
Kinematics, Speed, and Anthropometry-Based Ankle Joint Torque Estimation: A Deep Learning Regression Approach





Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Acquisition
2.1.1. Participants
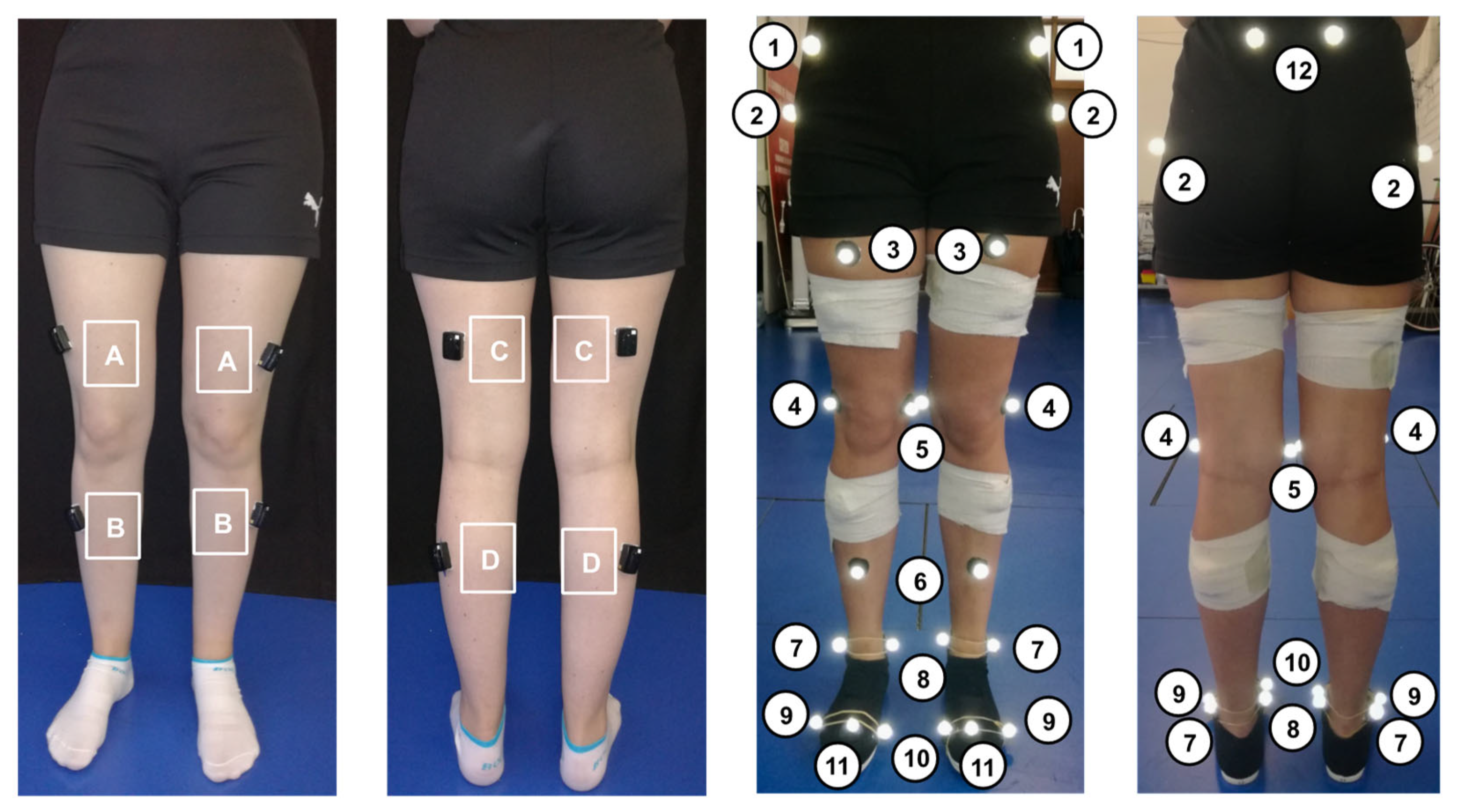
2.1.2. Instrumentation and Data Collection
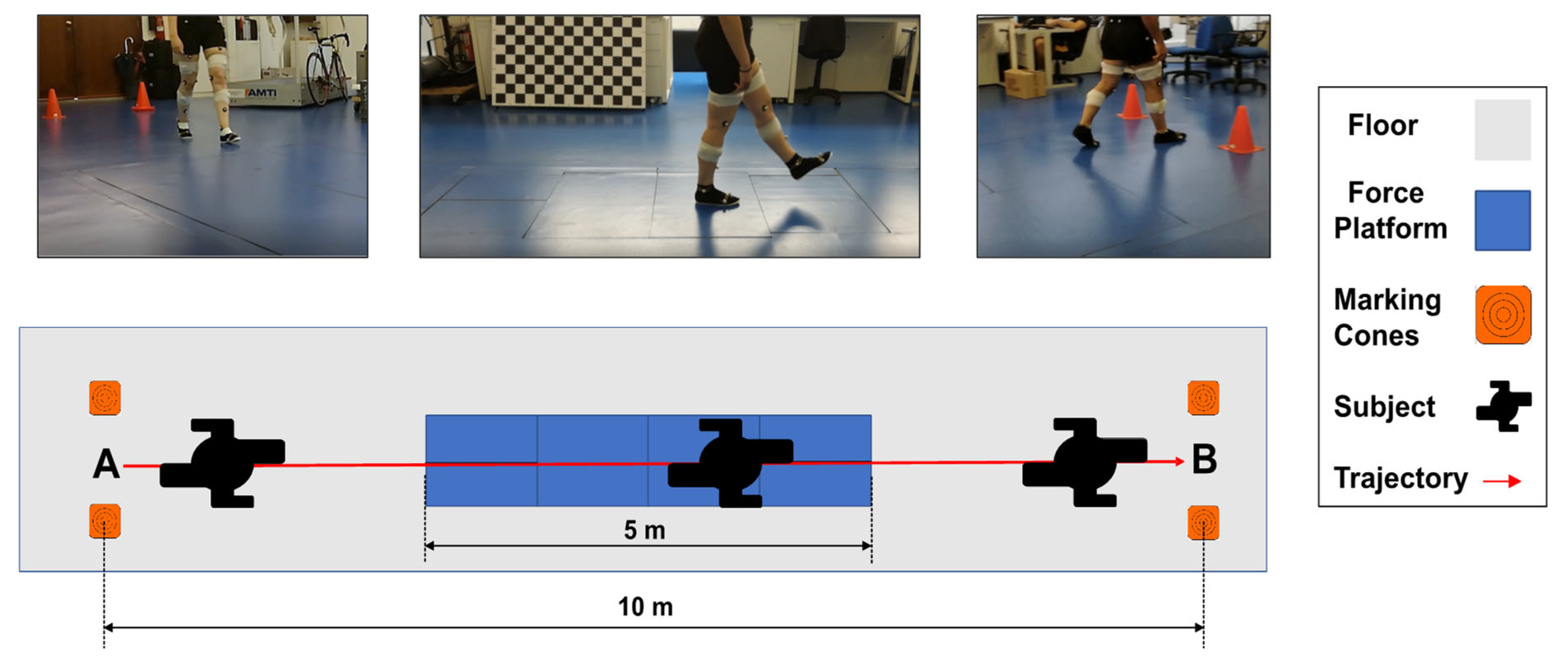
2.1.3. Experimental Protocol
2.2. Data Processing
2.3. Data Preparation
2.4. Implementation of the Regression Models
2.5. Model Evaluation Metrics
3. Results
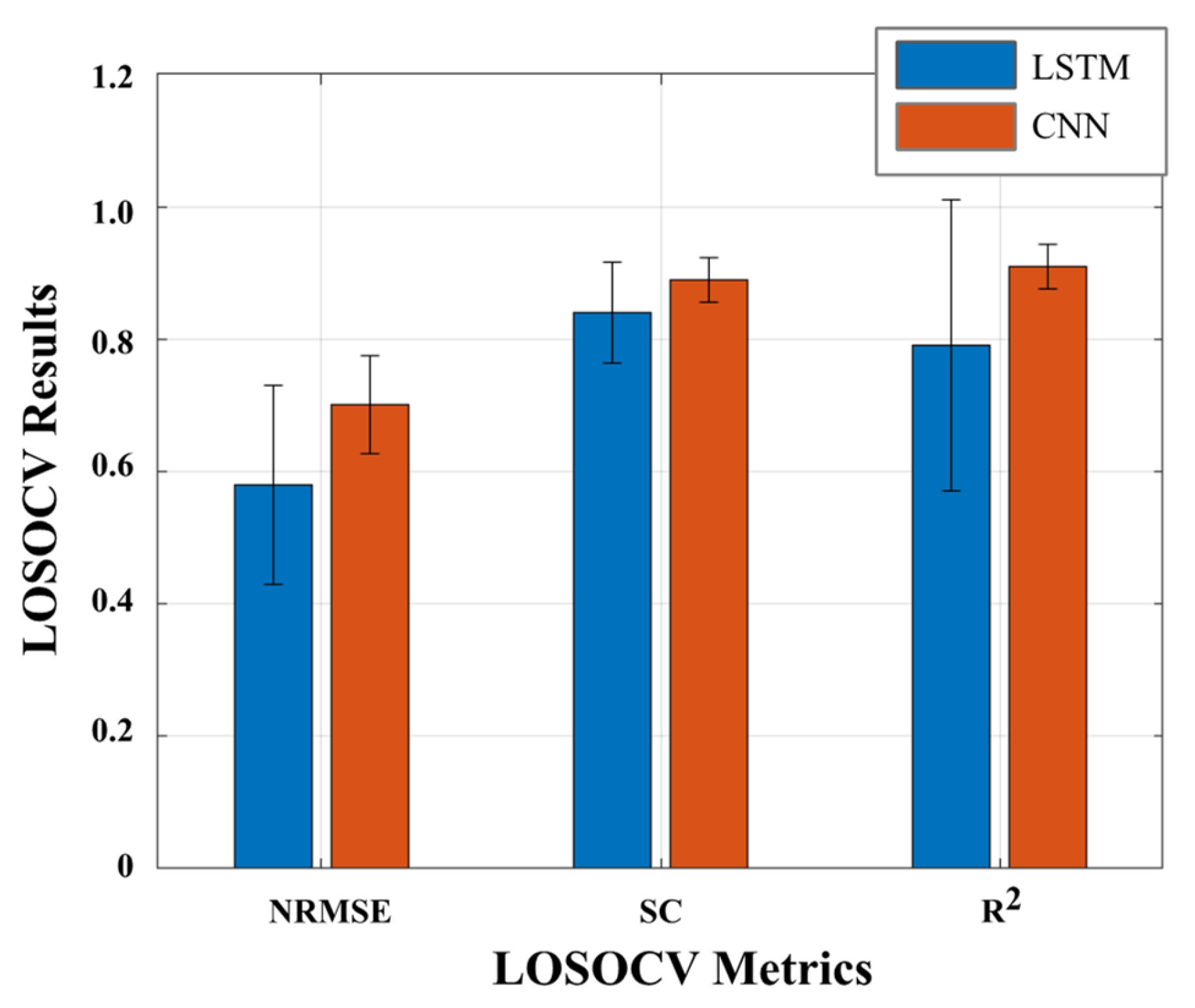
3.1. Comparative Analysis of Regression Models without Using EMG Signals
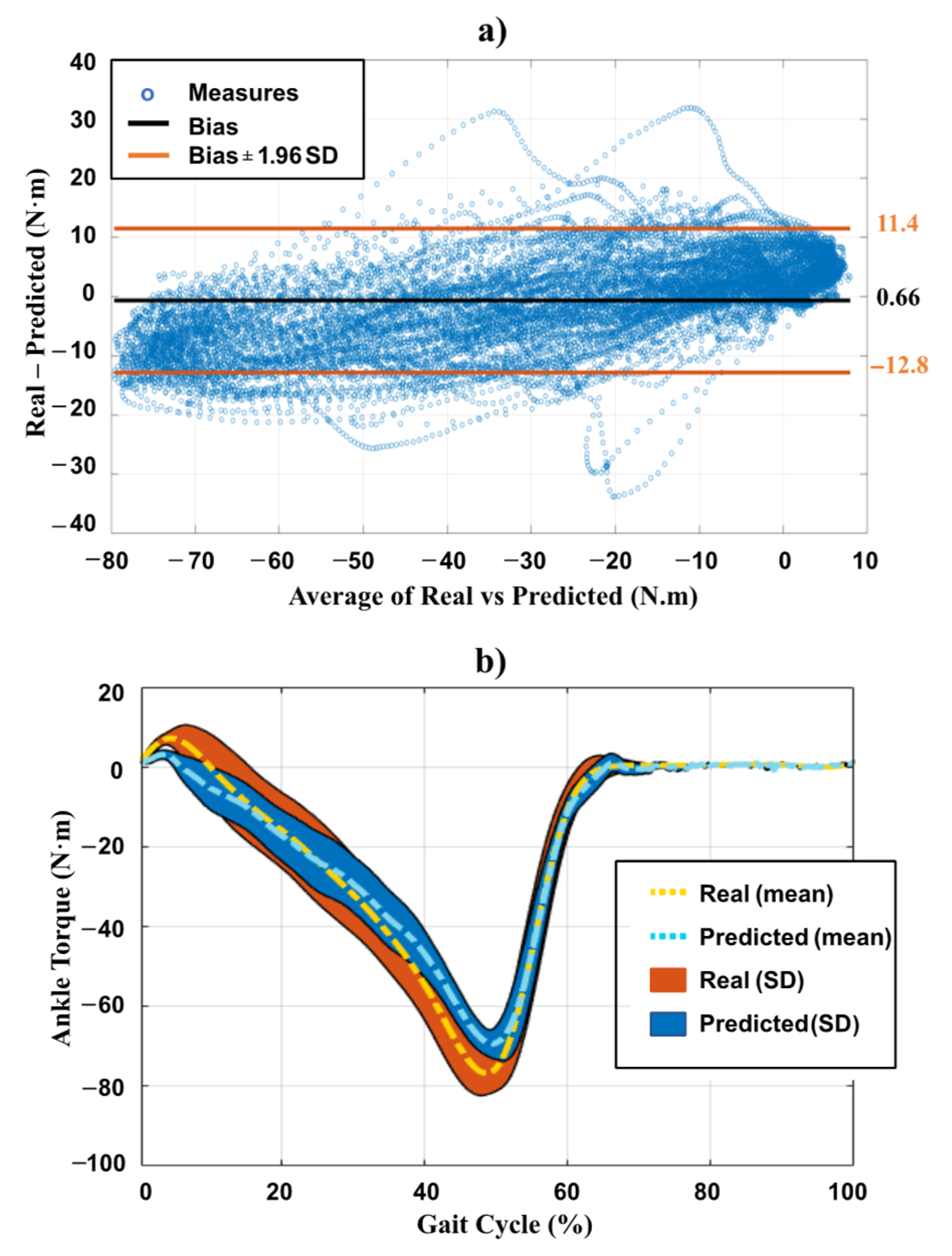
3.2. Detailed Analysis of CNN Performance
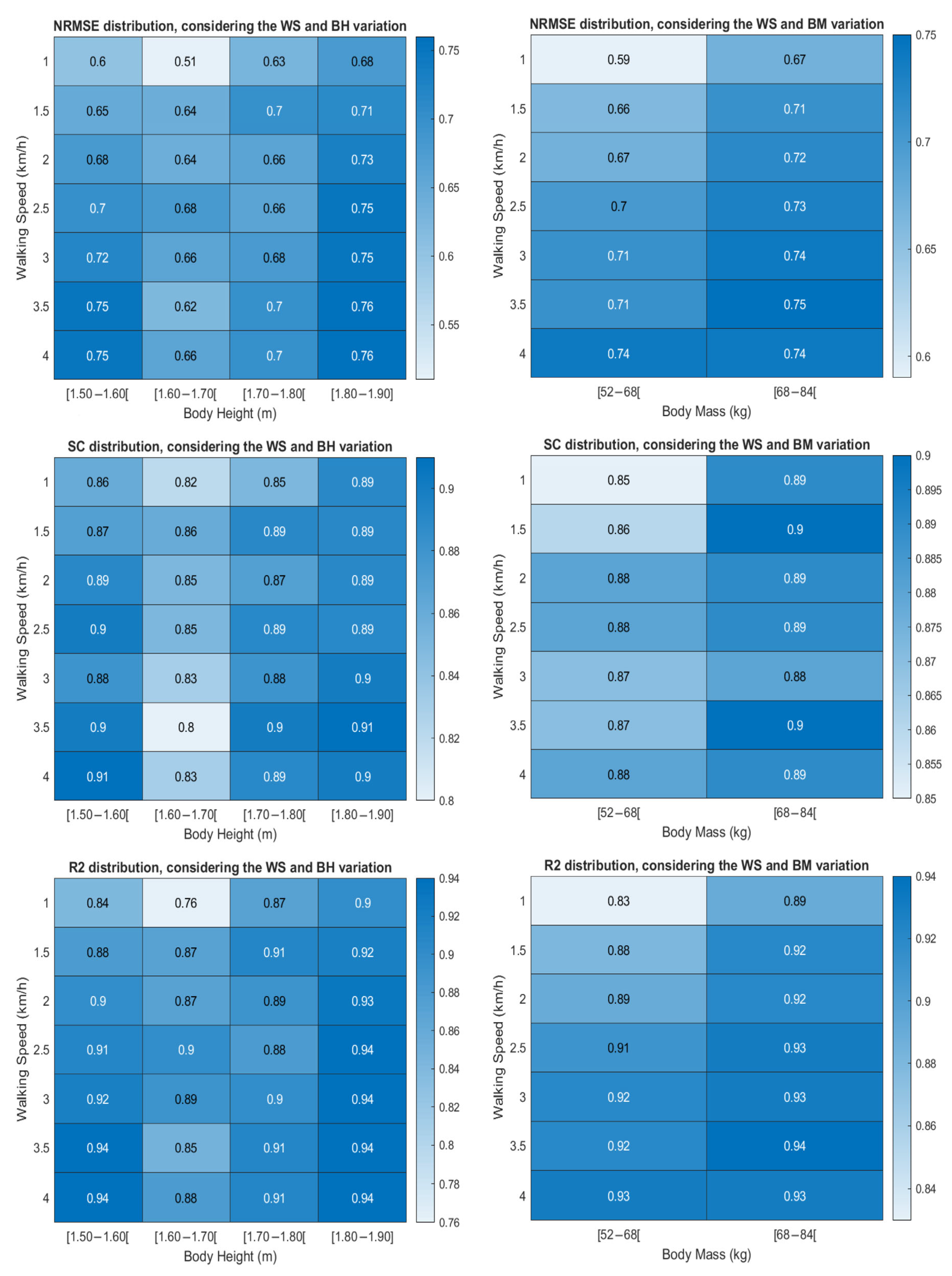
3.3. Walking Speed Versus Body Mass and Height Analysis
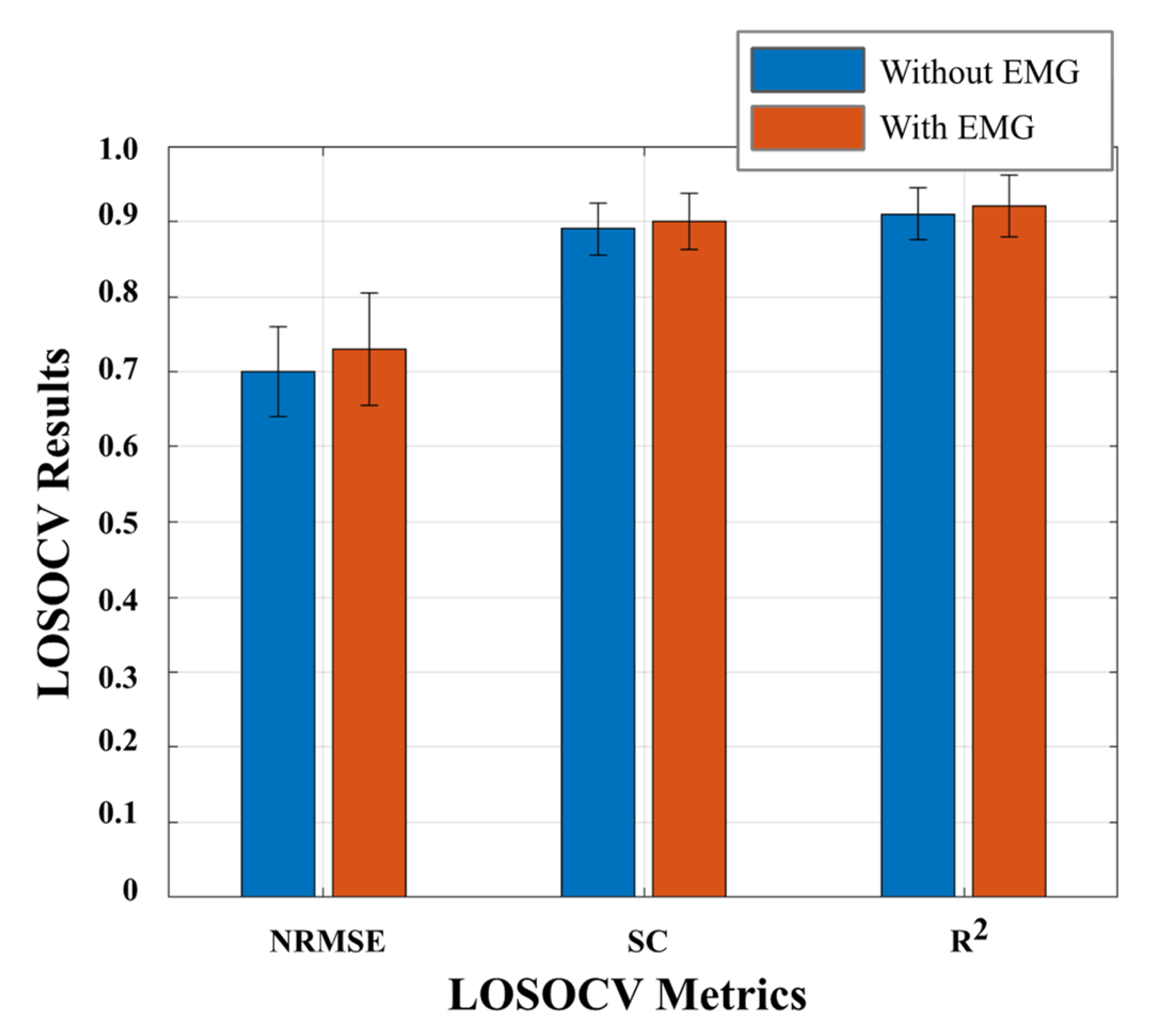
3.4. EMG Inclusion for Ankle Joint Torque Prediction
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Sample 1–Sample 2 | Metric | Z | p-Value |
|---|---|---|---|
| 1.0–1.5 km/h | NRMSE | −2.35 | 0.02 |
| SC | −1.33 | 0.18 | |
| R2 | −2.35 | 0.02 | |
| 1.0–2.0 km/h | NRMSE | −2.59 | 0.01 |
| SC | −1.57 | 0.12 | |
| R2 | −2.43 | 0.02 | |
| 1.0–2.5 km/h | NRMSE | −2.82 | 0.01 |
| SC | −1.65 | 0.10 | |
| R2 | −2.82 | 0.01 | |
| 1.0–3.0 km/h | NRMSE | −3.06 | 0.00 |
| SC | −1.10 | 0.27 | |
| R2 | −3.06 | 0.00 | |
| 1.0–3.5 km/h | NRMSE | −3.06 | 0.00 |
| SC | −1.26 | 0.21 | |
| R2 | −3.06 | 0.00 | |
| 1.0–4.0 km/h | NRMSE | −3.06 | 0.00 |
| SC | −1.57 | 0.12 | |
| R2 | −3.06 | 0.00 | |
| 1.5–2.0 km/h | NRMSE | −1.41 | 0.16 |
| SC | −0.47 | 0.64 | |
| R2 | −1.33 | 0.18 | |
| 1.5–2.5 km/h | NRMSE | −1.26 | 0.21 |
| SC | 0.00 | 1.00 | |
| R2 | −1.18 | 0.24 | |
| 1.5–3.0 km/h | NRMSE | −1.33 | 0.18 |
| SC | −0.47 | 0.64 | |
| R2 | −1.33 | 0.18 | |
| 1.5–3.5 km/h | NRMSE | −1.33 | 0.18 |
| SC | −0.47 | 0.64 | |
| R2 | −1.26 | 0.21 | |
| 1.5–4.0 km/h | NRMSE | −1.26 | 0.21 |
| SC | −0.55 | 0.58 | |
| R2 | −1.26 | 0.21 | |
| 2.0–2.5 km/h | NRMSE | −1.18 | 0.24 |
| SC | −0.62 | 0.53 | |
| R2 | −1.26 | 0.21 | |
| 2.0–3.0 km/h | NRMSE | −1.02 | 0.31 |
| SC | −0.47 | 0.64 | |
| R2 | −1.18 | 0.24 | |
| 2.0–3.5 km/h | NRMSE | −1.10 | 0.27 |
| SC | −0.28 | 0.78 | |
| R2 | −1.02 | 0.31 | |
| 2.0–4.0 km/h | NRMSE | −1.33 | 0.18 |
| SC | -0.39 | 0.70 | |
| R2 | −1.10 | 0.27 | |
| 2.5–3.0 km/h | NRMSE | −0.08 | 0.94 |
| SC | −0.78 | 0.43 | |
| R2 | 0.00 | 1.00 | |
| 2.5–3.5 km/h | NRMSE | −0.71 | 0.48 |
| SC | −0.47 | 0.64 | |
| R2 | −0.08 | 0.94 | |
| 2.5–4.0 km/h | NRMSE | −0.63 | 0.53 |
| SC | −0.55 | 0.58 | |
| R2 | −0.55 | 0.58 | |
| 3.0–3.5 km/h | NRMSE | −0.55 | 0.58 |
| SC | −1.02 | 0.31 | |
| R2 | −0.47 | 0.64 | |
| 3.0–4.0 km/h | NRMSE | −0.94 | 0.35 |
| SC | −0.63 | 0.53 | |
| R2 | −0.78 | 0.43 | |
| 3.5–4.0 km/h | NRMSE | −1.10 | 0.27 |
| SC | −0.23 | 0.81 | |
| R2 | −0.94 | 0.35 |
| Walking Speed | Metric | Body Height | Body Mass | ||
|---|---|---|---|---|---|
| Kruskal–Wallis H | p-Value | Kruskal–Wallis H | p-Value | ||
| 1.0 km/h | NRMSE | 5.54 | 0.17 | 2.38 | 0.12 |
| SC | 5.08 | 0.17 | 1.11 | 0.29 | |
| R2 | 5.54 | 0.14 | 2.38 | 0.12 | |
| 1.5 km/h | NRMSE | 1.52 | 0.68 | 0.80 | 0.37 |
| SC | 1.52 | 0.68 | 0.80 | 0.37 | |
| R2 | 1.52 | 0.68 | 0.80 | 0.37 | |
| 2.0 km/h | NRMSE | 3.98 | 0.26 | 0.32 | 0.57 |
| SC | 5.44 | 0.14 | 0.16 | 0.68 | |
| R2 | 3.98 | 0.26 | 0.32 | 0.57 | |
| 2.5 km/h | NRMSE | 2.69 | 0.44 | 0.53 | 0.46 |
| SC | 4.38 | 0.22 | 0.06 | 0.80 | |
| R2 | 2.69 | 0.44 | 0.53 | 0.46 | |
| 3.0 km/h | NRMSE | 3.98 | 0.26 | 1.11 | 0.29 |
| SC | 4.21 | 0.24 | 0.01 | 0.94 | |
| R2 | 3.98 | 0.26 | 1.11 | 0.29 | |
| 3.5 km/h | NRMSE | 4.77 | 0.19 | 0.80 | 0.37 |
| SC | 4.85 | 0.18 | 0.01 | 0.94 | |
| R2 | 4.77 | 0.19 | 0.78 | 0.37 | |
| 4.0 km/h | NRMSE | 3.14 | 0.37 | 0.01 | 0.94 |
| SC | 4.96 | 0.18 | 0.06 | 0.81 | |
| R2 | 3.14 | 0.37 | 0.01 | 0.94 | |
References
- Johnson, W.; Onuma, O.; Owolabi, M.; Sachdev, S.; Bulletin of World Health Organization. Stroke: A Global Response Is Needed. 2016. Available online: https://www.who.int/bulletin/volumes/94/9/16-181636/en/ (accessed on 5 June 2019).
- Johnson, C.O.; Nguyen, M.; Roth, G.A.; Nichols, E.; Alam, T.; Abate, D.; Abd-Allah, F.; Abdelalim, A.; Abraha, H.N.; Abu-Rmeileh, N.M.; et al. Global, regional, and national burden of stroke, 1990–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet Neurol. 2019, 18, 439–458. [Google Scholar] [CrossRef] [Green Version]
- Rajsic, S.; Gothe, H.; Borba, H.H.; Sroczynski, G.; Vujicic, J.; Toell, T.; Siebert, U. Economic burden of stroke: A systematic review on post-stroke care. Eur. J. Health Econ. 2019, 20, 107–134. [Google Scholar] [CrossRef]
- Luengo-Fernandez, R.; Leal, J.; Candio, P.; Violato, M. The Economic Impact of Stroke in Europe: Current Costs of Stroke throughout Europe. Eur. Stroke J. 2019, 5, 17–25. [Google Scholar] [CrossRef] [PubMed]
- Li, S.; Francisco, G.E.; Zhou, P. Post-stroke Hemiplegic Gait: New Perspective and Insights. Front. Physiol. 2018, 9, 1021. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Da Saúde, D.G. Programa Nacional de Prevenção e Controlo das Doenças Cardiovasculares. Dgs. 2006, p. 28. Available online: https://www.google.pt/url?sa=t&rct=j&q=&esrc=s&source=web&cd=1&cad=rja&uact=8&ved=0ahUKEwin1rHhmc3MAhUDuhoKHYOvAe4QFggiMAA&url=http://1nj5ms2lli5hdggbe3mm7ms5.wpengine.netdna-cdn.com/files/2015/08/Programa-Nacional-de-Prevencao-das-Doencas-Cardiovasculare (accessed on 4 August 2021).
- Tucker, M.R.; Olivier, L.; Pagel, A.; Bleuler, H.; Bouri, M.; Lambercy, O.; Millán, J.D.R.; Riener, R.; Vallery, H.; Gassert, R. Control strategies for active lower extremity prosthetics and orthotics: A review. J. Neuroeng. Rehabil. 2015, 12, 1. [Google Scholar] [CrossRef] [Green Version]
- Jamwal, P.K.; Xie, S.Q.; Hussain, S.; Parsons, J.G. An Adaptive Wearable Parallel Robot for the Treatment of Ankle Injuries. IEEE/ASME Trans. Mechatron. 2012, 19, 64–75. [Google Scholar] [CrossRef]
- Meng, W.; Liu, Q.; Zhou, Z.; Ai, Q.; Sheng, B.; Xie, S. Recent development of mechanisms and control strategies for robot-assisted lower limb rehabilitation. Mechatronics 2015, 31, 132–145. [Google Scholar] [CrossRef]
- Figueiredo, J.S.C. Smart wearable orthosis to assist impaired human walking. Ph.D. Thesis, University of Minho, Braga, Portugal, 2019. [Google Scholar]
- Fleischer, C.; Hommel, G. A Human--Exoskeleton Interface Utilizing Electromyography. IEEE Trans. Robot. 2008, 24, 872–882. [Google Scholar] [CrossRef]
- Hassani, W.; Mohammed, S.; Rifai, H.; Amirat, Y. EMG based approach for wearer-centered control of a knee joint actuated orthosis. In Proceedings of the 2013 IEEE/RSJ International Conference on Intelligent Robots and Systems, Tokyo, Japan, 3–7 November 2013; pp. 990–995. [Google Scholar]
- Hassani, W.; Mohammed, S.; Amirat, Y. Real-Time EMG Driven Lower Limb Actuated Orthosis for Assistance as Needed Movement Strategy. In Proceedings of the Robotics: Science and Systems 2013, Berlin, Germany, 24−28 June 2013. [Google Scholar]
- Hassani, W.; Mohammed, S.; Rifaï, H.; Amirat, Y. Powered orthosis for lower limb movements assistance and rehabilitation. Control. Eng. Pract. 2014, 26, 245–253. [Google Scholar] [CrossRef]
- Zhang, J.; Cheah, C.C.; Collins, S.H. Experimental comparison of torque control methods on an ankle exoskeleton during human walking. In Proceedings of the 2015 IEEE International Conference on Robotics and Automation (ICRA), Seattle, WA, USA, 26–30 May 2015; pp. 5584–5589. [Google Scholar]
- Koopman, B.; van Asseldonk, E.; van der Kooij, H. Speed-dependent reference joint trajectory generation for robotic gait support. J. Biomech. 2014, 47, 1447–1458. [Google Scholar] [CrossRef]
- Bogert, A.J.V.D.; Geijtenbeek, T.; Even-Zohar, O.; Steenbrink, F.; Hardin, E.C. A real-time system for biomechanical analysis of human movement and muscle function. Med. Biol. Eng. Comput. 2013, 51, 1069–1077. [Google Scholar] [CrossRef] [Green Version]
- Bovi, G.; Rabuffetti, M.; Mazzoleni, P.; Ferrarin, M. A multiple-task gait analysis approach: Kinematic, kinetic and EMG reference data for healthy young and adult subjects. Gait Posture 2011, 33, 6–13. [Google Scholar] [CrossRef] [PubMed]
- Lencioni, T.; Carpinella, I.; Rabuffetti, M.; Marzegan, A.; Ferrarin, M. Human kinematic, kinetic and EMG data during different walking and stair ascending and descending tasks. Sci. Data 2019, 6, 309. [Google Scholar] [CrossRef] [Green Version]
- Moore, J.K.; Hnat, S.K.; Bogert, A.J.V.D. An elaborate data set on human gait and the effect of mechanical perturbations. PeerJ 2015, 3, e918. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Branco, M.; Santos-Rocha, R.; Vieira, M.F. Biomechanics of Gait during Pregnancy. Sci. World J. 2014, 2014, 1–5. Available online: http://www.hindawi.com/journals/tswj155/2014/527940/ (accessed on 4 August 2021). [CrossRef] [Green Version]
- Lelas, J.L.; Merriman, G.J.; Riley, P.O.; Kerrigan, D. Predicting peak kinematic and kinetic parameters from gait speed. Gait Posture 2003, 17, 106–112. [Google Scholar] [CrossRef]
- Mundt, M.; Thomsen, W.; Witter, T.; Koeppe, A.; David, S.; Bamer, F.; Potthast, W.; Markert, B. Prediction of lower limb joint angles and moments during gait using artificial neural networks. Med. Biol. Eng. Comput. 2019, 58, 211–225. [Google Scholar] [CrossRef]
- Schwartz, M.H.; Rozumalski, A.; Trost, J. The effect of walking speed on the gait of typically developing children. J. Biomech. 2008, 41, 1639–1650. [Google Scholar] [CrossRef] [PubMed]
- Silva, F.R.; Muniz, A.M.D.S.; Cerqueira, L.S.; Nadal, J. Biomechanical alterations of gait on overweight subjects. Res. Biomed. Eng. 2018, 34, 291–298. [Google Scholar] [CrossRef]
- Stoquart, G.; Detrembleur, C.; Lejeune, T. Effect of speed on kinematic, kinetic, electromyographic and energetic reference values during treadmill walking. Neurophysiol. Clin. Neurophysiol. 2008, 38, 105–116. [Google Scholar] [CrossRef]
- Beaman, C.; Peterson, C.; Neptune, R.; Kautz, S. Differences in self-selected and fastest-comfortable walking in post-stroke hemiparetic persons. Gait Posture 2010, 31, 311–316. [Google Scholar] [CrossRef] [Green Version]
- Smith, A.J.J.; Lemaire, E.D.; Nantel, J. Lower limb sagittal kinematic and kinetic modeling of very slow walking for gait trajectory scaling. PLoS ONE 2018, 13, e0203934. [Google Scholar] [CrossRef] [Green Version]
- Chandrapal, M.; Chen, X.; Wang, W.; Stanke, B.; Le Pape, N. Investigating improvements to neural network based EMG to joint torque estimation. Paladyn J. Behav. Robot. 2011, 2, 185–192. [Google Scholar] [CrossRef]
- Hahn, M.E. Feasibility of estimating isokinetic knee torque using a neural network model. J. Biomech. 2007, 40, 1107–1114. [Google Scholar] [CrossRef]
- Geyer, H.; Herr, H.M. A Muscle-Reflex Model That Encodes Principles of Legged Mechanics Produces Human Walking Dynamics and Muscle Activities. IEEE Trans. Neural Syst. Rehabil. Eng. 2010, 18, 263–273. [Google Scholar] [CrossRef] [PubMed]
- Caldas, R.; Fadel, T.; Buarque, F.; Markert, B. Adaptive predictive systems applied to gait analysis: A systematic review. Gait Posture 2020, 77, 75–82. [Google Scholar] [CrossRef]
- Goodfellow, I.; Bengio, Y.; Courville, A. Deep Learning; MIT Press: Cambridge, MA, USA, 2016. [Google Scholar]
- Fawaz, H.I.; Forestier, G.; Weber, J.; Idoumghar, L.; Muller, P.-A. Deep learning for time series classification: A review. Data Min. Knowl. Discov. 2019, 33, 917–963. [Google Scholar] [CrossRef] [Green Version]
- Skansi, S. Introduction to Deep Learning: From Logical Calculus to Artificial Intelligence; Springer: Berlin/Heidelberg, Germany, 2018; Volume 114. [Google Scholar]
- Zaroug, A.; Lai, D.T.H.; Mudie, K.; Begg, R. Lower Limb Kinematics Trajectory Prediction Using Long Short-Term Memory Neural Networks. Front. Bioeng. Biotechnol. 2020, 8, 362. [Google Scholar] [CrossRef]
- Moreira, L.; Cerqueira, S.; Figueiredo, J.; Vilas-Boas, J.; Santos, C. AI-based Reference Ankle Joint Torque Trajectory Generation for Robotic Gait Assistance: First Steps. In Proceedings of the 2020 IEEE International Conference on Autonomous Robot Systems and Competitions (ICARSC), Ponta Delgada, Portugal, 15–17 April 2020; pp. 22–27. [Google Scholar]
- Balaban, B.; Tok, F. Gait Disturbances in Patients with Stroke. PM&R 2014, 6, 635–642. [Google Scholar] [CrossRef]
- Parri, A.; Yuan, K.; Marconi, D.; Yan, T.; Crea, S.; Munih, M.; Lova, R.M.; Vitiello, N.; Wang, Q. Real-Time Hybrid Locomotion Mode Recognition for Lower Limb Wearable Robots. IEEE/ASME Trans. Mechatron. 2017, 22, 2480–2491. [Google Scholar] [CrossRef]
- Kim, H.; Shin, Y.J.; Kim, J. Kinematic-based locomotion mode recognition for power augmentation exoskeleton. Int. J. Adv. Robot. Syst. 2017, 14, 1729881417730321. [Google Scholar] [CrossRef]
- Zhu, L.; Wang, Z.; Ning, Z.; Zhang, Y.; Liu, Y.; Cao, W.; Wu, X.; Chen, C. A Novel Motion Intention Recognition Approach for Soft Exoskeleton via IMU. Electronics 2020, 9, 2176. [Google Scholar] [CrossRef]
- Gong, C.; Xu, D.; Zhou, Z.; Vitiello, N.; Wang, Q. Real-Time On-Board Recognition of Locomotion Modes for an Active Pelvis Orthosis. In Proceedings of the 2018 IEEE-RAS 18th International Conference on Humanoid Robots (Humanoids), Beijing, China, 6–9 November 2018; pp. 346–350. [Google Scholar]
- Kim, D.-H.; Cho, C.-Y.; Ryu, J. Real-Time Locomotion Mode Recognition Employing Correlation Feature Analysis Using EMG Pattern. ETRI J. 2014, 36, 99–105. [Google Scholar] [CrossRef]
- Kerrigan, D.C.; Todd, M.K.; Della Croce, U. Gender differences in joint biomechanics during walking Normative Study in Young Adults. Am. J. Phys. Med. Rehabil. 1998, 77, 2–7. [Google Scholar] [CrossRef]
- Perkins, J.M.; Subramanian, S.; Smith, G.D.; Özaltin, E. Adult height, nutrition, and population health. Nutr. Rev. 2016, 74, 149–165. [Google Scholar] [CrossRef] [Green Version]
- Hermens, H.J.; Freriks, B.; Disselhorst-Klug, C.; Rau, G. Development of recommendations for SEMG sensors and sensor placement procedures. J. Electromyogr. Kinesiol. 2000, 10, 361–374. [Google Scholar] [CrossRef]
- Moreira, L.; Figueiredo, J.; Fonseca, P.; Vilas-Boas, J.P.; Santos, C.P. Lower limb kinematic, kinetic, and EMG data from young healthy humans during walking at controlled speeds. Sci. Data 2021, 8, 103. [Google Scholar] [CrossRef] [PubMed]
- Farfán, F.D.; Politti, J.C.; Felice, C.J. Evaluation of EMG processing techniques using Information Theory. Biomed. Eng. Online 2010, 9, 72. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rabuffetti, M.; Marzegan, A.; Crippa, A.; Carpinella, I.; Lencioni, T.; Castagna, A.; Ferrarin, M. The LAMB gait analysis protocol: Definition and experimental assessment of operator-related variability. Proc. Inst. Mech. Eng. Part H J. Eng. Med. 2019, 233, 342–353. [Google Scholar] [CrossRef] [PubMed]
- Perry, J. Gait Analysis: Normal and Pathological Function; SLACK Incorporated: Thorofare, NJ, USA, 1992. [Google Scholar]
- Su, B.; Gutierrez-Farewik, E.M. Gait Trajectory and Gait Phase Prediction Based on an LSTM Network. Sensors 2020, 20, 7127. [Google Scholar] [CrossRef] [PubMed]
- Liu, G.; Zhang, L.; Han, B.; Zhang, T.; Wang, Z.; Wei, P. sEMG-Based Continuous Estimation of Knee Joint Angle Using Deep Learning with Convolutional Neural Network. In Proceedings of the 2019 IEEE 15th International Conference on Automation Science and Engineering (CASE), Vancouver, BC, Canada, 22–26 August 2019; Volume 2019, pp. 140–145. [Google Scholar]
- Breslow, N. Lessons in biostatistics. Past Present Future Stat. Sci. 2014, 25, 335–347. [Google Scholar]
- Silva, L.L.M.E.; De Moura, C.E.M.; De Godoy, J.R.P. A marcha no paciente hemiparético. Universitas: Ciências da Saúde 2005, 3, 261–273. [Google Scholar] [CrossRef]
- Hanlon, M.; Anderson, R. Prediction methods to account for the effect of gait speed on lower limb angular kinematics. Gait Posture 2006, 24, 280–287. [Google Scholar] [CrossRef] [PubMed]
- De Luca, C.J.; Gilmore, L.D.; Kuznetsov, M.; Roy, S.H. Filtering the surface EMG signal: Movement artifact and baseline noise contamination. J. Biomech. 2010, 43, 1573–1579. [Google Scholar] [CrossRef] [PubMed]






| ID | Gender | Body Height (m) | Body Mass (kg) | Age (Years) | Foot Length (m) | Shank Length (m) |
|---|---|---|---|---|---|---|
| 1 | Male | 1.81 | 66.2 | 25 | 0.28 | 0.42 |
| 2 | Female | 1.56 | 54.4 | 23 | 0.24 | 0.38 |
| 3 | Female | 1.57 | 53.5 | 26 | 0.24 | 0.39 |
| 4 | Male | 1.79 | 74.4 | 24 | 0.27 | 0.44 |
| 5 | Female | 1.65 | 60.0 | 21 | 0.24 | 0.39 |
| 6 | Female | 1.54 | 58.4 | 21 | 0.21 | 0.35 |
| 7 | Male | 1.72 | 75.8 | 23 | 0.27 | 0.41 |
| 8 | Male | 1.80 | 83.7 | 26 | 0.27 | 0.44 |
| 9 | Male | 1.82 | 76.8 | 25 | 0.26 | 0.42 |
| 10 | Female | 1.51 | 52.0 | 23 | 0.25 | 0.40 |
| 11 | Male | 1.83 | 73.4 | 25 | 0.23 | 0.46 |
| 12 | Female | 1.61 | 53.5 | 27 | 0.21 | 0.32 |
| 13 | Female | 1.60 | 65.3 | 26 | 0.26 | 0.34 |
| Mean | 1.68 | 65.2 | 24.2 | 0.25 | 0.40 | |
| Standard Deviation | 0.12 | 10.3 | 1.85 | 0.02 | 0.04 | |
| DL Model | Hyperparameters | NRMSE | SC | R2 | Prediction Time (ms/Sample) | ||||
|---|---|---|---|---|---|---|---|---|---|
| LOSOCV | Test | LOSOCV | Test | LOSOCV | Test | ||||
| LSTM | Number of neurons | 100 | 0.58 ± 0.20 | 0.71 | 0.84 ± 0.08 | 0.92 | 0.79 ± 0.22 | 0.92 | 3.7 |
| LSTM layers | 1 | ||||||||
| Normalization method | z-score | ||||||||
| Batch size | 20 | ||||||||
| Dropout (%) | 50 | ||||||||
| CNN | Kernel size | 2 × 2 | 0.70 ± 0.06 | 0.76 | 0.89 ± 0.03 | 0.92 | 0.91 ± 0.03 | 0.94 | 0.51 |
| Number of layers (number of filters) | 2 (8–16) | ||||||||
| Normalization method | Robust | ||||||||
| Batch size | 20 | ||||||||
| Dropout (%) | 25 | ||||||||
| DL Model | Hyperparameters | NRMSE | SC | R2 | Prediction Time (ms/Sample) | ||||
|---|---|---|---|---|---|---|---|---|---|
| LOSOCV | Test | LOSOCV | Test | LOSOCV | Test | ||||
| LSTM | Number of neurons | 100 | 0.59 ± 0.15 | 0.48 | 0.88 ± 0.05 | 0.78 | 0.81 ± 0.13 | 0.73 | 4.80 |
| LSTM layers | 1 | ||||||||
| Normalization method | z-score | ||||||||
| Batch size | 20 | ||||||||
| Dropout (%) | 50 | ||||||||
| CNN | Kernel size | 2 × 2 | 0.73 ± 0.08 | 0.72 | 0.90 ± 0.04 | 0.89 | 0.92 ± 0.04 | 0.92 | 0.78 |
| Number of layers (number of filters) | 2 (8–16) | ||||||||
| Normalization method | Robust | ||||||||
| Batch size | 20 | ||||||||
| Dropout (%) | 25 | ||||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Moreira, L.; Figueiredo, J.; Vilas-Boas, J.P.; Santos, C.P. Kinematics, Speed, and Anthropometry-Based Ankle Joint Torque Estimation: A Deep Learning Regression Approach. Machines 2021, 9, 154. https://doi.org/10.3390/machines9080154
Moreira L, Figueiredo J, Vilas-Boas JP, Santos CP. Kinematics, Speed, and Anthropometry-Based Ankle Joint Torque Estimation: A Deep Learning Regression Approach. Machines. 2021; 9(8):154. https://doi.org/10.3390/machines9080154
Chicago/Turabian StyleMoreira, Luís, Joana Figueiredo, João Paulo Vilas-Boas, and Cristina Peixoto Santos. 2021. "Kinematics, Speed, and Anthropometry-Based Ankle Joint Torque Estimation: A Deep Learning Regression Approach" Machines 9, no. 8: 154. https://doi.org/10.3390/machines9080154
APA StyleMoreira, L., Figueiredo, J., Vilas-Boas, J. P., & Santos, C. P. (2021). Kinematics, Speed, and Anthropometry-Based Ankle Joint Torque Estimation: A Deep Learning Regression Approach. Machines, 9(8), 154. https://doi.org/10.3390/machines9080154