Prognostic Value of Admission Chest CT Findings for Invasive Ventilation Therapy in COVID-19 Pneumonia

 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Collection
2.2. Image Acquisition
2.3. Image Interpretation
2.4. Statistical Analysis
3. Results
3.1. Clinical Characteristics and Demographic Data
3.2. Imaging Findings within our Study Cohort
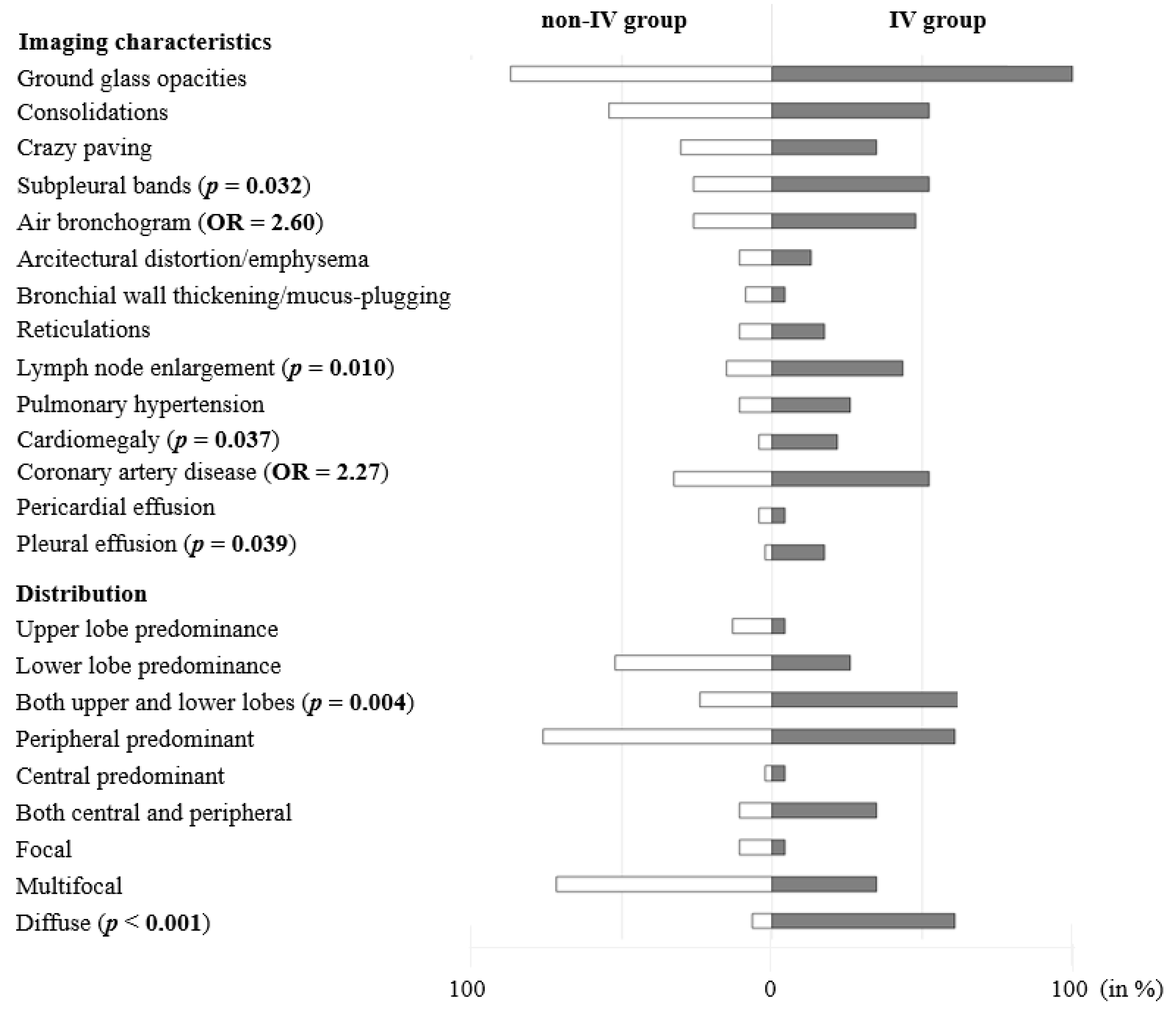
3.3. Group-related Differences in Imaging Characteristics
3.4. Group-Related Differences in Distribution Patterns
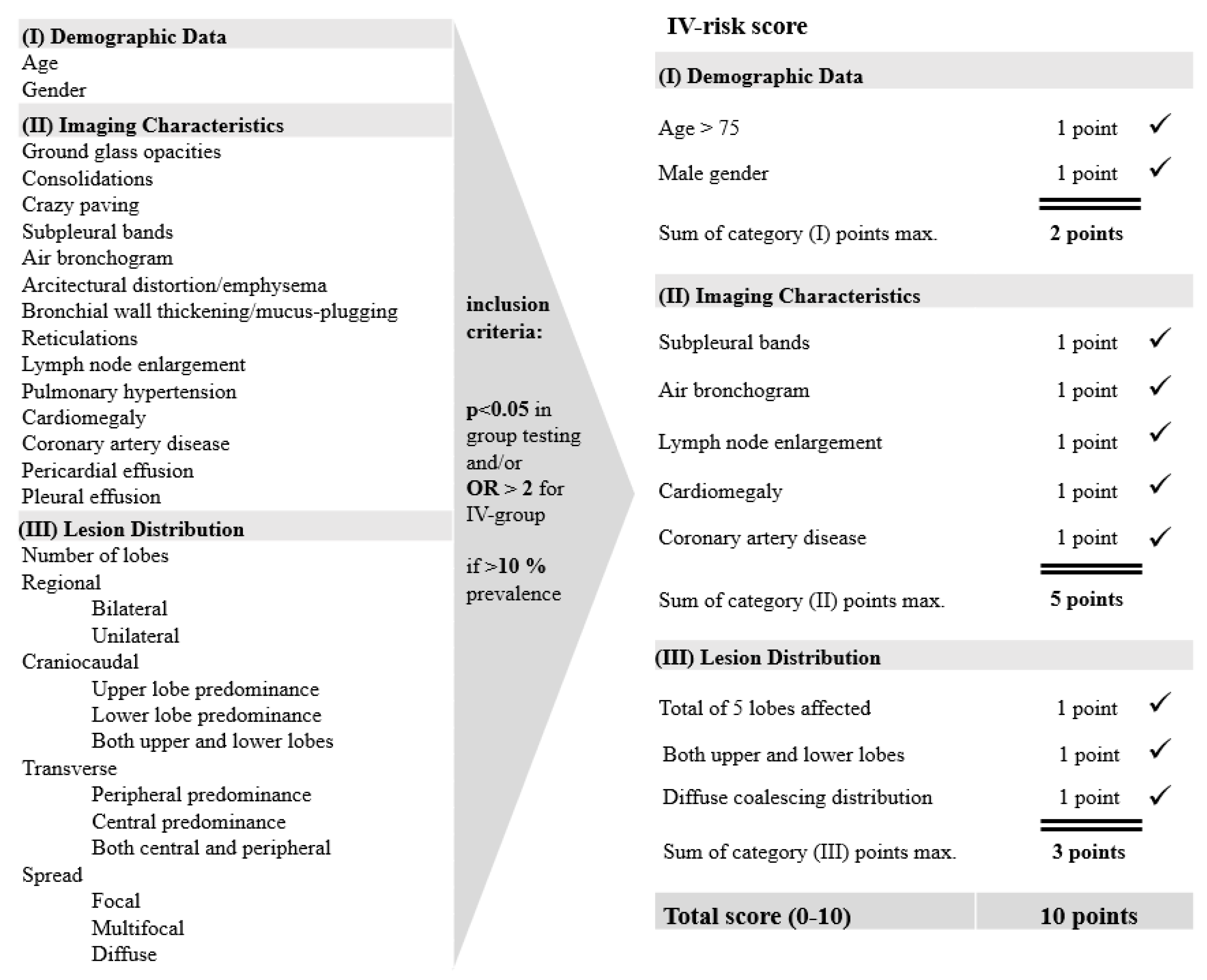
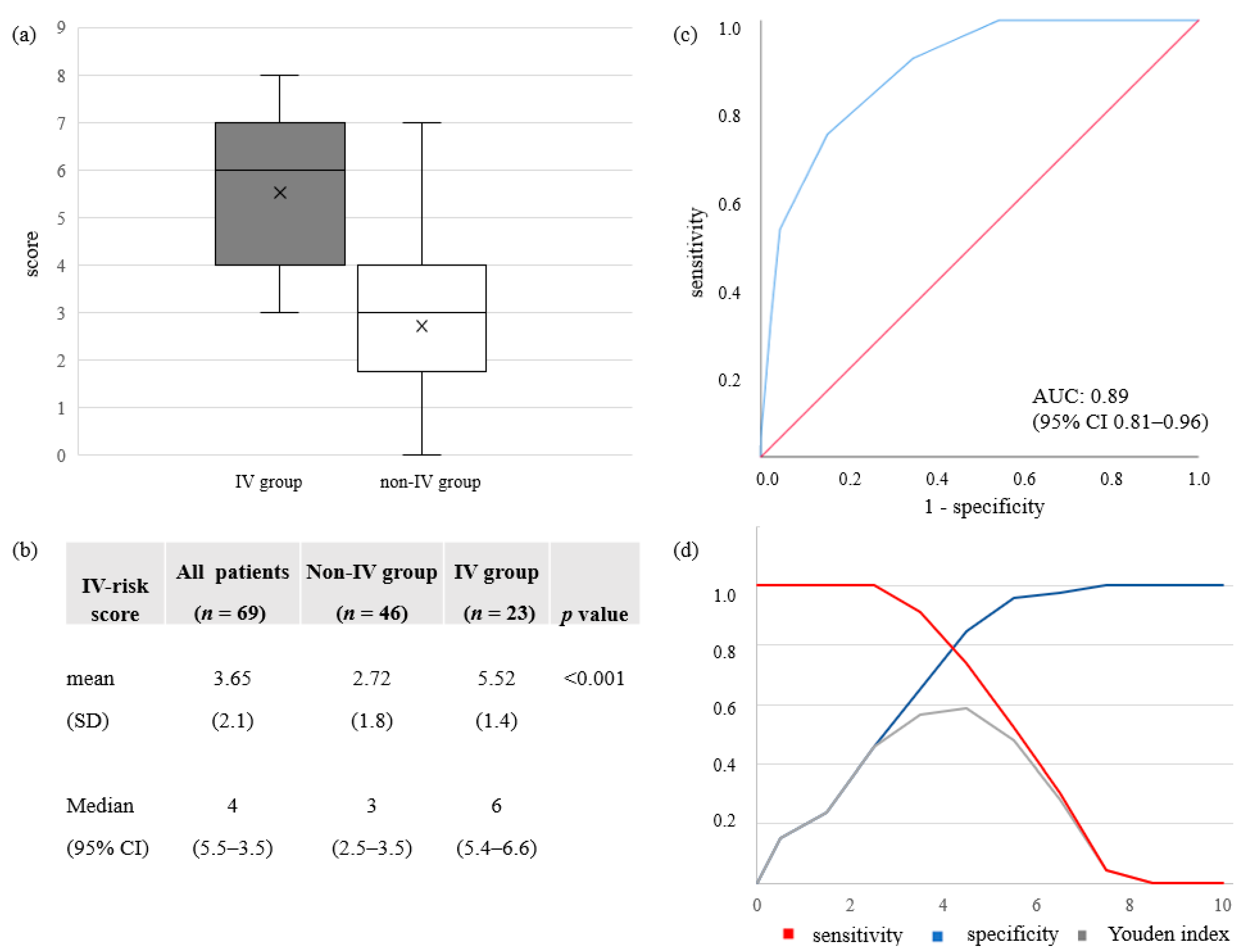
3.5. IV-Risk Score for Invasive Ventilation Therapy
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- WHO. The World Health Report 2004: Changing History; World Health Organisation: Geneva, Switzerland, 2004. [Google Scholar]
- Boccia, S.; Ricciardi, W.; Ioannidis, J.P.A. What other countries can learn from italy during the covid-19 pandemic. Jama Intern. Med. 2020, 180, 927–928. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Johns Hopkins University: Coronavirus Covid-19 Global Cases by the Center for Systems Science and Engineering (Csse). 2020. Available online: https://gisanddata.maps.arcgis.com/apps/opsdashboard/index.html#/bda7594740fd40299423467b48e9ecf6 (accessed on 10 December 2020).
- Wise, J. Covid-19: Risk of second wave is very real, say researchers. BMJ 2020, 369, m2294. [Google Scholar] [CrossRef] [PubMed]
- Armstrong, R.A.; Kane, A.D.; Cook, T.M. Outcomes from intensive care in patients with covid-19: A systematic review and meta-analysis of observational studies. Anaesthesia 2020, 75, 1340–1349. [Google Scholar] [CrossRef] [PubMed]
- Karagiannidis, C.; Mostert, C.; Hentschker, C.; Voshaar, T.; Malzahn, J.; Schillinger, G.; Klauber, J.; Janssens, U.; Marx, G.; Weber-Carstens, S.; et al. Case characteristics, resource use, and outcomes of 10 021 patients with covid-19 admitted to 920 german hospitals: An observational study. Lancet. Respir. Med. 2020, 8, 853–862. [Google Scholar] [CrossRef]
- Abate, S.M.; Ahmed Ali, S.; Mantfardo, B.; Basu, B. Rate of intensive care unit admission and outcomes among patients with coronavirus: A systematic review and meta-analysis. PLoS ONE 2020, 15, e0235653. [Google Scholar] [CrossRef]
- Rothe, C.; Schunk, M.; Sothmann, P.; Bretzel, G.; Froeschl, G.; Wallrauch, C.; Zimmer, T.; Thiel, V.; Janke, C.; Guggemos, W.; et al. Transmission of 2019-ncov infection from an asymptomatic contact in germany. N. Engl. J. Med. 2020, 382, 970–971. [Google Scholar] [CrossRef] [Green Version]
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in wuhan, china. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef] [Green Version]
- Li, Y.; Yao, L.; Li, J.; Chen, L.; Song, Y.; Cai, Z.; Yang, C. Stability issues of rt-pcr testing of sars-cov-2 for hospitalized patients clinically diagnosed with covid-19. J. Med Virol. 2020, 92, 903–908. [Google Scholar] [CrossRef] [Green Version]
- Huang, P.; Liu, T.; Huang, L.; Liu, H.; Lei, M.; Xu, W.; Hu, X.; Chen, J.; Liu, B. Use of chest ct in combination with negative rt-pcr assay for the 2019 novel coronavirus but high clinical suspicion. Radiology 2020, 295, 22–23. [Google Scholar] [CrossRef]
- Xie, X.; Zhong, Z.; Zhao, W.; Zheng, C.; Wang, F.; Liu, J. Chest ct for typical 2019-ncov pneumonia: Relationship to negative rt-pcr testing. Radiology 2020, 296, 200343. [Google Scholar] [CrossRef] [Green Version]
- Fang, Y.; Zhang, H.; Xie, J.; Lin, M.; Ying, L.; Pang, P.; Ji, W. Sensitivity of chest ct for covid-19: Comparison to rt-pcr. Radiology 2020, 296, 200432. [Google Scholar]
- Ai, T.; Yang, Z.; Hou, H.; Zhan, C.; Chen, C.; Lv, W.; Tao, Q.; Sun, Z.; Xia, L. Correlation of chest ct and rt-pcr testing in coronavirus disease 2019 (covid-19) in china: A report of 1014 cases. Radiology 2020, 296, 200642. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kovacs, A.; Palasti, P.; Vereb, D.; Bozsik, B.; Palko, A.; Kincses, Z.T. The sensitivity and specificity of chest ct in the diagnosis of covid-19. Eur. Radiol. 2020. [Google Scholar] [CrossRef] [PubMed]
- Rubin, G.D.; Ryerson, C.J.; Haramati, L.B.; Sverzellati, N.; Kanne, J.P.; Raoof, S.; Schluger, N.W.; Volpi, A.; Yim, J.J.; Martin, I.B.K.; et al. The role of chest imaging in patient management during the covid-19 pandemic: A multinational consensus statement from the fleischner society. Chest 2020, 296, 172–180. [Google Scholar] [CrossRef] [Green Version]
- Kim, J.Y.; Choe, P.G.; Oh, Y.; Oh, K.J.; Kim, J.; Park, S.J.; Park, J.H.; Na, H.K.; Oh, M.D. The first case of 2019 novel coronavirus pneumonia imported into korea from wuhan, china: Implication for infection prevention and control measures. J. Korean Med Sci. 2020, 35, e61. [Google Scholar] [CrossRef] [PubMed]
- Salehi, S.; Abedi, A.; Balakrishnan, S.; Gholamrezanezhad, A. Coronavirus disease 2019 (covid-19): A systematic review of imaging findings in 919 patients. Ajr. Am. J. Roentgenol. 2020, 215, 87–93. [Google Scholar] [CrossRef] [PubMed]
- Hani, C.; Trieu, N.H.; Saab, I.; Dangeard, S.; Bennani, S.; Chassagnon, G.; Revel, M.P. Covid-19 pneumonia: A review of typical ct findings and differential diagnosis. Diagn. Interv. Imaging 2020, 101, 263–268. [Google Scholar] [CrossRef]
- Zhou, Z.; Guo, D.; Li, C.; Fang, Z.; Chen, L.; Yang, R.; Li, X.; Zeng, W. Coronavirus disease 2019: Initial chest ct findings. Eur. Radiol. 2020, 30, 4398–4406. [Google Scholar] [CrossRef] [Green Version]
- Caruso, D.; Zerunian, M.; Polici, M.; Pucciarelli, F.; Polidori, T.; Rucci, C.; Guido, G.; Bracci, B.; de Dominicis, C.; Laghi, A. Chest ct features of covid-19 in rome, italy. Radiology 2020, 296, E79–E85. [Google Scholar] [CrossRef]
- Huang, G.; Gong, T.; Wang, G.; Wang, J.; Guo, X.; Cai, E.; Li, S.; Li, X.; Yu, Y.; Lin, L. Timely diagnosis and treatment shortens the time to resolution of coronavirus disease (covid-19) pneumonia and lowers the highest and last ct scores from sequential chest ct. Ajr. Am. J. Roentgenol. 2020, 215, 367–373. [Google Scholar] [CrossRef]
- Wang, Y.; Dong, C.; Hu, Y.; Li, C.; Ren, Q.; Zhang, X.; Shi, H.; Zhou, M. Temporal changes of ct findings in 90 patients with covid-19 pneumonia: A longitudinal study. Radiology 2020, 296, E55–E64. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ye, Z.; Zhang, Y.; Wang, Y.; Huang, Z.; Song, B. Chest ct manifestations of new coronavirus disease 2019 (covid-19): A pictorial review. Eur. Radiol. 2020, 30, 4381–4389. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pan, F.; Ye, T.; Sun, P.; Gui, S.; Liang, B.; Li, L.; Zheng, D.; Wang, J.; Hesketh, R.L.; Yang, L.; et al. Time course of lung changes on chest ct during recovery from 2019 novel coronavirus (covid-19) pneumonia. Radiology 2020, 200370. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhao, W.; Zhong, Z.; Xie, X.; Yu, Q.; Liu, J. Relation between chest ct findings and clinical conditions of coronavirus disease (covid-19) pneumonia: A multicenter study. Am. J. Roentgenol. 2020, 214, 1072–1077. [Google Scholar] [CrossRef] [PubMed]
- Li, K.; Wu, J.; Wu, F.; Guo, D.; Chen, L.; Fang, Z.; Li, C. The clinical and chest ct features associated with severe and critical covid-19 pneumonia. Investig. Radiol. 2020, 55, 327–331. [Google Scholar] [CrossRef]
- Wu, J.; Wu, X.; Zeng, W.; Guo, D.; Fang, Z.; Chen, L.; Huang, H.; Li, C. Chest ct findings in patients with coronavirus disease 2019 and its relationship with clinical features. Investig. Radiol. 2020, 55, 257–261. [Google Scholar] [CrossRef]
- Yuan, M.; Yin, W.; Tao, Z.; Tan, W.; Hu, Y. Association of radiologic findings with mortality of patients infected with 2019 novel coronavirus in wuhan, china. PLoS ONE 2020, 15, e0230548. [Google Scholar] [CrossRef] [Green Version]
- Li, K.; Fang, Y.; Li, W.; Pan, C.; Qin, P.; Zhong, Y.; Liu, X.; Huang, M.; Liao, Y.; Li, S. Ct image visual quantitative evaluation and clinical classification of coronavirus disease (covid-19). Eur. Radiol. 2020, 30, 4407–4416. [Google Scholar] [CrossRef] [Green Version]
- Robin, X.; Turck, N.; Hainard, A.; Tiberti, N.; Lisacek, F.; Sanchez, J.C.; Muller, M. Proc: An open-source package for r and s+ to analyze and compare roc curves. BMC Bioinform. 2011, 12, 77. [Google Scholar] [CrossRef]
- DeLong, E.R.; DeLong, D.M.; Clarke-Pearson, D.L. Comparing the areas under two or more correlated receiver operating characteristic curves: A nonparametric approach. Biometrics 1988, 44, 837–845. [Google Scholar]
- Kligerman, S.J.; Franks, T.J.; Galvin, J.R. From the radiologic pathology archives: Organization and fibrosis as a response to lung injury in diffuse alveolar damage, organizing pneumonia, and acute fibrinous and organizing pneumonia. Radiographics 2013, 33, 1951–1975. [Google Scholar] [CrossRef] [PubMed]
- Weidmann, M.D.; Ofori, K.; Rai, A.J. Laboratory biomarkers in the management of patients with covid-19. Am. J. Clin. Pathol. 2020. [Google Scholar] [CrossRef] [PubMed]
- Sung, J.; Choudry, N.; Bachour, R. Development and validation of a simple risk score for diagnosing covid-19 in the emergency room. Epidemiol. Infect. 2020, 148, e273. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Xu, S.; Yu, M.; Wang, K.; Tao, Y.; Zhou, Y.; Shi, J.; Zhou, M.; Wu, B.; Yang, Z.; et al. Risk factors for severity and mortality in adult covid-19 inpatients in wuhan. J. Allergy Clin. Immunol. 2020, 146, 110–118. [Google Scholar] [CrossRef] [PubMed]
- Alhazzani, W.; Moller, M.H.; Arabi, Y.M.; Loeb, M.; Gong, M.N.; Fan, E.; Oczkowski, S.; Levy, M.M.; Derde, L.; Dzierba, A.; et al. Surviving sepsis campaign: Guidelines on the management of critically ill adults with coronavirus disease 2019 (covid-19). Crit. Care Med. 2020, 46, 854–887. [Google Scholar]
- Kluge, S.; Janssens, U.; Welte, T.; Weber-Carstens, S.; Marx, G.; Karagiannidis, C. German recommendations for critically ill patients with covid19. Med. Klin. Intensivmed. Und Notf. 2020, 1–4. [Google Scholar] [CrossRef] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Data are n (%) if Not Indicated Differently | All Patients (n = 69) | Non-IV-Group (n = 46) | IV-Group (n = 23) | p-Values |
|---|---|---|---|---|
| Clinical and demographic data | ||||
| Age in years; median (95% CI)/ mean (SD) | 62 (58.4–65.6)/ 61.0 (15.3) | 61 (56.6–65.4)/ 61.5 (15.2) | 64 (57.5–70.5)/ 60.2 (15.8) | 0.944 |
| Sex: | <0.001 | |||
| Male | 47 (68.0) | 25 (54.0) | 22 (96.0) | |
| Female | 22 (32.0) | 21 (46.0) | 1 (4.0) | |
| Underlying disease: | 57 (82.6) | 36 (78.3) | 21 (91.3) | 0.985 |
| Cardiovascular | 40 (70.2) | 23 (63.9) | 17 (81.0) | |
| Respiratory | 13 (22.8) | 7 (19.4) | 6 (28.6) | |
| Immunologic/endocrinologic | 14 (24.6) | 8 (22.2) | 6 (28.6) | |
| Obesity (BMI > 30) | 8 (14.0) | 5 (13.9) | 3 (14.3) | |
| No disease known: | 12 (17.4) | 10 (21.7) | 2 (8.7) | 0.178 |
| Laboratory data on admission in mean (SD) | ||||
| CRP (mg/dL) | 7.6 (8.2) | 5.5 (6.1) | 11.9 (9.9) | 0.004 |
| Procalcitonin (ng/mL) | 1.0 (3.5) | 0.2 (0.5) | 2.4 (5.6) | 0.032 |
| Creatinine (mg/dL) | 1.1 (0.8) | 0.9 (0.5) | 1.5 (1.0) | 0.490 |
| LDH (U/L) | 374.0 (208.5) | 326.2 (209.0) | 469.6 (171.6) | <0.001 |
| Leucocytes (×109/L) | 11.5 (36.5) | 5.8 (2.9) | 22.7 (61.0) | 0.912 |
| Lymphocytes (×109/L) | 1.1 (0.6) | 1.1 (0.7) | 1.0 (0.3) | 0.849 |
| IL-6 (ng/L) | 884.6 (197.8) | 34.1 (31.6) | 482.3 (1351.2) | <0.001 |
| INR | 1.0 (0.1) | 1.0 (0.2) | 1.0 (0.1) | 0.904 |
| aPTT (seconds) | 29.2 (4.6) | 29.3 (4.9) | 28.9 (4.0) | 0.803 |
| D-dimer (mg/L) | 2.1 (4.5) | 1.5 (1.8) | 3.3 (7.1) | 0.280 |
| Symptoms on admission | ||||
| Dry cough | 49 (71.0) | 33 (71.7) | 16 (69.6) | 0.851 |
| Fever | 56 (81.2) | 37 (80.4) | 19 (82.6) | 1 |
| Sore throat/loss of taste | 13 (18.8) | 9 (19.6) | 4 (17.4) | 1 |
| Reduced general condition | 45 (65.2) | 31 (67.4) | 14 (60.9) | 0.592 |
| Limb pain/chills | 13 (18.8) | 8 (17.4) | 5 (21.7) | 0.663 |
| Retrosternal/chest pain | 11 (15.9) | 9 (19.6) | 2 (8.7) | 0.314 |
| Dyspnea | 37 (53.6) | 22 (47.8) | 15 (65.2) | 0.172 |
| Diarrhea/nausea/vomiting | 24 (34.8) | 17 (37.0) | 7 (30.4) | 0.592 |
| Dizziness/syncope/headache | 10 (14.5) | 6 (13.0) | 4 (17.4) | 0.721 |
| Symptoms onset | ||||
| Week of symptoms; mean (SD) | 1.9 (0.75) | 1.7 (0.73) | 2.4 (0.75) | 0.010 |
| Outcome parameters | ||||
| Length of hospital stay (days) | 21.0 (32.4) | 9.7 (7.6) | 43.6 (47.7) | <0.001 |
| In-hospital mortality | 7 (10.1) | 2 (4.3) | 5 (21.7) | 0.039 |
| Time from admission to intubation (days) | - | - | 2.9 (3.1) |
| CT Features Data are n (%) if Not Indicated Differently | All Patients (n = 69) | No/Non-Invasive Ventilation Group (n = 46) | Invasive Ventilation Group (n = 23) | p-Values | Odds Ratios (OR) |
|---|---|---|---|---|---|
| Native high-resolution (HR-CT) protocol | 53 (76.8) | 39 (84.8) | 14 (60.9) | ||
| Contrast-enhanced (CE) pulmonary embolism protocol: | 16 (23.2) | 7 (15.2) | 9 (39.1) | ||
| Pulmonary embolism present | 3 (18.6) | 2 (28.6) | 1 (11.1) | 0.550 | |
| Imaging findings | |||||
| Ground glass opacities (GGOs) | 63 (91.3) | 40 (87.0) | 23 (100.0) | 0.168 | -* |
| Consolidations | 37 (53.6) | 25 (54.3) | 12 (52.2) | 0.864 | 0.91 |
| Crazy paving | 22 (31.9) | 14 (30.4) | 8 (34.8) | 0.715 | 1.11 |
| Subpleural bands | 24 (34.8) | 12 (26.1) | 12 (52.2) | 0.032 | 3.09 |
| Air bronchogram | 32 (46.4) | 20 (43.5) | 12 (52.2) | 0.495 | 2.60 |
| Architectural distortion/emphysema | 16 (23.2) | 13 (28.3) | 3 (13.0) | 0.158 | 1.24 |
| Bronchial wall thickening/mucus-plugging | 5 (7.2) | 4 (8.7) | 1 (4.3) | 0.511 | 0.48 |
| Reticulations | 9 (13.0) | 5 (10.9) | 4 (17.4) | 0.448 | 1.73 |
| Lymph node enlargement | 8 (11.6) | 7 (15.2) | 10 (43.5) | 0.010 | 4.30 |
| Pulmonary hypertension | 11 (15.9) | 5 (10.9) | 6 (26.1) | 0.104 | 1.59 |
| Cardiomegaly | 7 (10.1) | 2 (4.3) | 5 (21.7) | 0.037 | 6.92 |
| Coronary artery disease | 27 (39.1) | 15 (32.6) | 12 (52.2) | 0.116 | 2.27 |
| Pericardial effusion | 3 (4.3) | 2 (4.3) | 1 (4.3) | 1.000 | 1.0 |
| Pleural effusion | 5 (7.2) | 1 (2.2) | 4 (17.4) | 0.039 | 9.55 |
| Distribution | |||||
| Number of lobes; mean (SD) | 4.04 (1.7) | 3.5 (1.9) | 4.9 (0.6) | 0.008 | |
| Regional distribution: | |||||
| Bilateral | 56 (81.2) | 34 (74.0) | 22 (95.7) | 0.241 | |
| Unilateral | 8 (11.6) | 7 (15.2) | 1 (4.3) | ||
| Craniocaudal distribution: | |||||
| Upper lobe predominance | 7 (10.1) | 6 (13.0) | 1 (4.3) | 0.004 | |
| Lower lobe predominance | 30 (43.5) | 24 (52.2) | 6 (26.1) | ||
| Both upper and lower lobes | 27 (39.1) | 11 (24.0) | 16 (69.6) | ||
| Transverse distribution: | |||||
| Peripheral predominance | 49 (71.0) | 35 (76.1) | 14 (60.9) | 0.055 | |
| Central predominance | 2 (2.9) | 1 (2.2) | 1 (4.3) | ||
| Both central and peripheral | 13 (18.8) | 5 (10.9) | 8 (34.8) | ||
| Spread: | |||||
| Focal | 6 (8.7) | 5 (10.9) | 1 (4.3) | <0.001 | |
| Multifocal | 42 (60.9) | 33 (71.7) | 8 (34.8) | ||
| Diffuse | 17 (24.6) | 3 (6.5) | 14 (60.9) | ||
| No CT findings | 5 (7.2) | 5 (10.9) | 0 (0.0) | ||
| CT lung involvement score (0-20); mean (SD) | 13.01 (6.5) | 10.76 (6.6) | 17.52 (3.0) | <0.001 | |
| CXR present 48 h < or > of CT scan | 31 (44.9) | 11 (23.9) | 20 (87.0) | ||
| Indicative signs for pulmonary involvement | 27 (87.1) | 7 (63.6) | 20 (100.0) | 0.010 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gresser, E.; Rueckel, J.; Puhr-Westerheide, D.; Schwarze, V.; Fink, N.; Kunz, W.G.; Wassilowsky, D.; Irlbeck, M.; Ricke, J.; Ingrisch, M.; et al. Prognostic Value of Admission Chest CT Findings for Invasive Ventilation Therapy in COVID-19 Pneumonia. Diagnostics 2020, 10, 1108. https://doi.org/10.3390/diagnostics10121108
Gresser E, Rueckel J, Puhr-Westerheide D, Schwarze V, Fink N, Kunz WG, Wassilowsky D, Irlbeck M, Ricke J, Ingrisch M, et al. Prognostic Value of Admission Chest CT Findings for Invasive Ventilation Therapy in COVID-19 Pneumonia. Diagnostics. 2020; 10(12):1108. https://doi.org/10.3390/diagnostics10121108
Chicago/Turabian StyleGresser, Eva, Johannes Rueckel, Daniel Puhr-Westerheide, Vincent Schwarze, Nicola Fink, Wolfgang G. Kunz, Dietmar Wassilowsky, Michael Irlbeck, Jens Ricke, Michael Ingrisch, and et al. 2020. "Prognostic Value of Admission Chest CT Findings for Invasive Ventilation Therapy in COVID-19 Pneumonia" Diagnostics 10, no. 12: 1108. https://doi.org/10.3390/diagnostics10121108
APA StyleGresser, E., Rueckel, J., Puhr-Westerheide, D., Schwarze, V., Fink, N., Kunz, W. G., Wassilowsky, D., Irlbeck, M., Ricke, J., Ingrisch, M., & Sabel, B. O. (2020). Prognostic Value of Admission Chest CT Findings for Invasive Ventilation Therapy in COVID-19 Pneumonia. Diagnostics, 10(12), 1108. https://doi.org/10.3390/diagnostics10121108