Right Heart Size and Right Ventricular Reserve in Pulmonary Hypertension: Impact on Management and Prognosis


Abstract
:1. Introduction
2. Materials and Methods
2.1. Literature Search
2.2. Study Selection
3. Results
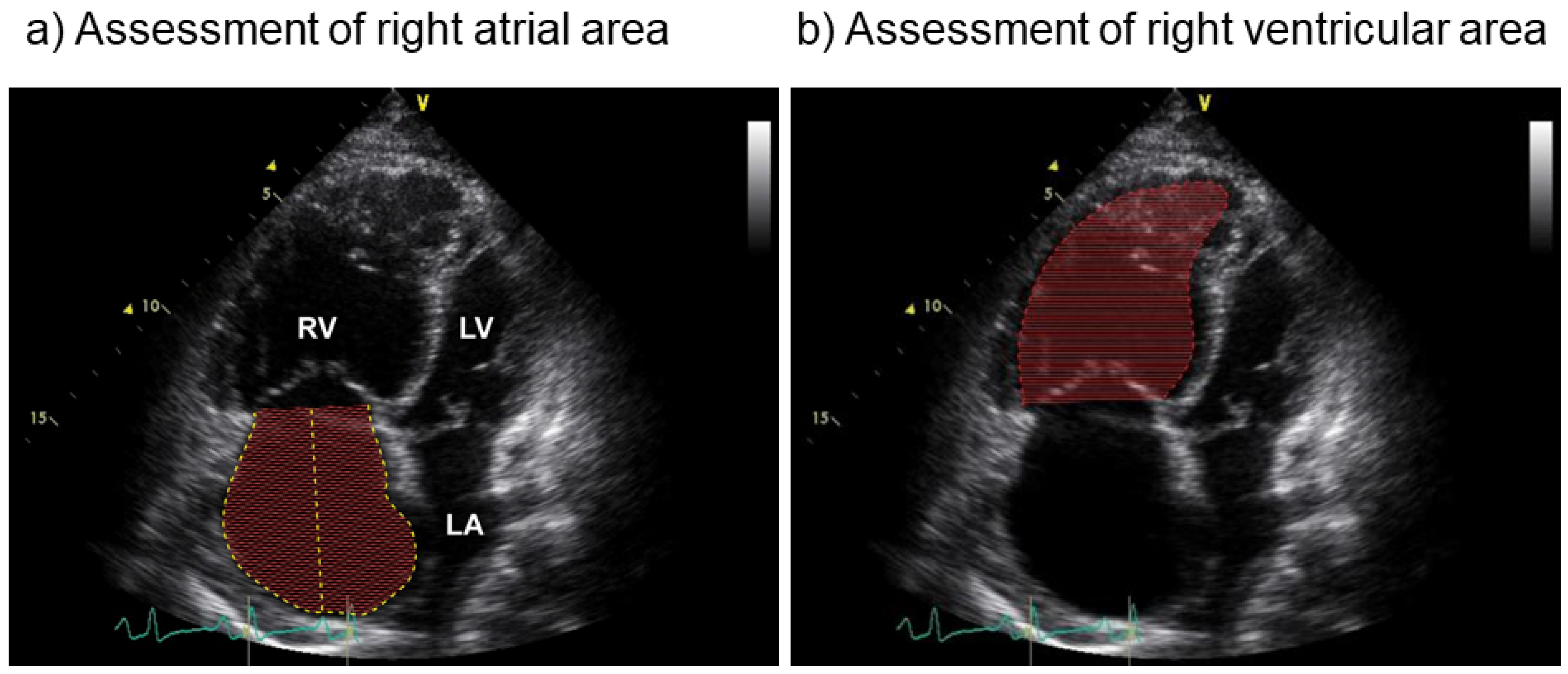
3.1. Definitions of Right Heart Size
3.2. Definitions of Right Ventricular Reserve
3.3. Prognostic Importance of Right Heart Size
3.4. Prognostic Importance of Right Ventricular Reserve
3.5. Treatment Effects on Right Heart Size and Function
4. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- D’Alonzo, G.E.; Barst, R.J.; Ayres, S.M.; Bergofsky, E.H.; Brundage, B.H.; Detre, K.M.; Fishman, A.P.; Goldring, R.M.; Groves, B.M.; Kernis, J.T.; et al. Survival in patients with primary pulmonary hypertension. Ann. Intern. Med. 1991, 115, 343–355. [Google Scholar] [CrossRef] [PubMed]
- Vonk-Noordegraaf, A.; Haddad, F.; Chin, K.M.; Forfia, P.R.; Kawut, S.M.; Lumens, J.; Naeije, R.; Newman, J.; Oudiz, R.J.; Provencher, S.; et al. Right heart adaptation to pulmonary arterial hypertension: Physiology and pathobiology. J. Am. Coll. Cardiol. 2013, 62, D22–D33. [Google Scholar] [CrossRef] [PubMed]
- Haddad, F.; Vrtovec, B.; Ashley, E.A.; Deschamps, A.; Haddad, H.; Denault, A.Y. The concept of ventricular reserve in heart failure and pulmonary hypertension: An old metric that brings us one step closer in our quest for prediction. Curr. Opin. Cardiol. 2011, 26, 123–131. [Google Scholar] [CrossRef] [PubMed]
- Amsallem, M.; Boulate, D.; Aymami, M.; Guihaire, J.; Selej, M.; Huo, J.; Denault, A.Y.; McConnell, M.V.; Schnittger, I.; Fadel, E.; et al. Load Adaptability in Patients With Pulmonary Arterial Hypertension. Am. J. Cardiol. 2017, 120, 874–882. [Google Scholar] [CrossRef] [PubMed]
- Vonk Noordegraaf, A.; Westerhof, B.E.; Westerhof, N. The Relationship between the Right Ventricle and its Load in Pulmonary Hypertension. J. Am. Coll. Cardiol. 2017, 69, 236–243. [Google Scholar] [CrossRef]
- Galiè, N.; Humbert, M.; Vachiery, J.L.; Gibbs, S.; Lang, I.; Torbicki, A.; Simonneau, G.; Peacock, A.; Vonk Noordegraaf, A.; Beghetti, M.; et al. 2015 ESC/ERS Guidelines for the diagnosis and treatment of pulmonary hypertension: The Joint Task Force for the Diagnosis and Treatment of Pulmonary Hypertension of the European Society of Cardiology (ESC) and the European Respiratory Society (ERS): Endorsed by: Association for European Paediatric and Congenital Cardiology (AEPC), International Society for Heart and Lung Transplantation (ISHLT). Eur. Respir. J. 2015, 46, 903–975. [Google Scholar] [CrossRef]
- Cordina, R.L.; Playford, D.; Lang, I.; Celermajer, D.S. State-of-the-Art Review: Echocardiography in Pulmonary Hypertension. Heart Lung Circ. 2019, 28, 1351–1364. [Google Scholar] [CrossRef] [Green Version]
- Grünig, E.; Henn, P.; D’Andrea, A.; Claussen, M.; Ehlken, N.; Maier, F.; Naeije, R.; Nagel, C.; Prange, F.; Weidenhammer, J.; et al. Reference values for and determinants of right atrial area in healthy adults by 2-dimensional echocardiography. Circ. Cardiovasc. Imaging 2013, 6, 117–124. [Google Scholar] [CrossRef] [Green Version]
- Naeije, R.; Manes, A. The right ventricle in pulmonary arterial hypertension. Eur. Respir. Rev. 2014, 23, 476–487. [Google Scholar] [CrossRef] [Green Version]
- Vanderpool, R.R.; Pinsky, M.R.; Naeije, R.; Deible, C.; Kosaraju, V.; Bunner, C.; Mathier, M.A.; Lacomis, J.; Champion, H.C.; Simon, M.A. RV-pulmonary arterial coupling predicts outcome in patients referred for pulmonary hypertension. Heart 2015, 101, 37–43. [Google Scholar] [CrossRef] [Green Version]
- Spruijt, O.A.; de Man, F.S.; Groepenhoff, H.; Oosterveer, F.; Westerhof, N.; Vonk-Noordegraaf, A.; Bogaard, H.J. The effects of exercise on right ventricular contractility and right ventricular-arterial coupling in pulmonary hypertension. Am. J. Respir. Crit. Care Med. 2015, 191, 1050–1057. [Google Scholar] [CrossRef] [PubMed]
- Hsu, S.; Houston, B.A.; Tampakakis, E.; Bacher, A.C.; Rhodes, P.S.; Mathai, S.C.; Damico, R.L.; Kolb, T.M.; Hummers, L.K.; Shah, A.A.; et al. Right Ventricular Functional Reserve in Pulmonary Arterial Hypertension. Circulation 2016, 133, 2413–2422. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vonk Noordegraaf, A.; Chin, K.M.; Haddad, F.; Hassoun, P.M.; Hemnes, A.R.; Hopkins, S.R.; Kawut, S.M.; Langleben, D.; Lumens, J.; Naeije, R. Pathophysiology of the right ventricle and of the pulmonary circulation in pulmonary hypertension: An update. Eur. Respir. J. 2019, 53. [Google Scholar] [CrossRef] [PubMed]
- Tello, K.; Dalmer, A.; Axmann, J.; Vanderpool, R.; Ghofrani, H.A.; Naeije, R.; Roller, F.; Seeger, W.; Sommer, N.; Wilhelm, J.; et al. Reserve of Right Ventricular-Arterial Coupling in the Setting of Chronic Overload. Circ. Heart Fail. 2019, 12, e005512. [Google Scholar] [CrossRef] [PubMed]
- Naeije, R.; Richter, M.J.; Vanderpool, R.; Tello, K. When it all comes down to pressure: Right ventricular ejection fraction at cardiac catheterisation. Eur. Respir. J. 2020, 55. [Google Scholar] [CrossRef]
- Coghlan, J.G.; Denton, C.P.; Grunig, E.; Bonderman, D.; Distler, O.; Khanna, D.; Muller-Ladner, U.; Pope, J.E.; Vonk, M.C.; Doelberg, M.; et al. Evidence-based detection of pulmonary arterial hypertension in systemic sclerosis: The DETECT study. Ann. Rheum. Dis. 2014, 73, 1340–1349. [Google Scholar] [CrossRef] [Green Version]
- Coghlan, J.G.; Wolf, M.; Distler, O.; Denton, C.P.; Doelberg, M.; Harutyunova, S.; Marra, A.M.; Benjamin, N.; Fischer, C.; Grunig, E. Incidence of pulmonary hypertension and determining factors in patients with systemic sclerosis. Eur. Respir. J. 2018, 51. [Google Scholar] [CrossRef] [Green Version]
- Nagel, C.; Marra, A.M.; Benjamin, N.; Blank, N.; Cittadini, A.; Coghlan, G.; Distler, O.; Denton, C.P.; Egenlauf, B.; Fiehn, C.; et al. Reduced Right Ventricular Output Reserve in Patients With Systemic Sclerosis and Mildly Elevated Pulmonary Artery Pressure. Arthritis Rheumatol. 2019, 71, 805–816. [Google Scholar] [CrossRef]
- Grünig, E.; Biskupek, J.; D’Andrea, A.; Ehlken, N.; Egenlauf, B.; Weidenhammer, J.; Marra, A.M.; Cittadini, A.; Fischer, C.; Bossone, E. Reference ranges for and determinants of right ventricular area in healthy adults by two-dimensional echocardiography. Respiration 2015, 89, 284–293. [Google Scholar] [CrossRef]
- Fischer, L.; Benjamin, N.; Blank, N.; Egenlauf, B.; Fischer, C.; Harutyunova, S.; Koegler, M.; Lorenz, H.M.; Marra, A.M.; Nagel, C.; et al. Right heart size and function significantly correlate in patients with pulmonary arterial hypertension-a cross-sectional study. Respir. Res. 2018, 19, 216. [Google Scholar] [CrossRef]
- Kovacs, G.; Herve, P.; Barbera, J.A.; Chaouat, A.; Chemla, D.; Condliffe, R.; Garcia, G.; Grünig, E.; Howard, L.; Humbert, M.; et al. An official European Respiratory Society statement: Pulmonary haemodynamics during exercise. Eur. Respir. J. 2017, 50, 1700578. [Google Scholar] [CrossRef]
- Domingo, E.; Grignola, J.C.; Aguilar, R.; Arredondo, C.; Bouteldja, N.; Messeguer, M.L.; Roman, A. Impairment of pulmonary vascular reserve and right ventricular systolic reserve in pulmonary arterial hypertension. BMC Pulm. Med. 2014, 14, 69. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grünig, E.; Weissmann, S.; Ehlken, N.; Fijalkowska, A.; Fischer, C.; Fourme, T.; Galie, N.; Ghofrani, A.; Harrison, R.E.; Huez, S.; et al. Stress Doppler echocardiography in relatives of patients with idiopathic and familial pulmonary arterial hypertension: Results of a multicenter European analysis of pulmonary artery pressure response to exercise and hypoxia. Circulation 2009, 119, 1747–1757. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sano, H.; Tanaka, H.; Motoji, Y.; Mukai, J.; Suto, M.; Takada, H.; Soga, F.; Hatani, Y.; Matsuzoe, H.; Hatazawa, K.; et al. Echocardiography during preload stress for evaluation of right ventricular contractile reserve and exercise capacity in pulmonary hypertension. Echocardiography 2018, 35, 1997–2004. [Google Scholar] [CrossRef] [PubMed]
- Jain, P.; Rao, S.; Macdonald, P.; Kotlyar, E.; Jabbour, A.; Hayward, C.; Keogh, A. Diagnostic Performance of Pulmonary Capacitance at Rest and During Exercise in Idiopathic Pulmonary Arterial Hypertension. Heart Lung Circ. 2019, 28, 289–294. [Google Scholar] [CrossRef]
- Sanz, J.; Kariisa, M.; Dellegrottaglie, S.; Prat-Gonzalez, S.; Garcia, M.J.; Fuster, V.; Rajagopalan, S. Evaluation of pulmonary artery stiffness in pulmonary hypertension with cardiac magnetic resonance. JACC Cardiovasc. Imaging 2009, 2, 286–295. [Google Scholar] [CrossRef]
- Wang, Z.; Chesler, N.C. Pulmonary vascular wall stiffness: An important contributor to the increased right ventricular afterload with pulmonary hypertension. Pulm. Circ. 2011, 1, 212–223. [Google Scholar] [CrossRef] [Green Version]
- Rich, S. Right ventricular adaptation and maladaptation in chronic pulmonary arterial hypertension. Cardiol. Clin. 2012, 30, 257–269. [Google Scholar] [CrossRef]
- Schäfer, M.; Myers, C.; Brown, R.D.; Frid, M.G.; Tan, W.; Hunter, K.; Stenmark, K.R. Pulmonary Arterial Stiffness: Toward a New Paradigm in Pulmonary Arterial Hypertension Pathophysiology and Assessment. Curr. Hypertens. Rep. 2016, 18, 4. [Google Scholar] [CrossRef]
- Stevens, G.R.; Garcia-Alvarez, A.; Sahni, S.; Garcia, M.J.; Fuster, V.; Sanz, J. RV dysfunction in pulmonary hypertension is independently related to pulmonary artery stiffness. JACC Cardiovasc. Imaging 2012, 5, 378–387. [Google Scholar] [CrossRef] [Green Version]
- Van de Veerdonk, M.C.; Kind, T.; Marcus, J.T.; Mauritz, G.J.; Heymans, M.W.; Bogaard, H.J.; Boonstra, A.; Marques, K.M.; Westerhof, N.; Vonk-Noordegraaf, A. Progressive right ventricular dysfunction in patients with pulmonary arterial hypertension responding to therapy. J. Am. Coll. Cardiol. 2011, 58, 2511–2519. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grünig, E.; Tiede, H.; Enyimayew, E.O.; Ehlken, N.; Seyfarth, H.J.; Bossone, E.; D’Andrea, A.; Naeije, R.; Olschewski, H.; Ulrich, S.; et al. Assessment and prognostic relevance of right ventricular contractile reserve in patients with severe pulmonary hypertension. Circulation 2013, 128, 2005–2015. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guo, D.C.; Li, Y.D.; Yang, Y.H.; Zhu, W.W.; Sun, L.L.; Jiang, W.; Ye, X.G.; Cai, Q.Z.; Lu, X.Z. Influence of impaired right ventricular contractile reserve on exercise capacity in patients with precapillary pulmonary hypertension: A study with exercise stress echocardiography. Echocardiography 2019, 36, 671–677. [Google Scholar] [CrossRef] [PubMed]
- Almeida, A.R.; Loureiro, M.J.; Lopes, L.; Cotrim, C.; Lopes, L.; Repolho, D.; Pereira, H. Echocardiographic assessment of right ventricular contractile reserve in patients with pulmonary hypertension. Rev. Port. Cardiol. 2014, 33, 155–163. [Google Scholar] [CrossRef] [PubMed]
- Galiè, N.; Channick, R.N.; Frantz, R.P.; Grünig, E.; Jing, Z.C.; Moiseeva, O.; Preston, I.R.; Pulido, T.; Safdar, Z.; Tamura, Y.; et al. Risk stratification and medical therapy of pulmonary arterial hypertension. Eur. Respir. J. 2019, 53, 801889. [Google Scholar] [CrossRef]
- Bustamante-Labarta, M.; Perrone, S.; De La Fuente, R.L.; Stutzbach, P.; De La Hoz, R.P.; Torino, A.; Favaloro, R. Right atrial size and tricuspid regurgitation severity predict mortality or transplantation in primary pulmonary hypertension. J. Am. Soc. Echocardiogr. 2002, 15, 1160–1164. [Google Scholar] [CrossRef] [Green Version]
- Raymond, R.J.; Hinderliter, A.L.; Willis, P.W.; Ralph, D.; Caldwell, E.J.; Williams, W.; Ettinger, N.A.; Hill, N.S.; Summer, W.R.; de Boisblanc, B.; et al. Echocardiographic predictors of adverse outcomes in primary pulmonary hypertension. J. Am. Coll. Cardiol. 2002, 39, 1214–1219. [Google Scholar] [CrossRef] [Green Version]
- Austin, C.; Alassas, K.; Burger, C.; Safford, R.; Pagan, R.; Duello, K.; Kumar, P.; Zeiger, T.; Shapiro, B. Echocardiographic assessment of estimated right atrial pressure and size predicts mortality in pulmonary arterial hypertension. Chest 2015, 147, 198–208. [Google Scholar] [CrossRef] [Green Version]
- Van Wolferen, S.A.; Marcus, J.T.; Boonstra, A.; Marques, K.M.; Bronzwaer, J.G.; Spreeuwenberg, M.D.; Postmus, P.E.; Vonk-Noordegraaf, A. Prognostic value of right ventricular mass, volume, and function in idiopathic pulmonary arterial hypertension. Eur. Heart J. 2007, 28, 1250–1257. [Google Scholar] [CrossRef] [Green Version]
- Van de Veerdonk, M.C.; Marcus, J.T.; Westerhof, N.; de Man, F.S.; Boonstra, A.; Heymans, M.W.; Bogaard, H.J.; Vonk Noordegraaf, A. Signs of right ventricular deterioration in clinically stable patients with pulmonary arterial hypertension. Chest 2015, 147, 1063–1071. [Google Scholar] [CrossRef]
- Van de Veerdonk, M.C.; Huis In, T.V.A.E.; Marcus, J.T.; Westerhof, N.; Heymans, M.W.; Bogaard, H.J.; Vonk-Noordegraaf, A. Upfront combination therapy reduces right ventricular volumes in pulmonary arterial hypertension. Eur. Respir. J. 2017, 49. [Google Scholar] [CrossRef] [PubMed]
- Weatherald, J.; Boucly, A.; Chemla, D.; Savale, L.; Peng, M.; Jevnikar, M.; Jais, X.; Taniguchi, Y.; O’Connell, C.; Parent, F.; et al. Prognostic Value of Follow-Up Hemodynamic Variables After Initial Management in Pulmonary Arterial Hypertension. Circulation 2018, 137, 693–704. [Google Scholar] [CrossRef] [PubMed]
- Blumberg, F.C.; Arzt, M.; Lange, T.; Schroll, S.; Pfeifer, M.; Wensel, R. Impact of right ventricular reserve on exercise capacity and survival in patients with pulmonary hypertension. Eur. J. Heart Fail. 2013, 15, 771–775. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chaouat, A.; Sitbon, O.; Mercy, M.; Poncot-Mongars, R.; Provencher, S.; Guillaumot, A.; Gomez, E.; Selton-Suty, C.; Malvestio, P.; Regent, D.; et al. Prognostic value of exercise pulmonary haemodynamics in pulmonary arterial hypertension. Eur. Respir. J. 2014, 44, 704–713. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mahapatra, S.; Nishimura, R.A.; Sorajja, P.; Cha, S.; McGoon, M.D. Relationship of pulmonary arterial capacitance and mortality in idiopathic pulmonary arterial hypertension. J. Am. Coll. Cardiol. 2006, 47, 799–803. [Google Scholar] [CrossRef] [PubMed]
- Al-Naamani, N.; Preston, I.R.; Paulus, J.K.; Hill, N.S.; Roberts, K.E. Pulmonary Arterial Capacitance Is an Important Predictor of Mortality in Heart Failure With a Preserved Ejection Fraction. JACC Heart Fail. 2015, 3, 467–474. [Google Scholar] [CrossRef]
- Miller, W.L.; Grill, D.E.; Borlaug, B.A. Clinical features, hemodynamics, and outcomes of pulmonary hypertension due to chronic heart failure with reduced ejection fraction: Pulmonary hypertension and heart failure. JACC Heart Fail. 2013, 1, 290–299. [Google Scholar] [CrossRef]
- Pellegrini, P.; Rossi, A.; Pasotti, M.; Raineri, C.; Cicoira, M.; Bonapace, S.; Dini, F.L.; Temporelli, P.L.; Vassanelli, C.; Vanderpool, R.; et al. Prognostic relevance of pulmonary arterial compliance in patients with chronic heart failure. Chest 2014, 145, 1064–1070. [Google Scholar] [CrossRef]
- Dragu, R.; Rispler, S.; Habib, M.; Sholy, H.; Hammerman, H.; Galie, N.; Aronson, D. Pulmonary arterial capacitance in patients with heart failure and reactive pulmonary hypertension. Eur. J. Heart Fail. 2015, 17, 74–80. [Google Scholar] [CrossRef]
- Medrek, S.K.; Kloefkorn, C.; Nguyen, D.T.M.; Graviss, E.A.; Frost, A.E.; Safdar, Z. Longitudinal change in pulmonary arterial capacitance as an indicator of prognosis and response to therapy and in pulmonary arterial hypertension. Pulm. Circ. 2017, 7, 399–408. [Google Scholar] [CrossRef] [Green Version]
- Gan, C.T.; Lankhaar, J.W.; Westerhof, N.; Marcus, J.T.; Becker, A.; Twisk, J.W.; Boonstra, A.; Postmus, P.E.; Vonk-Noordegraaf, A. Noninvasively assessed pulmonary artery stiffness predicts mortality in pulmonary arterial hypertension. Chest 2007, 132, 1906–1912. [Google Scholar] [CrossRef] [PubMed]
- Ghio, S.; D’Alto, M.; Badagliacca, R.; Vitulo, P.; Argiento, P.; Mulè, M.; Tuzzolino, F.; Scelsi, L.; Romeo, E.; Raineri, C.; et al. Prognostic relevance of pulmonary arterial compliance after therapy initiation or escalation in patients with pulmonary arterial hypertension. Int. J. Cardiol. 2017, 230, 53–58. [Google Scholar] [CrossRef] [PubMed]
- Marra, A.M.; Egenlauf, B.; Ehlken, N.; Fischer, C.; Eichstaedt, C.; Nagel, C.; Bossone, E.; Cittadini, A.; Halank, M.; Gall, H.; et al. Change of right heart size and function by long-term therapy with riociguat in patients with pulmonary arterial hypertension and chronic thromboembolic pulmonary hypertension. Int. J. Cardiol. 2015, 195, 19–26. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marra, A.M.; Halank, M.; Benjamin, N.; Bossone, E.; Cittadini, A.; Eichstaedt, C.A.; Egenlauf, B.; Harutyunova, S.; Fischer, C.; Gall, H.; et al. Right ventricular size and function under riociguat in pulmonary arterial hypertension and chronic thromboembolic pulmonary hypertension (the RIVER study). Respir. Res. 2018, 19, 258. [Google Scholar] [CrossRef] [PubMed]
- Badagliacca, R.; Papa, S.; Matsubara, H.; Lang, I.M.; Poscia, R.; Manzi, G.; Vizza, C.D. The importance of right ventricular evaluation in risk assessment and therapeutic strategies: Raising the bar in pulmonary arterial hypertension. Int. J. Cardiol. 2020, 301, 183–189. [Google Scholar] [CrossRef] [PubMed]
- Vanderpool, R.R.; Desai, A.A.; Knapp, S.M.; Simon, M.A.; Abidov, A.; Yuan, J.X.; Garcia, J.G.N.; Hansen, L.M.; Knoper, S.R.; Naeije, R.; et al. How prostacyclin therapy improves right ventricular function in pulmonary arterial hypertension. Eur. Respir. J. 2017, 50. [Google Scholar] [CrossRef] [Green Version]
- Nagel, C.; Benjamin, N.; Egenlauf, B.; Eichstaedt, C.A.; Fischer, C.; Palevičiūtė, E.; Celutkiene, J.; Harutyunova, S.; Mayer, E.; Nasereddin, M.; et al. Effect of supervised training therapy on pulmonary arterial compliance and stroke volume in severe pulmonary arterial hypertension and inoperable or persistent chronic thromboembolic pulmonary hypertension. Respiration 2020, in press. [Google Scholar]



{kind=link}
{kind=link}
| Parameter | Calculation | Reference Values |
|---|---|---|
| Right heart catheterization | ||
| RV reserve [16,17] | >20%: sensitivity 70% specificity 80% for predicting 18-month survival [16,17] | |
| Peak CI [16,17]. | - | |
| Pulmonary vascular/Cardiovascular reserve/Pressure-flow relationship [13,16] | Cardiovascular reserve = mPAP/CO slope = mPAP/CO | >3 mmHg/L/min = abnormal [13,16] |
| End-systolic elastance [18] | - | |
| PAC [19] | Exercise PAC < 3.2 mL/mmHg: diagnosis of PAH sensitivity 90% specificity 100% | |
| Stress-Doppler Echocardiography | ||
| RV output reserve [20] | <30 mmHg = worse survival | |
| RV contractile reserve Combination of ΔTAPSE ΔRVFAC ΔS‘ [21,22] | Rest to exercise: change in TAPSE change in RV fractional area change change in Doppler-derived tricuspid lateral annular peak systolic velocity | Significantly reduced compared to controls |
| RV free wall strain increase [23] | Increase of strain from rest to a leg-positive pressure stress | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Grünig, E.; Eichstaedt, C.A.; Seeger, R.; Benjamin, N. Right Heart Size and Right Ventricular Reserve in Pulmonary Hypertension: Impact on Management and Prognosis. Diagnostics 2020, 10, 1110. https://doi.org/10.3390/diagnostics10121110
Grünig E, Eichstaedt CA, Seeger R, Benjamin N. Right Heart Size and Right Ventricular Reserve in Pulmonary Hypertension: Impact on Management and Prognosis. Diagnostics. 2020; 10(12):1110. https://doi.org/10.3390/diagnostics10121110
Chicago/Turabian StyleGrünig, Ekkehard, Christina A. Eichstaedt, Rebekka Seeger, and Nicola Benjamin. 2020. "Right Heart Size and Right Ventricular Reserve in Pulmonary Hypertension: Impact on Management and Prognosis" Diagnostics 10, no. 12: 1110. https://doi.org/10.3390/diagnostics10121110
APA StyleGrünig, E., Eichstaedt, C. A., Seeger, R., & Benjamin, N. (2020). Right Heart Size and Right Ventricular Reserve in Pulmonary Hypertension: Impact on Management and Prognosis. Diagnostics, 10(12), 1110. https://doi.org/10.3390/diagnostics10121110