



Self-Mobilization Exercise Program Improved Postural Stability in the Anterior-Posterior Direction with Eyes Closed


Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Interventions
2.3. Procedures and Measurements
2.4. Statistical Analysis
3. Results
3.1. Subjects
3.2. Sway Parameters in Eyes-Open Condition
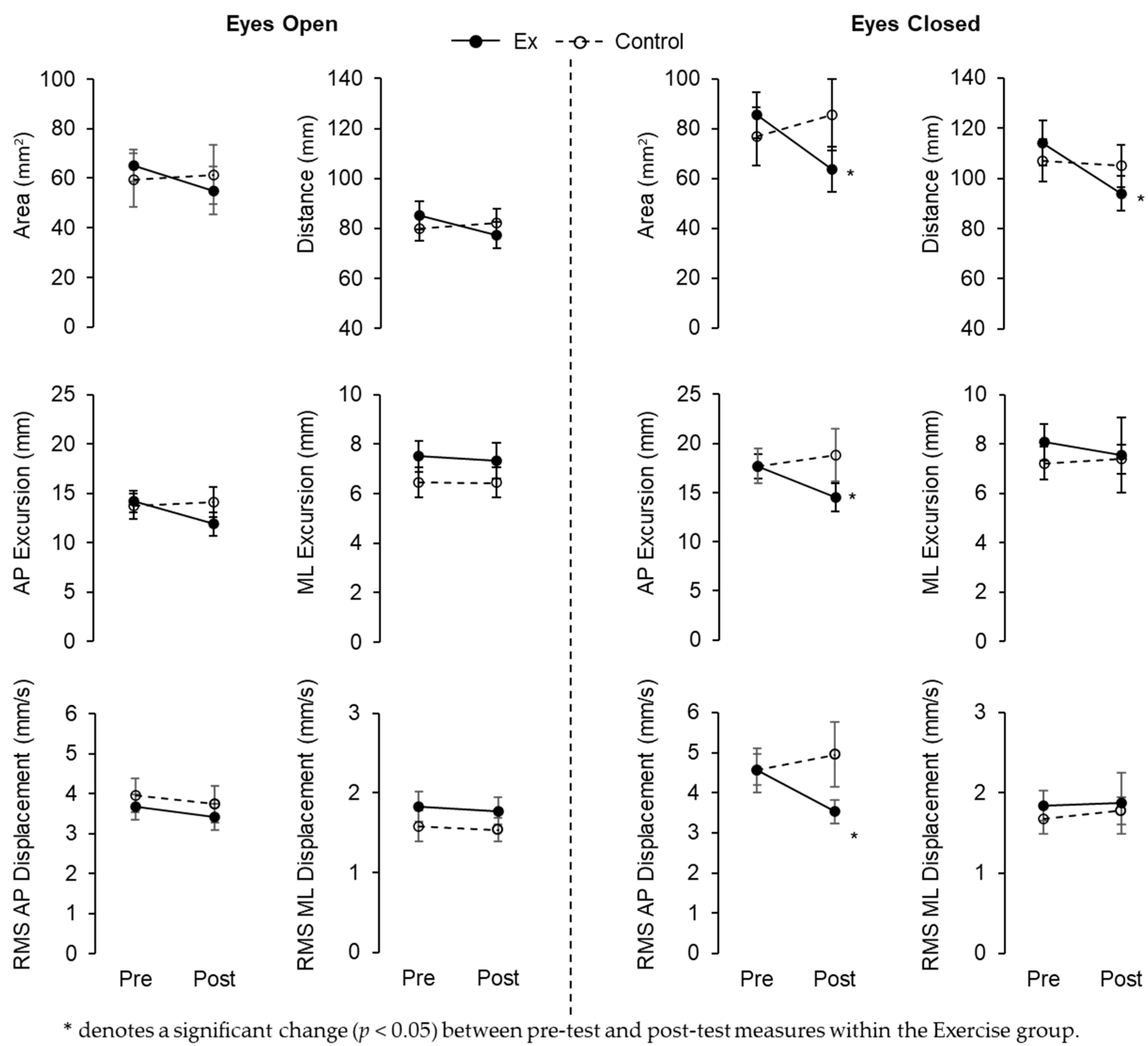
3.3. Sway Parameters in Eyes-Closed Condition
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Enoka, R.M. Neural Control of Movement. In Neuromechanics of Human Movement, 5th ed.; Human Kinetics: Champaign, IL, USA, 2015. [Google Scholar]
- Wade, M.G.; Jones, G. The Role of Vision and Spatial Orientation in the Maintenance of Posture. Phys. Ther. 1997, 619, 619–628. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kavounoudias, A.; Roll, R.; Roll, J.P. Foot Sole and Ankle Muscle Inputs Contribute Jointly to Human Erect Posture Regulation. J. Physiol. 2001, 532, 869–878. [Google Scholar] [CrossRef] [PubMed]
- Teasdale, N.; Furmanek, M.P.; Germain Robitaille, M.; de Oliveira, F.C.L.; Simoneau, M. Sensory Integration during Vibration of Postural Muscle Tendons When Pointing to a Memorized Target. Front. Hum. Neurosci. 2017, 10, 682. [Google Scholar] [CrossRef] [Green Version]
- Qiu, F.; Cole, M.H.; Davids, K.W.; Hennig, E.M.; Silburn, P.A.; Netscher, H.; Kerr, G.K. Enhanced Somatosensory Information Decreases Postural Sway in Older People. Gait Posture 2012, 35, 630–635. [Google Scholar] [CrossRef]
- Goble, D.J.; Coxon, J.P.; Van Impe, A.; Geurts, M.; Doumas, M.; Wenderoth, N.; Swinnen, S.P. Brain Activity during Ankle Proprioceptive Stimulation Predicts Balance Performance in Young and Older Adults. J. Neurosci. 2011, 31, 16344–16352. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guskiewicz, K.M. Balance Assessment in the Management of Sport-Related Concussion. Clin. Sport. Med. 2011, 30, 89–102, ix. [Google Scholar] [CrossRef]
- Allum, J.H.J.; Adkin, A.L.; Carpenter, M.G.; Held-Ziolkowska, M.; Honegger, F.; Pierchala, K. Trunk Sway Measures of Postural Stability during Clinical Balance Tests: Effects of a Unilateral Vestibular Deficit. Gait Posture 2001, 14, 227–237. [Google Scholar] [CrossRef]
- Morton, S.M.; Bastian, A.J. Cerebellar Control of Balance and Locomotion. Neuroscientist 2004, 10, 247–259. [Google Scholar] [CrossRef]
- Goodwin, G.M.; Mccloskey, D.I.; Matthews, P.B.C. Proprioceptive Illusions Induced by Muscle Vibration: Contribution by Muscle Spindles to Perception? Science 1972, 175, 1382–1384. [Google Scholar] [CrossRef]
- Edin, B.B.; Johansson, N. Skin Strain Patterns Provide Kinaesthetic Information to the Human Central Nervous System. J. Physiol. 1995, 487, 243–251. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Burgess, P.R.; Wei, J.Y.; Clark, F.J.; Simon, J. Signaling of Kinesthetic Information by Peripheral Sensory Receptors. Annu. Rev. Neurosci. 1982, 5, 171–187. [Google Scholar] [CrossRef]
- Adamcova, N.; Hlavacka, F. Modification of Human Postural Responses to Soleus Muscle Vibration by Rotation of Visual Scene. Gait Posture 2007, 25, 99–105. [Google Scholar] [CrossRef]
- Ceyte, H.; Cian, C.; Zory, R.; Barreaud, P.-A.; Roux, A.; Guerraz, M. Effects of Bilateral Achilles Tendon Vibration on Postural Orientation. Neurosci. Lett. 2007, 416, 71–75. [Google Scholar] [CrossRef] [PubMed]
- Imagama, S.; Ito, Z.; Wakao, N.; Seki, T.; Hirano, K.; Muramoto, A.; Sakai, Y.; Matsuyama, Y.; Hamajima, N.; Ishiguro, N.; et al. Influence of Spinal Sagittal Alignment, Body Balance, Muscle Strength, and Physical Ability on Falling of Middle-Aged and Elderly Males. Eur. Spine J. 2013, 22, 1346–1353. [Google Scholar] [CrossRef] [PubMed]
- Shibata, D. Gait & Posture Improvement of Dynamic Postural Stability by an Exercise Program. Gait Posture 2020, 80, 178–184. [Google Scholar] [CrossRef] [PubMed]
- Hee Lee, J. Effects of Forward Head Posture on Static and Dynamic Balance Control. J. Phys. Ther. Sci. 2016, 28, 274–277. [Google Scholar] [CrossRef] [Green Version]
- Kang, J.-H.; Park, R.-Y.; Lee, S.-J.; Kim, J.-Y.; Yoon, S.-R.; Jung, K.-I. The Effect of the Forward Head Posture on Postural Balance in Long Time Computer Based Worker. Ann. Rehabil. Med. 2012, 36, 98–104. [Google Scholar] [CrossRef] [Green Version]
- O’Neil, D.; Olafsdottir, K.; Caneiro, J.P.; Barach, A.; Tveit, O.; Burnett, A.; O’Sullivan, P. The Influence of Different Sitting Postures on Head/Neck Posture and Muscle Activity. Man. Ther. 2009, 15, 54–60. [Google Scholar] [CrossRef]
- Nurwulan, N.R.; Jiang, B.C.; Iridiastadi, H. Posture and Texting: Effect on Balance in Young Adults. PLoS ONE 2015, 10, e0134230. [Google Scholar] [CrossRef]
- Vuillerme, N.; Rougier, P. Effects of Head Extension on Undisturbed Upright Stance Control in Humans. Gait Posture 2005, 21, 318–325. [Google Scholar] [CrossRef]
- Yokoyama, S.; Gamada, K.; Sugino, S.; Sasano, R. The Effect of “the Core Conditioning Exercises” Using the Stretch Pole on Thoracic Expansion Difference in Healthy Middle-Aged and Elderly Persons. J. Bodyw. Mov. Ther. 2012, 16, 326–329. [Google Scholar] [CrossRef]
- Sadakiyo, M.; Sugino, S.; Gamada, K.; Yamamoto, D.; Yokoyama, S. Effectiveness of Core-Conditioning Exercises Using a Stretch-Pole on the Spinal Realingmnet and Flexibility: A Single-Blinded Randomized Control Trial. In Proceedings of the 15th International Congress of the World Confederation for Physical Therapy, Vancouver, BC, Canada, 2–7 June 2007. [Google Scholar]
- Palmieri, R.M.; Ingersoll, C.D.; Stone, M.B.; Krause, B.A. Center-of-Pressure Parameters Used in the Assessment of Postural Control. J. Sport Rehabil. 2002, 11, 51–66. [Google Scholar] [CrossRef] [Green Version]
- Boruah, K. Effectiveness of Thoracic Core Conditioning Using Stretch Pole for Community Elderly with Moderate COPD-A Single Blind Study. Int. J. Physiother. Res. 2014, 2, 394–402. [Google Scholar]
- Kim, C.-B.; Yang, J.-M.; Choi, J.-D. The Effects of Chest Expansion Resistance Exercise on Chest Expansion and Maximal Respiratory Pressure in Elderly with Inspiratory Muscle Weakness. J. Phys. Ther. Sci. 2015, 27, 1121–1124. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Niam, S.; Cheung, W.; Sullivan, P.E.; Kent, S.; Gu, X. Balance and Physical Impairments after Stroke. Arch. Phys. Med. Rehabil. 1999, 80, 1227–1233. [Google Scholar] [CrossRef] [PubMed]
- Winter, D.A. Human Balance and Posture Control during Standing and Walking. Gait Posture 1995, 3, 193–214. [Google Scholar] [CrossRef]
- Lee, S.P.; Souza, R.B.; Powers, C.M. The Influence of Hip Abductor Muscle Performance on Dynamic Postural Stability in Females with Patellofemoral Pain. Gait Posture 2012, 36, 425–429. [Google Scholar] [CrossRef] [PubMed]
- Thompson, C.; Bélanger, M.; Fung, J. Effects of Plantar Cutaneo-Muscular and Tendon Vibration on Posture and Balance during Quiet and Perturbed Stance. Hum. Mov. Sci. 2011, 30, 153–171. [Google Scholar] [CrossRef]
- Peterka, R.J. Sensorimotor Integration in Human Postural Control. J. Neurophysiol. 2002, 88, 1097–1118. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oie, K.S.; Kiemel, T.; Jeka, J.J. Multisensory Fusion: Simultaneous Re-Weighting of Vision and Touch for the Control of Human Posture. Cogn. Brain Res. 2002, 14, 164–176. [Google Scholar] [CrossRef]


{kind=link}
| Exercise (n = 16) | Control (n = 16) | |
|---|---|---|
| Age (years) | 22.44 ± 5.39 | 22.81 ± 6.15 |
| Sex (male/female) | 9/7 | 9/7 |
| Height (cm) | 170.33 ± 10.32 | 168.63 ± 11.62 |
| Weight (kg) | 71.32 ± 17.85 | 73.72 ± 21.34 |
| Body mass index (kg/m2) | 24.34 ± 4.18 | 25.50 ± 5.08 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shibata, D.; Yoshida, Y. Self-Mobilization Exercise Program Improved Postural Stability in the Anterior-Posterior Direction with Eyes Closed. Symmetry 2023, 15, 1321. https://doi.org/10.3390/sym15071321
Shibata D, Yoshida Y. Self-Mobilization Exercise Program Improved Postural Stability in the Anterior-Posterior Direction with Eyes Closed. Symmetry. 2023; 15(7):1321. https://doi.org/10.3390/sym15071321
Chicago/Turabian StyleShibata, Daisuke, and Yuri Yoshida. 2023. "Self-Mobilization Exercise Program Improved Postural Stability in the Anterior-Posterior Direction with Eyes Closed" Symmetry 15, no. 7: 1321. https://doi.org/10.3390/sym15071321
APA StyleShibata, D., & Yoshida, Y. (2023). Self-Mobilization Exercise Program Improved Postural Stability in the Anterior-Posterior Direction with Eyes Closed. Symmetry, 15(7), 1321. https://doi.org/10.3390/sym15071321