Microstructural Predictors of Cognitive Impairment in Cerebral Small Vessel Disease and the Conditions of Their Formation

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
Study Population
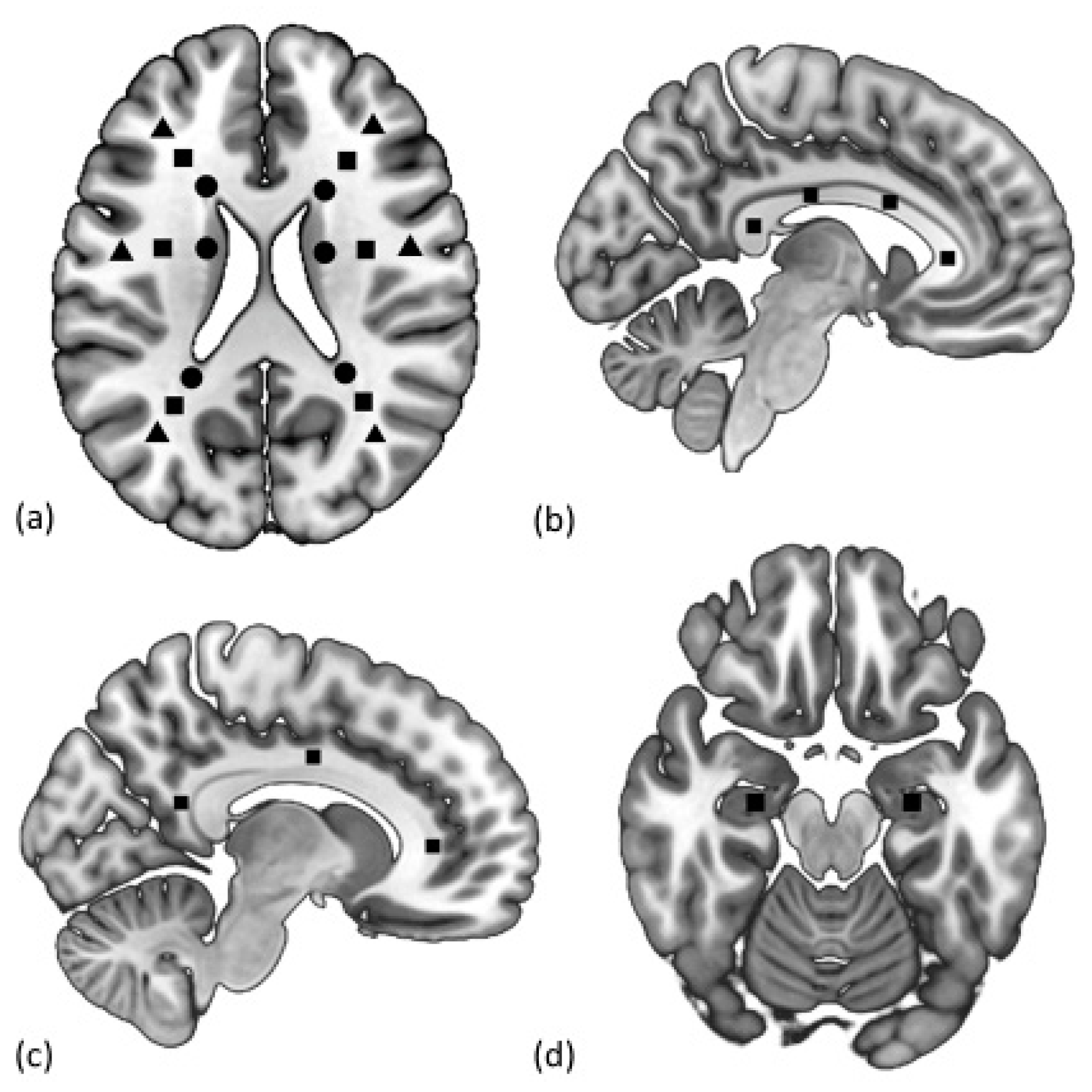
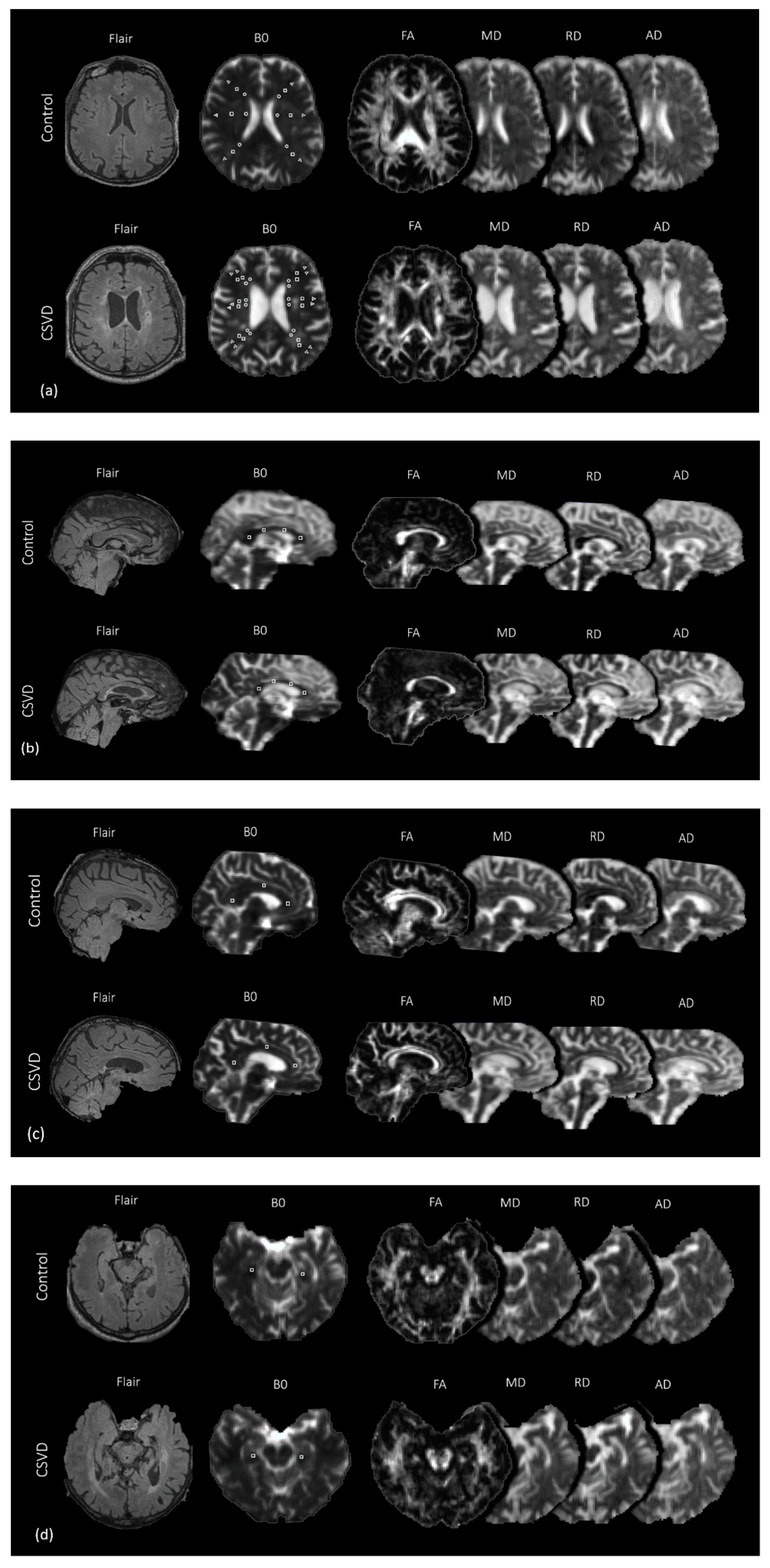
3. MRI Protocol and Imaging Analysis
3.1. Routine MRI
3.2. Diffusion-Tensor Imaging
3.3. Phase Contrast MRI
3.4. Brain Segmentation
3.5. Statistical Analysis
4. Results
4.1. Participant Characteristics
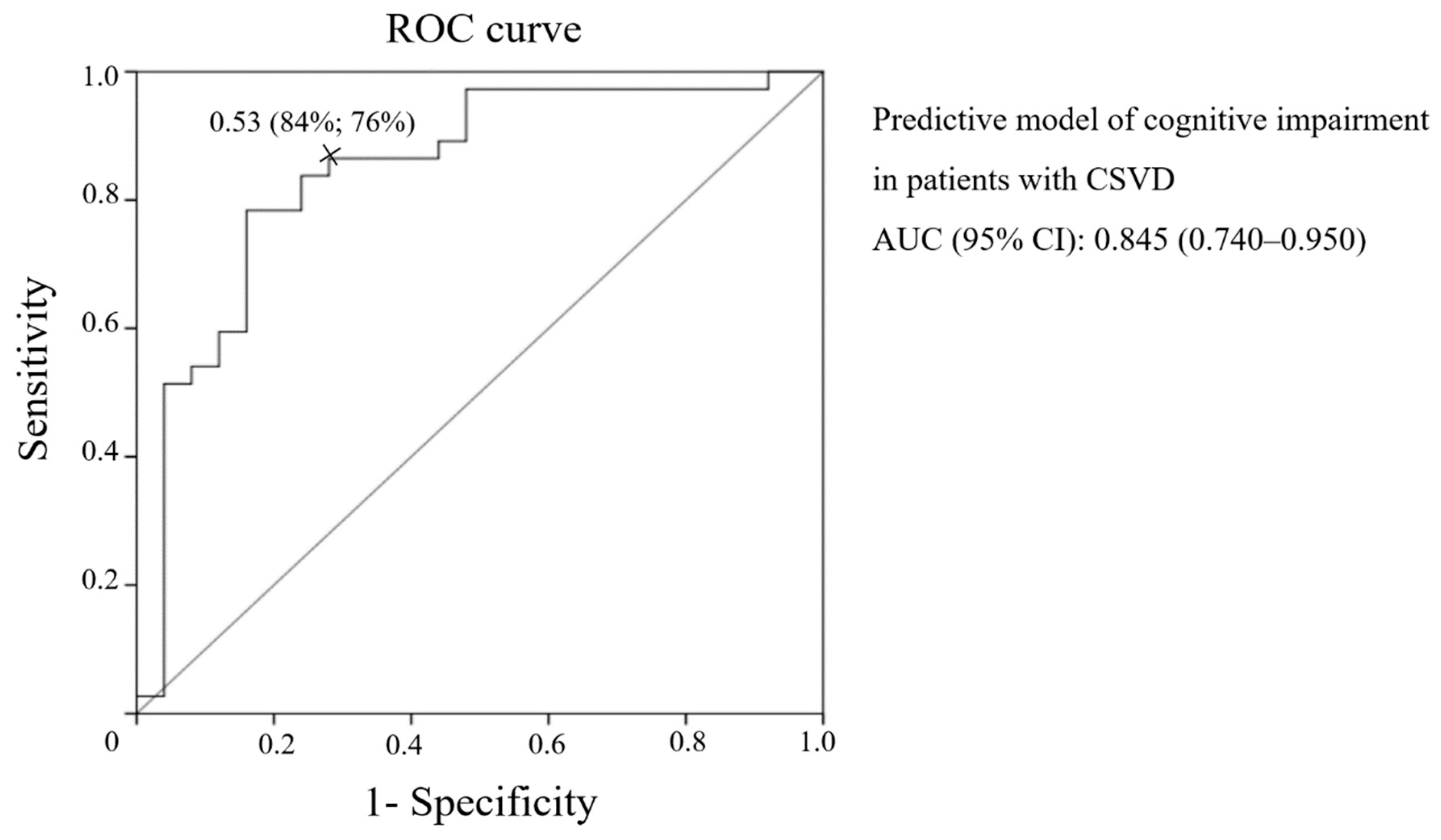
4.2. Association between DTI Values and Cognitive Impairment
4.3. Association between DTI Parameters and Blood Flow, CSF Flow, and Brain Atrophy
5. Discussion
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| AD | Axial diffusivity |
| AH | Arterial hypertension |
| aqCSF flow | Aqueduct cerebrospinal fluid flow |
| AUC | Area under the curve |
| CB | Cingulum bundle |
| CC | Corpus callosum |
| CI | Confidence interval |
| CSF | Cerebrospinal fluid |
| CSVD | Cerebral small vessel disease |
| DM | Diabetes mellitus |
| dNAWM | Deep normal appearing white matter |
| DTI | Diffusion tensor imaging |
| FA | Fractional anisotropy |
| jcNAWM | Juxtacortical normal appearing white matter |
| MCI | Mild cognitive impairment |
| MD | Mean Diffusivity |
| MoCA | Montreal Cognitive Assessment |
| MRI | Magnetic resonance imaging |
| NAWM | Normal appearing white matter |
| OR | Odds ratio |
| PC-MRI | Phase contrast magnetic resonance imaging |
| Pi | Pulsatility index |
| pvNAWM | Periventricular normal appearing white matter |
| RD | Radial diffusivity |
| ROC | Receiver operating characteristic |
| ROI | Region of interest |
| stVBF | Straight sinus venous blood flow |
| SCI | Subjective cognitive impairment |
| sssVBF | Superior sagittal sinus venous blood flow |
| sAq | Surface area aqueduct |
| tABF | Total arterial blood flow |
| tBV | Total brain volume |
| tCSF | Total cerebrospinal fluid |
| tGM | Total gray matter |
| tWM | Total white matter |
| vLV | Volume of lateral ventricles |
| vWMH | Volume of white matter hyperintensity |
| WMHs | White matter hyperintensities |
Appendix A

References
- Gorelick, P.B.; Scuteri, A.; Black, S.E.; Decarli, C.; Greenberg, S.M.; Iadecola, C.; Launer, L.J.; Laurent, S.; Lopez, O.L.; Nyenhuis, D.; et al. Vascular contributions to cognitive impairment and dementia: A statement for healthcare professionals from the American Heart Association/American Stroke Association. Stroke 2011, 42, 2672–2713. [Google Scholar] [CrossRef] [PubMed]
- Deramecourt, V.; Slade, J.Y.; Oakley, A.E.; Perry, R.H.; Ince, P.G.; Maurage, C.-A.; Kalaria, R.N. Staging and natural history of cerebrovascular pathology in dementia. Neurology 2012, 78, 1043–1050. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wardlaw, J.M.; Smith, C.; Dichgans, M. Mechanisms of sporadic cerebral small vessel disease: Insights from neuroimaging. Lancet Neurol. 2013, 12, 483–497. [Google Scholar] [CrossRef] [Green Version]
- Livingston, G.; Sommerlad, A.; Orgeta, V.; Costafreda, S.G.; Huntley, J.; Ames, D.; Ballard, C.; Banerjee, S.; Burns, A.; Cohen-Mansfield, J.; et al. Dementia prevention, intervention, and care. Lancet 2017, 390, 2673–2734. [Google Scholar] [CrossRef] [Green Version]
- Azarpazhooh, M.R.; Avan, A.; Cipriano, L.E.; Munoz, D.G.; Sposato, L.A.; Hachinski, V. Concomitant vascular and neurodegenerative pathologies double the risk of dementia. Alzheimers Dement. 2018, 14, 148–156. [Google Scholar] [CrossRef]
- Smith, E.E.; Beaudin, A.E. New insights into cerebral small vessel disease and vascular cognitive impairment from MRI. Curr. Opin. Neurol. 2018, 31, 36–43. [Google Scholar] [CrossRef]
- Wardlaw, J.M.; Smith, E.E.; Biessels, G.J.; Cordonnier, C.; Fazekas, F.; Frayne, R.; Lindley, R.I.; O’Brien, J.T.; Barkhof, F.; Benavente, O.R.; et al. Neuroimaging standards for research into small vessel disease and its contribution to ageing and neurodegeneration. Lancet Neurol. 2013, 12, 822–838. [Google Scholar] [CrossRef] [Green Version]
- Dichgans, M.; Wardlaw, J.; Smith, E.E.; Zietmann, V.; Seshadri, S.; Sachdev, P.; Biessels, G.J.; Fazekas, F.; Benavente, O.R.; Pantoni, L.; et al. METACOHORTS for the study of vascular disease and its contribution to cognitive decline and neurodegeneration: An initiative of the Joint Programme for Neurodegenerative Disease Research. Alzheimers Dement. 2016, 12, 1235–1249. [Google Scholar] [CrossRef] [Green Version]
- Smith, E.E.; Biessels, G.J.; De Guio, F.; de Leeuw, F.E.; Duchesne, S.; During, M.; Frayne, R.; Ikram, M.A.; Jouvent, E.; MacIntosh, B.J.; et al. Harmonizing brain magnetic resonance imaging methods for vascular contributions to neurodegeneration. Alzheimers Dement. 2019, 11, 191–204. [Google Scholar] [CrossRef]
- Schmidt, R.; Berghold, A.; Jokinen, H.; Gouw, A.; van der Flier, W.; Barkof, F.; Scheltens, P.; Petrovic, K.; Madureira, S.; Verdelho, A.; et al. White matter lesion progression in LADIS: Frequency, clinical effects, and sample size calculations. Stroke 2012, 43, 2643–2647. [Google Scholar] [CrossRef]
- Pasi, M.; van Uden, I.W.; Tuladhar, A.M.; de Leeuw, F.E.; Pantoni, L. White matter microstructural damage on diffusion tensor imaging in cerebral small vessel disease: Clinical consequences. Stroke 2016, 47, 1679–1684. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Raja, R.; Rosenberg, G.; Caprihan, A. Review of diffusion MRI studies in chronic white matter diseases. Neurosci. Lett. 2019, 694, 198–207. [Google Scholar] [CrossRef] [PubMed]
- Gouw, A.A.; Seewann, A.; van der Flier, W.M.; Barkhof, F.; Rozemuller, A.M.; Scheltens, P.; Geurts, J.J.G. Heterogeneity of small vessel disease: A systematic review of MRI and histopathology correlations. J. Neurol. Neurosurg. Psychiatr. 2011, 82, 126–135. [Google Scholar] [CrossRef] [PubMed]
- Hase, Y.; Horsburgh, K.; Ihara, M.; Kalaria, R.N. White matter degeneration in vascular and other ageing-related dementias. J. Neurochem. 2018, 144, 617–633. [Google Scholar] [CrossRef] [PubMed]
- Lawrence, A.J.; Brookes, R.L.; Zeestraten, E.A.; Barrick, T.R.; Morris, R.G.; Markus, H.S. Pattern and rate of cognitive decline in cerebral small vessel disease: A prospective study. PLoS ONE 2015, 10, e0135523. [Google Scholar] [CrossRef]
- Benjamin, P.; Zeestraten, E.; Lambert, C.; Ster, I.C.; Williams, O.A.; Lawrence, A.J.; Patel, B.; MacKinnon, A.D.; Barrick, T.R.; Markus, H.S. Progression of MRI markers in cerebral small vessel disease: Sample size considerations for clinical trials. J. Cereb. Blood Flow Metab. 2016, 36, 228–240. [Google Scholar] [CrossRef]
- Pasi, M.; Salvadori, E.; Poggesi, A.; Ciolli, L.; Del Bene, A.; Marini, S.; Nannucci, S.; Pescini, F.; Valenti, R.; Ginestroni, A.; et al. White matter microstructural damage in small vessel disease is associated with Montreal cognitive assessment but not with mini mental state examination performances: Vascular mild cognitive impairment Tuscany study. Stroke 2015, 46, 262–264. [Google Scholar] [CrossRef] [Green Version]
- O’Sullivan, M.; Morris, R.G.; Huckstep, B.; Jones, D.K.; Williams, S.C.; Markus, H.S. Diffusion tensor MRI correlates with executive dysfunction in patients with ischaemic leukoaraiosis. J. Neurol. Neurosurg. Psychiatr. 2004, 75, 441–447. [Google Scholar] [CrossRef] [Green Version]
- Nitkunan, A.; Barrick, T.R.; Charlton, R.A.; Clark, C.A.; Markus, H.S. Multimodal MRI in cerebral small vessel disease: Its relationship with cognition and sensitivity to change over time. Stroke 2008, 39, 1999–2005. [Google Scholar] [CrossRef] [Green Version]
- Tuladhar, A.M.; van Norden, A.G.; de Laat, K.F.; Zwiers, M.P.; van Dijk, E.J.; Norris, D.G.; de Leeuw, F.-E. White matter integrity in small vessel disease is related to cognition. Neuroimag. Clin. 2015, 7, 518–524. [Google Scholar] [CrossRef] [Green Version]
- Baykara, E.; Gesierich, B.; Adam, R.; Tuladhar, A.M.; Biesbroek, J.M.; Koek, H.L.; Ropele, S.; Jouvent, E.; Chabriat, H.; Ertl-Wagnere, B.; et al. A novel imaging marker for small vessel disease based on skeletonization of white matter tracts and diffusion histograms. Ann. Neurol. 2016, 80, 581–592. [Google Scholar] [CrossRef] [PubMed]
- Croall, I.D.; Lohner, V.; Moynihan, B.; Moynihan, B.; Khan, U.; Hassan, A.; O’Brien, J.T.; Morris, R.G.; Tozer, D.J.; Cambridge, V.C.; et al. Using DTI to assess white matter microstructure in cerebral small vessel disease (SVD) in multicentre studies. Clin. Sci. (London) 2017, 131, 1361–1373. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Song, S.K.; Sun, S.W.; Ju, W.K.; Lin, S.J.; Cross, A.H.; Neufeld, A.H. Diffusion tensor imaging detects and differentiates axon and myelin degeneration in mouse optic nerve after retinal ischemia. Neuroimage 2003, 20, 1714–1722. [Google Scholar] [CrossRef] [PubMed]
- Winklewski, P.J.; Sabisz, A.; Naumczyk, P.; Jodzio, K.; Szurowska, E.; Szarmach, A. Understanding the physiopathology behind axial and radial diffusivity changes-what do we know? Front. Neurol. 2018, 9, 92. [Google Scholar] [CrossRef] [Green Version]
- Lawrence, A.J.; Patel, B.; Morris, R.G.; MacKinnon, A.D.; Rich, P.M.; Barrick, T.R.; Markus, H.S. Mechanisms of cognitive impairment in cerebral small vessel disease: Multimodal MRI results from the St George’s cognition and neuroimaging in stroke (SCANS) study. PLoS ONE 2013, 8, e61014. [Google Scholar] [CrossRef]
- Williams, O.A.; Zeestraten, E.A.; Benjamin, P.; Lambert, C.; Lawrence, A.J.; MacKinnon, A.D.; Morris, R.G.; Markus, H.S.; Charlton, R.A.; Barrick, T.R. Diffusion tensor image segmentation of the cerebrum provides a single measure of cerebral small vessel disease severity related to cognitive change. Neuroimag. Clin. 2017, 16, 330–342. [Google Scholar] [CrossRef]
- Williams, O.A.; Zeestraten, E.A.; Benjamin, P.; Lambert, C.; Lawrence, A.J.; MacKinnon, A.D.; Morris, R.G.; Markus, H.S.; Charlton, R.A.; Barrick, T.R. Predicting dementia in cerebral small vessel disease using an automatic diffusion tensor image segmentation technique. Stroke 2019, 50, 2775–2782. [Google Scholar] [CrossRef]
- Van der Holst, H.M.; Tuladhar, A.M.; van Norden, A.G.; de Laat, K.F.; van Uden, I.W.N.; van Oudheusden, L.J.B.; Zwiers, M.P.; Norris, D.G.; Kessels, R.P.C.; de Leeuw, F.E. Microstructural integrity of the cingulum is related to verbal memory performance in elderly with cerebral small vessel disease: The RUN DMC study. Neuroimage 2013, 65, 416–423. [Google Scholar] [CrossRef] [Green Version]
- Liu, X.; Cheng, R.; Chen, L.; Luo, T.; Lv, F.; Gong, J.; Jiang, P. Alterations of white matter integrity in subcortical ischemic vascular disease with and without cognitive impairment: A TBSS study. J. Mol. Neurosci. 2019, 67, 595–603. [Google Scholar] [CrossRef]
- Palesi, F.; De Rinaldis, A.; Vitali, P.; Castellazzi, G.; Casiraghi, L.; Germani, G.; Bernini, S.; Anzalone, N.; Cotta Ramusino, M.; Denaro, F.M.; et al. Specific patterns of white matter alterations help distinguishing alzheimer’s and vascular dementia. Front. Neurosci. 2018, 12, 274. [Google Scholar] [CrossRef]
- Reed, B.R.; Mungas, D.M.; Kramer, J.H.; Ellis, W.; Vinters, H.V.; Zarow, C.; Jagust, W.J.; Chui, H.C. Profiles of neuropsychological impairment in autopsy-defined Alzheimer’s disease and cerebrovascular disease. Brain 2007, 130 Pt 3, 731–739. [Google Scholar] [CrossRef] [PubMed]
- Vasquez, B.P.; Zakzanis, K.K. The neuropsychological profile of vascular cognitive impairment not demented: A meta-analysis. J. Neuropsychol. 2015, 109–136. [Google Scholar] [CrossRef] [PubMed]
- Dobrynina, L.A.; Gadzhieva ZSh Kalashnikova, L.A.; Gnedovskaya, E.V.; Piradov, M.A. Neuropsychological profile and vascular risk factors in patients with cerebral microangiopathy. Ann. Clin. Exp. Neurol. 2018, 12, 5–15. (In Russian) [Google Scholar] [CrossRef]
- Shim, Y.S.; Yang, D.W.; Roe, C.M.; Coats, M.A.; Benzinger, T.L.; Xiong, C.; Galvin, J.E.; Cairns, N.J.; Morris, J.C. Pathological correlates of white matter hyperintensities on magnetic resonance imaging. Dement. Geriatr. Cogn. Disord. 2015, 39, 92–104. [Google Scholar] [CrossRef] [Green Version]
- Mancia, G.; Fagard, R.; Narkiewicz, K.; Redón, J.; Zanchetti, A.; Böhm, M.; Christiaens, T.; Cifkova, R.; De Backer, G.; Dominiczak, A.; et al. 2013 ESH/ESC Guidelines for the management of arterial hypertension: The Task Force for the management of arterial hypertension of the European Society of Hypertension (ESH) and of the European Society of Cardiology (ESC). J. Hypertens. 2013, 31, 1281–1357. [Google Scholar] [CrossRef] [Green Version]
- Nasreddine, Z.S.; Phillips, N.A.; Bédirian, V.; Charbonneau, S.; Whitehead, V.; Collin, I.; Cummings, J.L.; Chertkow, H. The montreal cognitive assessment, MoCA: A brief screening tool for mild cognitive impairment. J. Am. Geriatr. Soc. 2005, 53, 695–699. [Google Scholar] [CrossRef]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; DSM-5; American Psychiatric Publishing: Arlington, VA, USA, 2013; p. 991. [Google Scholar]
- Albert, M.S.; DeKosky, S.T.; Dickson, D.; Dubois, B.; Feldman, H.H.; Fox, N.C.; Gamst, A.; Holtzman, D.M.; Jagust, W.J.; Petersen, R.C.; et al. The diagnosis of mild cognitive impairment due to Alzheimer’s disease: Recommendations from the National Institute on Aging-Alzheimer’s Association workgroups on diagnostic guidelines for Alzheimer’s disease. Alzheimers Dement. 2011, 7, 270–279. [Google Scholar] [CrossRef] [Green Version]
- McKhann, G.M.; Knopman, D.S.; Chertkow, H.; Hyman, B.T.; Jack, C.R.; Kawas, C.H., Jr.; Klunk, W.E.; Koroshetz, W.J.; Manly, J.J.; Mayeux, R.; et al. The diagnosis of dementia due to Alzheimer’s disease: Recommendations from the National Institute on Aging-Alzheimer’s Association workgroups on diagnostic guidelines for Alzheimer’s disease. Alzheimers Dement. 2011, 7, 263–269. [Google Scholar] [CrossRef] [Green Version]
- Whelton, P.K.; Carey, R.M.; Aronow, W.S.; Casey, D.E., Jr.; Collins, K.J.; Dennison Himmelfarb, C.; DePalma, S.M.; Gidding, S.; Jamerson, K.A.; Jones, D.W.; et al. 2017 guideline for the prevention, detection, evaluation, and management of high blood pressure in adults: Executive summary; A report of the American College of Cardiology/American Heart Association Task Force on clinical practice guidelines. Circulation 2018, 138, e426–e483. [Google Scholar] [CrossRef]
- Dobrynina, L.A.; Zabitova, M.R.; Shabalina, A.A.; Kremneva, E.I.; Akhmetzyanov, B.M.; Gadzhieva, Z.S.; Berdalin, A.B.; Kalashnikova, L.A.; Gnedovskaya, E.V.; Krotenkova, M.V.; et al. MRI types of cerebral small vessel disease and circulating markers of vascular wall damage. Diagnostics 2020, 10, 354. [Google Scholar] [CrossRef]
- Roth, G.A.; Fihn, S.D.; Mokdad, A.H.; Aekplakorn, W.; Hasegawa, T.; Lim, S.S. High total serum cholesterol, medication coverage and therapeutic control: An analysis of national health examination survey data from eight countries. Bull. World Health Organ. 2011, 89, 92–101. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. World Health Statistics 2016: Monitoring Health for the Sustainable Development Goals Sustainable Development Goals; World Health Organization: Geneva, Switzerland, 2016; p. 122. [Google Scholar]
- Fazekas, F.; Chawluk, J.B.; Alavi, A.; Hurtig, H.I.; Zimmerman, R.A. MR signal abnormalities at 1.5 T in Alzheimer’s dementia and normal aging. AJR Am. J. Roentgenol. 1987, 149, 351–356. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leemans, A.; Jones, D.K. The B-matrix must be rotated when correcting for subject motion in DTI data. Magn. Reason. Med. 2009, 61, 1336–1349. [Google Scholar] [CrossRef]
- Nosarti, C.; Rushe, T.M.; Woodruff, P.W.; Stewart, A.L.; Rifkin, L.; Murray, R.M. Corpus callosum size and very preterm birth: Relationship to neuropsychological outcome. Brain 2004, 127 Pt 9, 2080–2089. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Concha, L.; Gross, D.W.; Beaulieu, C. Diffusion tensor tractography of the limbic system. AJNR Am. J. Neuroradiol. 2005, 26, 2267–2274. [Google Scholar] [PubMed]
- Kim, K.W.; MacFall, J.R.; Payne, M.E. Classification of white matter lesions on magnetic resonance imaging in elderly persons. Biol. Psychiatr. 2008, 64, 273–280. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ashburner, J.; Friston, K.J. Voxel-based morphometry—The methods. Neuroimage 2000, 11 Pt 1, 805–821. [Google Scholar] [CrossRef] [Green Version]
- Schmidt, P.; Wink, L. LST: A Lesion Segmentation Tool for SPM.; Manual/Documentation for Version 3.0.0; Monash Department of Neuroscience: Melbourne, Australia, October 2019. [Google Scholar]
- Kalaria, R.N. Neuropathological diagnosis of vascular cognitive impairment and vascular dementia with implications for Alzheimer’s disease. Acta Neuropathol. 2016, 131, 659–685. [Google Scholar] [CrossRef] [Green Version]
- Abraham, H.M.; Wolfson, L.; Moscufo, N.; Guttmann, C.R.; Kaplan, R.F.; White, W.B. Cardiovascular risk factors and small vessel disease of the brain: Blood pressure, white matter lesions, and functional decline in older persons. J. Cereb. Blood Flow Metab. 2016, 36, 132–142. [Google Scholar] [CrossRef] [Green Version]
- Yamanouchi, H.; Sugiura, S.; Shimada, H. Loss of nerve fibres in the corpus callosum of progressive subcortical vascular encephalopathy. J. Neurol. 1990, 237, 39–41. [Google Scholar] [CrossRef]
- Huang, S.Y.; Fan, Q.; Machado, N.; Eloyan, A.; Bireley, J.D.; Russo, A.W.; Tobyne, S.M.; Patel, K.R.; Brewer, K.; Rapaport, S.F.; et al. Corpus callosum axon diameter relates to cognitive impairment in multiple sclerosis. Ann. Clin. Transl. Neurol. 2019, 6, 882–892. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xie, M.; Tobin, J.E.; Budde, M.D.; Chen, C.I.; Trinkaus, K.; Cross, A.H.; McDaniel, D.P.; Song, S.K.; Armstrong, R.C. Rostrocaudal analysis of corpus callosum demyelination and axon damage across disease stages refines diffusion tensor imaging correlations with pathological features. J. Neuropathol. Exp. Neurol. 2010, 69, 704–716. [Google Scholar] [CrossRef] [PubMed]
- Ryberg, C.; Rostrup, E.; Paulson, O.B.; Barkhof, F.; Scheltens, P.; van Straaten, E.C.; van der Flier, W.M.; Fazekas, F.; Schmidt, R.; Ferro, J.M.; et al. Corpus callosum atrophy as a predictor of age-related cognitive and motor impairment: A 3-year follow-up of the LADIS study cohort. J. Neurol. Sci. 2011, 307, 100–105. [Google Scholar] [CrossRef] [PubMed]
- Metzler-Baddeley, C.; Jones, D.K.; Steventon, J.; Westacott, L.; Aggleton, J.P.; O’Sullivan, M.J. Cingulum microstructure predicts cognitive control in older age and mild cognitive impairment. J. Neurosci. 2012, 32, 17612–17619. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, S.; Choi, S.H.; Lee, Y.M.; Kim, M.J.; Kim, Y.D.; Kim, J.Y.; Park, J.H.; Myung, W.; Na, H.R.; Han, H.J.; et al. Periventricular white matter hyperintensities and the risk of dementia: A CREDOS study. Int. Psychogeriatr. 2015, 27, 2069–2077. [Google Scholar] [CrossRef] [PubMed]
- Parlatini, V.; Radua, J.; Dell’Acqua, F.; Leslie, A.; Simmons, A.; Murphy, D.G.; Catani, M.; Thiebaut de Schotten, M. Functional segregation and integration within fronto-parietal networks. Neuroimage 2017, 146, 367–375. [Google Scholar] [CrossRef]
- Bateman, G.A. Pulse-wave encephalopathy: A comparative study of the hydrodynamics of leukoaraiosis and normal-pressure hydrocephalus. Neuroradiology 2002, 44, 740–748. [Google Scholar] [CrossRef]
- Bateman, G.A.; Levi, C.R.; Schofield, P.; Wang, Y.; Lovett, E.C. The venous manifestations of pulse wave encephalopathy: Windkessel dysfunction in normal aging and senile dementia. Neuroradiology 2008, 50, 491–497. [Google Scholar] [CrossRef]
- Schmidt, R.; Schmidt, H.; Haybaeck, J.; Loitfelder, M.; Weis, S.; Cavalieri, M.; Seiler, S.; Enzinger, C.; Ropele, S.; Erkinjuntti, T.; et al. Heterogeneity in age-related white matter changes. Acta Neuropathol. 2011, 122, 171–185. [Google Scholar] [CrossRef]
- Castejón, O.J. Ultrastructural pathology of oligodendroglial cells in traumatic and hydrocephalic human brain edema: A review. Ultrastruct. Pathol. 2015, 39, 359–368. [Google Scholar] [CrossRef]
- Castejón, O.J.; Arismendi, G.J. Nerve cell death types in the edematous human cerebral cortex. J. Submicrosc. Cytol. Pathol. 2006, 38, 21–36. [Google Scholar] [PubMed]
- Dobrynina, L.A.; Akhmetzyanov, B.M.; Gadzhieva, Z.S.; Kremneva, E.I.; Kalashnikova, L.A.; Krotenkova, M.V. The role of arterial and venous blood flow and cerebrospinal fluid flow disturbances in the development of cognitive impairments in cerebral microangiopathy. Ann. Clin. Exp. Neurol. 2019, 13, 19–31. (In Russian) [Google Scholar] [CrossRef]
- Verheggen, I.C.M.; Van Boxtel, M.P.J.; Verhey, F.R.J.; Jansen, J.F.A.; Backes, W.H. Interaction between blood-brain barrier and glymphatic system in solute clearance. Neurosci. Biobehav. Rev. 2018, 90, 26–33. [Google Scholar] [CrossRef] [PubMed]
- Rasmussen, M.K.; Mestre, H.; Nedergaard, M. The glymphatic pathway in neurological disorders. Lancet Neurol. 2018, 17, 1016–1024. [Google Scholar] [CrossRef] [Green Version]
- Habes, M.; Sotiras, A.; Erus, G.; Toledo, J.B.; Janowitz, D.; Wolk, D.A.; Shou, H.; Bryan, N.R.; Doshi, J.; Völzke, H.; et al. White matter lesions: Spatial heterogeneity, links to risk factors, cognition, genetics, and atrophy. Neurology 2018, 91, e964–e975. [Google Scholar] [CrossRef]
- Marnane, M.; Al-Jawadi, O.O.; Mortazavi, S.; Pogorzelec, K.J.; Wang, B.W.; Feldman, H.H.; Hsiung, G.Y.; Alzheimer’s Disease Neuroimaging Initiative. Periventricular hyperintensities are associated with elevated cerebral amyloid. Neurology 2016, 86, 535–543. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
{kind=link}
| Parameters | CSVD (n = 74) | Control (n = 18) | p |
|---|---|---|---|
| Sex, women (n, %) | 48 (64.8%) | 12 (66.6%) | 0.559 |
| Age, years (mean ± SD, min., max.) | 60.7 ± 6.9, min. 45, max. 70 | 57.8 ± 5.9, min. 45, max. 67 | 0.084 |
| Education, years (mean ± SD, min., max.) | 14.3 ± 2.4, min. 8, max. 20 | 15.7 ± 2.2, min. 11, max. 20 | 0.136 |
| AH (n, %) | 60 (81.1%) | 7 (38.9%) | <0.001 |
| Degree of AH (n, %) | |||
| stage 1 | 7 (9.5%) | 4 (22.2%) | |
| stage 2 | 12 (16.2%) | 2 (11.1%) | |
| stage 3 | 41 (55.4%) | 1 (5.6%) | |
| DM type 2 (n, %) | 16 (21.6%) | 0 (0%) | 0.065 |
| Hypercholesterolemia (total cholesterol > 6.2 mmol/L or statin use) (n, %) | 34 (45.9%) | 6 (33.3%) | 0.128 |
| Smoking (n, %) | 21 (28.4%) | 6 (33.3%) | 0.559 |
| Obesity (body mass index > 30 kg/m²) (n, %) | 27 (36.5%) | 1 (5.6%) | 0.354 |
| MoCA score (Me [Q25%; Q75%]) | 25 [22; 27] | 29 [28; 30] | <0.001 |
| Cognitive impairment (n, %): | 74 (100%) | ||
| SCI | 29 (39.2%) | ||
| MCI | 33 (44.6%) | ||
| dementia | 12 (16.2%) | ||
| WMH, Fazekas Scale (n, %) | 74 (100%) | ||
| grade 1 | 19 (25.6%) | ||
| grade 2 | 23 (31.1%) | ||
| grade 3 | 32 (43.3%) | ||
| Lacunae (n, %) | 36 (48.6%) | ||
| Microbleeds (n, %) | 28 (37.8%) | ||
| Perivascular spaces (n, %) | 74 (100%) |
| ROI | FA (Mean ± SD) | p | MD (Mean ± SD) | p | ||
|---|---|---|---|---|---|---|
| CSVD (n = 74) | Control (n = 18) | CSVD (n = 74) | Control (n = 18) | |||
| Anterior frontal | ||||||
| jcNAWM | 33.14 ± 7.99 | 29.03 ± 7.74 | 0.023 | 9.26 ± 0.73 | 10.29 ± 0.97 | <0.001 |
| dNAWM | 33.29 ± 10.04 | 28.55 ± 6.97 | 0.014 | 9.12 ± 0.82 | 10.05 ± 1.16 | <0.001 |
| pvNAWM | 27.15 ± 8.94 | 34.15 ± 11.49 | 0.047 | 9.32 ± 0.82 | 10.09 ± 1.44 | 0.041 |
| Posterior frontal | ||||||
| jcNAWM | 35.86 ± 7.52 | 35.89 ± 9.28 | 0.919 | 9.50 ± 0.75 | 10.18 ± 1.16 | 0.015 |
| dNAWM | 34.29 ± 7.10 | 34.16 ± 8.16 | 0.646 | 8.67 ± 0.78 | 9.69 ± 1.09 | <0.001 |
| pvNAWM | 36.80 ± 9.78 | 27.67 ± 9.38 | 0.004 | 8.64 ± 0.80 | 11.45 ± 2.34 | <0.001 |
| Temporoparietal | ||||||
| jcNAWM | 43.84 ± 7.78 | 35.26 ± 10.35 | 0.002 | 8.58 ± 0.54 | 9.78 ± 1.25 | <0.001 |
| dNAWM | 34.37 ± 7.22 | 35.28 ± 10.83 | 0.935 | 9.43 ± 1.14 | 9.67 ± 1.21 | 0.584 |
| pvNAWM | 47.74 ± 7.89 | 50.69 ± 12.67 | 0.256 | 9.38 ± 0.52 | 10.19 ± 1.38 | 0.022 |
| Anterior CB | ||||||
| left | 46.69 ± 8.38 | 39.47 ± 10.42 | 0.017 | 9.41 ± 1.17 | 10.25 ± 1.13 | 0.019 |
| right | 46.32 ± 9.11 | 41.06 ± 11.89 | 0.059 | 8.69 ± 1.10 | 9.86 ± 1.28 | 0.001 |
| Middle CB | ||||||
| left | 58.86 ± 10.96 | 49.12 ± 12.41 | 0.005 | 8.46 ± 0.88 | 9.29 ± 1.17 | 0.002 |
| right | 54.57 ± 11.89 | 49.28 ± 11.42 | 0.068 | 8.55 ± 0.97 | 9.09 ± 1.42 | 0.106 |
| Posterior CB | ||||||
| left | 35.81 ± 11.77 | 33.79 ±1 3.61 | 0.370 | 10.22 ± 4.34 | 9.62 ± 1.25 | 0.306 |
| right | 37.03 ± 18.91 | 33.30 ± 12.46 | 0.466 | 9.19 ± 1.08 | 9.65 ± 1.67 | 0.121 |
| Anterior CC | 90.93 ± 4.82 | 76.83 ± 14.81 | <0.001 | 7.48 ± 0.76 | 9.41 ± 2.52 | 0.002 |
| Mid-anterior CC | 61.48 ± 7.92 | 46.35 ± 14.77 | <0.001 | 11.36 ± 1.69 | 13.65 ± 3.17 | 0.004 |
| Mid-posterior CC | 57.61 ± 13.49 | 48.25 ± 15.21 | 0.040 | 12.16 ± 1.98 | 14.99 ± 3.90 | 0.022 |
| Posterior CC | 86.99 ± 4.13 | 79.35 ± 12.54 | 0.018 | 8.53 ± 1.04 | 9.79 ± 2.23 | 0.004 |
| Hippocampus | ||||||
| left | 30.51 ± 9.45 | 30.68 ± 8.69 | 0.946 | 10.82 ± 1.50 | 10.88 ± 1.77 | 0.899 |
| right | 31.34 ± 7.16 | 30.09 ± 9.59 | 0.858 | 10.29 ± 1.05 | 10.67 ± 1.91 | 0.273 |
| ROI | AD (Mean ± SD) | p | RD (Mean ± SD) | p | ||
|---|---|---|---|---|---|---|
| CSVD (n = 74) | Control (n = 18) | CSVD (n = 74) | Control (n = 18) | |||
| Anterior frontal | ||||||
| jcNAWM | 12.52 ± 1.14 | 13.38 ± 1.29 | <0.001 | 7.62 ± 0.91 | 8.75 ± 1.17 | 0.017 |
| dNAWM | 12.19 ± 1.13 | 12.99 ± 1.26 | 0.001 | 7.58 ± 0.94 | 8.59 ± 1.01 | 0.008 |
| pvNAWM | 11.94 ± 0.92 | 13.87 ± 2.18 | 0.001 | 8.01 ± 1.09 | 8.20 ± 1.66 | 0.582 |
| Posterior frontal | ||||||
| jcNAWM | 13.19 ± 1.20 | 14.06 ± 1.59 | 0.064 | 7.65 ± 0.85 | 8.24 ± 1.32 | 0.026 |
| dNAWM | 11.83 ± 1.03 | 13.21 ± 1.55 | 0.005 | 7.09 ± 0.88 | 7.94 ± 1.19 | 0.002 |
| pvNAWM | 12.39 ± 0.82 | 14.71 ± 2.34 | <0.001 | 6.76 ± 1.22 | 9.82 ± 2.53 | <0.001 |
| Temporoparietal | ||||||
| jcNAWM | 12.77 ± 1.21 | 13.48 ± 1.48 | <0.001 | 6.48 ± 0.69 | 7.93 ± 1.55 | 0.053 |
| dNAWM | 12.98 ± 1.45 | 13.35 ± 1.57 | 0.754 | 7.66 ± 1.16 | 7.84 ± 1.47 | 0.618 |
| pvNAWM | 14.45 ± 1.72 | 16.45 ± 2.61 | 0.730 | 6.85 ± 0.76 | 7.05 ± 1.68 | 0.636 |
| Anterior CB | ||||||
| left | 14.57 ± 1.59 | 14.79 ± 1.74 | 0.010 | 6.83 ± 1.49 | 7.98 ± 1.35 | 0.798 |
| right | 13.45 ± 1.65 | 14.45 ± 1.96 | 0.002 | 6.31 ± 1.20 | 7.56 ± 1.63 | 0.001 |
| Middle CB | ||||||
| left | 14.46 ± 2.52 | 14.78 ± 2.29 | 0.005 | 5.46 ± 1.15 | 6.54 ± 1.41 | 0.630 |
| right | 14.39 ± 2.19 | 14.45 ± 2.63 | 0.917 | 5.63 ± 1.13 | 6.40 ± 1.41 | 0.976 |
| Posterior CB | ||||||
| left | 14.03 ± 4.35 | 13.38 ± 2.25 | 0.545 | 8.31 ± 4.53 | 7.74 ± 1.59 | 0.608 |
| right | 13.05 ± 2.60 | 13.39 ± 2.31 | 0.201 | 7.26 ± 1.88 | 7.78 ± 1.57 | 0.290 |
| Anterior CC | 19.26 ± 1.79 | 19.85 ± 2.43 | 0.259 | 1.62 ± 0.77 | 4.19 ± 3.09 | 0.454 |
| Mid-anterior CC | 20.41 ± 2.46 | 20.94 ± 2.29 | 0.407 | 6.83 ± 1.61 | 9.99 ± 3.86 | 0.355 |
| Mid-posterior CC | 20.91 ± 2.24 | 23.36 ± 2.89 | <0.001 | 7.79 ± 2.49 | 10.81 ± 4.67 | 0.010 |
| Posterior CC | 20.34 ± 1.81 | 21.26 ± 2.21 | 0.075 | 2.62 ± 1.37 | 4.05 ± 2.68 | 0.098 |
| Hippocampus | ||||||
| left | 14.35 ± 1.31 | 14.51 ± 1.85 | 0.678 | 9.06 ± 1.84 | 9.06 ± 2.01 | 0.976 |
| right | 13.93 ± 1.51 | 14.15 ± 1.98 | 0.609 | 8.48 ± 1.07 | 8.92 ± 2.12 | 0.393 |
| Predictors | B (Coefficients of Predictors) | p | OR | 95% CI | |
|---|---|---|---|---|---|
| Lower | Upper | ||||
| AD of posterior frontal pvNAWM (χ1) | 11,053.52 | 0.014 | 4.050 | 1.375 | 11.928 |
| AD of right middle CB (χ2) | 7248.06 | 0.011 | 2.966 | 1.128 | 7.801 |
| AD of mid-posterior CC (χ3) | 6310.07 | 0.046 | 4.955 | 1.724 | 14.242 |
| Constant | –39.81 | 0.025 | |||
| Parameters | CSVD (n = 74) | Control (n = 18) | p |
|---|---|---|---|
| tABF (ml/min) | 506.86 ± 128.25 | 566.22 ± 127.84 | 0.159 |
| stVBF (ml/min) | 86.15 ± 23.29 | 99.39 ± 18.93 | 0.067 |
| sssVBF (ml/min) | 241.85 ± 59.95 | 285.94 ± 62.21 | 0.024 |
| Pi | 1.12 ± 0.29 | 1.05 ± 0.23 | 0.351 |
| aqCSF flow (mm3/s) | 74.16 ± 65.97 | 47.76 ± 19.46 | 0.011 |
| sAq (mm2) | 8.18 ± 3.28 | 6.47 ± 1.09 | 0.093 |
| tBV (cm3) | 1009.91 ± 113.57 | 1102.74 ± 68.59 | 0.004 |
| vLV (cm3) | 39.92 ± 24.64 | 19.79 ± 9.42 | 0.001 |
| tCSF (cm3) | 497.01 ± 112.93 | 390.32 ± 82.15 | 0.001 |
| tWM (cm3) | 450.30 ± 59.79 | 465.86 ± 43.43 | 0.276 |
| tGM (cm3) | 559.61 ± 74.09 | 636.88 ± 43.19 | 0.001 |
| tWM/tBV | 0.446 ± 0.037 | 0.422 ± 0.024 | 0.009 |
| tGM/tBV | 0.554 ± 0.037 | 0.577 ± 0.024 | 0.009 |
| vWMH (cm3) | 22.963 ± 13.6 |
| Parameters | AD of Posterior Frontal pvNAWM | AD of Mid−Posterior CC | AD of Right Middle CB |
|---|---|---|---|
| tABF | −0.451 ** | −0.406 ** | 0.152 |
| stVBF | −0.461 ** | −0.371 ** | 0.222 |
| sssVBF | −0.317 ** | −0.415 ** | 0.218 |
| Pi | 0.313 * | 0.406 ** | 0.030 |
| aqCSF flow | 0.269 * | 0.073 | 0.234 * |
| sAq | 0.237 * | 0.200 | 0.328 ** |
| tBV | −0.189 | −0.167 | 0.020 |
| vLV | 0.580 ** | 0.377 ** | 0.135 |
| tCSF | 0.570 ** | 0.308 ** | 0.221 * |
| tWM | 0.013 | −0.026 | 0.089 |
| tGM | −0.294 * | −0.230 * | −0.038 |
| tWM/tBV | 0.285 | 0.173 | 0.132 |
| tGM/tBV | −0.285 * | −0.173 | −0.132 |
| vWMH | 0.410 ** | 0.360 ** | 0.080 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dobrynina, L.A.; Gadzhieva, Z.S.; Shamtieva, K.V.; Kremneva, E.I.; Akhmetzyanov, B.M.; Kalashnikova, L.A.; Krotenkova, M.V. Microstructural Predictors of Cognitive Impairment in Cerebral Small Vessel Disease and the Conditions of Their Formation. Diagnostics 2020, 10, 720. https://doi.org/10.3390/diagnostics10090720
Dobrynina LA, Gadzhieva ZS, Shamtieva KV, Kremneva EI, Akhmetzyanov BM, Kalashnikova LA, Krotenkova MV. Microstructural Predictors of Cognitive Impairment in Cerebral Small Vessel Disease and the Conditions of Their Formation. Diagnostics. 2020; 10(9):720. https://doi.org/10.3390/diagnostics10090720
Chicago/Turabian StyleDobrynina, Larisa A., Zukhra Sh. Gadzhieva, Kamila V. Shamtieva, Elena I. Kremneva, Bulat M. Akhmetzyanov, Ludmila A. Kalashnikova, and Marina V. Krotenkova. 2020. "Microstructural Predictors of Cognitive Impairment in Cerebral Small Vessel Disease and the Conditions of Their Formation" Diagnostics 10, no. 9: 720. https://doi.org/10.3390/diagnostics10090720
APA StyleDobrynina, L. A., Gadzhieva, Z. S., Shamtieva, K. V., Kremneva, E. I., Akhmetzyanov, B. M., Kalashnikova, L. A., & Krotenkova, M. V. (2020). Microstructural Predictors of Cognitive Impairment in Cerebral Small Vessel Disease and the Conditions of Their Formation. Diagnostics, 10(9), 720. https://doi.org/10.3390/diagnostics10090720