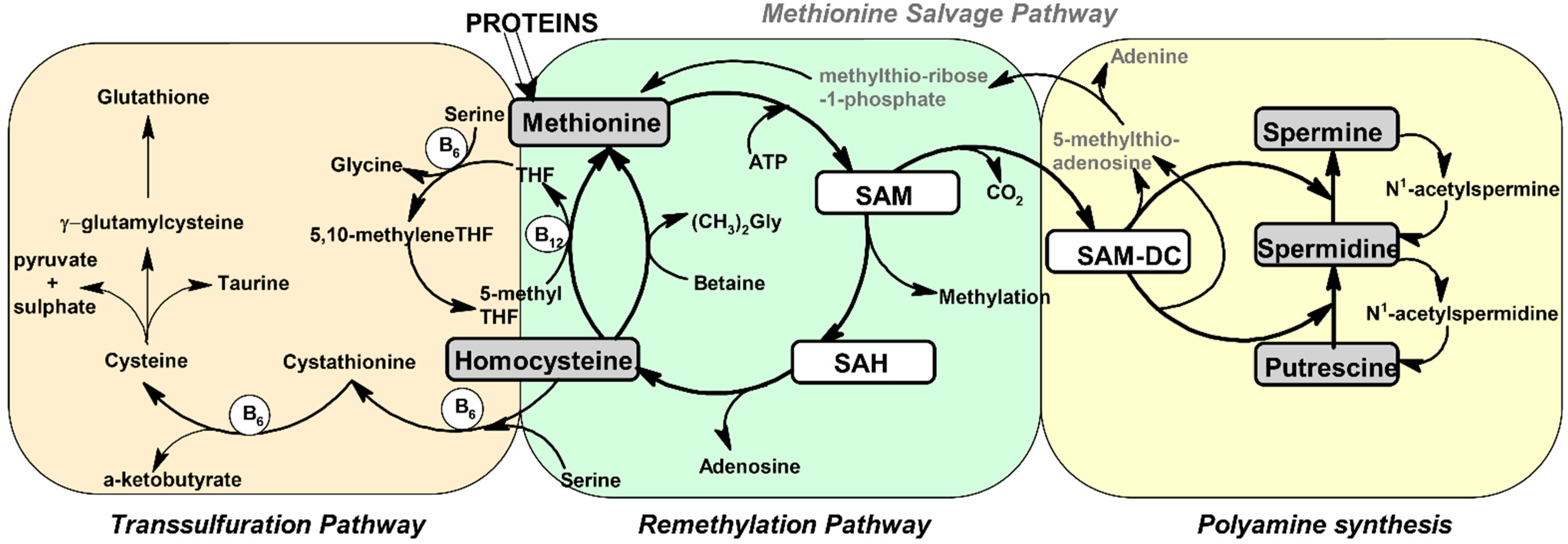
Methionine is a sulfur-containing, proteinogenic amino acid mainly provided by the diet. Its metabolism has a key role in the normal homeostasis of a cell, as it is a supplier of sulfur, propylamine groups, and methyl groups for the biosynthesis of different phospholipids, antioxidant nutrients, and compounds involved in deoxyribonucleic acid (DNA) transcription and ribonucleic acid (RNA) translation processes (
Figure 1). Met is activated by adenosine triphosphate (ATP) in the presence of methionine S-adenosyl transferase, and then the resulting S-adenosylmethionine (SAM) can be demethylated into S-adenosylhomocysteine (SAH) by methyl transferases or decarboxylated into S-adenosylmethioninamine (SAM-DC) by SAM-decarboxylase [
12]. By the decarboxylation reaction, SAM is involved in the synthesis of polyamines as an aminopropyl supplier. The polyamines spermidine and spermine are formed by the addition of aminopropyl groups, derived from SAM-DC, to the putrescine (Put) and Spd, respectively. These two reactions are mediated by spermidine and spermine synthases [
13,
14,
15]. The byproduct of these two reactions is 5-methylthio adenosine, which is used for the re-synthesis of Met by the Methionine salvage pathway in several steps (not discussed in detail here) [
16]. Polyamines are involved in multiple physiological processes, such as cell growth, proliferation, differentiation, immunity, migration, and gene regulation, as well as protein and nucleic acid synthesis [
15].
By the demethylation reaction, SAM plays the role of a vital donor of methyl groups, used for the methylation reactions of DNA, RNA, and numerous neurotransmitters. The product of this reaction, SAH, undergoes hydrolysis to Hcy and adenosine is catalyzed by S-adenosylhomocysteine hydrolase.
Hcy is a non-proteinogenic amino acid, whose normal levels are maintained by two metabolic pathways: Remethylation and transsulfuration. By the remethylation pathway, Hcy is converted into methionine by receiving a methyl group from 5-methyltetrahydrofolate, the active form of folic acid, or betaine. Outside the mitochondria, the reaction relies heavily on the enzyme methionine synthase and requires vitamin B
12 as a cofactor, while inside the mitochondria, the enzyme betaine-homocysteine S-methyltransferase (BHMT) requires betaine. Through the transsulfuration pathway, Hcy condenses with serine to cystathionine by cystathionine β-synthase (CBS) and is then involved in cysteine synthesis by γ-cystathioninase. Both enzymes involved in the transsulfuration pathway are pyridoxal-5′-phosphate-dependent and require vitamin B
6 as cofactor [
12].
Since numerous studies have established a condition of hyperhomocysteinemia (plasma Hcy >15 µM) in psoriatic patients [
7,
9] and alteration in the PA levels in psoriatic lesions [
4,
5], and considering that homocysteine and PA are derived from methionine metabolism [
12,
13,
14,
15], herein we aimed to evaluate the correlation between these metabolites in the skin. As far as we know, the relationship between Hcy, Met, and PA has been slightly neglected in scientific investigations.
The goals of this study were (1) to examine the Met, Hcy, Put, Spd, and Spm levels in serum, saliva, lesions, and non-affected skin; (2) to compare the non-affected skin results with those from lesions; (3) to investigate the possible relationship among the analyte levels in cutaneous samples; (4) to evaluate the possible correlation of each metabolite among the tested samples.
2. Materials and Methods
2.1. Ethics
The survey performed on human skin was conducted after receiving approval from the local ethical committee—the Ethics Committee of the Medical University of Sofia (KENIMUS). All participants received information about the aim of the study and none of them were employed in the research without his or her informed consent. The study was conducted at the Departments of Dermatology and Venereology, Faculty of Medicine, Medical University, Sofia.
2.2. Sample Collection
Twenty-four patients with a mild-to-moderate plaque form of psoriasis vulgaris were enrolled in the study. All subjects were generally healthy. For collection of saliva samples, the participants were asked to provide a 2 mL sample. They were instructed to spit into plastic polyethylene tubes. The collected saliva samples were centrifuged at 13,500 rpm and 4 °C for 10 min, within an hour after the collection procedure, to eliminate debris and cellular matter.
Venous blood samples were drawn from all participants after fasting and collected in heparinized tubes. To obtain serum, the blood samples were centrifuged at 13,500 rpm and 4 °C for 10 min.
The skin samples were taken from the back of the patients via the escribed, standardized epidermal shave technique [
17], based on the method of Arthur and Shelley [
18]. The non-lesional skin samples were taken from the back of the patients, at a minimum of 5 cm from a psoriatic lesion. All epidermal shave biopsies were processed in cryogenic nitrogen and frozen at −196 °C.
The serum, saliva, and skin samples from the psoriatic patients were immediately frozen and stored at −80 °C until assayed.
2.3. Inclusion Criteria
The psoriatic patients were selected with clinical forms of the disease (eruptive, chronic-recurrent, or erythrodermic), aged 18 years or above, and onset of the disease greater than a year. The patients were washed out of any systemic and topical treatment and phototherapy two weeks prior to the investigation.
2.4. Exclusion Criteria
Subjects with obesity/body mass index (BMI) >22, hypertension, metabolic syndrome, thrombophlebitis, and other dermatological diseases were not included in the study. The other exclusion criteria were metabolic syndrome, renal or hepatic failure, hypothyroidism, systemic lupus erythematosus, and central or peripheral vascular accidents, as well as patients taking any antipsoriatic drugs (including methotrexate, folic acid, and acitretin) or drugs affecting homocysteine levels and leading to homocysteinemia.
2.5. Methods
Sample Preparation
To an aliquot of 50 µL of supernatant from the serum and saliva samples were added 20 µL tris(2-carboxyethyl)phosphine hydrochloride (TCEP.HCl) (10 g/L in water). The reaction mixture was incubated for 20 min at 45 °C, and 50 µL of 0.1 M perchloric acid as added. Then, the samples were centrifuged at 13,500 rpm and 4 °C for 10 min.
The tissue samples were accurately weighed in round-bottomed centrifuge tubes, 300 mL of 1 M perchloric acid was added, and the samples were homogenized by mechanical homogenizer at 26,000 rpm (MICCRA 1, ART, Heitersheim, Germany). Then, all samples were centrifuged for 10 min at 4 °C and 13,500 rpm.
2.6. LC-MS/MS Analysis
2.6.1. Equipment
The chromatographic elution of Hcy, Met, Put, Spd, and Spm derivatives was carried out on the Surveyor® Plus high-performance liquid chromatography (HPLC) system, consisting of a binary gradient pump, autosampler, and photodiode array detector (PDA) detector (ThermoScientific Co, San Jose, CA, USA).
Mass analysis was carried out on a linear trap quadrupole (LTQ) Orbitrap® Discovery mass spectrometer (Thermo Scientific Co, San Jose, CA, USA) equipped with electrospray ionization module IonMax® (Thermo Scientific Co, San Jose, CA, USA). Data acquisition and processing were carried out with XCalibur® software package (ThermoScientific Co, San Jose, CA, USA).
All analyses were performed as originally described by Ruseva et al. [
19] with slight modifications in the sample preparation.
In brief, to an aliquot of 70 µL of supernatant was added 20 µL 8 of M acrylamide and incubated for 20 min at 45 °C temperature. Then, 120 µL of buffer solution (0.5 M Na2CO3/NaHCO3 and 5 mM ethylenediaminetetraacetic acid (EDTA)) and 200 µL of derivatizing reagent 1-({[2-(2-fluoro-9-oxoacridin-10(9H)-yl)ethoxy] carbonyl}oxy) pyrrolidine-2,5-dione (FAESC) (5 mM in acetonitrile (ACN)) were added and allowed to react at room temperature for 60 min. The reaction mixture was acidified with 30 µL of concentrated hydrochloric acid. Then, 100 µL of it was diluted with 100 µL of ACN:H2O mixture (50:50). Lastly, 10 µL of diluted samples were used for the analyses.
2.6.2. Statistical Analysis
Statistical analysis was performed using Sigma Plot 12.0 (Systat Software, Inc, San Jose, CA, USA). The normal distribution of the collected data was assessed by the Shapiro–Wilk test. The normality test proved that some of the data sets were abnormally distributed, so the descriptive statistics were expressed as mean ± standard error of the mean (SEM) for normally distributed variables and as medians (minimum and maximum) for the abnormally distributed ones. The comparison of the normally and abnormally distributed data from non-affected skin and lesions were performed according to the Student’s two-tailed t-test and the Mann–Whitney rank sum test, respectively. Differences at a level of p < 0.05 were considered statistically significant. Relationships between the variables were evaluated by Spearman’s rank order correlation coefficients. Statistical significance was accepted for p < 0.05.
3. Results
The study was conducted on a group of 24 patients (11 women and 13 men) with a confirmed diagnosis of psoriasis vulgaris and a mean onset of the disease within 7.58 years. The disease activity was assessed according to the Psoriasis Area and Severity Index (PASI). The disease with a PASI score <10 was classified as a mild, 10–20 as moderate, and <20 as severe psoriasis. The estimation of psoriasis severity showed a mean PASI score of 12.78. The age of the enrolled patients in the study ranged from 21 to 67 years (with a mean of 44.1 years).
The levels of Hcy, Met, Put, Spd, and Spm in the saliva, serum, lesions and non-affective skin were determined. All results obtained for the investigated analytes from the serum, saliva and skin samples, expressed as mean values ± SEM and medians (minimum and maximum), are summarized in
Table 1.
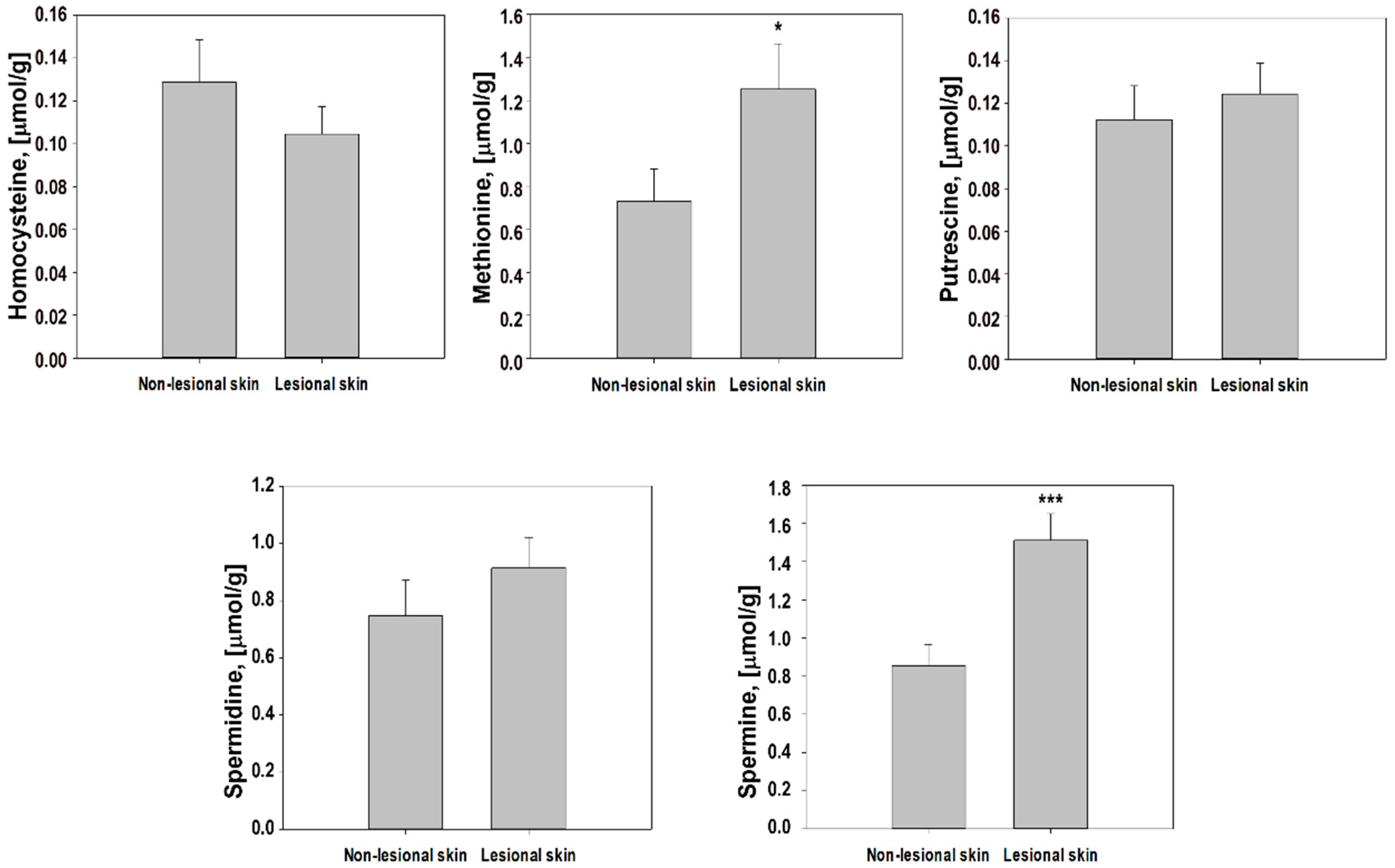
The obtained results for Put, Spd, and Spm from the skin samples were in accordance with the data reported in the literature: Put (non-affected skin: 0.19 ± 0.07 μmol/g and lesions: 0.44 ± 0.28 μmol/g), Spd (non-affected skin: 0.85 ± 0.20 μmol/g and lesions: 1.71 ± 0.36 μmol/g), and Spm (non-affected skin: 0.78 ± 0.13 μmol/g and lesions: 1.96 ± 0.43 μmol/g), respectively [
4,
5]. As far as we know, there are no data about Hcy and Met skin concentrations in the scientific literature. In lesional skin, the levels of Met and Spm increased the most (1.9 times), followed by Put, Spd (1.4 times), and, interestingly, the Hcy level was slightly decreased (0.9 times). The ratio of Spd/Spm, considered as an indicator of proliferation activity, was 0.9 for non-affected skin and 0.6 for lesions. Our results did not support the hypothesis of the significance of the Spd/Spm ratio in the evaluation of the proliferative rate [
17], but confirmed the results reported by Broshtilova et al. [
4,
5].
The data obtained from the serum samples showed that the level of Hcy was greater than 15 µM in the serum (37.8 ± 3.8 µM); therefore, a condition of hyperhomocysteinemia was noted. This condition of psoriatic patients has been observed by other authors [
7,
9] as well. The serum levels of Spm were in accordance with the data reported for psoriatic patients (7.23 µM) [
24]; however, on the contrary, the concentration Spd in our study was a little bit lower than the literature data (5.51 µM) [
24]. To the best of our knowledge, data in the literature about Met and Put in the serum of psoriatic patients are missing.
The salivary levels of Hcy, Met, Put, Spd, and Spm from psoriatic patients are given in
Table 1. Since there is no information about their levels in the literature, we were tempted to use the reported salivary levels of these metabolites from healthy people. Considering the limitations of this comparison, we will not speculate with it. However, the Spm level (47.6 ± 9.7 µM) was found to be drastically higher when compared to the declared values for healthy people (0.63 ± 0.67 μM) [
21,
23]. The eventual difference between these levels could be an interesting direction for future investigations.
3.1. Comparison Analyses
A significant increase in Met (
p < 0.05) and Spm (
p < 0.001) concentrations in the psoriatic plaques were found, in comparison to the non-affected skin results. This result is statistically reliable and supports our assumption about the relationship between the remethylation pathway and PA synthesis. The levels of the other three metabolites practically did not differ, compared to their concentrations from non-affected skin (
p = 0.587 for Hcy,
p = 0.410 for Put, and
p = 0.125 for Spd). The comparison between analyte levels in non-affected skin and lesions from psoriatic patients is given in
Figure 2.
3.2. Correlation Analysis
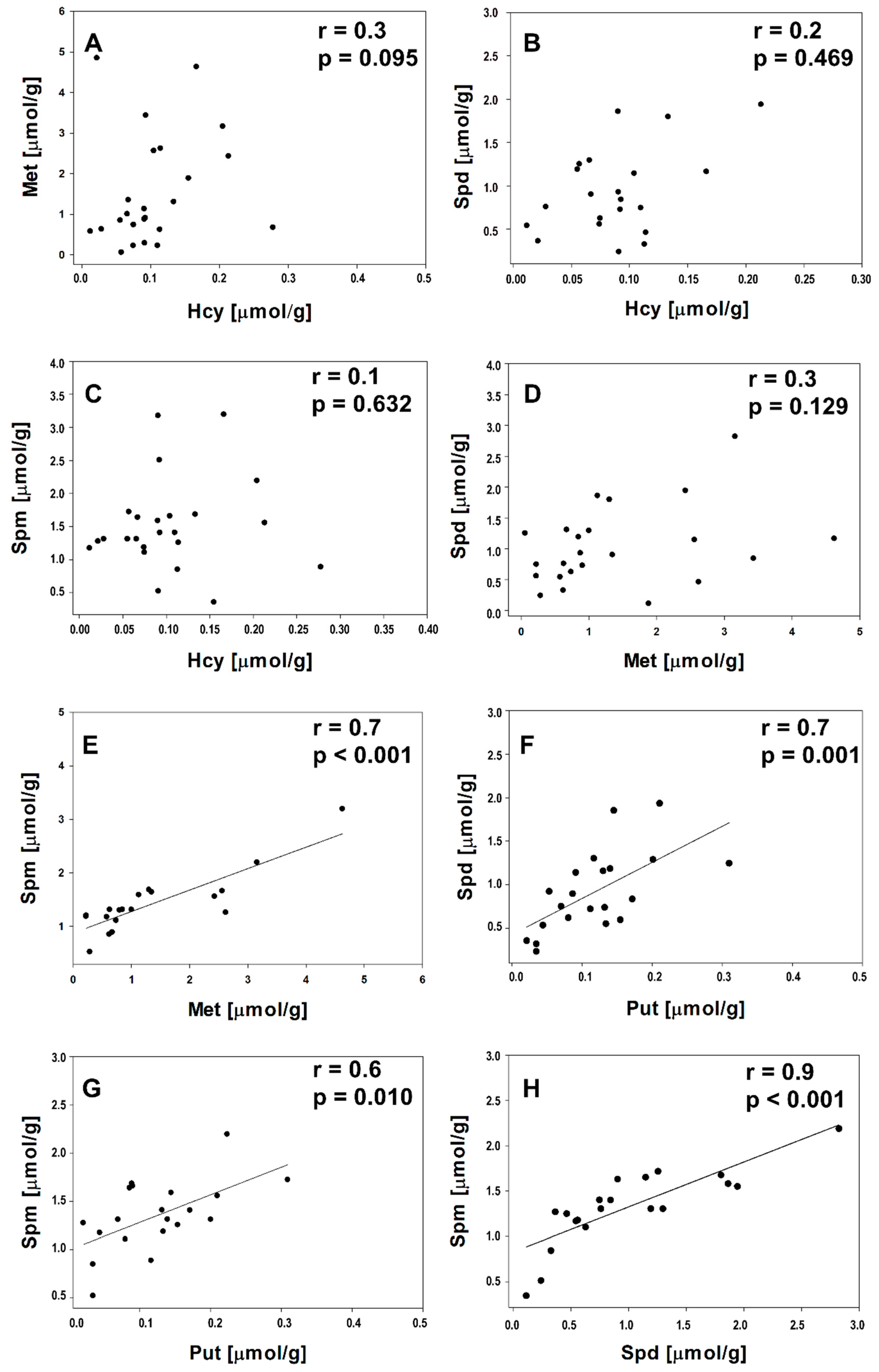
The correlations between Hcy/Met, Hcy/Spd, Hcy/Spm, Met/Spd, Met/Spm, Put/Spd, Put/Spm, and Spd/Spm in the lesions and non-affected skin were statistically evaluated. The correlation coefficients and
p-values from the correlation analyses are shown in
Figure 3 and
Figure 4. In the uninvolved skin of psoriatic patients were observed moderate positive correlations between Hcy/Met (r = 0.6;
p = 0.004), Hcy/Spd (r = 0.6;
p = 0.005), and Met/Spd (r = 0.7;
p < 0.001), whereas the lesions did not show significant correlations between these analyte pairs (
p > 0.05). Statistically significant correlations were found between Met/Spm, Put/Spd, Put/Spm, and Spd/Spm in both types of investigated cutaneous samples: Lesions and non-affected skin (r > 0.7;
p ≤ 0.01).
It is interesting that in the lesional skin, correlations between Hcy/Met, Hcy/Spd, and Met/Spd were not observed. The lack of correlations with the Hcy levels in lesions could signify that normal Hcy metabolic conversions are disrupted in affected skin. The altered Hcy levels in lesions could be explained by acceleration or suppression of both: Transsulfuration or remethylation pathways.
There were no statistically significant correlations (p > 0.05) between the levels of the studied metabolites (Hcy, Met, Put, Spd, and Spm) among the analyzed samples—serum, saliva, lesions, and non-affected skin (data not shown). It is revealed from these results that a direct association of the Hcy, Met, Put, Spd, and Spm levels among the tested samples in psoriasis was missing.
4. Discussion
Multiple scientific studies have reported abnormal metabolism of polyamines [
4,
5,
14] and elevated plasma Hcy levels in psoriatic patients [
7,
9]. Considering the fact that SAM is a conjunction unit for Hcy and polyamine metabolism, in the present article, we examined the eventual relationship between the Hcy level and the increased polyamine synthesis. The obtained data demonstrated that the total serum Hcy level of psoriatic patients (37.8 ± 3.8 µM) was elevated and a condition of hyperhomocysteinemia was observed. This is in accordance with the published data for psoriasis patients [
7,
9].
Since, there is no information in the literature about salivary Hcy, Met, Put, Spd, and Spm levels from psoriatic patients, we were tempted to use the reported salivary levels of these metabolites from healthy people. Considering the limitations of this comparison, we will not speculate with it. However, the Spm level (47.6 ± 9.7 µM) was found to be drastically higher when compared to the declared values for healthy people (0.63 ± 0.67 μM) [
21,
23]. The eventual difference between these levels could be an interesting direction for future investigations.
The lesional and non-lesional skin concentrations of all of the investigated metabolites were compared to elucidate eventual changes of Hcy metabolism, resulting in accelerated polyamine synthesis in damaged skin. The Put, Spd, and Spm levels are in accordance with the literature data [
4,
5]. As far as we know, there are no data about Hcy and Met skin concentrations in the scientific literature. A significant increase in the Met (
p < 0.05) and Spm (
p < 0.001) concentrations in psoriatic plaques were found when compared to non-affected skin (
Figure 2). The levels of the other three metabolites practically did not differ compared to their concentrations in non-affected skin. However, the levels of Met and Spm increased the most in the proliferating tissues, followed by Put and Spd, and interestingly, the Hcy level slightly decreased. Since no significant correlation existed between the lesional skin and the serum Hcy levels, it is unlikely that the cutaneous Hcy content could strongly affect the serum levels. However, bearing in mind the observed condition of hyperhomocysteinemia, possible Hcy eflux in serum cannot be completely excluded. The ratio of Spd/Spm, considered as an indicator of proliferation activity, was 0.9 for non-affected skin and 0.6 for lesions. This result is consistent with the data reported by Brosthilova et al. [
4], but, on the contrary, did not support the hypothesis of the positive correlation between the tissue proliferation activity in the epidermis and the Spd/Spm ratio [
25]. Nevertheless, the statistically significant elevation of the Spm level in the epidermis enhances the possible role of this polyamine in the epidermal hyperplasia.
The findings that the levels of Met and Spm were significantly higher in lesions, when compared to non-affected skin, and the positive correlation between Met/Spm, as well as the correlations among the PA levels in lesions, indicate the tight relationship between these metabolites in affected skin. The observed stimulation of methionine decarboxylation in lesions and Spm synthesis, by incorporation of propylamine groups, corresponds well with the known phenomenon of lower ATP levels in affected tissues. Moreover, the byproduct of the PA biosynthesis 5-methylthio adenosine can be recycled back to methionine via the methionine salvage pathway [
16].
Significant positive correlations (
p ≤ 0.01) were found between Met/Spm, Put/Spd, Put/Spm, and Spd/Spm in both types of investigated cutaneous samples. These results indicate that the metabolic pattern of the investigated compounds in psoriatic patients is identical in the lesions and non-affected skin of psoriatic patients. The observed alterations in the levels of polyamines in lesions may be explained by the accelerated polyamine synthesis—Spm in particular. In the uninvolved skin were evidenced high correlations between Hcy/Met, Hcy/Spd, and Met/Spd, which were not observed in the lesions. These findings, together with the significantly elevated Met and Spm levels in lesions, indicate that the high polyamine levels could be a result of an imbalance in Hcy metabolism, particularly a disturbance in the transsulfuration pathway. This is consistent with the fact that SAM (the precursor for Hcy, Spd, and Spm synthesis) is a key determinant in the regulation of Hcy metabolism. The accumulation of SAM stimulates the transsulfuration pathway by increasing CBS activity and decrease the level of potentially cytotoxic Hcy. Duran et al. showed that a decrease in the tissue concentration of SAM induces inhibition of Hcy catabolism by transsulfuration [
12]. Contributing to this assumption is the confirmed correlation between the skin Spd/Spm levels, which other authors have interpreted as an indication of the major role of S-adenosyl-L-methionine decarboxylase—the enzyme responsible for the decarboxylation of SAM [
5].
The acceleration of PA synthesis could lead to the depletion of SAM; therefore, it is possible to affect the methylation ability of the cell and the remethylation and transsulfuration pathways of Hcy metabolism. Alterations Alternations in these metabolic reactions could lead to hypomethylation, a decrease in cysteine and gluthathione level, and an impact on the antioxidant activity of cells. All of these abnormalities have been reported in psoriatic patients [
3,
26]. Moreover, this suggestion is supported by the reported data about the benefits of a low-protein diet for psoriasis patients [
26].








{kind=link}
{kind=link}
{kind=link}
{kind=link}