Efficient Anomaly Detection with Generative Adversarial Network for Breast Ultrasound Imaging

 , , , , ,
, , , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Breast Ultrasound Examinations
2.3. Data Set
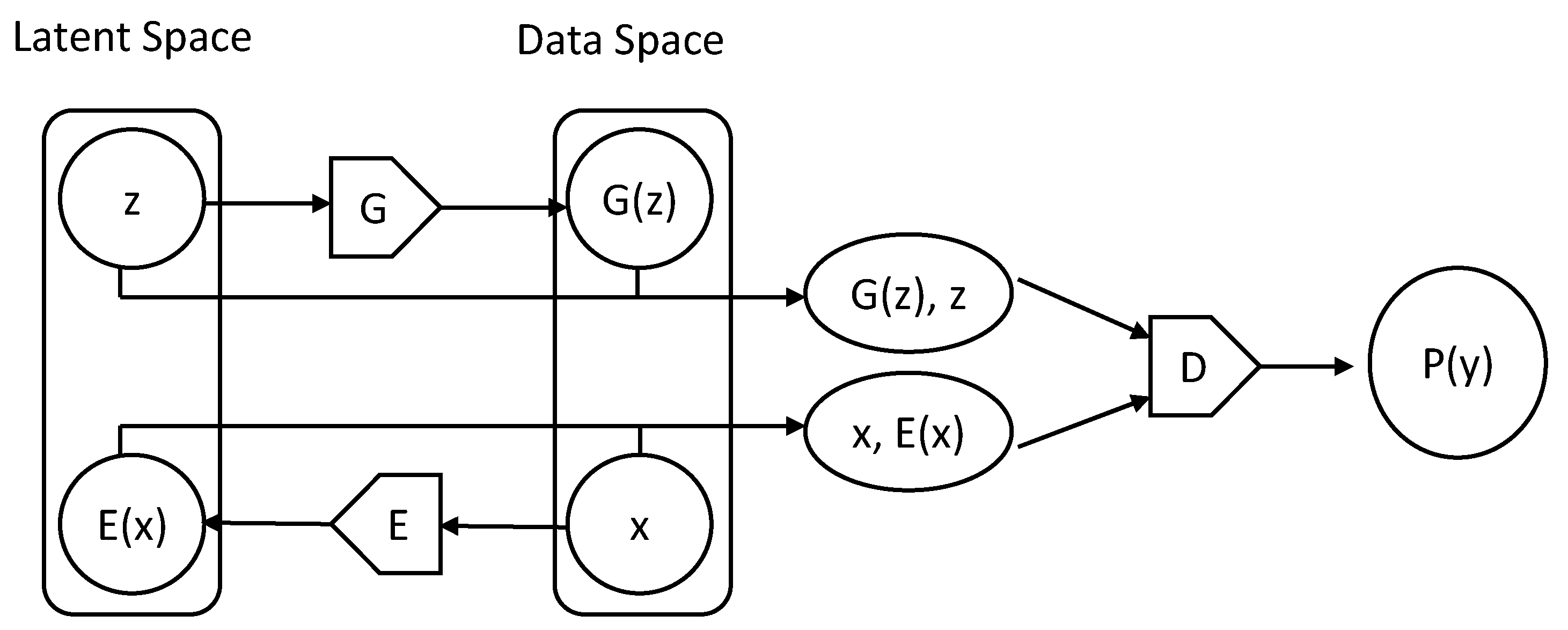
2.4. DL Model
2.5. Statistical Analysis
3. Results
4. Discussion
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer Statistics. CA Cancer J. Clin. 2018, 68, 7–30. [Google Scholar] [CrossRef] [PubMed]
- Kornecki, A. Current status of breast ultrasound. Can Assoc. Radiol. J. 2011, 62, 31–40. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hooley, R.J.; Scoutt, L.M.; Philpotts, L.E. Breast ultrasonography: State of the art. Radiology 2013, 268, 642–659. [Google Scholar] [CrossRef] [PubMed]
- Guo, R.; Lu, G.; Qin, B.; Fei, B. Ultrasound imaging technologies for breast cancer detection and management: A review. Ultrasound Med. Biol. 2018, 44, 37–70. [Google Scholar] [CrossRef]
- D’Orsi, C.; Sickles, E.; Mendelson, E.; Morris, E. Breast Imaging Reporting and Data System, 5th ed.; American College of Radiology: Reston, VA, USA, 2013. [Google Scholar]
- Muenzel, D.; Engels, H.P.; Bruegel, M.; Kehl, V.; Rummeny, E.J.; Metz, S. Intra- and inter-observer variability in measurement of target lesions: Implication on response evaluation according to RECIST 1.1. Radiol. Oncol. 2012, 46, 8–18. [Google Scholar] [CrossRef]
- Bruno, M.A.; Walker, E.A.; Abujudeh, H.H. Understanding and confronting our mistakes: The epidemiology of error in radiology and strategies for error reduction. RadioGraphics 2015, 35, 1668–1676. [Google Scholar] [CrossRef]
- Mendelson, E.B. Artificial intelligence in breast imaging: Potentials and limitations. Am. J. Roentgenol. 2019, 212, 293–299. [Google Scholar] [CrossRef]
- Le, E.P.V.; Wang, Y.; Huang, Y.; Hickman, S.; Gilbert, F.J. Artificial intelligence in breast imaging. Clin. Radiol. 2019, 74, 357–366. [Google Scholar] [CrossRef]
- Wu, G.G.; Zhou, L.Q.; Xu, J.W.; Wang, J.Y.; Wei, Q.; Deng, Y.B.; Cui, X.W.; Dietrich, C.F. Artificial intelligence in breast ultrasound. World J. Radiol. 2019, 11, 19–26. [Google Scholar] [CrossRef]
- Fujioka, T.; Mori, M.; Kubota, K.; Kikuchi, Y.; Katsuta, L.; Adachi, M.; Oda, G.; Nakagawa, T.; Kitazume, Y.; Tateishi, U. Breast ultrasound image synthesis using deep convolutional generative adversarial networks. Diagnostics (Basel) 2019, 9, 176. [Google Scholar] [CrossRef] [Green Version]
- Yi, X.; Walia, E.; Babyn, P. Generative adversarial network in medical imaging: A review. Med. Image Anal. 2019, 58, 101552. [Google Scholar] [CrossRef] [Green Version]
- Fujioka, T.; Kubota, K.; Mori, M.; Kikuchi, Y.; Katsuta, L.; Kasahara, M.; Oda, G.; Ishiba, T.; Nakagawa, T.; Tateishi, U. Distinction between benign and malignant breast masses at breast ultrasound using deep learning method with convolutional neural network. Jpn. J. Radiol. 2019, 37, 466–472. [Google Scholar] [CrossRef] [PubMed]
- Ravi, D.; Wong, C.; Deligianni, F.; Berthelot, M.; Andreu-Perez, J.; Lo, B.; Yang, G.Z. Deep learning for health informatics. IEEE J. Biomed. Health Inform. 2017, 21, 4–21. [Google Scholar] [CrossRef] [Green Version]
- Adachi, M.; Fujioka, T.; Mori, M.; Kubota, K.; Kikuchi, Y.; Xiaotong, W.; Oyama, J.; Kimura, K.; Oda, G.; Nakagawa, T.; et al. Detection and diagnosis of breast cancer using artificial intelligence based assessment of maximum intensity projection dynamic contrast-enhanced magnetic resonance images. Diagnostics 2020, 10, 330. [Google Scholar] [CrossRef] [PubMed]
- Fujioka, T.; Katsuta, L.; Kubota, K.; Mori, M.; Kikuchi, Y.; Kato, A.; Oda, G.; Nakagawa, T.; Kitazume, Y.; Tateishi, U. Classification of breast masses on ultrasound shear wave elastography using convolutional neural networks. Ultrason Imaging 2020. [Google Scholar] [CrossRef] [PubMed]
- Martí, L.; Sanchez-Pi, N.; Molina, J.M.; Garcia, A.C. Anomaly detection based on sensor data in petroleum industry applications. Sensors (Basel) 2015, 15, 2774–2797. [Google Scholar] [CrossRef] [Green Version]
- Schubert, E.; Zimek, A.; Kriegel, H.P. Local Outlier Detection Reconsidered: A generalized view on locality with applications to spatial, video, and network outlier detection. Data Min. Knowl. Discov. 2014, 28, 190–237. [Google Scholar] [CrossRef]
- Schlegl, T.; Seeböck, P.; Waldstein, S.M.; Schmidt-Erfurth, U.; Langs, G. Unsupervised anomaly detection with generative adversarial networks to guide marker discovery. IPMI 2017, 146–157. [Google Scholar]
- Schlegl, T.; Seeböck, P.; Waldstein, S.M.; Langs, G.; Schmidt-Erfurth, U. f-AnoGAN: Fast unsupervised anomaly detection with generative adversarial networks. Med. Image Anal. 2019, 54, 30–44. [Google Scholar] [CrossRef]
- Zenati, H.; Foo, C.S.; Lecouat, B.; Manek, G.; Chandrasekhar, V.R. Efficient Gan-based anomaly detection. arXiv 2018, arXiv:1802.06222. [Google Scholar]
- Goodfellow, I.J.; Pouget-Abadie, J.; Mirza, M.; Xu, B.; Warde-Farley, D.; Ozair, S.; Courville, A.; Bengio, Y. Generative adversarial networks. arXiv 2014, arXiv:1406.2661. [Google Scholar]
- Ngo, C.P.; Winarto, A.A.; Li, C.K.K.; Park, S.; Akram, F.; Lee, H.K. Fence GAN: Towards better anomaly detection. arXiv 2019, arXiv:1904.01209. [Google Scholar]
- Donahue, J.; Krahenbuhl, P.; Darrell, T. Adversarial feature learning. arXiv 2016, arXiv:1605.09782. [Google Scholar]
- Kanda, Y. Investigation of the freely available easy-to-use software ‘EZR’ for medical statistics. Bone Marrow Transplant. 2013, 48, 452–458. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fujioka, T.; Kubota, K.; Mori, M.; Katsuta, L.; Kikuchi, Y.; Kimura, K.; Kimura, M.; Adachi, M.; Oda, G.; Nakagawa, T.; et al. Virtual Interpolation Images of Tumor Development and Growth on Breast Ultrasound Image Synthesis with Deep Convolutional Generative Adversarial Networks. J. Ultrasound Med. 2020. [Google Scholar] [CrossRef]
- Chen, X.; Konukoglu, E. Unsupervised Detection of Lesions in Brain MRI using constrained adversarial auto-encoders. arXiv 2018, arXiv:1806.04972. [Google Scholar]
- Choi, H.; Ha, S.; Kang, H.; Lee, H.; Lee, D.S. Deep Learning Only by Normal Brain PET identify unheralded brain anomalies for the Alzheimer’s disease. EBioMedicine 2019, 43, 447–453. [Google Scholar] [CrossRef] [Green Version]
- Tong, Y.Y.; Sun, P.X.; Zhou, J.; Shi, Z.T.; Chang, C.; Li, J.W. The association between ultrasound features and biological properties of invasive breast carcinoma is modified by age, tumor size, and the preoperative axilla status. J. Ultrasound Med. 2019, 39, 1125–1134. [Google Scholar] [CrossRef]
- Basile, T.; Fanizzi, A.; Losurdo, L.; Bellotti, R.; Bottigli, U.; Dentamaro, R.; Didonna, V.; Fausto, A.; Massafra, R.; Moschetta, M.; et al. Microcalcification detection in full-field digital mammograms: A fully automated computer-aided system. Phys. Med. 2019, 64, 1–9. [Google Scholar] [CrossRef]
- Fausto, A.; Bernini, M.; La Forgia, D.; Fanizzi, A.; Marcasciano, M.; Volterrani, L.; Casella, D.; Mazzei, M.A. Six-year prospective evaluation of second-look US with volume navigation for MRI-detected additional breast lesions. Eur. Radiol. 2019, 29, 1799–1808. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Header | Training Data | Test Data | |||
|---|---|---|---|---|---|
| Normal | Normal | Benign | Malignant | ||
| Patients (n) | 70 | 27 | 48 | 72 | |
| Images (n) | 531 | 51 | 48 | 72 | |
| Age | Mean ± SD (years) | 56.8 ± 12.9 | 52.6 ± 15.8 | 49.2 ± 12.8 | 62.3 ± 13.3 |
| Range (years) | 27–85 | 22–77 | 25–78 | 35–92 | |
| Maximum Diameter | Mean ± SD (mm) | 12.8 ± 7.4 | 18.2 ± 9.2 | ||
| Range (mm) | 5–39 | 5–41 | |||
| Test Data | |
|---|---|
| Benign (n = 48) | Malignant (n = 72) |
| Fibroadenoma, 17 | Ductal carcinoma in situ, 3 |
| Intraductal papilloma, 8 | Invasive ductal carcinoma, 57 |
| Mastopathy, 5 | Mucinous carcinoma, 3 |
| Adenosis, 1 | Invasive lobular carcinoma, 4 |
| Pseudoangiomatous stromal hyperplasia, 1 | Apocrine carcinoma, 2 |
| Radial scar/complex sclerosing lesion, 1 | Invasive micropapillary carcinoma, 2 |
| No malignancy, 2 | Malignant lymphoma, 1 |
| Unknown, 13 (Diagnosed at follow-up) | |
| Header | Mean ± SD | Minimal | Maximum | p | |
|---|---|---|---|---|---|
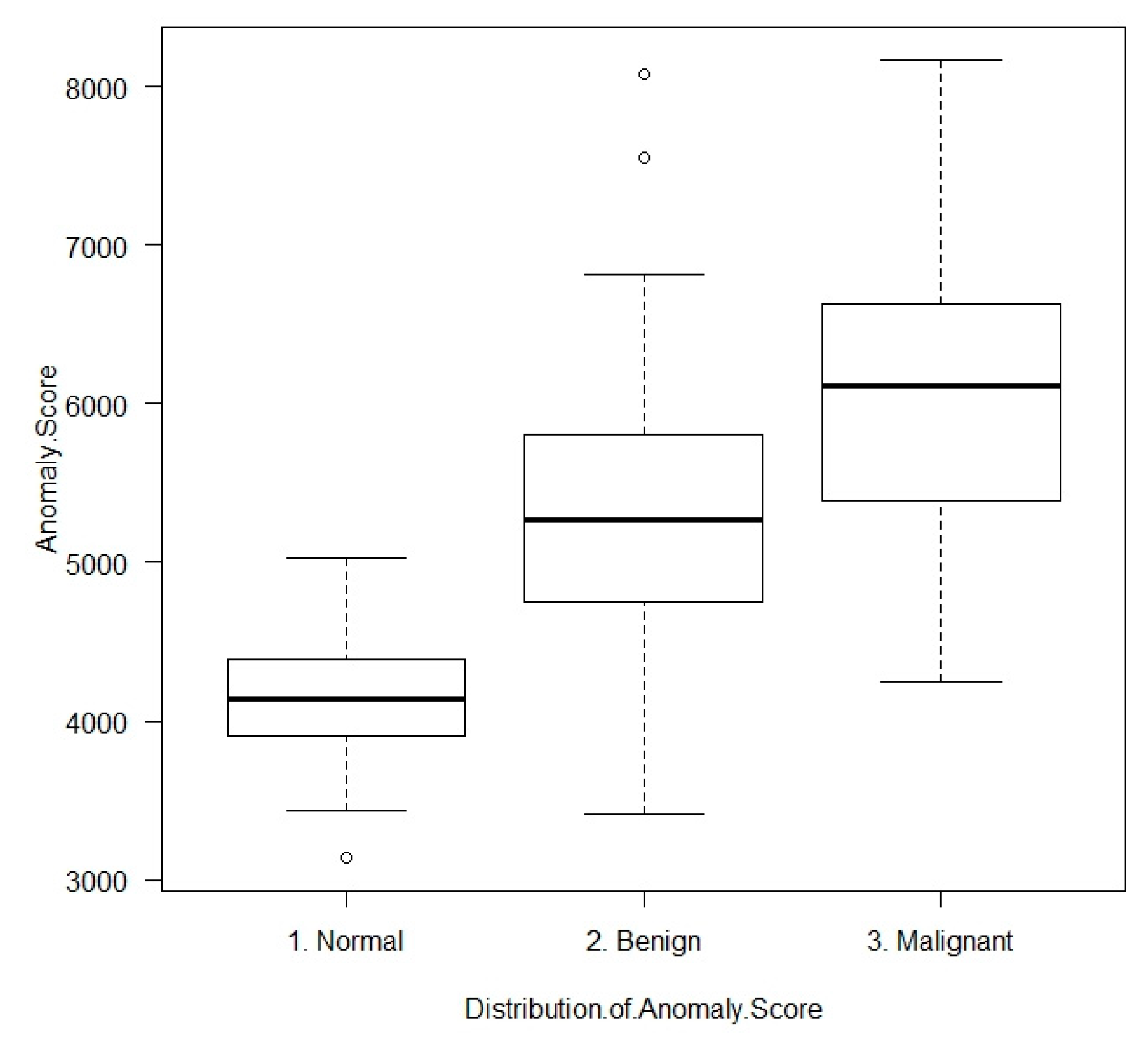
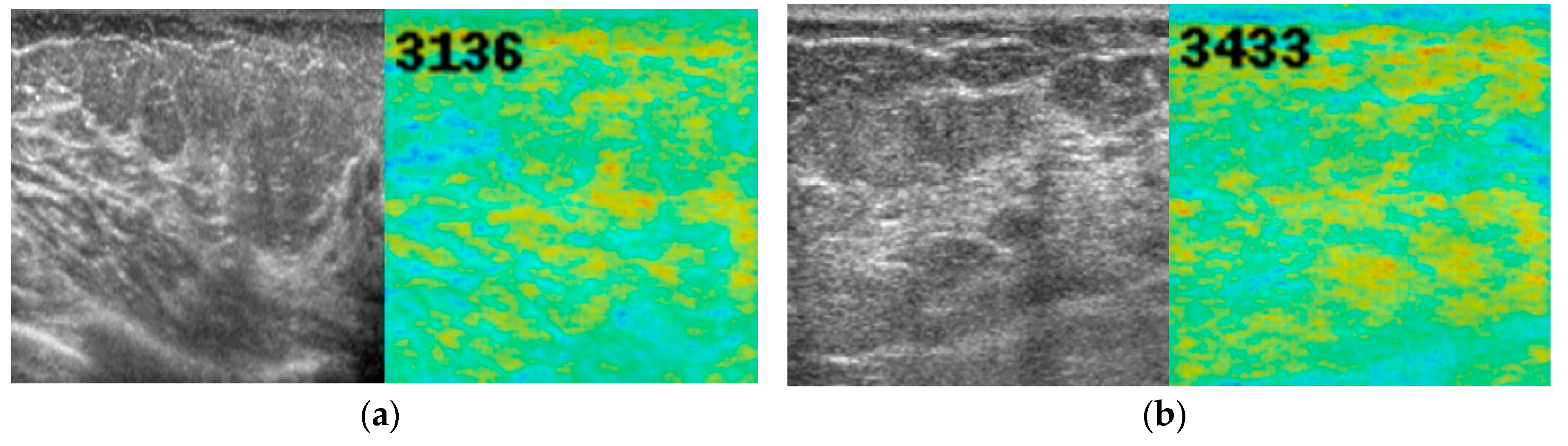
| Normal | 4157.5 ± 418.3 | 3136 | 5021 | <0.001 a | |
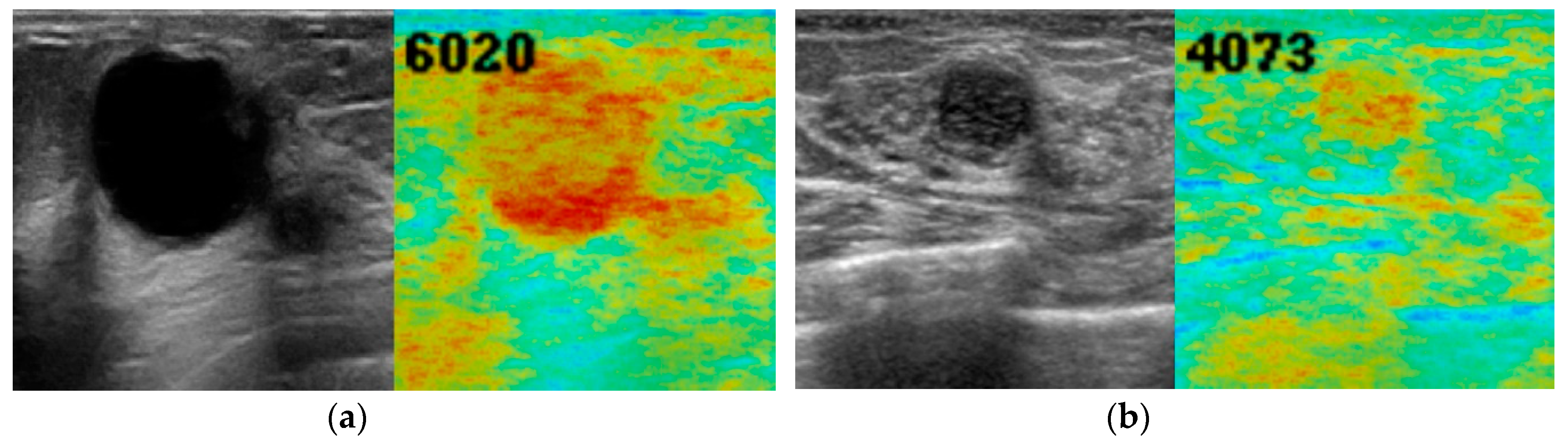
| Benign | 5283.4 ± 953.3 | 3411 | 8082 | ||
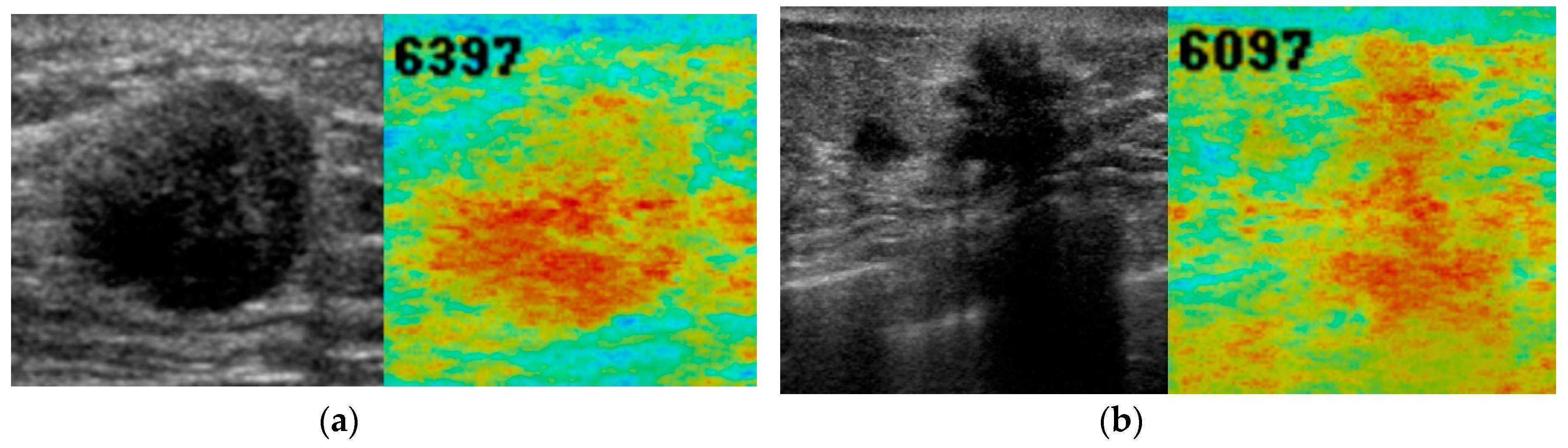
| Malignant | 6047.0 ± 842.1 | 4249 | 8170 | ||
| All | 5269.1 ± 1107.2 | 3136 | 8170 | ||
| Benign | <15 mm | 5271.8 ± 916.5 | 3589 | 7552 | =0.907 b |
| ≥15 mm | 5306.7 ± 1054.1 | 3411 | 8082 | ||
| Malignant | <15 mm | 5813.7 ± 763.5 | 4656 | 8170 | =0.025 b |
| ≥15 mm | 6255.7 ± 863.7 | 4249 | 7202 | ||
| Header | Sensitivity | Specificity | Cutoff Value (Anomaly Score) | AUC [95% CI] |
|---|---|---|---|---|
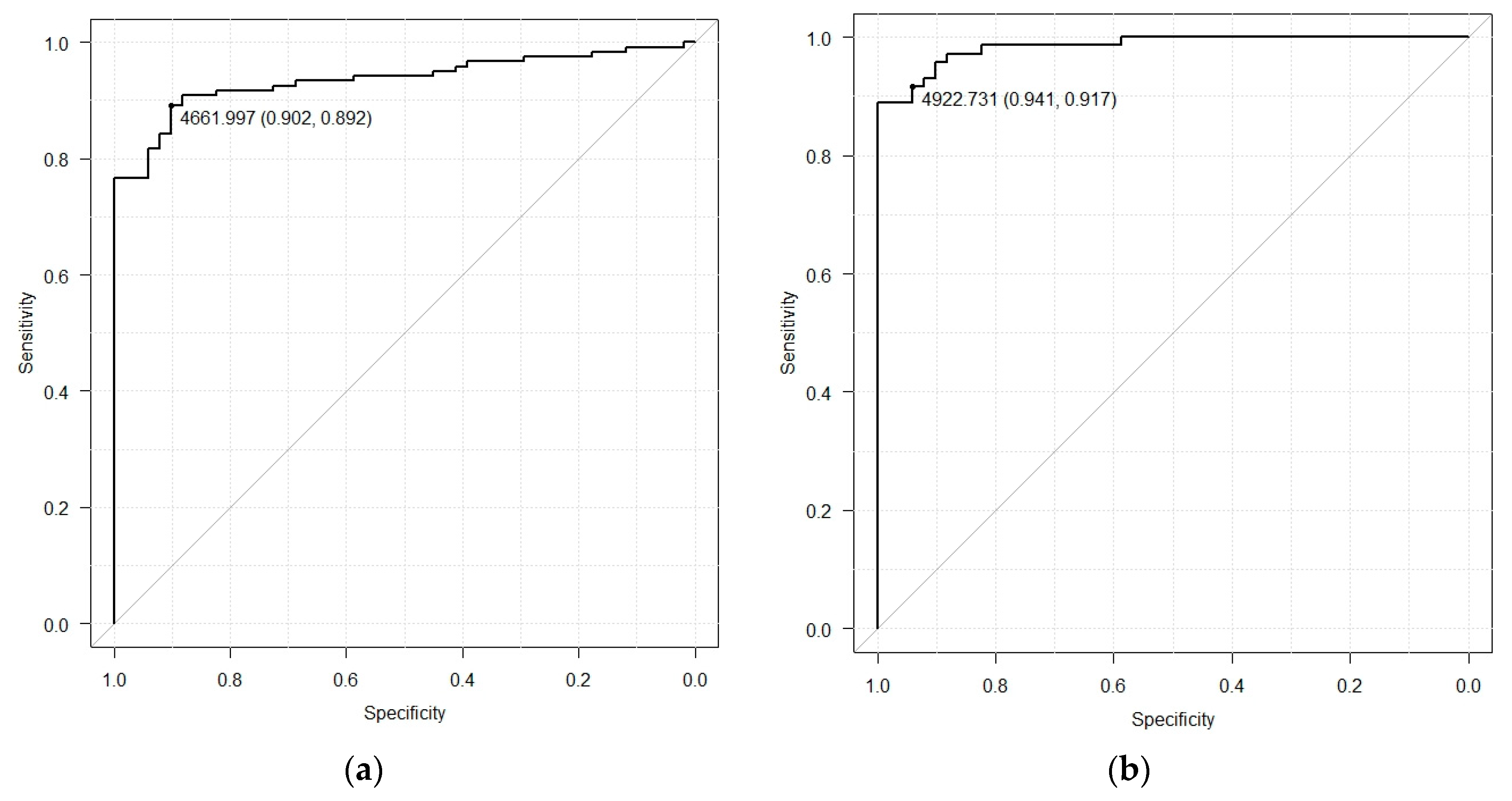
| Normal Vs. Benign + Malignant | 89.2% | 90.2% | 4662 | 0.936 [0.900–0.972] |
| Normal Vs. Malignant | 91.7% | 94.1% | 4923 | 0.985 [0.969–1.000] |
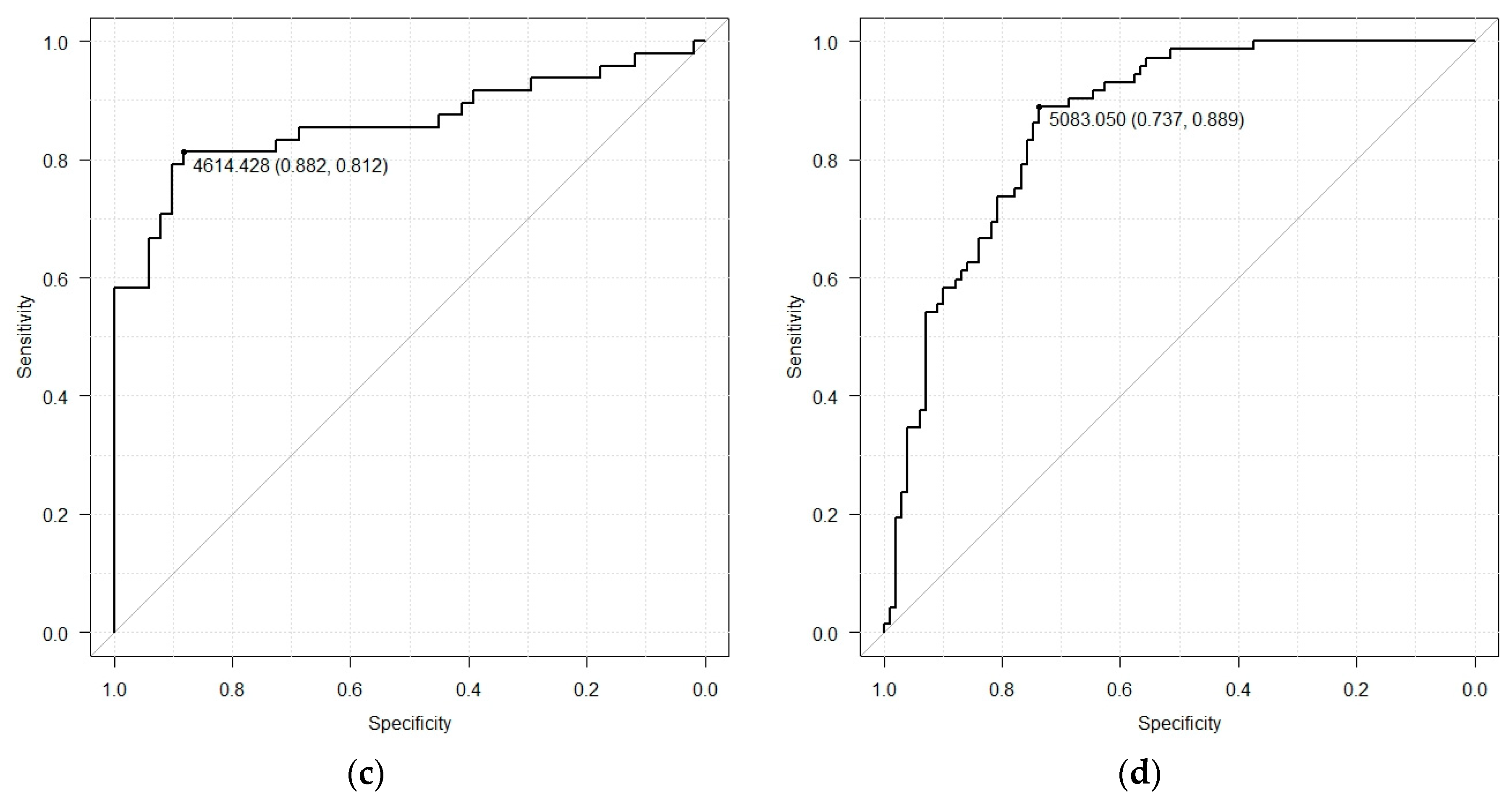
| Normal Vs. Benign | 81.2% | 88.2% | 4614 | 0.862 [0.783–0.941] |
| Normal + Benign Vs. Malignant | 88.9% | 73.7% | 5083 | 0.863 [0.809–0.917] |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fujioka, T.; Kubota, K.; Mori, M.; Kikuchi, Y.; Katsuta, L.; Kimura, M.; Yamaga, E.; Adachi, M.; Oda, G.; Nakagawa, T.; et al. Efficient Anomaly Detection with Generative Adversarial Network for Breast Ultrasound Imaging. Diagnostics 2020, 10, 456. https://doi.org/10.3390/diagnostics10070456
Fujioka T, Kubota K, Mori M, Kikuchi Y, Katsuta L, Kimura M, Yamaga E, Adachi M, Oda G, Nakagawa T, et al. Efficient Anomaly Detection with Generative Adversarial Network for Breast Ultrasound Imaging. Diagnostics. 2020; 10(7):456. https://doi.org/10.3390/diagnostics10070456
Chicago/Turabian StyleFujioka, Tomoyuki, Kazunori Kubota, Mio Mori, Yuka Kikuchi, Leona Katsuta, Mizuki Kimura, Emi Yamaga, Mio Adachi, Goshi Oda, Tsuyoshi Nakagawa, and et al. 2020. "Efficient Anomaly Detection with Generative Adversarial Network for Breast Ultrasound Imaging" Diagnostics 10, no. 7: 456. https://doi.org/10.3390/diagnostics10070456
APA StyleFujioka, T., Kubota, K., Mori, M., Kikuchi, Y., Katsuta, L., Kimura, M., Yamaga, E., Adachi, M., Oda, G., Nakagawa, T., Kitazume, Y., & Tateishi, U. (2020). Efficient Anomaly Detection with Generative Adversarial Network for Breast Ultrasound Imaging. Diagnostics, 10(7), 456. https://doi.org/10.3390/diagnostics10070456